
Do Vedolizumab trough Levels Predict the Outcome of Subsequent Therapy in Inflammatory Bowel Disease?
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Measurement of Vedolizumab Concentrations
2.3. Determination of Anti-Vedolizumab Antibody Concentration
2.4. Clinical and Endoscopic Scores
2.5. Statistical Analysis
3. Results
3.1. Vedolizumab and Subsequent Therapy
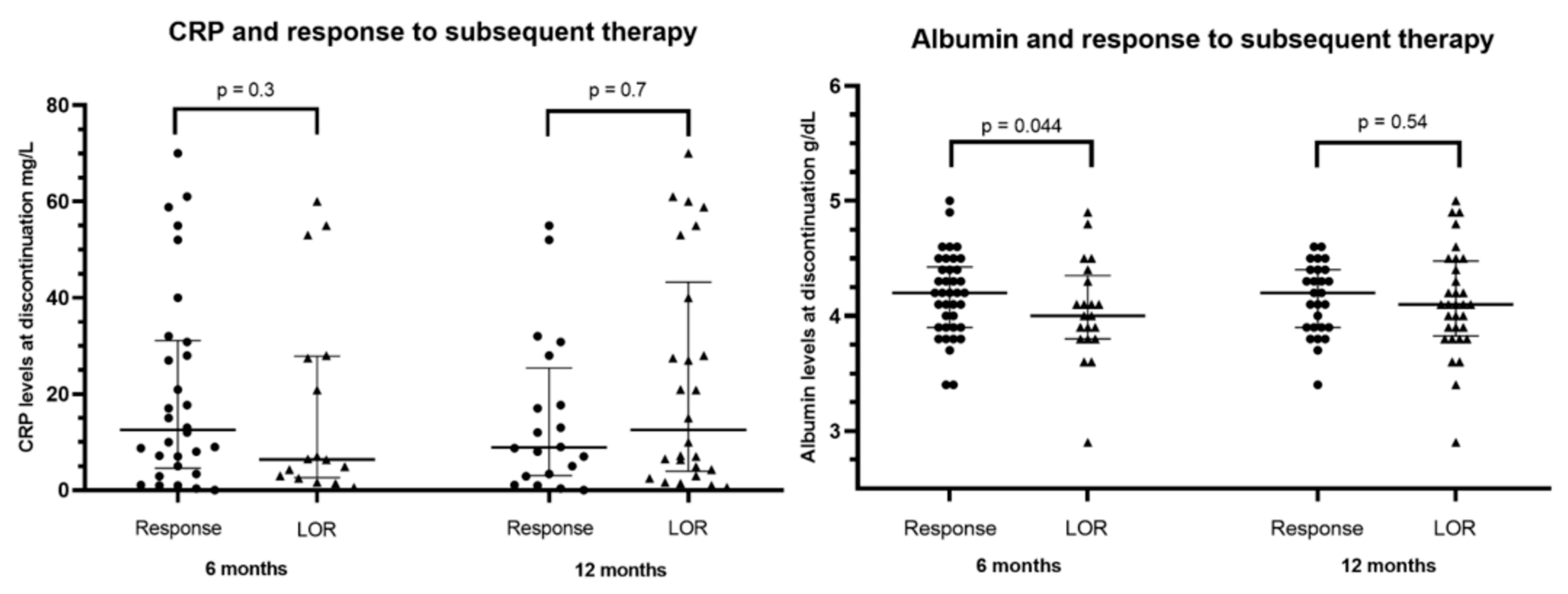
3.2. Outcome of Subsequent Medical (Non-Surgical) Therapy
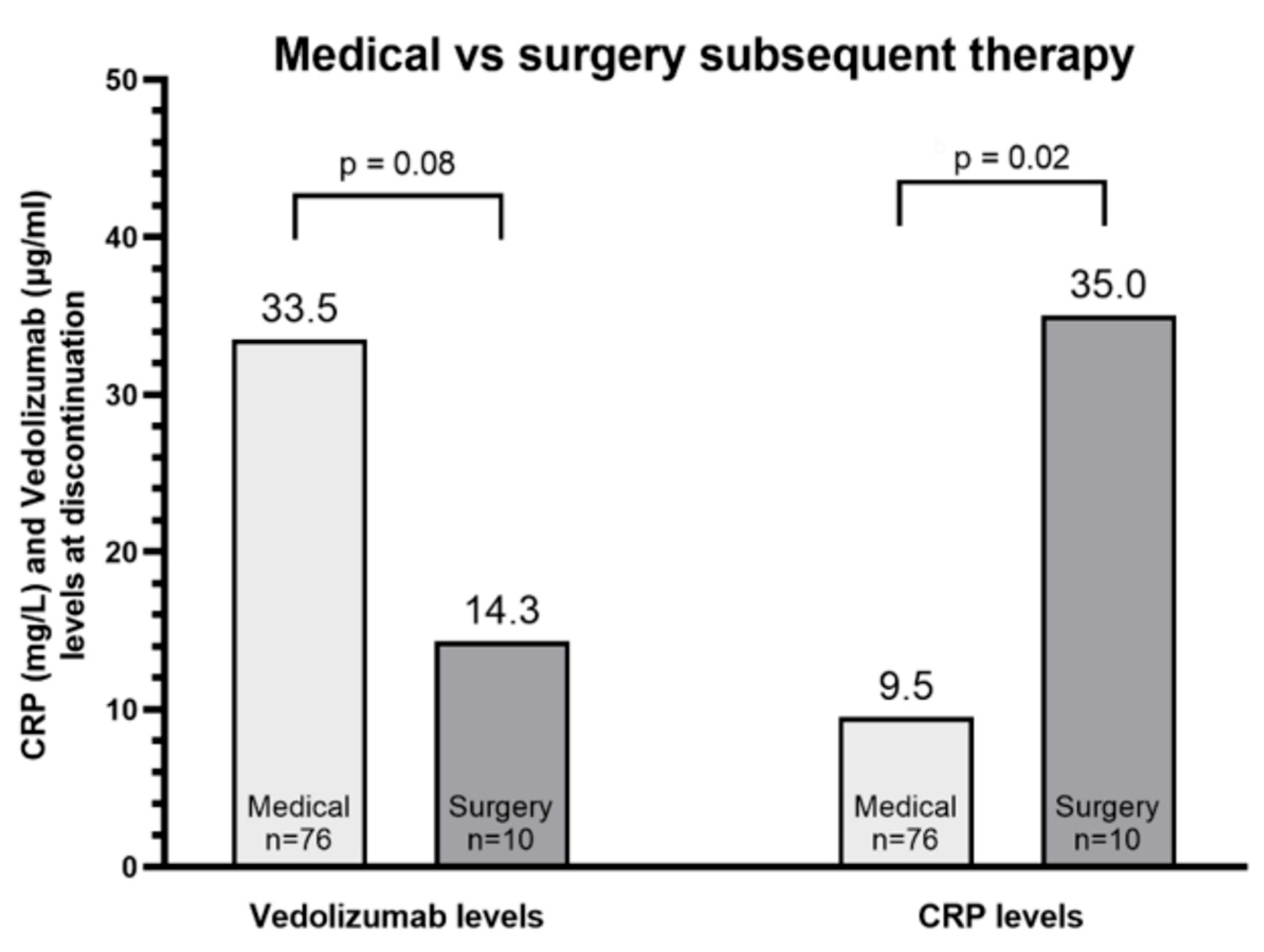
3.3. Subsequent Surgical Therapy
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feagan, B.G.; Rutgeerts, P.; Sands, B.E.; Hanauer, S.; Colombel, J.-F.; Sandborn, W.J.; Van Assche, G.; Axler, J.; Kim, H.-J.; Danese, S.; et al. Vedolizumab as Induction and Maintenance Therapy for Ulcerative Colitis. N. Engl. J. Med. 2013, 369, 699–710. [Google Scholar] [CrossRef] [PubMed]
- Sandborn, W.J.; Feagan, B.G.; Rutgeerts, P.; Hanauer, S.; Colombel, J.F.; Sands, B.E.; Lukas, M.; Fedorak, R.N.; Lee, S.; Bressler, B.; et al. Vedolizumab as induction and maintenance therapy for Crohn’s disease: Commentary. Inflamm. Bowel Dis. Monit. 2014, 14, 55–56. [Google Scholar] [CrossRef] [PubMed]
- Rosario, M.; French, J.L.; Dirks, N.L.; Sankoh, S.; Parikh, A.; Yang, H.; Danese, S.; Colombel, J.-F.; Smyth, M.; Sandborn, W.J.; et al. Exposure–efficacy Relationships for Vedolizumab Induction Therapy in Patients with Ulcerative Colitis or Crohn’s Disease. J. Crohn’s Colitis 2017, 11, 921–929. [Google Scholar] [CrossRef]
- Vermeire, S.; Loftus, E.V., Jr.; Colombel, J.-F.; Feagan, B.G.; Sandborn, W.J.; Sands, B.E.; Danese, S.; D’Haens, G.R.; Kaser, A.; Panaccione, R.; et al. Long-term Efficacy of Vedolizumab for Crohn’s Disease. J. Crohn’s Colitis 2017, 11, 412–424. [Google Scholar] [CrossRef]
- Loftus, E.V., Jr.; Colombel, J.-F.; Feagan, B.G.; Vermeire, S.; Sandborn, W.J.; Sands, B.E.; Danese, S.; D’Haens, G.R.; Kaser, A.; Panaccione, R.; et al. Long-term Efficacy of Vedolizumab for Ulcerative Colitis. J. Crohn’s Colitis 2017, 11, 400–411. [Google Scholar] [CrossRef] [PubMed]
- Ungar, B.; Levy, I.; Yavne, Y.; Yavzori, M.; Picard, O.; Fudim, E.; Loebstein, R.; Chowers, Y.; Eliakim, R.; Kopylov, U.; et al. Optimizing Anti-TNF-α Therapy: Serum Levels of Infliximab and Adalimumab Are Associated with Mucosal Healing in Patients with Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2016, 14, 550–557.e2. [Google Scholar] [CrossRef]
- Davidov, Y.; Ungar, B.; Bar-Yoseph, H.; Carter, D.; Haj-Natour, O.; Yavzori, M.; Chowers, Y.; Eliakim, R.; Ben-Horin, S.; Kopylov, U. Association of Induction Infliximab Levels with Clinical Response in Perianal Crohn’s Disease. J. Crohn’s Colitis 2016, 11, 549–555. [Google Scholar] [CrossRef]
- Bortlik, M.; Duricova, D.; Malickova, K.; Machkova, N.; Bouzkova, E.; Hrdlicka, L.; Komárek, A.; Lukas, M. Infliximab trough levels may predict sustained response to infliximab in patients with Crohn’s disease. J. Crohn’s Colitis 2013, 7, 736–743. [Google Scholar] [CrossRef]
- Wilson, A.; Choi, B.; Sey, M.; Ponich, T.; Beaton, M.; Kim, R.B. High infliximab trough concentrations are associated with sustained histologic remission in inflammatory bowel disease: A prospective cohort study. BMC Gastroenterol. 2021, 21, 77. [Google Scholar] [CrossRef]
- Dreesen, E.; Verstockt, B.; Bian, S.; de Bruyn, M.; Compernolle, G.; Tops, S.; Noman, M.; Van Assche, G.; Ferrante, M.; Gils, A.; et al. Evidence to Support Monitoring of Vedolizumab Trough Concentrations in Patients with Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2018, 16, 1937–1946.e8. [Google Scholar] [CrossRef]
- Al-Bawardy, B.; Ramos, G.P.; Willrich, M.A.V.; Jenkins, S.M.; Park, S.H.; Aniwan, S.; Schoenoff, S.A.; Bruining, D.H.; Papadakis, K.A.; Raffals, L.; et al. Vedolizumab Drug Level Correlation with Clinical Remission, Biomarker Normalization, and Mucosal Healing in Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2019, 25, 580–586. [Google Scholar] [CrossRef] [PubMed]
- Yacoub, W.; Williet, N.; Pouillon, L.; Di-Bernado, T.; Bittencourt, M.D.C.; Nancey, S.; Lopez, A.; Paul, S.; Zallot, C.; Roblin, X.; et al. Early vedolizumab trough levels predict mucosal healing in inflammatory bowel disease: A multicentre prospective observational study. Aliment. Pharmacol. Ther. 2018, 47, 906–912. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Dulai, P.S.; Casteele, N.V.; Battat, R.; Fumery, M.; Boland, B.S.; Sandborn, W.J. Systematic review with meta-analysis: Association between vedolizumab trough concentration and clinical outcomes in patients with inflammatory bowel diseases. Aliment. Pharmacol. Ther. 2019, 50, 848–857. [Google Scholar] [CrossRef]
- Peyrin-Biroulet, L.; Danese, S.; Argollo, M.; Pouillon, L.; Peppas, S.; Gonzalez-Lorenzo, M.; Lytras, T.; Bonovas, S. Loss of Response to Vedolizumab and Ability of Dose Intensification to Restore Response in Patients with Crohn’s Disease or Ulcerative Colitis: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2019, 17, 838–846.e2. [Google Scholar] [CrossRef] [PubMed]
- Vaughn, B.P.; Yarur, A.J.; Graziano, E.; Campbell, J.P.; Bhattacharya, A.; Lee, J.Y.; Gheysens, K.; Papamichael, K.; Osterman, M.T.; Cheifetz, A.S.; et al. Vedolizumab Serum Trough Concentrations and Response to Dose Escalation in Inflammatory Bowel Disease. J. Clin. Med. 2020, 9, 3142. [Google Scholar] [CrossRef]
- Ungar, B.; Malickova, K.; Hanžel, J.; Abu Arisha, M.; Paul, S.; Rocha, C.; Ben Shatach, Z.; Abitbol, C.M.; Natour, O.H.; Selinger, L.; et al. Dose optimisation for Loss of Response to Vedolizumab— Pharmacokinetics and Immune Mechanisms. J. Crohn’s Colitis 2021, 15, 1707–1719. [Google Scholar] [CrossRef]
- Wu, Y.; Lin, B.; Thilakanathan, C.; Lehmann, P.; Xuan, W.; Mohsen, W.; Toong, C.; Williams, A.; Ng, W.; Connor, S. Therapeutic drug monitoring in inflammatory bowel disease reduces unnecessary use of infliximab with substantial associated cost-savings. Intern. Med. J. 2021, 51, 739–745. [Google Scholar] [CrossRef]
- Cheifetz, A.S.; Abreu, M.T.; Afif, W.; Cross, R.K.; Dubinsky, M.C.; Loftus, E.V.; Osterman, M.T.; Saroufim, A.; Siegel, C.A.; Yarur, A.J.; et al. A Comprehensive Literature Review and Expert Consensus Statement on Therapeutic Drug Monitoring of Biologics in Inflammatory Bowel Disease. Am. J. Gastroenterol. 2021, 116, 2014–2025. [Google Scholar] [CrossRef]
- Higgins, P.D.R.; Schwartz, M.; Mapili, J.; Krokos, I.; Leung, J.; Zimmermann, E.M. Patient defined dichotomous end points for remission and clinical improvement in ulcerative colitis. Gut 2005, 54, 782–788. [Google Scholar] [CrossRef]
- Brooke, B.N. Index of Crohn’S Disease Activity. Lancet 1980, 315, 711. [Google Scholar] [CrossRef]
- Daperno, M.; Haens, G.D.; Assche, G.; Van Baert, F. Development and validation of a new, simplified endoscopic activity score for Crohn’s disease: The SES-CD. Gastrointest. Endosc. 2004, 60, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Osterman, M.T.; Rosario, M.; Lasch, K.; Barocas, M.; Wilbur, J.D.; Dirks, N.L.; Gastonguay, M.R. Vedolizumab exposure levels and clinical outcomes in ulcerative colitis: Determining the potential for dose optimisation. Aliment. Pharmacol. Ther. 2019, 49, 408–418. [Google Scholar] [CrossRef] [PubMed]
- Casteele, N.V.; Sandborn, W.J.; Feagan, B.G.; Vermeire, S.; Dulai, P.S.; Yarur, A.; Roblin, X.; Ben-Horin, S.; Dotan, I.; Osterman, M.T.; et al. Real-world multicentre observational study including population pharmacokinetic modelling to evaluate the exposure–response relationship of vedolizumab in inflammatory bowel disease: ERELATE Study. Aliment. Pharmacol. Ther. 2022, 56, 463–476. [Google Scholar] [CrossRef] [PubMed]
- Guidi, L.; Pugliese, D.; Tonucci, T.P.; Bertani, L.; Costa, F.; Privitera, G.; Tolusso, B.; Di Mario, C.; Albano, E.; Tapete, G.; et al. Early vedolizumab trough levels predict treatment persistence over the first year in inflammatory bowel disease. United Eur. Gastroenterol. J. 2019, 7, 1189–1197. [Google Scholar] [CrossRef]
- Hanžel, J.; Sever, N.; Ferkolj, I.; Štabuc, B.; Smrekar, N.; Kurent, T.; Koželj, M.; Novak, G.; Compernolle, G.; Tops, S.; et al. Early vedolizumab trough levels predict combined endoscopic and clinical remission in inflammatory bowel disease. United Eur. Gastroenterol. J. 2019, 7, 741–749. [Google Scholar] [CrossRef]
- Liefferinckx, C.; Minsart, C.; Cremer, A.; Amininejad, L.; Tafciu, V.; Quertinmont, E.; Tops, S.; Devière, J.; Gils, A.; van Gossum, A.; et al. Early vedolizumab trough levels at induction in inflammatory bowel disease patients with treatment failure during maintenance. Eur. J. Gastroenterol. Hepatol. 2019, 31, 478–485. [Google Scholar] [CrossRef]
- Yarur, A.J.; Bruss, A.; Naik, S.; Beniwal-Patel, P.; Fox, C.; Jain, A.; Berens, B.; Patel, A.; Ungaro, R.; Bahur, B.; et al. Vedolizumab Concentrations Are Associated with Long-Term Endoscopic Remission in Patients with Inflammatory Bowel Diseases. Dig. Dis. Sci. 2019, 64, 1651–1659. [Google Scholar] [CrossRef]
- Outtier, A.; Wauters, L.; Rahier, J.F.; Bossuyt, P.; Colard, A.; Franchimont, D.; Lambrecht, G.; Macken, E.; Van Moerkercke, W.; Baert, F.; et al. Effect of vedolizumab dose intensification on serum drug concentrations and regain of response in inflammatory bowel disease patients with secondary loss of response. GastroHep 2021, 3, 63–71. [Google Scholar] [CrossRef]
- Vermeire, S.; Lukáš, M.; Magro, F.; Adsul, S.; Lindner, D.; Rosario, M.; Roth, J.; Danese, S. Vedolizumab efficacy, safety, and pharmacokinetics with reduced frequency of dosing from every 4 weeks to every 8 weeks in patients with Crohn’s disease or ulcerative colitis. J. Crohn’s Colitis 2020, 14, 1066–1073. [Google Scholar] [CrossRef]
- Osterman, M.T.; Jairath, V.; Rana-Khan, Q.; James, A.; Balma, D.; Mehrotra, S.; Yang, L.; Lasch, K.; Yarur, A.J. A randomized trial of vedolizumab dose optimization in patients with moderate to severe ulcerative colitis who have early nonresponse and high drug clearance: The enterpret trial. Gastroenterology 2022, 162, 7. [Google Scholar] [CrossRef]
- Ungar, B.; Kopylov, U.; Yavzori, M.; Fudim, E.; Picard, O.; Lahat, A.; Coscas, D.; Waterman, M.; Haj-Natour, O.; Orbach-Zingboim, N.; et al. Association of Vedolizumab Level, Anti-Drug Antibodies, and α4β7 Occupancy with Response in Patients with Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2018, 16, 697–705.e7. [Google Scholar] [CrossRef] [PubMed]
- Schulze, H.; Esters, P.; Hartmann, F.; Stein, J.; Christ, C.; Zorn, M.; Dignass, A. A prospective cohort study to assess the relevance of vedolizumab drug level monitoring in IBD patients. Scand. J. Gastroenterol. 2018, 53, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Dulai, P.S.; Boland, B.S.; Singh, S.; Chaudrey, K.; Koliani-Pace, J.L.; Kochhar, G.; Parikh, M.P.; Shmidt, E.; Hartke, J.; Chilukuri, P.; et al. Development and Validation of a Scoring System to Predict Outcomes of Vedolizumab Treatment in Patients with Crohn’s Disease. Gastroenterology 2018, 155, 687–695.e10. [Google Scholar] [CrossRef] [PubMed]
- Parrish, A.B.; Lopez, N.E.; Truong, A.; Zaghiyan, K.; Melmed, G.Y.; McGovern, D.P.B.; Ha, C.; Syal, G.; Bonthala, N.; Jain, A.; et al. Preoperative Serum Vedolizumab Levels Do Not Impact Postoperative Outcomes in Inflammatory Bowel Disease. Dis. Colon Rectum 2021, 10, 1259–1266. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Population n = 86 | |
| Age of diagnosis, n (median, IQR) | 26 (18, 39.5) |
| Male, n (%) Female, n (%) | 48 (55.8) 38 (44.2) |
| CD, n (%) UC, n (%) | 51 (59.3) 35 (40.7) |
| CD extent, n (% of CD patients) L1 (ileal) L2 (colonic) L3 (ileo-colonic) Perianal disease | 19 (37.2) 4 (7.8) 28 (55) 16 (31.4) |
| CD behavior, n (% of CD patients) B1 (non-stricturing and non-penetrating) B2 (stricturing) B3 (penetrating) B2 + B3 | 13 (25.5) 16 (31.4) 18 (35.3) 4 (7.8) |
| UC extent, n (% of UC patients) E1 (proctitis) E2 (left sided colitis) E3 (right sided colitis) | 0 (0) 13 (37.1) 22 (62.9) |
| Extra-intestinal manifestations, n (%) | 39 (45.3) |
| Smoking (current or past), n (%) | 19 (22.1) |
| Past IBD Treatment | |
| Immunomodulator, n (%) | 56 (65.1) |
| 5-ASA derivatives, n (%) | 49 (57) |
| Infliximab and reason for cessation, n (%) LOR Immunogenicity Adverse event Compliance Other | 53 (61.6) 26 (49.1) 13 (24.5) 11 (20.7) 0 (0) 3 (5.7) |
| Adalimumab and reason for cessation, n (%) LOR Immunogenicity Adverse event Compliance Other | 37 (43) 23 (62.1) 6 (16.2) 5 (13.5) 1 (2.7) 2 (5.4) |
| Ustekinumab and reason for cessation, n (%) LOR | 5 (5.8) 5 (100) |
| Vedolizumab Treatment | |
| Duration of treatment, median weeks, n (IQR) | 46.4 (29.6, 83.6) |
| Reason for therapy cessation, n (%) LOR Adverse event Compliance | 72 (83.7) 13 (15.1) 1 (1.2) |
| Adverse events leading to therapy cessation, n (% of adverse events) Erythema Nodosum Arthralgia Paraesthesia Rash Acute otitis media Headache Recurrent pharyngitis Elevated liver enzymes | 1 (7.7) 4 (30.7) 1 (7.7) 3 (23.1) 1 (7.7) 1 (7.7) 1 (7.7) 1 (7.7) |
| Additional therapy on stop, n (%) Steroids Immunomodulators 5-ASA derivatives | 28 (32.5) 9 (10.4) 24 (27.9) |
| Last drug levels, μg/mL (IQR) | 30 (12.5, 53) |
| Vedolizumab dose interval on discontinuation, n (%) 4 weeks 8 weeks | 60 (69.8) 26 (30.2) |
| CRP on stop, mg/L (IQR) | 11 (4.6, 34.25) |
| Sequential Treatment, n (%) | |
| Infliximab Adalimumab Ustekinumab Certolizumab Golimumab Tofacitinib Tacrolimus Research Surgery | 19 (22.1) 7 (8.1) 24 (27.9) 6 (7) 1 (1.2) 7 (8.1) 1 (1.2) 11 (12.8) 10 (11.6) |
| Duration between vedolizumab cessation and initiation of subsequent therapy, median weeks, n (IQR) | 8.8 (5.32, 21.1) |
| Reason for cessation of subsequent therapy, n (%) LOR Immunogenicity Adverse event Compliance Other Therapy ongoing | 39 (51.3) 2 (2.6) 9 (11.8) 1 (1.3) 2 (2.6) 24 (31.6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Levartovsky, A.; Cohen, I.; Abitbol, C.M.; Yavzori, M.; Fudim, E.; Picard, O.; Kopylov, U.; Ben-Horin, S.; Ungar, B. Do Vedolizumab trough Levels Predict the Outcome of Subsequent Therapy in Inflammatory Bowel Disease? Biomedicines 2023, 11, 1553. https://doi.org/10.3390/biomedicines11061553
Levartovsky A, Cohen I, Abitbol CM, Yavzori M, Fudim E, Picard O, Kopylov U, Ben-Horin S, Ungar B. Do Vedolizumab trough Levels Predict the Outcome of Subsequent Therapy in Inflammatory Bowel Disease? Biomedicines. 2023; 11(6):1553. https://doi.org/10.3390/biomedicines11061553
Chicago/Turabian StyleLevartovsky, Asaf, Ido Cohen, Chaya Mushka Abitbol, Miri Yavzori, Ella Fudim, Orit Picard, Uri Kopylov, Shomron Ben-Horin, and Bella Ungar. 2023. "Do Vedolizumab trough Levels Predict the Outcome of Subsequent Therapy in Inflammatory Bowel Disease?" Biomedicines 11, no. 6: 1553. https://doi.org/10.3390/biomedicines11061553