
High Intratumoral i-tRF-GlyGCC Expression Predicts Short-Term Relapse and Poor Overall Survival of Colorectal Cancer Patients, Independent of the TNM Stage

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Collection of Colorectal Tissue Samples
2.2. Clinical Characteristics of CRC Patients
2.3. Total RNA Extraction and Polyadenylation, Followed by First-Strand cDNA Synthesis
2.4. SYBR Green Based Real-Time Quantitative PCR (qPCR)
2.5. Extended Biostatistics, including Disease-Free and Overall Survival Analyses
3. Results
3.1. i-tRF-GlyGCC Expression Is Downregulated in CRC Tissues, Compared to Adjacent Normal Colorectal Tissues
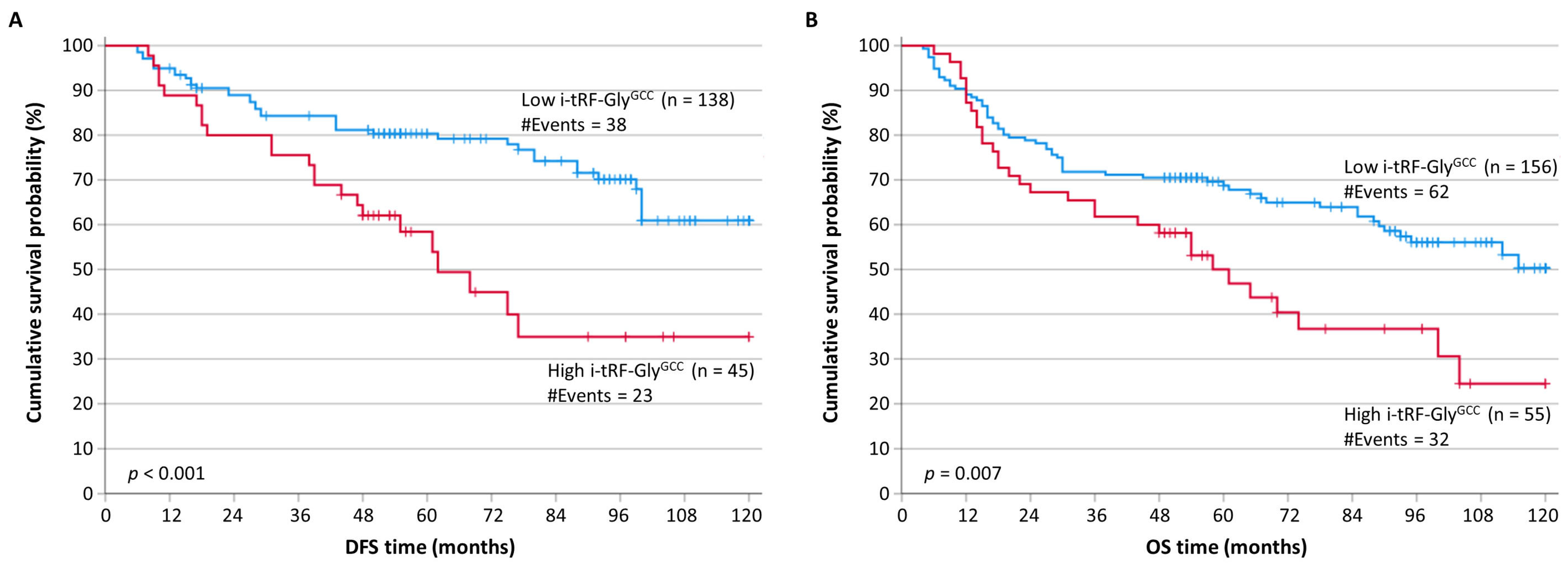
3.2. i-tRF-GlyGCC Overexpression Represents a Reliable Indicator of Poor Prognosis in CRC
3.3. The Prognostic Signficance of i-tRF-GlyGCC Expression Is Independent of Other Classical Prognostic Factors Applied in CRC
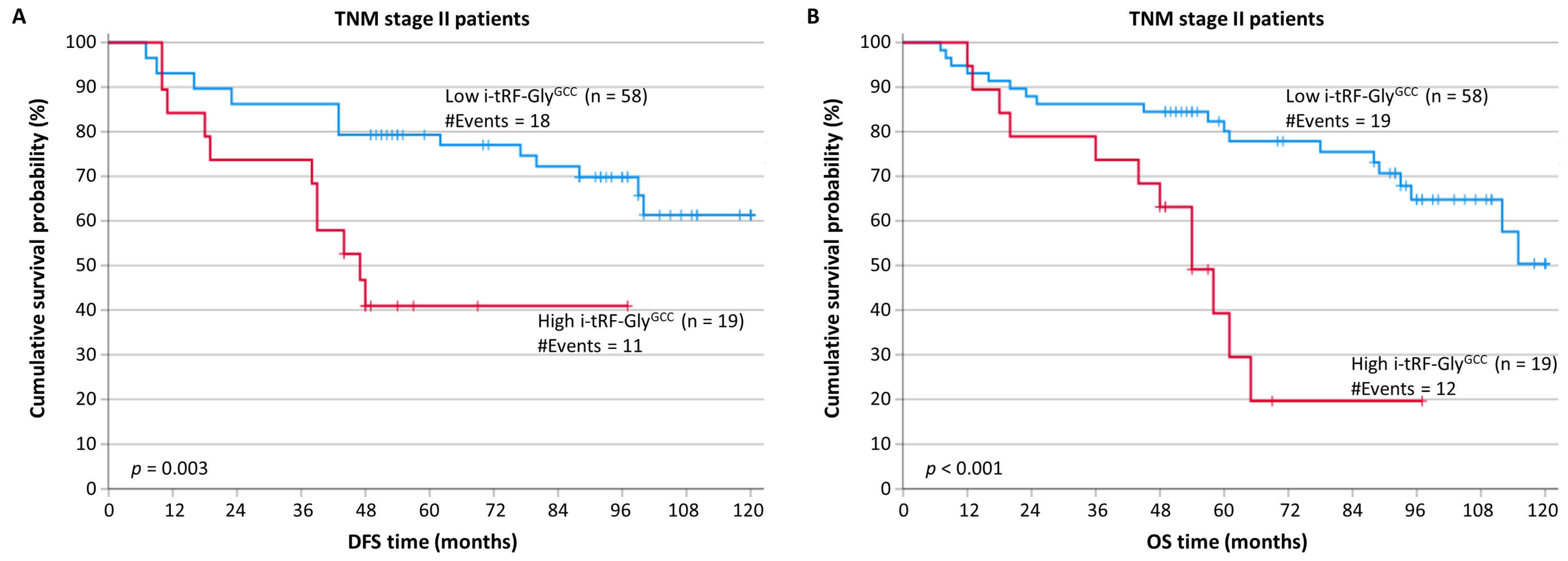
3.4. i-tRF-GlyGCC Overexpression Predicts Tumor Recurence and Poor Prognostic Outcome in CRC Patients in TNM Stage II
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Patel, S.G.; Karlitz, J.J.; Yen, T.; Lieu, C.H.; Boland, C.R. The rising tide of early-onset colorectal cancer: A comprehensive review of epidemiology, clinical features, biology, risk factors, prevention, and early detection. Lancet Gastroenterol. Hepatol. 2022, 7, 262–274. [Google Scholar] [CrossRef] [PubMed]
- Sinicrope, F.A. Increasing Incidence of Early-Onset Colorectal Cancer. N. Engl. J. Med. 2022, 386, 1547–1558. [Google Scholar] [CrossRef]
- Zhao, H.; Ming, T.; Tang, S.; Ren, S.; Yang, H.; Liu, M.; Tao, Q.; Xu, H. Wnt signaling in colorectal cancer: Pathogenic role and therapeutic target. Mol. Cancer 2022, 21, 144. [Google Scholar] [CrossRef] [PubMed]
- Eng, C.; Jácome, A.A.; Agarwal, R.; Hayat, M.H.; Byndloss, M.X.; Holowatyj, A.N.; Bailey, C.; Lieu, C.H. A comprehensive framework for early-onset colorectal cancer research. Lancet Oncol. 2022, 23, e116–e128. [Google Scholar] [CrossRef]
- Zygulska, A.L.; Pierzchalski, P. Novel Diagnostic Biomarkers in Colorectal Cancer. Int. J. Mol. Sci. 2022, 23, 852. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, N.N. Colorectal Cancer: Preoperative Evaluation and Staging. Surg. Oncol. Clin. N. Am. 2022, 31, 127–141. [Google Scholar] [CrossRef]
- Poston, G.J. Staging of advanced colorectal cancer. Surg. Oncol. Clin. N. Am. 2008, 17, 503–517. [Google Scholar] [CrossRef]
- Jin, M.; Frankel, W.L. Lymph Node Metastasis in Colorectal Cancer. Surg. Oncol. Clin. N. Am. 2018, 27, 401–412. [Google Scholar] [CrossRef]
- Lea, D.; Håland, S.; Hagland, H.R.; Søreide, K. Accuracy of TNM staging in colorectal cancer: A review of current culprits, the modern role of morphology and stepping-stones for improvements in the molecular era. Scand. J. Gastroenterol. 2014, 49, 1153–1163. [Google Scholar] [CrossRef]
- Delattre, J.-F.; Selcen Oguz Erdogan, A.; Cohen, R.; Shi, Q.; Emile, J.-F.; Taieb, J.; Tabernero, J.; André, T.; Meyerhardt, J.A.; Nagtegaal, I.D.; et al. A comprehensive overview of tumour deposits in colorectal cancer: Towards a next TNM classification. Cancer Treat. Rev. 2022, 103, 102325. [Google Scholar] [CrossRef]
- Lech, G.; Slotwinski, R.; Słodkowski, M.; Krasnodębski, I.W. Colorectal cancer tumour markers and biomarkers: Recent therapeutic advances. World J. Gastroenterol. 2016, 22, 1745–1755. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.-J.; Zhao, Q.; Liu, J.; Zheng, J.-B.; Qiu, M.-Z.; Ju, H.-Q.; Xu, R.-H. Novel Genetic and Epigenetic Biomarkers of Prognostic and Predictive Significance in Stage II/III Colorectal Cancer. Mol. Ther. 2021, 29, 587–596. [Google Scholar] [CrossRef] [PubMed]
- Ciardiello, F.; Ciardiello, D.; Martini, G.; Napolitano, S.; Tabernero, J.; Cervantes, A. Clinical management of metastatic colorectal cancer in the era of precision medicine. CA Cancer J. Clin. 2022, 72, 372–401. [Google Scholar] [CrossRef]
- Malla, M.; Loree, J.M.; Kasi, P.M.; Parikh, A.R. Using Circulating Tumor DNA in Colorectal Cancer: Current and Evolving Practices. J. Clin. Oncol. 2022, 40, 2846–2857. [Google Scholar] [CrossRef]
- Luo, H.; Zhao, Q.; Wei, W.; Zheng, L.; Yi, S.; Li, G.; Wang, W.; Sheng, H.; Pu, H.; Mo, H.; et al. Circulating tumor DNA methylation profiles enable early diagnosis, prognosis prediction, and screening for colorectal cancer. Sci. Transl. Med. 2020, 12, eaax7533. [Google Scholar] [CrossRef]
- Artemaki, P.I.; Papatsirou, M.; Boti, M.A.; Adamopoulos, P.G.; Christodoulou, S.; Vassilacopoulou, D.; Scorilas, A.; Kontos, C.K. Revised Exon Structure of l-DOPA Decarboxylase (DDC) Reveals Novel Splice Variants Associated with Colorectal Cancer Progression. Int. J. Mol. Sci. 2020, 21, 8568. [Google Scholar] [CrossRef] [PubMed]
- Kontos, C.K.; Adamopoulos, P.G.; Scorilas, A. Prognostic and predictive biomarkers in prostate cancer. Expert Rev. Mol. Diagn. 2015, 15, 1567–1576. [Google Scholar] [CrossRef] [Green Version]
- Papanota, A.-M.; Karousi, P.; Kontos, C.K.; Artemaki, P.I.; Liacos, C.-I.; Papadimitriou, M.-A.; Bagratuni, T.; Eleutherakis-Papaiakovou, E.; Malandrakis, P.; Ntanasis-Stathopoulos, I.; et al. A Cancer-Related microRNA Signature Shows Biomarker Utility in Multiple Myeloma. Int. J. Mol. Sci. 2021, 22, 13144. [Google Scholar] [CrossRef]
- Papatsirou, M.; Artemaki, P.I.; Karousi, P.; Scorilas, A.; Kontos, C.K. Circular RNAs: Emerging Regulators of the Major Signaling Pathways Involved in Cancer Progression. Cancers 2021, 13, 2744. [Google Scholar] [CrossRef]
- Skeparnias, I.; Anastasakis, D.; Grafanaki, K.; Kyriakopoulos, G.; Alexopoulos, P.; Dougenis, D.; Scorilas, A.; Kontos, C.K.; Stathopoulos, C. Contribution of miRNAs, tRNAs and tRFs to Aberrant Signaling and Translation Deregulation in Lung Cancer. Cancers 2020, 12, 3056. [Google Scholar] [CrossRef]
- Artemaki, P.I.; Kontos, C.K. Editorial for the Special Issue “Molecular Biomarkers in Colorectal Adenocarcinoma”. Int. J. Mol. Sci. 2021, 22, 2052. [Google Scholar] [CrossRef] [PubMed]
- Kontos, C.K.; Avgeris, M.; Vassilacopoulou, D.; Ardavanis, A.; Scorilas, A. Molecular Effects of Treatment of Human Colorectal Cancer Cells with Natural and Classical Chemotherapeutic Drugs: Alterations in the Expression of Apoptosis-related BCL2 Family Members, Including BCL2L12. Curr. Pharm. Biotechnol. 2018, 19, 1064–1075. [Google Scholar] [CrossRef] [PubMed]
- Artemaki, P.I.; Scorilas, A.; Kontos, C.K. Circular RNAs: A New Piece in the Colorectal Cancer Puzzle. Cancers 2020, 12, 2464. [Google Scholar] [CrossRef]
- Alexopoulou, D.K.; Kontos, C.K.; Christodoulou, S.; Papadopoulos, I.N.; Scorilas, A. KLK11 mRNA expression predicts poor disease-free and overall survival in colorectal adenocarcinoma patients. Biomark. Med. 2014, 8, 671–685. [Google Scholar] [CrossRef] [PubMed]
- Christodoulou, S.; Alexopoulou, D.K.; Kontos, C.K.; Scorilas, A.; Papadopoulos, I.N. Kallikrein-related peptidase-6 (KLK6) mRNA expression is an independent prognostic tissue biomarker of poor disease-free and overall survival in colorectal adenocarcinoma. Tumor Biol. 2014, 35, 4673–4685. [Google Scholar] [CrossRef] [PubMed]
- Kontos, C.K.; Chantzis, D.; Papadopoulos, I.N.; Scorilas, A. Kallikrein-related peptidase 4 (KLK4) mRNA predicts short-term relapse in colorectal adenocarcinoma patients. Cancer Lett. 2013, 330, 106–112. [Google Scholar] [CrossRef]
- Kontos, C.K.; Mavridis, K.; Talieri, M.; Scorilas, A. Kallikrein-related peptidases (KLKs) in gastrointestinal cancer: Mechanistic and clinical aspects. Thromb. Haemost. 2013, 110, 450–457. [Google Scholar] [CrossRef]
- Kontos, C.K.; Scorilas, A. Kallikrein-related peptidases (KLKs): A gene family of novel cancer biomarkers. Clin. Chem. Lab. Med. 2012, 50, 1877–1891. [Google Scholar] [CrossRef]
- Kontos, C.K.; Papadopoulos, I.N.; Fragoulis, E.G.; Scorilas, A. Quantitative expression analysis and prognostic significance of L-DOPA decarboxylase in colorectal adenocarcinoma. Br. J. Cancer 2010, 102, 1384–1390. [Google Scholar] [CrossRef] [Green Version]
- Kontos, C.K.; Papadopoulos, I.N.; Scorilas, A. Quantitative expression analysis and prognostic significance of the novel apoptosis-related gene BCL2L12 in colon cancer. Biol. Chem. 2008, 389, 1467–1475. [Google Scholar] [CrossRef]
- Kontos, C.K.; Christodoulou, M.-I.; Scorilas, A. Apoptosis-related BCL2-family members: Key players in chemotherapy. Anticancer Agents Med. Chem. 2014, 14, 353–374. [Google Scholar] [CrossRef]
- Artemaki, P.I.; Sklirou, A.D.; Kontos, C.K.; Liosi, A.-A.; Gianniou, D.D.; Papadopoulos, I.N.; Trougakos, I.P.; Scorilas, A. High clusterin (CLU) mRNA expression levels in tumors of colorectal cancer patients predict a poor prognostic outcome. Clin. Biochem. 2020, 75, 62–69. [Google Scholar] [CrossRef]
- Kalioraki, M.A.; Artemaki, P.I.; Sklirou, A.D.; Kontos, C.K.; Adamopoulos, P.G.; Papadopoulos, I.N.; Trougakos, I.P.; Scorilas, A. Heat shock protein beta 3 (HSPB3) is an unfavorable molecular biomarker in colorectal adenocarcinoma. Mol. Carcinog. 2020, 59, 116–125. [Google Scholar] [CrossRef]
- Papatsirou, M.; Artemaki, P.I.; Scorilas, A.; Kontos, C.K. The role of circular RNAs in therapy resistance of patients with solid tumors. Pers. Med. 2020, 17, 469–490. [Google Scholar] [CrossRef] [PubMed]
- Papatsirou, M.; Diamantopoulos, M.A.; Katsaraki, K.; Kletsas, D.; Kontos, C.K.; Scorilas, A. Identification of Novel Circular RNAs of the Human Protein Arginine Methyltransferase 1 (PRMT1) Gene, Expressed in Breast Cancer Cells. Genes 2022, 13, 1133. [Google Scholar] [CrossRef] [PubMed]
- Adamopoulos, P.G.; Kontos, C.K.; Rapti, S.-M.; Papadopoulos, I.N.; Scorilas, A. miR-224 overexpression is a strong and independent prognosticator of short-term relapse and poor overall survival in colorectal adenocarcinoma. Int. J. Oncol. 2015, 46, 849–859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kontos, C.K.; Tsiakanikas, P.; Avgeris, M.; Papadopoulos, I.N.; Scorilas, A. miR-15a-5p, A Novel Prognostic Biomarker, Predicting Recurrent Colorectal Adenocarcinoma. Mol. Diagn. Ther. 2017, 21, 453–464. [Google Scholar] [CrossRef]
- Rapti, S.-M.; Kontos, C.K.; Christodoulou, S.; Papadopoulos, I.N.; Scorilas, A. miR-34a overexpression predicts poor prognostic outcome in colorectal adenocarcinoma, independently of clinicopathological factors with established prognostic value. Clin. Biochem. 2017, 50, 918–924. [Google Scholar] [CrossRef]
- Rapti, S.-M.; Kontos, C.K.; Papadopoulos, I.N.; Scorilas, A. Enhanced miR-182 transcription is a predictor of poor overall survival in colorectal adenocarcinoma patients. Clin. Chem. Lab. Med. 2014, 52, 1217–1227. [Google Scholar] [CrossRef]
- Rapti, S.-M.; Kontos, C.K.; Papadopoulos, I.N.; Scorilas, A. High miR-96 levels in colorectal adenocarcinoma predict poor prognosis, particularly in patients without distant metastasis at the time of initial diagnosis. Tumor Biol. 2016, 37, 11815–11824. [Google Scholar] [CrossRef]
- Skourti, E.; Logotheti, S.; Kontos, C.K.; Pavlopoulou, A.; Dimoragka, P.T.; Trougakos, I.P.; Gorgoulis, V.; Scorilas, A.; Michalopoulos, I.; Zoumpourlis, V. Progression of mouse skin carcinogenesis is associated with the orchestrated deregulation of mir-200 family members, mir-205 and their common targets. Mol. Carcinog. 2016, 55, 1229–1242. [Google Scholar] [CrossRef]
- Ferraro, A.; Kontos, C.K.; Boni, T.; Bantounas, I.; Siakouli, D.; Kosmidou, V.; Vlassi, M.; Spyridakis, Y.; Tsipras, I.; Zografos, G.; et al. Epigenetic regulation of miR-21 in colorectal cancer: ITGB4 as a novel miR-21 target and a three-gene network (miR-21-ITGBeta4-PDCD4) as predictor of metastatic tumor potential. Epigenetics Off. J. DNA Methylation Soc. 2014, 9, 129–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karousi, P.; Adamopoulos, P.G.; Papageorgiou, S.G.; Pappa, V.; Scorilas, A.; Kontos, C.K. A novel, mitochondrial, internal tRNA-derived RNA fragment possesses clinical utility as a molecular prognostic biomarker in chronic lymphocytic leukemia. Clin. Biochem. 2020, 85, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Krishna, S.; Raghavan, S.; DasGupta, R.; Palakodeti, D. tRNA-derived fragments (tRFs): Establishing their turf in post-transcriptional gene regulation. Cell. Mol. Life Sci. 2021, 78, 2607–2619. [Google Scholar] [CrossRef] [PubMed]
- Katsaraki, K.; Karousi, P.; Artemaki, P.I.; Scorilas, A.; Pappa, V.; Kontos, C.K.; Papageorgiou, S.G. MicroRNAs: Tiny Regulators of Gene Expression with Pivotal Roles in Normal B-Cell Development and B-Cell Chronic Lymphocytic Leukemia. Cancers 2021, 13, 593. [Google Scholar] [CrossRef]
- Kuscu, C.; Kumar, P.; Kiran, M.; Su, Z.; Malik, A.; Dutta, A. tRNA fragments (tRFs) guide Ago to regulate gene expression post-transcriptionally in a Dicer-independent manner. RNA 2018, 24, 1093–1105. [Google Scholar] [CrossRef] [Green Version]
- Kishore, C.; Karunagaran, D. Non-coding RNAs as emerging regulators and biomarkers in colorectal cancer. Mol. Cell. Biochem. 2022, 477, 1817–1828. [Google Scholar] [CrossRef]
- Lu, S.; Wei, X.; Tao, L.; Dong, D.; Hu, W.; Zhang, Q.; Tao, Y.; Yu, C.; Sun, D.; Cheng, H. A novel tRNA-derived fragment tRF-3022b modulates cell apoptosis and M2 macrophage polarization via binding to cytokines in colorectal cancer. J. Hematol. Oncol. 2022, 15, 176. [Google Scholar] [CrossRef]
- Han, Y.; Peng, Y.; Liu, S.; Wang, X.; Cai, C.; Guo, C.; Chen, Y.; Gao, L.; Huang, Q.; He, M.; et al. tRF3008A suppresses the progression and metastasis of colorectal cancer by destabilizing FOXK1 in an AGO-dependent manner. J. Exp. Clin. Cancer Res. 2022, 41, 32. [Google Scholar] [CrossRef]
- Panoutsopoulou, K.; Dreyer, T.; Dorn, J.; Obermayr, E.; Mahner, S.; Gorp, T.V.; Braicu, I.; Zeillinger, R.; Magdolen, V.; Avgeris, M.; et al. tRNA(GlyGCC)-Derived Internal Fragment (i-tRF-GlyGCC) in Ovarian Cancer Treatment Outcome and Progression. Cancers 2021, 14, 24. [Google Scholar] [CrossRef]
- Karousi, P.; Katsaraki, K.; Papageorgiou, S.G.; Pappa, V.; Scorilas, A.; Kontos, C.K. Identification of a novel tRNA-derived RNA fragment exhibiting high prognostic potential in chronic lymphocytic leukemia. Hematol. Oncol. 2019, 37, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Nagtegaal, I.D.; Quirke, P.; Schmoll, H.-J. Has the new TNM classification for colorectal cancer improved care? Nat. Rev. Clin. Oncol. 2011, 9, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Kerimis, D.; Kontos, C.K.; Christodoulou, S.; Papadopoulos, I.N.; Scorilas, A. Elevated expression of miR-24-3p is a potentially adverse prognostic factor in colorectal adenocarcinoma. Clin. Biochem. 2017, 50, 285–292. [Google Scholar] [CrossRef]
- Diamantopoulos, M.A.; Kontos, C.K.; Kerimis, D.; Papadopoulos, I.N.; Scorilas, A. Upregulated miR-16 expression is an independent indicator of relapse and poor overall survival of colorectal adenocarcinoma patients. Clin. Chem. Lab. Med. 2017, 55, 737–747. [Google Scholar] [CrossRef]
- Tsiakanikas, P.; Kontos, C.K.; Kerimis, D.; Papadopoulos, I.N.; Scorilas, A. High microRNA-28-5p expression in colorectal adenocarcinoma predicts short-term relapse of node-negative patients and poor overall survival of patients with non-metastatic disease. Clin. Chem. Lab. Med. 2018, 56, 990–1000. [Google Scholar] [CrossRef] [PubMed]
- Cronin, K.A.; Scott, S.; Firth, A.U.; Sung, H.; Henley, S.J.; Sherman, R.L.; Siegel, R.L.; Anderson, R.N.; Kohler, B.A.; Benard, V.B.; et al. Annual report to the nation on the status of cancer, part 1: National cancer statistics. Cancer 2022, 128, 4251–4284. [Google Scholar] [CrossRef]
- Guinney, J.; Dienstmann, R.; Wang, X.; de Reyniès, A.; Schlicker, A.; Soneson, C.; Marisa, L.; Roepman, P.; Nyamundanda, G.; Angelino, P.; et al. The consensus molecular subtypes of colorectal cancer. Nat. Med. 2015, 21, 1350–1356. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.; Lu, B.; Zhang, J.; Ding, J.; Liu, P.; Lu, Y. tRNA-derived RNA fragments in cancer: Current status and future perspectives. J. Hematol. Oncol. 2020, 13, 121. [Google Scholar] [CrossRef]
- Huang, S.-Q.; Sun, B.; Xiong, Z.-P.; Shu, Y.; Zhou, H.-H.; Zhang, W.; Xiong, J.; Li, Q. The dysregulation of tRNAs and tRNA derivatives in cancer. J. Exp. Clin. Cancer Res. 2018, 37, 101. [Google Scholar] [CrossRef]
- Haussecker, D.; Huang, Y.; Lau, A.; Parameswaran, P.; Fire, A.Z.; Kay, M.A. Human tRNA-derived small RNAs in the global regulation of RNA silencing. RNA 2010, 16, 673–695. [Google Scholar] [CrossRef] [Green Version]
- Ivanov, P.; Emara, M.M.; Villen, J.; Gygi, S.P.; Anderson, P. Angiogenin-induced tRNA fragments inhibit translation initiation. Mol. Cell 2011, 43, 613–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maute, R.L.; Schneider, C.; Sumazin, P.; Holmes, A.; Califano, A.; Basso, K.; Dalla-Favera, R. tRNA-derived microRNA modulates proliferation and the DNA damage response and is down-regulated in B cell lymphoma. Proc. Natl. Acad. Sci. USA 2013, 110, 1404–1409. [Google Scholar] [CrossRef] [PubMed]
- Pekarsky, Y.; Balatti, V.; Palamarchuk, A.; Rizzotto, L.; Veneziano, D.; Nigita, G.; Rassenti, L.Z.; Pass, H.I.; Kipps, T.J.; Liu, C.G.; et al. Dysregulation of a family of short noncoding RNAs, tsRNAs, in human cancer. Proc. Natl. Acad. Sci. USA 2016, 113, 5071–5076. [Google Scholar] [CrossRef]
- Balatti, V.; Pekarsky, Y.; Croce, C.M. Role of the tRNA-Derived Small RNAs in Cancer: New Potential Biomarkers and Target for Therapy. Adv. Cancer Res. 2017, 135, 173–187. [Google Scholar] [CrossRef]
- Katsaraki, K.; Artemaki, P.I.; Papageorgiou, S.G.; Pappa, V.; Scorilas, A.; Kontos, C.K. Identification of a novel, internal tRNA-derived RNA fragment as a new prognostic and screening biomarker in chronic lymphocytic leukemia, using an innovative quantitative real-time PCR assay. Leuk. Res. 2019, 87, 106234. [Google Scholar] [CrossRef] [PubMed]
- Katsaraki, K.; Adamopoulos, P.G.; Papageorgiou, S.G.; Pappa, V.; Scorilas, A.; Kontos, C.K. A 3′ tRNA-derived fragment produced by tRNALeuAAG and tRNALeuTAG is associated with poor prognosis in B-cell chronic lymphocytic leukemia, independently of classical prognostic factors. Eur. J. Haematol. 2021, 106, 821–830. [Google Scholar] [CrossRef]
- Karousi, P.; Papanota, A.-M.; Artemaki, P.I.; Liacos, C.-I.; Patseas, D.; Mavrianou-Koutsoukou, N.; Liosi, A.-A.; Kalioraki, M.-A.; Ntanasis-Stathopoulos, I.; Gavriatopoulou, M.; et al. tRNA Derivatives in Multiple Myeloma: Investigation of the Potential Value of a tRNA-Derived Molecular Signature. Biomedicines 2021, 9, 1811. [Google Scholar] [CrossRef]
- Balatti, V.; Nigita, G.; Veneziano, D.; Drusco, A.; Stein, G.S.; Messier, T.L.; Farina, N.H.; Lian, J.B.; Tomasello, L.; Liu, C.-G.; et al. tsRNA signatures in cancer. Proc. Natl. Acad. Sci. USA 2017, 114, 8071–8076. [Google Scholar] [CrossRef]
- Xiong, W.; Wang, X.; Cai, X.; Xiong, W.; Liu, Y.; Li, C.; Liu, Q.; Qin, J.; Li, Y. Identification of tRNA-derived fragments in colon cancer by comprehensive small RNA sequencing. Oncol. Rep. 2019, 42, 735–744. [Google Scholar] [CrossRef]
- Tsiakanikas, P.; Adamopoulos, P.G.; Tsirba, D.; Artemaki, P.I.; Papadopoulos, I.N.; Kontos, C.K.; Scorilas, A. High Expression of a tRNA(Pro) Derivative Associates with Poor Survival and Independently Predicts Colorectal Cancer Recurrence. Biomedicines 2022, 10, 1120. [Google Scholar] [CrossRef]
- Wu, Y.; Yang, X.; Jiang, G.; Zhang, H.; Ge, L.; Chen, F.; Li, J.; Liu, H.; Wang, H. 5′-tRF-GlyGCC: A tRNA-derived small RNA as a novel biomarker for colorectal cancer diagnosis. Genome. Med. 2021, 13, 20. [Google Scholar] [CrossRef] [PubMed]
- Piawah, S.; Venook, A.P. Targeted therapy for colorectal cancer metastases: A review of current methods of molecularly targeted therapy and the use of tumor biomarkers in the treatment of metastatic colorectal cancer. Cancer 2019, 125, 4139–4147. [Google Scholar] [CrossRef]
- Purcell, R.V.; Schmeier, S.; Lau, Y.C.; Pearson, J.F.; Frizelle, F.A. Molecular subtyping improves prognostication of Stage 2 colorectal cancer. BMC Cancer 2019, 19, 1155. [Google Scholar] [CrossRef] [Green Version]
- Karousi, P.; Artemaki, P.I.; Sotiropoulou, C.D.; Christodoulou, S.; Scorilas, A.; Kontos, C.K. Identification of Two Novel Circular RNAs Deriving from BCL2L12 and Investigation of Their Potential Value as a Molecular Signature in Colorectal Cancer. Int. J. Mol. Sci. 2020, 21, 8867. [Google Scholar] [CrossRef] [PubMed]
- Duran-Sanchon, S.; Herrera-Pariente, C.; Moreira, L. New non-invasive biomarkers for colorectal cancer screening. Rev. Esp. Enferm. Dig. 2020, 112, 642–648. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Number of Patients (%) | |
|---|---|
| Histological grade | |
| I | 26 (12.3%) |
| II | 154 (73.0%) |
| III | 31 (14.7%) |
| T (tumor invasion) | |
| T1 | 9 (4.3%) |
| T2 | 37 (17.5%) |
| T3 | 116 (55.0%) |
| T4 | 49 (23.2%) |
| N (nodal status) | |
| N0 | 123 (58.3%) |
| N1 | 60 (28.4%) |
| N2 | 28 (13.3%) |
| M (distant metastasis) | |
| M0 | 183 (86.7%) |
| M1 | 28 (13.3%) |
| TNM stage | |
| I | 40 (19.0%) |
| II | 77 (36.5%) |
| III | 66 (31.3%) |
| IV | 28 (13.2%) |
| Treatment with radiotherapy (207/211 patients) | |
| No | 165 (79.7%) |
| Yes | 42 (20.3%) |
| Treatment with chemotherapy (207/211 patients) | |
| No | 83 (40.1%) |
| Yes | 124 (59.9%) |
| Variable | Mean ± SEM | Range | Quartiles | ||
|---|---|---|---|---|---|
| 1st | 2nd (Median) | 3rd | |||
| Normalized i-tRF-GlyGCC expression (RQU) | |||||
| in cancerous tissues (n = 211) | 0.44 ± 0.036 | 0.001–3.4 | 0.11 | 0.30 | 0.59 |
| in normal tissues (n = 83) | 0.36 ± 0.031 | 0.002–1.1 | 0.12 | 0.32 | 0.52 |
| Patient age (years) | 65 ± 0.8 | 35–93 | 57 | 66 | 72 |
| Tumor size (cm2) | 19.3 ± 1.1 | 0.8–132 | 9.8 | 14.0 | 24.0 |
| Univariate Analysis (n = 183) | Multivariate Analysis (n = 181) | |||||
|---|---|---|---|---|---|---|
| Covariate | HR 1 | BCa 2 95% CI 3 | p Value 4 | HR 1 | BCa 2 95% CI 3 | p Value 4 |
| i-tRF-GlyGCC expression (high vs. low) | 2.39 | 1.40–4.29 | <0.001 | 2.64 | 1.45–5.33 | 0.004 |
| Tumor size | 0.99 | 0.96–1.00 | 0.13 | |||
| Histological grade (ordinal) | 2.51 | 1.46–4.54 | 0.003 | 2.20 | 1.13–4.80 | 0.027 |
| T (ordinal) | 1.69 | 1.22–2.59 | 0.008 | 1.59 | 0.97–2.81 | 0.065 |
| N (ordinal) | 1.47 | 0.98–2.16 | 0.051 | 1.06 | 0.61–1.78 | 0.82 |
| Treatment with radiotherapy (yes vs. no) | 1.34 | 0.72–2.39 | 0.36 | 0.84 | 0.38–1.61 | 0.60 |
| Treatment with chemotherapy (yes vs. no) | 1.72 | 0.99–3.33 | 0.062 | 1.17 | 0.55–2.50 | 0.69 |
| Univariate Analysis (n = 211) | Multivariate Analysis (n = 207) | |||||
|---|---|---|---|---|---|---|
| Covariate | HR 1 | BCa 2 95% CI 3 | p Value 4 | HR 1 | BCa 2 95% CI 3 | p Value 4 |
| i-tRF-GlyGCC expression (high vs. low) | 1.79 | 1.18–2.68 | 0.003 | 1.56 | 0.98–2.43 | 0.046 |
| Tumor size | 1.00 | 0.99–1.02 | 0.53 | |||
| Histological grade (ordinal) | 1.91 | 1.21–3.04 | 0.008 | 1.24 | 0.73–2.07 | 0.41 |
| T (ordinal) | 1.88 | 1.34–2.74 | 0.002 | 1.42 | 0.93–2.31 | 0.12 |
| N (ordinal) | 1.99 | 1.48–2.75 | <0.001 | 1.46 | 0.96–2.14 | 0.047 |
| M (M1 vs. M0) | 7.17 | 4.13–13.52 | <0.001 | 4.71 | 2.21–12.48 | <0.001 |
| Treatment with radiotherapy (yes vs. no) | 0.94 | 0.53–1.54 | 0.84 | 1.16 | 0.57–2.08 | 0.63 |
| Treatment with chemotherapy (yes vs. no) | 1.15 | 0.75–1.86 | 0.53 | 0.57 | 0.33–0.98 | 0.033 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Christodoulou, S.; Katsaraki, K.; Vassiliu, P.; Danias, N.; Michalopoulos, N.; Tzikos, G.; Sideris, D.C.; Arkadopoulos, N. High Intratumoral i-tRF-GlyGCC Expression Predicts Short-Term Relapse and Poor Overall Survival of Colorectal Cancer Patients, Independent of the TNM Stage. Biomedicines 2023, 11, 1945. https://doi.org/10.3390/biomedicines11071945
Christodoulou S, Katsaraki K, Vassiliu P, Danias N, Michalopoulos N, Tzikos G, Sideris DC, Arkadopoulos N. High Intratumoral i-tRF-GlyGCC Expression Predicts Short-Term Relapse and Poor Overall Survival of Colorectal Cancer Patients, Independent of the TNM Stage. Biomedicines. 2023; 11(7):1945. https://doi.org/10.3390/biomedicines11071945
Chicago/Turabian StyleChristodoulou, Spyridon, Katerina Katsaraki, Panteleimon Vassiliu, Nikolaos Danias, Nikolaos Michalopoulos, Georgios Tzikos, Diamantis C. Sideris, and Nikolaos Arkadopoulos. 2023. "High Intratumoral i-tRF-GlyGCC Expression Predicts Short-Term Relapse and Poor Overall Survival of Colorectal Cancer Patients, Independent of the TNM Stage" Biomedicines 11, no. 7: 1945. https://doi.org/10.3390/biomedicines11071945