
Cannabis for the Treatment of Fibromyalgia: A Systematic Review
 , , and
, , and
Abstract
:1. Introduction
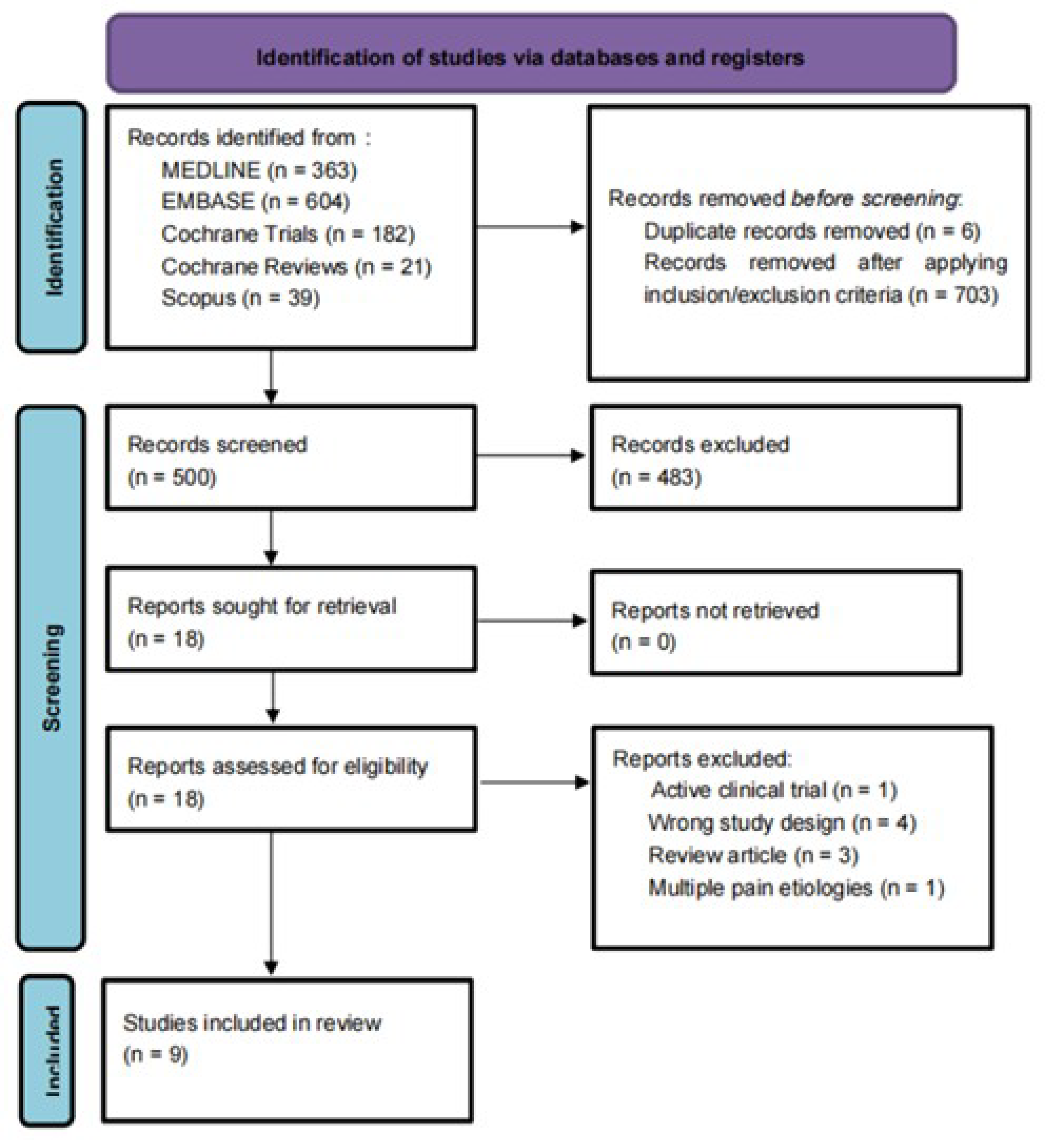
2. Methods
3. Results
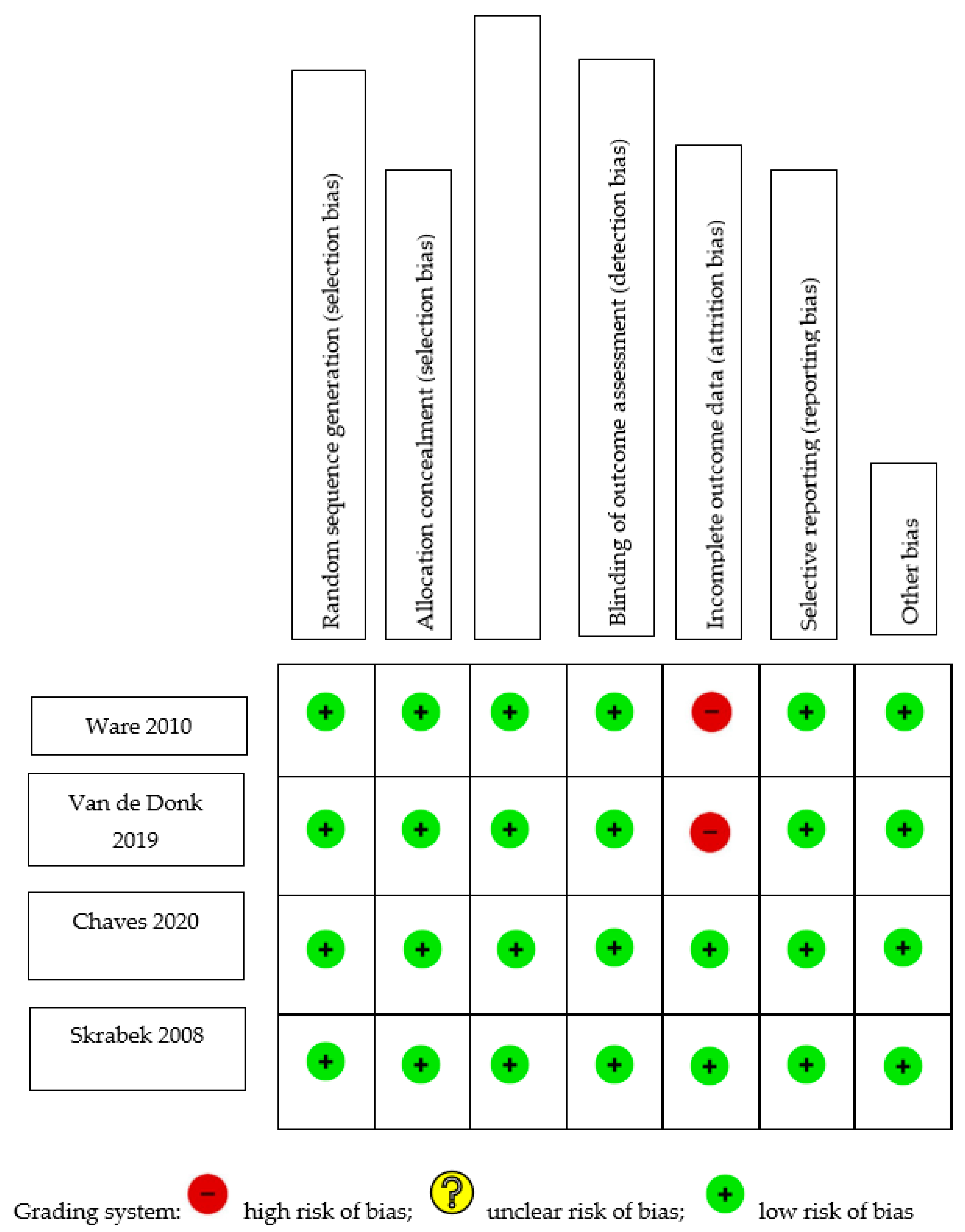
Quality Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CBT | Cognitive behavioral therapy |
| THC | Delta-9- tetrahydrocannabinol |
| CBD | Cannabidiol |
| CB1 | Type 1 cannabinoid receptor |
| CB2 | Type 2 cannabinoid receptor |
| FDA | Food and Drug Administration |
References
- Clauw, D.J. Fibromyalgia: A clinical review. JAMA 2014, 311, 1547–1555. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sluka, K.A.; Clauw, D.J. Neurobiology of fibromyalgia and chronic widespread pain. Neuroscience 2016, 338, 114–129. [Google Scholar] [CrossRef] [Green Version]
- Berger, A.; Dukes, E.; Martin, S.; Edelsberg, J.; Oster, G. Characteristics and healthcare costs of patients with fibromyalgia syndrome. Int. J. Clin. Pract. 2007, 61, 1498–1508. [Google Scholar] [CrossRef] [Green Version]
- Mascarenhas, R.O.; Souza, M.B.; Oliveira, M.X.; Lacerda, A.C.; Mendonça, V.A.; Henschke, N.; Oliveira, V.C. Association of Therapies with Reduced Pain and Improved Quality of Life in Patients With Fibromyalgia: A Systematic Review and Meta-analysis. JAMA Intern. Med. 2021, 181, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Savage, S.R.; Romero-Sandoval, A.; Schatman, M.; Wallace, M.; Fanciullo, G.; Mccarberg, B.; Warell, M. Cannabis in Pain Treatment: Clinical and Research Considerations. J. Pain 2016, 17, 654–668. [Google Scholar] [CrossRef] [PubMed]
- Ebbert, J.O.; Scharf, E.L.; Hurt, R.T. Medical Cannabis. Mayo Clin. Proc. 2018, 93, 1842–1847. [Google Scholar] [CrossRef] [Green Version]
- Levinsohn, E.A.; Hill, K.P. Clinical uses of cannabis and cannabinoids in the United States. J. Neurol. Sci. 2020, 411, 116717. [Google Scholar] [CrossRef] [Green Version]
- Yadav, V.; Bever, C., Jr.; Bowen, J.; Bowling, A.; Weinstock-Guttman, B.; Cameron, M.H.; Bourdette, D.; Gronseth, G.S.; Narayanaswami, P. Summary of evidence-based guideline: Complementary and alternative medicine in multiple sclerosis: Report of the guideline development subcommittee of the American Academy of Neurology. Neurology 2014, 82, 1083–1092. [Google Scholar] [CrossRef] [Green Version]
- Uberall, M.A. A Review of Scientific Evidence for THC:CBD Oromucosal Spray (Nabiximols) in the Management of Chronic Pain. J. Pain Res. 2020, 13, 399–410. [Google Scholar] [CrossRef] [Green Version]
- Fiz, J.; Duran, M.; Capella, D.; Carbonell, J.; Farré, M. Cannabis use in patients with fibromyalgia: Effect on symptoms relief and health-related quality of life. PLoS ONE 2011, 6, e18440. [Google Scholar] [CrossRef] [Green Version]
- Yassin, M.; Oron, A.; Robinson, D. Effect of adding medical cannabis to analgesic treatment in patients with low back pain related to fibromyalgia: An observational cross-over single centre study. Clin. Exp. Rheumatol. 2019, 37 (Suppl. S116), 13–20. [Google Scholar] [CrossRef] [PubMed]
- Habib, G.; Artul, S. Medical Cannabis for the Treatment of Fibromyalgia. J. Clin. Rheumatol. 2018, 24, 255–258. [Google Scholar] [CrossRef]
- Sagy, I.; Bar-Lev Schleider, L.; Abu-Shakra, M.; Novack, V. Safety and Efficacy of Medical Cannabis in Fibromyalgia. J. Clin. Med. 2019, 8, 807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hershkovich, O.; Hayun, Y.; Oscar, N.; Shtein, A.; Lotan, R. The role of cannabis in treatment-resistant fibromyalgia women. Pain Pract. 2023, 23, 180–184. [Google Scholar] [CrossRef]
- Ware, M.A.; Fitzcharles, M.A.; Joseph, L.; Shir, Y. The effects of nabilone on sleep in fibromyalgia: Results of a randomized controlled trial. Anesth. Analg. 2010, 110, 604–610. [Google Scholar] [CrossRef]
- van de Donk, T.; Niesters, M.; Kowal, M.A.; Olofsen, E.; Dahan, A.; van Velzen, M. An experimental randomized study on the analgesic effects of pharmaceutical-grade cannabis in chronic pain patients with fibromyalgia. Pain 2019, 160, 860–869. [Google Scholar] [CrossRef]
- Chaves, C.; Bittencourt, P.C.T.; Pelegrini, A. Ingestion of a THC-Rich Cannabis Oil in People with Fibromyalgia: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Pain Med. 2020, 21, 2212–2218. [Google Scholar] [CrossRef]
- Skrabek, R.Q.; Galimova, L.; Ethans, K.; Perry, D. Nabilone for the treatment of pain in fibromyalgia. J. Pain 2008, 9, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Kogan, N.M.; Mechoulam, R. Cannabinoids in health and disease. Dialogues Clin. Neurosci. 2007, 9, 413–430. [Google Scholar] [CrossRef] [PubMed]
- Vuckovic, S.; Srebro, D.; Vujovic, K.S.; Vučetić, Č.; Prostran, M. Cannabinoids and Pain: New Insights from Old Molecules. Front. Pharmacol. 2018, 9, 1259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schilling, J.M.; Hughes, C.G.; Wallace, M.S.; Sexton, M.; Backonja, M.; Moeller-Bertram, T. Cannabidiol as a Treatment for Chronic Pain: A Survey of Patients’ Perspectives and Attitudes. J. Pain Res. 2021, 14, 1241–1250. [Google Scholar] [CrossRef] [PubMed]
- Capano, A.; Weaver, R.; Burkman, E. Evaluation of the effects of CBD hemp extract on opioid use and quality of life indicators in chronic pain patients: A prospective cohort study. Postgrad. Med. 2020, 132, 56–61. [Google Scholar] [CrossRef] [Green Version]
- Nabilone. Drug Bank Online 2005. Retrieved 6 April 2023. Available online: https://go.drugbank.com/drugs/DB00486 (accessed on 5 April 2023).
- Rehabilitation and Fibromyalgia. Medscape. Retrieved 6 April 2023. Available online: https://emedicine.medscape.com/article/312778-overview (accessed on 5 February 2019).
- Whiting, P.F.; Wolff, R.F.; Deshpande, S.; Di Nisio, M.; Duffy, S.; Hernandez, A.V.; Keurentjes, J.C.; Lang, S.; Misso, K.; Ryder, S.; et al. Cannabinoids for Medical Use: A Systematic Review and Meta-analysis. JAMA 2015, 313, 2456–2473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attal, N.; Bouhassira, D. Pharmacotherapy of neuropathic pain: Which drugs, which treatment algorithms? Pain 2015, 156 (Suppl. S1), S104–S114. [Google Scholar] [CrossRef] [Green Version]
- Smith, L.A.; Azariah, F.; Lavender, V.T.; Stoner, N.S.; Bettiol, S. Cannabinoids for nausea and vomiting in adults with cancer receiving chemotherapy. Cochrane Database Syst. Rev. 2015, 2015, CD009464. [Google Scholar]
- Sexton, M.; Cuttler, C.; Finnell, J.S.; Mischley, L.K. A Cross-Sectional Survey of Medical Cannabis Users: Patterns of Use and Perceived Efficacy. Cannabis Cannabinoid Res. 2016, 1, 131–138. [Google Scholar] [CrossRef] [Green Version]
- Corchero, J.; Manzanares, J.; Fuentes, J.A. Cannabinoid/opioid crosstalk in the central nervous system. Crit. Rev. Neurobiol. 2004, 16, 159–172. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author | Year | Selection | Comparability | Outcome |
|---|---|---|---|---|
| Cannabis in Fibromyalgia Studies | ||||
| Fiz et al. [11] | 2011 | * | * | * |
| Yassin et al. [12] | 2019 | *** | - | ** |
| Habib et al. [13] | 2018 | * | - | * |
| Sagy et al. [14] | 2019 | *** | - | ** |
| Hershkovich et al. [15] | 2023 | *** | - | * |
| Certainty Assessment | Impact | Certainty | ||||||
|---|---|---|---|---|---|---|---|---|
| № of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | ||
| Fibromyalgia Impact Questionnaire (FIQ) Score | ||||||||
| 4 | 2 RCTs and 3 observational studies | Not serious | Serious a | Not serious | Not serious | Three out of the four studies reported reductions in FIQ score. Average score reductions ranged from −12.07 to −45 points. | ⨁⨁◯◯ Low | |
| Visual Analog Scale (VAS) for Acute and Chronic Pain | ||||||||
| 2 | 2 RCTs and 2 observational studies | Not serious | Not serious | Not serious | Not serious | Dose–response b | All four studies reported a reduction in pain score ranging from −2.04 to −4.8 cm. | ⨁⨁⨁◯ Moderate |
| Lower-Back Pain | ||||||||
| 1 | RCT | Not serious | Serious c | Not serious | Not serious | Strong association | Greater decrease in lower-back pain | ⨁⨁⨁◯ Moderate |
| Number of Tender Points | ||||||||
| 1 | RCT | Not serious | Not serious | Not serious | Not serious | Strong association | No significant decrease in number of tender points | ⨁⨁⨁⨁ High |
| Study Title | Study | Study Design | Diagnostic Criteria | Inclusion Criteria | FM Group | Control Group | # of all Study Patients | Median Age | Gender Distribution | Co-Morbidities | Exclusion Criteria | Intervention | Route of Administration | Follow-Up Length | Concurrent Therapies | Primary Outcome | Secondary Outcomes | Outcomes | Conclusions |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Nabilone for the Treatment of Pain in Fibromyalgia | Skrabek et al. (2008) [19] | RCT, parallel | 1990 ACR | 18–70 years old with FM, pain despite oral medications; no prior use of oral cannabinoids for pain management | Nabilone | Placebo with four-week washout period | 40 randomized (20 per group), 33 completed (15 intervention, 18 control) | Mean of study group: 47.6 (9.13); mean of control group: 50.11 (5.96) | NR | NR | Heart disease; schizophrenia or other psychotic disorder; severe liver dysfunction; untreated nonpsychotic emotional disorders; cognitive impairment; major illness in another organ system | 0.5 mg nabilone PO at bedtime × 1 week, increased to 0.5 mg BID after 1 week, and uptitration to max dose of 1 mg BID. | Oral | 2-week visit, 4-week visit, and 8-week visit after a 4-week washout period | None specified, but patients were allowed to continue using adjunctive therapies for pain treatment during the study | VAS at 2 and 4 weeks: significant decrease at 4 weeks (2.04, p < 0.02) | Number of tender points, average tender point pain threshold, Fibromyalgia Impact Questionnaire at 2 and 4 weeks | There were significant decreases in the VAS (2.04, p < 0.02), FIQ (12.07, p < 0.02) and anxiety (1.67, p < 0.02) in the nabilone group at 4 weeks. No significant improvements in the placebo group. More side effects in nabilone group at 2 and 4 weeks (1.58, p < 0.02 and 1.54, p < 0.05) | Nabilone is a beneficial, tolerable treatment option for fibromyalgia patients, with benefit sin pain relief and functional improvement |
| The Effects of Nabilone on Sleep in Fibromyalgia: Results of a Randomized Controlled Trial | Ware et al. (2010) [16] | RCT, cross-over | 1990 ACR | 18+ years old, adult men and non-pregnant women with FM1 and self-reported chronic insomnia. Twenty subjects remained on stable analgesic therapy with negative urine screening for cannabinoids at the baseline visit. Subjects who were using a cannabinoid or amitriptyline at screening underwent a 2-week washout period before entering the study | Nabilone | Amitriptyline 10–20 mg × 2 week with 2-week washout period | 32 randomized, 29 completed | 49.5 (11.2) | 26 F, 5 M, 1 missing data | NR | Cancer pain, unstable cardiac disease, psychotic disorder, schizophrenia, recent manic episode (within the past year), seizure disorder, glaucoma, urinary retention, hypersensitivity to cannabinoids, amitriptyline, or related tricyclic antidepressants, or were taking monoamine oxidase inhibitors | Crossover study comparing nabilone 0.5–1.0 mg for 2 weeks with 2-week washout period with amitriptyline 10–20 mg as an active control. Patients received one of either drug for two weeks, followed by a two-week washout period, and then started the second drug | Oral | 10-week study (initial washout period for previous cannabinoid/tricyclic use, two weeks of one drug, intervening washout period, two weeks of second drug, final washout). Data collected every two-week period | 20 subjects were on stable analgesic therapy but had to be negative for cannabinoid use at baseline | Quality of sleep (Insomnia Severity Index and Leeds Sleep Evaluation Questionnaire) | Pain, mood, QOL, global satisfaction with treatment, AEs | Nabilone was superior to amitriptyline (Insomnia Severity Index difference 3.2; 95% confidence interval 1.2–5.3). Nabilone was marginally better for restfulness (Leeds Sleep Evaluation Questionnaire difference 0.5 [0.0–1.0]) but not for wakefulness (difference 0.3 [0.2 to 0.8]). No effects on pain, mood, or QOL were observed. AEs were mostly mild–moderate and were more frequent with nabilone. The most common AEs for nabilone were dizziness, nausea, and dry mouth | Nabilone is well tolerated and effective in improving sleep in patients with FM. Low-dose nabilone given once daily at bedtime may be considered as an alternative to amitriptyline. Longer trials are needed to determine the duration of effect and to characterize long-term safety |
| Cannabis Use in Patients with Fibromyalgia: Effect on Symptoms Relief and Health-Related Quality of Life | Fiz et al. (2011) [11] | OBS, cross-sectional | 1990 ACR | 18+ years old with moderate–severe FM symptomatology and resistance to pharmacological treatment | Cannabis | 56 (28 THC users, 28 non-users) | 50 (11.9) | 53 females (26 users, 27 non-users) 3 males (2 users, 1 non-user) | NR | Severe illness and history of abuse or dependence for cannabis or other psychoactive substances | Observational study comparing survey responses of cannabis users and nonusers on perceived benefits of cannabis use, adverse effects, and quality of life | Oral (54%), smoked (46%), and combined (43%) | Concurrent therapies used but no significant differences between THC users and non-users | Quality of life (Fibromyalgia Impact Questionnaire and short-form health survey) | Sleep (Pittsburgh sleep quality index) and perceived benefits of cannabis (VAS) | After 2 h of cannabis use, VAS scores showed a statistically significant (p = 0.001) reduction in pain and stiffness, enhancement of relaxation, and an increase in somnolence and feeling of wellbeing. Mental health component summary score of the SF-36 was significantly higher (p = 0.05) in cannabis users than in non-users. No significant differences were found in the other SF-36 domains, in the FIQ, or in the PSQI | The use of cannabis was associated with beneficial effects on some FM symptoms | ||
| An experimental randomized study on the analgesic effects of pharmaceutical-grade cannabis in chronic pain patients with fibromyalgia | Van de Donk et al. (2019) [17] | RCT, cross-over | 2010 ACR | 18+-year-old females with FM, pain score ≥ 5 for most of the day (pain scale from 0 = no pain to 10 = max) | Each of the subjects tried all 4 substances, including placebo | 20 | 39 (13) | NR | NR | Age < 18 years old, any medical, neurological, or psychiatric illness, use of strong opioids or other painkillers except paracetamol and/or ibuprofen, benzodiazepine use, any known allergies to study medication, illicit drug or alcohol use, recent use of cannabis, pregnancy, breastfeeding, and the presence of pain syndromes other than FM | Patients visited the research unit on 5 occasions. On first visit, the patients were screened and familiarized with the experimental setup. On each of their next visits, the patients received 1 of 4 possible cannabis treatments (in a random order), with at least 2 weeks between visits. These were Bedrocan (22.4 mg THC, <1 mg CBD; Bedrocan International BV, Veendam, the Netherlands), Bediol (13.4 mg THC, 17.8 mg CBD; Bedrocan International BV, Veendam, the Netherlands), Bedrolite (18.4 mg CBD, <1 mg THC; Bedrocan International BV, Veendam, the Netherlands), and a placebo variety without any THC or CBD | Inhaled vapor from balloon | Visits every 2 weeks | Not reported | Relief of experimental pressure pain, electrical pain, and spontaneous pain (VAS) | Plasma concentrations and drug high (Bowdle questionnaire) | No treatment had an effect greater than that of the placebo on spontaneous or electrical pain responses. More subjects receiving Bediol had a 30% decrease in pain scores compared to the placebo (90% vs. 55% of patients, p = 0.01), with spontaneous pain scores correlating with the magnitude of drug high (ρ = −0.5, p < 0.001). Cannabis treatments containing THC caused a significant increase in pressure pain threshold relative to the placebo (p < 0.01). Cannabidiol inhalation increased THC plasma concentrations but diminished THC-induced analgesic effects | None of the treatments were effective in reducing spontaneous pain scores more than the placebo. Further studies are needed to assess efficacy and safety in clinical trials with prolonged treatment periods | |
| Effect of adding medical cannabis to analgesic treatment in patients with low back pain related to fibromyalgia: an observational cross-over single centre study. Clin Exp Rheumatol. 2019 Jan-Feb;37 Suppl 116(1):13–20. | Yassin et al. (2019) [12] | OBS, crossover | Not reported | Symptomatic FM for at least 12 months, symptomatic LBP of more than 12 months between T12 and the gluteal fold, failure of opiate therapy for at least 12 months | N/A | N/A | 31 | 33.4 (12.3) | Not reported | NR | Malignancy, improvement in pain to VAS < 4 after opiate therapy, refusal to undergo medication with duloxetine and opiates, inability to sign an informed consent form, severe cardiovascular disease preventing cannabis administration according to a cardiologist, severe psychiatric disease preventing cannabis administration according to a psychiatrist | 3 months of standardized analgesic therapy: 5 mg of oxycodone hydrochloride and 2.5 mg of naloxone hydrochloride twice a day, and duloxetine 30 mg once a day. Following 3 months of this therapy, the patients could opt for medical cannabis (20 g per month) and were treated for a minimum of 6 months | Inhaled (smoking or vaporization) | 3- and 6-month follow-up after start of medical cannabis therapy | Oxycodone 5 mg and duloxetine 30 mg | FIQR, VAS, ODI, SF-12, and lumbar range of motion using the modified Schober test | Analgesic drug use was assessed according to the patients’ medical records, including the list of pharmacy-dispensed medications | Medical cannabis therapy allowed a significantly higher improvement in all patient-reported outcomes at 3 months after initiation of medical cannabis, and the improvement was maintained at 6 months. ROM improved after 3 months of medical cannabis therapy and continued to improve at 6 months | Supplementation of analgesic therapy with medical cannabis therapy can alleviate pain in FM patients suffering from LBP |
| Safety and Efficacy of Medical Cannabis in Fibromyalgia. J Clin Med. 2019 Jun 5;8(6) | Sagy et al. (2019) [14] | OBS | 2010 ACR | FM who initiated treatment with medical cannabis from January 2015 to December 2017 | N/A | N/A | 367 | 52.9 (8.3) | 301 (82%) | Cigarette smokers (37.3%), cancer (9.5%), PTSD (6%) | NR | Low dose of cannabis (e.g., a drop of 15% THC-rich cannabis TID) with gradual increase (e.g., a single drop per day) until they achieved a therapeutic effect (e.g., subjective relief of their pain, significant improvement in their QOL). In case of inflorescence (each cigarette contained 0.75 g of cannabis), patients were instructed to use one breath every 3–4 h, and to increase the amount gradually in this interval until a therapeutic effect was achieved. | Oil, inflorescence (i.e., smoke), or both | 6-Month follow-up | Not reported | Treatment response defined as at least moderate or significant improvement in a patient’s condition at 6-month follow-up | Pain intensity—(NRS) Quality of life—global assessment by the patient using the Likert scale, with five options: very good, good, neither good nor bad, bad, or very bad. Perception of the general effect of cannabis—global assessment by using a Likert scale with seven options: significant improvement, moderate improvement, slight improvement, no change, slight deterioration, moderate deterioration, or significant deterioration | Pain intensity (scale 0–10) reduced from a median of 9.0 at baseline to 5.0 (p < 0.001), and 194 patients (81.1%) achieved a treatment response. In a multivariate analysis, age above 60 years (odds ratio (OR) 0.34, 95% C.I 0.16–0.72), concerns about cannabis treatment (OR 0.36, 95% C.I 0.16–0.80), spasticity (OR 2.26, 95% C.I 1.08–4.72), and previous use of cannabis (OR 2.46 95% C.I 1.06–5.74) were associated with treatment outcomes. The most common adverse effects were dizziness (7.9%), dry mouth (6.7%), and gastrointestinal symptoms (5.4%) | Medical cannabis appears to be a safe and effective alternative for the treatment of fibromyalgia symptoms |
| Ingestion of a THC-Rich Cannabis Oil in People with Fibromyalgia: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Pain Med. 2020 | Chaves et al. (2020) [18] | RCT, parallel | 2010 ACR | >18 years old with moderate-to-severe FM symptoms (presenting functional limitation in everyday activities) despite therapies in use, at least one medical or nursing consultation at the health center in the last year | THC-rich cannabis oil | Olive oil | 18 | 51.9 (9.8) | All F | NR | Decompensated organic comorbidities and/or risk of psychiatric conditions (schizophrenia, psychosis, severe personality disorder, current suicidal ideation), another well-defined cause of chronic pain, current pregnancy/lactation, moderate or severe cognitive impairment, and history of cannabinoid sensitivity | The cannabis group received a 30 mL green glass dropper bottle containing cannabis oil (olive oil extraction) of the White Widow variety, at a 24.44 mg/mL concentration of THC and 0.51 mg/mL of CBD—at a proportion of ∼48/1 THC/CBD, along with small quantities of other cannabinoids such as cannabigerol, tetrahydrocannabivarin, cannabinol, and cannabicromen. The initial dose in both groups was one drop (∼1.2 mg of THC and 0.02 mg of CBD) per day sublingually. Participants in both groups were seen at baseline and every 10 days for eight weeks. Dose increases respected the maximum of one drop for each evaluation moment. At each visit, patients filled out the Fibromyalgia Impact Questionnaire (FIQ) | Oral (Oil) | Participants in both groups were seen at baseline and every 10 days for 8 weeks. | Participants in the cannabis group had previously used antidepressants (62.5%), opioids (25%), and benzodiazepines (12.5%). In the placebo group, the rates of the same classes of medications use were 67%, 33%, and 11%, respectively. Patients self-medicated with mild analgesics and anti-inflammatory pills whenever necessary in both groups | Physical function, work status, wellbeing, and associated physical and mental symptoms in FM patients (FIQ) | Clinical and adverse effects | There were no significant differences in baseline FIQ scores between groups. The cannabis group presented a significant decrease in FIQ score in comparison with the placebo group (p = 0.005) and in comparison with the cannabis group’s baseline score when compared to post-intervention. (p < 0.001). The cannabis group presented significant improvements in the “feel good”, “pain”, “do work”, and “fatigue” scores. The placebo group presented significant improvements in “depression” score after the intervention. There were no severe adverse effects | Phytocannabinoids can be an economically feasible and well-tolerated therapy to reduce symptoms and increase the quality of life of patients with fibromyalgia |
| Study | Study Design | Intervention | Outcomes | Conclusions |
|---|---|---|---|---|
| Skrabek et al. (2008) [19] | RCT, parallel | Nabilone vs. placebo | Compared to placebo, the nabilone group demonstrated decreases in the VAS (2.04, p < 0.02), FIQ (12.07, p < 0.02), and anxiety (1.67, p < 0.02) at 4 weeks. More side effects were noted in the nabilone group at 2 and 4 weeks, with no major improvements measured in the placebo group | Nabilone is a well-tolerated treatment option for patients with fibromyalgia, with demonstrated benefits in pain relief and functional improvements in quality of life and anxiety |
| Ware et al. (2010) [16] | RCT, crossover | Nabilone vs. amitriptyline | Though both amitriptyline and nabilone were effective in improving sleep, nabilone proved superior to amitriptyline (Insomnia Severity Index difference 3.2; 95% confidence interval 1.2–5.3). Nabilone was rated better for restfulness (Leeds Sleep Evaluation Questionnaire difference 0.5 [0.0–1.0]), but not for wakefulness (0.3 [0.2 to 0.8]). No effects on pain, mood, or QOL were observed. Side effects were mostly mild–moderate and were more frequent with nabilone, with the most common symptoms being dizziness, nausea, and dry mouth | Nabilone is well tolerated in patients that have fibromyalgia and can improve their sleep. Low-dose nabilone at bedtime may prove an effective alternative to amitriptyline for sleep management in this population |
| Fiz et al. (2011) [11] | OBS, cross-sectional | Survey of cannabis users vs. non-users | Two hours following cannabis consumption, measured outcomes indicated a statistically significant (p = 0.001) improvement in subjects’ reported pain and stiffness, relaxation, and increased somnolence and feeling of wellbeing. Additionally, the mental health component of the SF-36 was significantly higher (p = 0.05) in cannabis users than in non-users | Cannabis use was associated with improvements in some fibromyalgia symptoms, including pain, feelings of wellbeing and relaxation, and mental health scores |
| Van de Donk et al. (2019) [17] | RCT, crossover | Inhaled THC/CBD combo vs. placebo | None of the treatment modalities impacted spontaneous or electrical pain responses when compared to the placebo. Cannabis varieties that contained THC resulted in a significant increase in subjects’ pain threshold for pressure when compared to the placebo (p < 0.01). Though inhalation of cannabidiol was noted to increase THC plasma concentrations, the analgesic effects associated with THC were found to be diminished in this route of administration | Analgesic benefits were limited to cannabis varieties containing THC and were observed exclusively in the evoked pressure pain model. None of the different treatments in this study were better than the placebo in improving spontaneous pain scores |
| Yassin et al. (2019) [12] | OBS, crossover | Inhaled cannabis vs. oxycodone/naloxone/duloxetine | While standard analgesic therapy showed modest improvements in scores when compared to baseline, the addition of medical cannabis resulted in a significantly higher improvement in all patient-reported outcomes at 3 months. This observed improvement was maintained at 6 months. Range of motion improved after 3 months of cannabis therapy and showed continued improvement at 6 months | Adjunct treatment with medical cannabis therapy in combination with other analgesics can alleviate lower-back pain in patients suffering from fibromyalgia |
| Sagy et al. (2019) [14] | OBS | Cannabis (oil, smoke, or both) | Pain was reduced from a baseline median of 9.0 to 5.0 (p < 0.001); 81.1% of patients achieved a treatment response. Factors associated with treatment outcomes included age over 60 years (odds ratio (OR) 0.34, 95% C.I 0.16–0.72), spasticity (OR 2.26, 95% C.I 1.08–4.72), concerns about cannabis treatment (OR 0.36, 95% C.I 0.16–0.80), and previous cannabis use (OR 2.46 95% C.I 1.06–5.74). The most common adverse effects were mild, including dizziness, dry mouth, and GI symptoms | Cannabis was found to be a well-tolerated and effective treatment modality for fibromyalgia symptoms. |
| Chaves et al. (2020) [18] | RCT, parallel | THC-rich cannabis oil vs. olive oil | There were no significant differences in baseline FIQ score between the groups at the beginning of the study. After the intervention, the cannabis oil group experienced a significant decrease in FIQ score relative to the olive-oil placebo (p = 0.005), as well as when compared with their own baseline score (p < 0.001). The cannabis group reported significant improvements in the “feel good”, “pain”, “do work”, and “fatigue” scores. The placebo group reported significant improvements in the “depression” score following the intervention. No major adverse effects were observed | Phytocannabinoids can be a low-cost therapy option with minimal adverse effects to alleviate symptoms and increase the quality of life in patients experiencing fibromyalgia |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strand, N.H.; Maloney, J.; Kraus, M.; Wie, C.; Turkiewicz, M.; Gomez, D.A.; Adeleye, O.; Harbell, M.W. Cannabis for the Treatment of Fibromyalgia: A Systematic Review. Biomedicines 2023, 11, 1621. https://doi.org/10.3390/biomedicines11061621
Strand NH, Maloney J, Kraus M, Wie C, Turkiewicz M, Gomez DA, Adeleye O, Harbell MW. Cannabis for the Treatment of Fibromyalgia: A Systematic Review. Biomedicines. 2023; 11(6):1621. https://doi.org/10.3390/biomedicines11061621
Chicago/Turabian StyleStrand, Natalie H., Jillian Maloney, Molly Kraus, Christopher Wie, Michal Turkiewicz, Diego A. Gomez, Olufunmilola Adeleye, and Monica W. Harbell. 2023. "Cannabis for the Treatment of Fibromyalgia: A Systematic Review" Biomedicines 11, no. 6: 1621. https://doi.org/10.3390/biomedicines11061621