

Relationship between Abnormal Placenta and Obstetric Outcomes: A Meta-Analysis
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
2.2. Systematic Literature Review Approach
2.3. Eligibility Criteria, Information Sources, and Search Strategy
2.4. Study Selection
2.5. Data Extraction
2.6. Analysis of Outcome Measures and Assessment of Bias Risk
2.7. Sensitivity Analysis
2.8. Meta-Analysis Plan
2.9. Statistical Analysis
3. Results of the Systematic Review
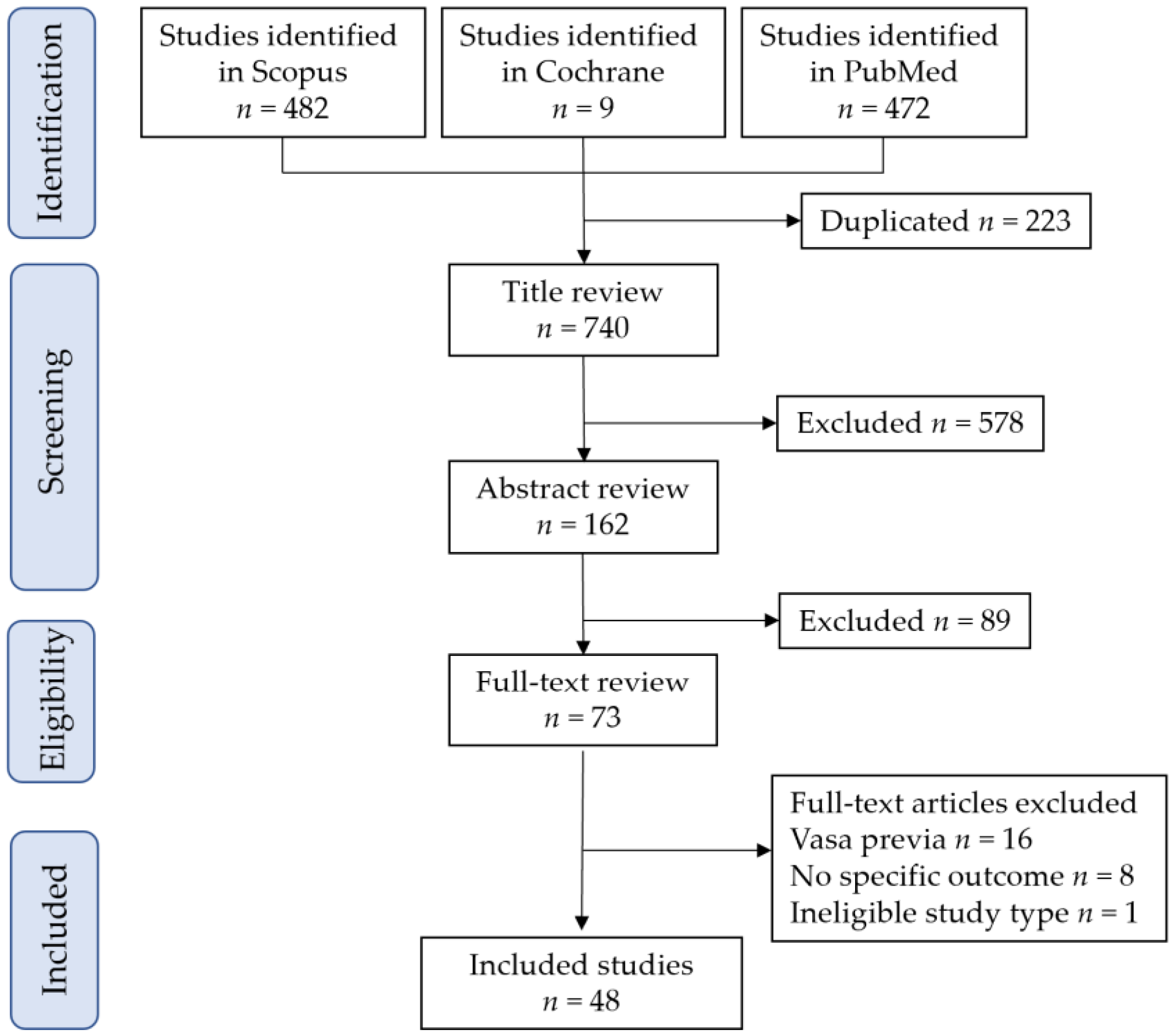
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias of Included Studies
4. Results of the Meta-Analysis
4.1. Circumvallate Placenta
4.1.1. Study Characteristics
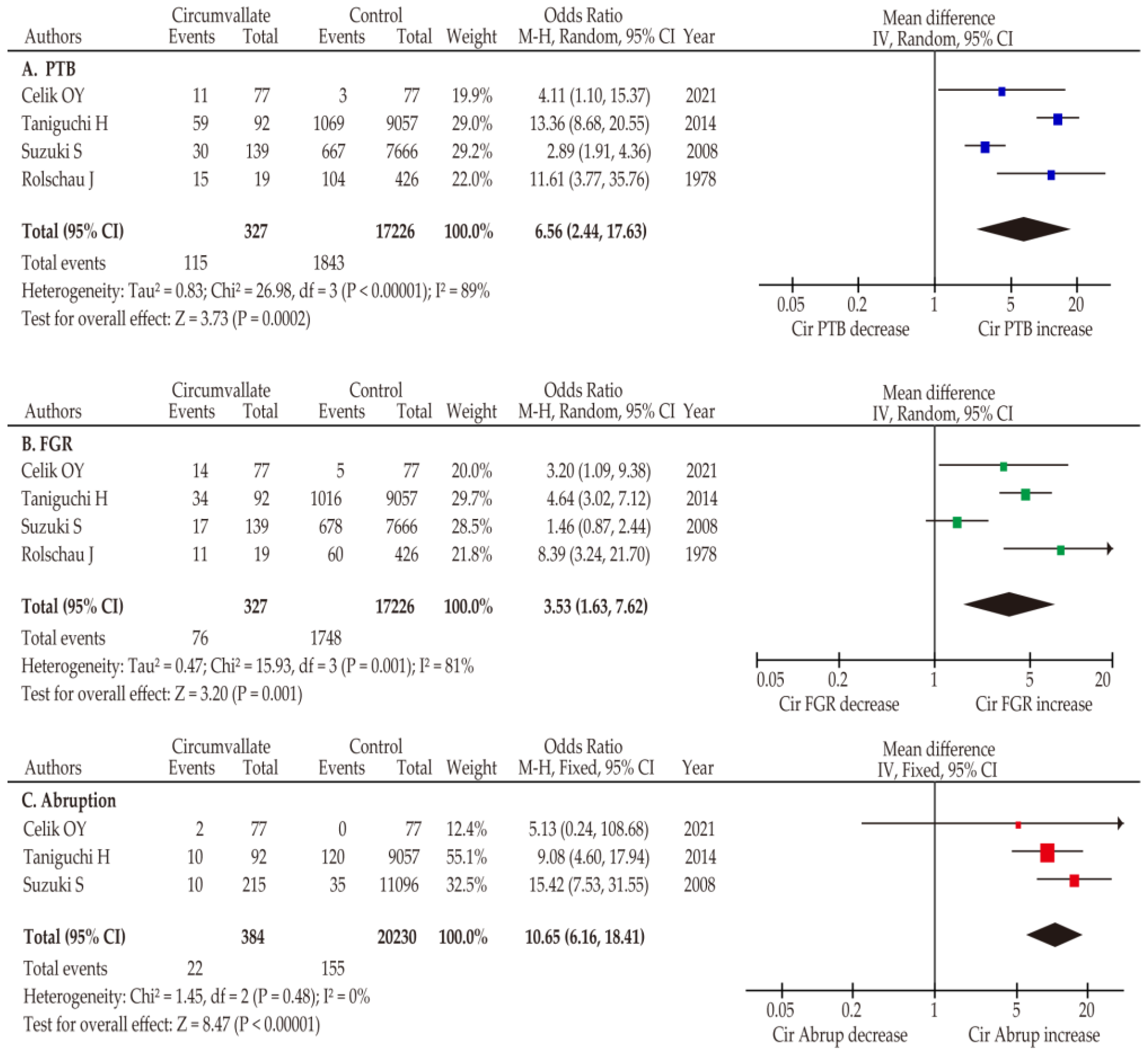
4.1.2. Primary Outcome: Obstetric Outcomes
4.1.3. Co-Primary Outcomes: Incidence
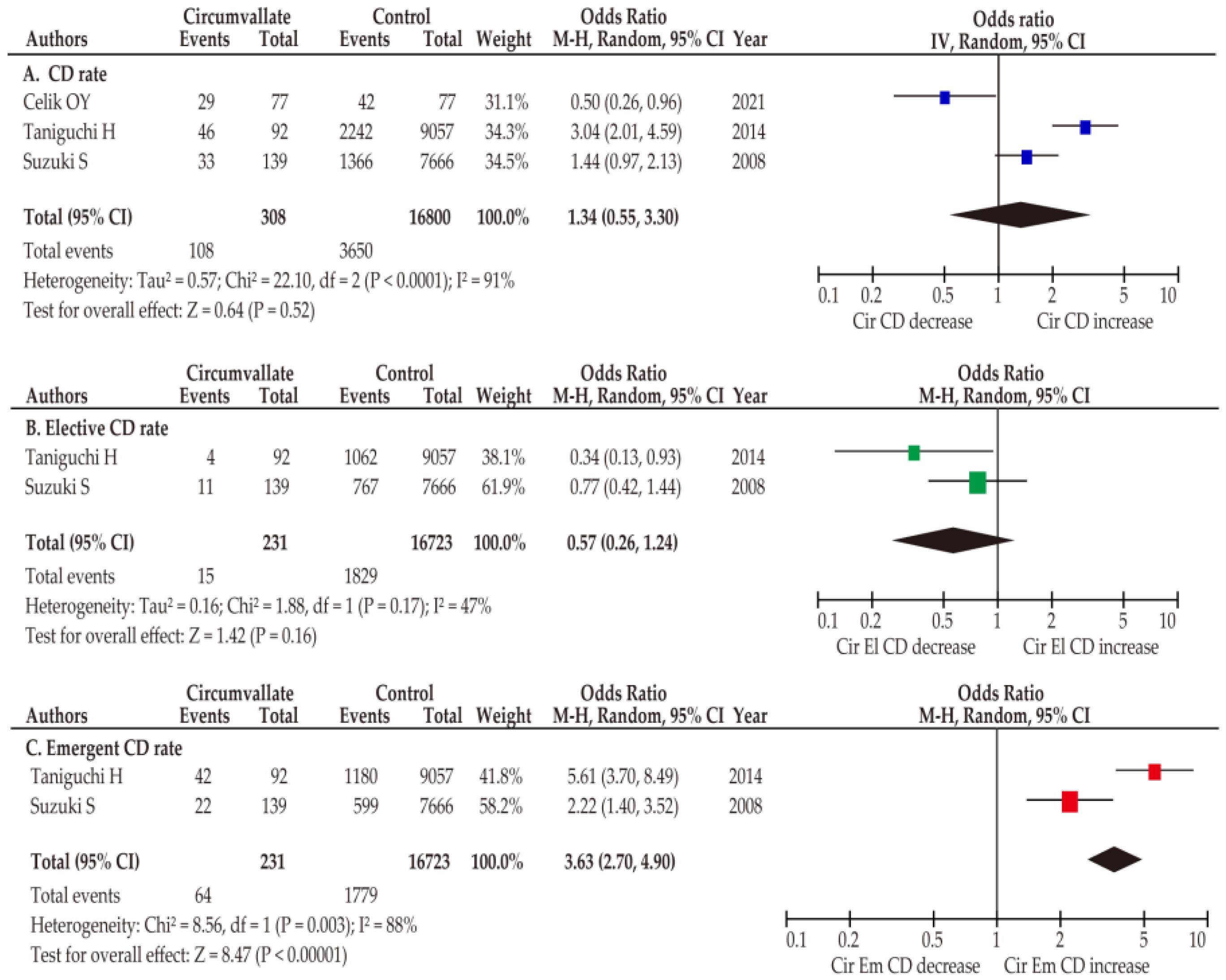
4.1.4. Secondary Outcome: Delivery Outcomes
4.1.5. Association between ART Pregnancy and Circumvallate Placenta
4.2. Succenturiate Lobe Placenta
4.2.1. Study Characteristics
4.2.2. Primary and Secondary Outcomes: Obstetric and Delivery Outcomes
4.2.3. Co-Primary Outcome: Incidence
4.3. Multilobed Placenta
4.3.1. Study Characteristics
4.3.2. Primary Outcome: Obstetric Outcomes
4.3.3. Co-primary Outcome: Incidence
4.3.4. Secondary Outcome: Delivery Outcomes
4.4. Placenta Membranacea
4.4.1. Study Characteristics
4.4.2. Primary Outcome: Obstetric Outcomes
4.4.3. Co-Primary Outcome: Incidence
4.4.4. Secondary Outcome: Delivery Outcomes
5. Discussion
5.1. Principal Findings
5.2. Strengths and Limitations
5.3. Comparison with Existing Literature
5.3.1. Primary Outcomes: Obstetric Outcomes in Abnormal Placenta
5.3.2. Co-Primary Outcomes: Incidence of Abnormal Placenta
5.3.3. Secondary Outcomes: Delivery Outcomes
5.3.4. Sensitivity Analysis: ART and Abnormal Placenta
6. Conclusions and Implications
6.1. Implications for Practice
6.2. Implications for Research
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Burton, G.J.; Hempstock, J.; Jauniaux, E. Nutrition of the human fetus during the first trimester—A review. Placenta 2001, 22 (Suppl. SA), S70–S77. [Google Scholar] [CrossRef] [PubMed]
- Costello, J.F.; Fisher, S.J. The Placenta—Fast, Loose, and in Control. N. Engl. J. Med. 2021, 385, 87–89. [Google Scholar] [CrossRef]
- Coorens, T.H.H.; Oliver, T.R.W.; Sanghvi, R.; Sovio, U.; Cook, E.; Vento-Tormo, R.; Haniffa, M.; Young, M.D.; Rahbari, R.; Sebire, N.; et al. Inherent mosaicism and extensive mutation of human placentas. Nature 2021, 592, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Rathbun, K.M.; Hildebrand, J.P. Placenta Abnormalities. In StatPearls; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Woods, L.; Perez-Garcia, V.; Hemberger, M. Regulation of placental development and its impact on fetal growth—New insights from mouse models. Front. Endocrinol. 2018, 9, 570. [Google Scholar] [CrossRef] [PubMed]
- Murphy, V.E.; Smith, R.; Giles, W.B.; Clifton, V.L. Endocrine regulation of human fetal growth: The role of the mother, placenta, and fetus. Endocr. Rev. 2006, 27, 141–169. [Google Scholar] [CrossRef]
- Matsuzaki, N.; Taniguchi, T.; Shimoya, K.; Neki, R.; Okada, T.; Saji, F.; Nakayama, M.; Suehara, N.; Tanizawa, O. Placental interleukin-6 production is enhanced in intrauterine infection but not in labor. Am. J. Obstet. Gynecol. 1993, 168, 94–97. [Google Scholar] [CrossRef]
- Matsuzaki, N.; Li, Y.; Masuhiro, K.; Jo, T.; Shimoya, K.; Taniguchi, T.; Saji, F.; Tanizawa, O. Trophoblast-derived transforming growth factor-beta 1 suppresses cytokine-induced, but not gonadotropin-releasing hormone-induced, release of human chorionic gonadotropin by normal human trophoblasts. J. Clin. Endocrinol. Metab. 1992, 74, 211–216. [Google Scholar] [CrossRef]
- Suzuki, S.; Kato, M. Clinical Significance of Pregnancies Complicated by Velamentous Umbilical Cord Insertion Associated with Other Umbilical Cord/Placental Abnormalities. J. Clin. Med. Res. 2015, 7, 853–856. [Google Scholar] [CrossRef]
- Ventolini, G.; Samlowski, R.; Hood, D.L. placental findings in low-risk, singleton, term pregnancies after uncomplicated deliveries. Am. J. Perinatol. 2004, 21, 325–328. [Google Scholar] [CrossRef]
- Taniguchi, H.; Aoki, S.; Sakamaki, K.; Kurasawa, K.; Okuda, M.; Takahashi, T.; Hirahara, F. Circumvallate placenta: Associated clinical manifestations and complications—A retrospective study. Obstet. Gynecol. Int. 2014, 2014, 986230. [Google Scholar] [CrossRef]
- Suzuki, S. Clinical significance of pregnancies with circumvallate placenta. J. Obstet. Gynaecol. Res. 2008, 34, 51–54. [Google Scholar] [CrossRef]
- Ma, J.-S.; Meia, X.; Niu, Y.-X.; Li, Q.-G.; Jiang, X.-F. Risk factors and adverse pregnancy outcomes of succenturiate placenta: A case-control study. J. Reprod. Med. 2016, 61, 139–144. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; the PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Matsuzaki, S.; Nagase, Y.; Ueda, Y.; Lee, M.; Matsuzaki, S.; Maeda, M.; Takiuchi, T.; Kakigano, A.; Mimura, K.; Endo, M.; et al. The association of endometriosis with placenta previa and postpartum hemorrhage: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. MFM 2021, 3, 100417. [Google Scholar] [CrossRef]
- Matsuzaki, S.; Nagase, Y.; Ueda, Y.; Kakuda, M.; Maeda, M.; Matsuzaki, S.; Kamiura, S. Placenta previa complicated with endometriosis: Contemporary clinical management, molecular mechanisms, and future research opportunities. Biomedicines 2021, 9, 1536. [Google Scholar] [CrossRef]
- Matsuzaki, S.; Ueda, Y.; Matsuzaki, S.; Kakuda, M.; Lee, M.; Takemoto, Y.; Hayashida, H.; Maeda, M.; Kakubari, R.; Hisa, T.; et al. The characteristics and obstetric outcomes of type II vasa previa: Systematic review and meta-analysis. Biomedicines 2022, 10, 3263. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Danna, S.; Graham, E.; Burns, R.; Deschênes, S.S.; Schmitz, N. Association between depressive symptoms and cognitive function in persons with diabetes mellitus: A systematic review. PLoS ONE 2016, 11, e0160809. [Google Scholar] [CrossRef]
- ROBINS-I Detailed Guidance. 2016. Available online: https://www.riskofbias.info/welcome/home/current-version-of-robins-i/robins-i-detailed-guidance-2016 (accessed on 20 September 2020).
- Matsuzaki, S.; Lee, M.; Nagase, Y.; Jitsumori, M.; Matsuzaki, S.; Maeda, M.; Takiuchi, T.; Kakigano, A.; Mimura, K.; Ueda, Y.; et al. A systematic review and meta-analysis of obstetric and maternal outcomes after prior uterine artery embolization. Sci. Rep. 2021, 11, 16914. [Google Scholar] [CrossRef]
- Matsuzaki, S.; Ueda, Y.; Nagase, Y.; Matsuzaki, S.; Kakuda, M.; Kakuda, S.; Sakaguchi, H.; Hisa, T.; Kamiura, S. Placenta accreta spectrum disorder complicated with endometriosis: Systematic review and meta-analysis. Biomedicines 2022, 10, 390. [Google Scholar] [CrossRef]
- Cochrane Handbook for Systematic Reviews of Interventions. Version 6.3, 2022. Chapter 10: Analysing Data and Undertaking Meta-Analyses. Available online: https://training.cochrane.org/handbook/current/chapter-10 (accessed on 10 April 2023).
- Swanson, K.; Huang, D.; Kaing, A.; Blat, C.; Rosenstein, M.G.; Mok-Lin, E.; Gras, J.; Sperling, J.D. Is preimplantation genetic testing associated with increased risk of abnormal placentation after frozen embryo transfer? Am. J. Perinatol. 2021, 38, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Kutuk, M.S.; Takmaz, T.; Bayram, A.; Ozturk, S. Prenatal sonographic detection of monochorionic twins with bipartite placenta. Fetal Pediatr. Pathol. 2021, 40, 685–690. [Google Scholar] [CrossRef] [PubMed]
- Celik, O.Y.; Obut, M.; Keles, A.; Calık, M.G.; Dagdeviren, G.; Yucel, A.; Sahin, D. Outcomes of pregnancies diagnosed with circumvallate placenta, and use of uterine artery pulsatility index and maternal serum alpha-fetoprotein for prediction of adverse outcomes. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 262, 57–61. [Google Scholar] [CrossRef]
- Detweiler, M.; Downs, E. Sonographic detection of placenta percreta with associated placenta previa and succenturiate lobe. J. Diagn. Med. Sonogr. 2021, 37, 194–199. [Google Scholar] [CrossRef]
- Volodarsky-Perel, A.; Nu, T.N.T.; Buckett, W.; Machado-Gedeon, A.; Cui, Y.; Shaul, J.; Dahan, M.H. Effect of embryo stage at transfer on placental histopathology features in singleton live births resulting from fresh embryo transfers. Fertil. Steril. 2021, 115, 673–682. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, J.; Furuya, N.; Doi, M.; Sasaki, T.; Takagi, M.; Suzuki, N. Sono-embryological assessments of a true knot that developed into a hypercoiled cord and circumvallate placenta. J. Matern. Neonatal Med. 2021, 34, 4162–4166. [Google Scholar] [CrossRef]
- Sacha, C.R.; Harris, A.L.; James, K.; Basnet, K.; Freret, T.S.; Yeh, J.; Kaimal, A.; Souter, I.; Roberts, D.J. Placental pathology in live births conceived with in vitro fertilization after fresh and frozen embryo transfer. Am. J. Obstet. Gynecol. 2020, 222, 360.e1–360.e16. [Google Scholar] [CrossRef]
- Volodarsky-Perel, A.; Nu, T.N.T.; Buckett, W.; Machado-Gedeon, A.; Cui, Y.; Shaul, J.; Dahan, M.H. Effect of newborn gender on placental histopathology and perinatal outcome in singleton live births following IVF. Reprod. Biomed. Online 2020, 41, 907–916. [Google Scholar] [CrossRef]
- Abgral, M.; Martinovic, J.; Bonnin, A.; Houllier, M.; Senat, M.V.; Bouchghoul, H. Two separate placental masses on ultrasound do not always indicate a dichorionic pregnancy. J. Gynecol. Obstet. Hum. Reprod. 2020, 49, 101694. [Google Scholar] [CrossRef]
- Walter, A.; Strizek, B.; Berg, C.; Geipel, A.; Gembruch, U.; Engels, A.C. Outcome of monochorionic twins with prenatally diagnosed bipartite placenta. Arch. Gynecol. Obstet. 2020, 302, 1549–1552. [Google Scholar] [CrossRef]
- Tang, L.; Xu, L.; Hu, Y.; Zhang, L.; Wei, Q.; Wu, L. Placenta membranacea: An anormaly of the placenta: Three case reports. Medicine 2019, 98, e16166. [Google Scholar] [CrossRef]
- Hamadeh, S.; Addas, B.; Rahman, J. Succenturiate placenta—Abruption in a young primigravida: An unusual presentation. Clin. Exp. Obstet. Gynecol. 2018, 45, 789–790. [Google Scholar] [CrossRef]
- Sharma, N.; Das, R.; Salam, S.; Jethani, R.; Singh, A.S. coexistent circumvallate placenta and battledore insertion of umbilical cord resulting in grave obstetric outcome: A case report. J. Reprod. Infertil. 2017, 18, 390–392. [Google Scholar]
- Stelzl, P.W.; Yadav, G.; Perley, L.; Silasi, M. Early sonographic detection of a succenturiate placenta after IVF in a 42-year-old woman with multiple comorbidities. BMJ Case Rep. 2017, 2017, bcr-2017. [Google Scholar] [CrossRef]
- Biswas, P.R.; Paul, G.K.; Chowdhury, M.; Selim, M. A rare shape of placenta; placenta bipartite, bilobata, dimidiate, duplex: A rare case report. Bangladesh J. Obstet. Gynaecol. 2017, 31, 101–103. [Google Scholar] [CrossRef]
- Ishibashi, M.; Yang, P.Y. HDliveFlow with HDlive silhouette mode in antenatal diagnosis of bilobed placenta. Donald Sch. J. Ultrasound Obstet. Gynecol. 2016, 10, 415–417. [Google Scholar] [CrossRef]
- Patra, S.; Mistry, P.K.; Dutta, M.; Das, I. Placenta Previa with succenturiate placenta–delivered with a living healthy baby. Bangladesh J. Obstet. Gynaecol. 2016, 30, 116–118. [Google Scholar] [CrossRef]
- Cavaliere, A.F.; Rosati, P.; Ciliberti, P.; Buongiorno, S.; Guariglia, L.; Scambia, G.; Tintoni, M. Succenturiate lobe of placenta with vessel anomaly: A case report of prenatal diagnosis and literature review. Clin. Imaging 2014, 38, 747–750. [Google Scholar] [CrossRef]
- Ravangard, S.F.; Henderson, K.; Fuller, K. Placenta membranacea. Arch. Gynecol. Obstet. 2013, 288, 709–712. [Google Scholar] [CrossRef]
- Morales-Roselló, J.; Llorens, N.P. Doppler impedance changes at the fetal brain vessels in a pregnancy affected with a multiple combination of uteroplacental anomalies. Case Rep. Med. 2012, 2012, 293156. [Google Scholar] [CrossRef]
- Suzuki, S.; Igarashi, M.; Inde, Y.; Miyake, H. Abnormally shaped placentae in twin pregnancy. Arch. Gynecol. Obstet. 2010, 281, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S. Antenatal screening for circumvallate placenta. J. Med. Ultrason. 2008, 35, 71–73. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Igarashi, M. Clinical significance of pregnancies with succenturiate lobes of placenta. Arch. Gynecol. Obstet. 2008, 277, 299–301. [Google Scholar] [CrossRef] [PubMed]
- Seleye-Fubara, D.; Akani, C.I. Succenturiate placenta: A rare variant in Rivers State Nigeria (a report of one case). Niger. J. Med. 2005, 14, 325–326. [Google Scholar] [PubMed]
- Brucks, U.A.; Duval, J.R. Perinatal Evaluation of the Bilobed or Bipartite Placenta. J. Diagn. Med. Sonogr. 2002, 18, 161–166. [Google Scholar] [CrossRef]
- Shukunami, K.-I.; Tsunezawa, W.; Hosokawa, K.; Tajima, K.; Kotsuji, F. Placenta previa of a succenturiate lobe: A report of two cases. Eur. J. Obstet. Gynecol. Reprod. Biol. 2001, 99, 276–277. [Google Scholar] [CrossRef]
- Walkup, D.W.M. a rare case of duplicated placenta and bifurcated umbilical cord in a singleton pregnancy. J. Diagn. Med. Sonogr. 2001, 17, 280–285. [Google Scholar] [CrossRef]
- Chihara, H.; Otsubo, Y.; Ohta, Y.; Araki, T. Prenatal diagnosis of succenturiate lobe by ultrasonography and color Doppler imaging. Arch. Gynecol. Obstet. 2000, 263, 137–138. [Google Scholar] [CrossRef]
- Harris, R.D.; Wells, W.A.; Black, W.C.; Chertoff, J.D.; Poplack, S.P.; Sargent, S.K.; Crow, H.C. Accuracy of prenatal sonography for detecting circumvallate placenta. Am. J. Roentgenol. 1997, 168, 1603–1608. [Google Scholar] [CrossRef]
- Steemers, N.Y.; De Rop, C.; Van Assche, A. Zonary placenta. Int. J. Gynecol. Obstet. 1995, 51, 251–253. [Google Scholar] [CrossRef]
- McCarthy, J.; Thurmond, A.S.; Jones, M.K.; Sistrom, C.; Scanlan, R.M.; Jacobson, S.L.; Lowensohn, R. Circumvallate placenta: Sonographic diagnosis. J. Ultrasound Med. 1995, 14, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Sistrom, C.L.; Ferguson, J.E. Abnormal membranes in obstetrical ultrasound: Incidence and significance of amniotic sheets and circumvallate placenta. Ultrasound Obstet. Gynecol. 1993, 3, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Dinh, T.V.; Bedi, D.G.; Salinas, J. Placenta membranacea, previa and accreta. A case report. J. Reprod. Med. 1992, 37, 97–99. [Google Scholar]
- Bey, M.; Dott, A.; Miller, J.M., Jr. The sonographic diagnosis of circumvallate placenta. Obstet. Gynecol. 1991, 78, 515–517. [Google Scholar]
- Greenberg, J.A.; Sorem, K.A.; Shifren, J.L.; Riley, L.E. Placenta membranacea with placenta increta: A case report and literature review. Obstet. Gynecol. 1991, 78, 512–514. [Google Scholar] [PubMed]
- Wilkins, B.S.; Batcup, G.; Vinall, P.S. Partial placenta membranacea. BJOG Int. J. Obstet. Gynaecol. 1991, 98, 675–679. [Google Scholar] [CrossRef]
- Hata, K.; Hata, T.; Aoki, S.; Takamori, H.; Takamiya, O.; Kitao, M. Succenturiate placenta diagnosed by ultrasound. Gynecol. Obstet. Investig. 1988, 25, 273–276. [Google Scholar] [CrossRef]
- Jeanty, P.; Kirkpatrick, C.; Verhoogen, C.; Struyven, J. The succenturiate placenta. J. Ultrasound Med. 1983, 2, 9–12. [Google Scholar] [CrossRef]
- Rolschau, J. Circumvallate placenta and intrauterine growth retardation. Acta Obstet. Gynecol. Scand. 1978, 57, 11–14. [Google Scholar] [CrossRef]
- Nelson, L.H.; Fishburne, J.I.; Stearns, B.R. Ultrasonographic description of succenturiate placenta. Obstet. Gynecol. 1977, 49, 79–80. [Google Scholar]
- Wladimiroff, J.W.; Wallenburg, H.C.S.; Putten, P.V.D.; Drogendijk, A.C. Ultrasonic diagnosis of placenta membranacea. Arch. Gynecol. Obstet. 1976, 221, 167–174. [Google Scholar] [CrossRef]
- Mathews, J. Placenta Membranacea. Aust. N. Z. J. Obstet. Gynaecol. 1974, 14, 45–47. [Google Scholar] [CrossRef]
- Matsuzaki, S.; Ueda, Y.; Matsuzaki, S.; Nagase, Y.; Kakuda, M.; Lee, M.; Maeda, M.; Kurahashi, H.; Hayashida, H.; Hisa, T.; et al. Assisted reproductive technique and abnormal cord insertion: A systematic review and meta-analysis. Biomedicines 2022, 10, 1722. [Google Scholar] [CrossRef]
- Takemoto, Y.; Matsuzaki, S.; Matsuzaki, S.; Kakuda, M.; Lee, M.; Hayashida, H.; Maeda, M.; Kamiura, S. Current evidence on vasa previa without velamentous cord insertion or placental morphological anomalies (type III vasa previa): Systematic review and meta-analysis. Biomedicines 2023, 11, 152. [Google Scholar] [CrossRef]
- Cruz-Martínez, R.; Figueras, F.; Hernandez-Andrade, E.; Oros, D.; Gratacos, E. Fetal Brain Doppler to Predict Cesarean Delivery for Nonreassuring Fetal Status in Term Small-for-Gestational-Age Fetuses. Obstet. Gynecol. 2011, 117, 618–626. [Google Scholar] [CrossRef]
- Severi, F.M.; Bocchi, C.; Visentin, A.; Falco, P.; Cobellis, L.; Florio, P.; Zagonari, S.; Pilu, G. Uterine and fetal cerebral Doppler predict the outcome of third-trimester small-for-gestational age fetuses with normal umbilical artery Doppler. Ultrasound Obstet. Gynecol. 2002, 19, 225–228. [Google Scholar] [CrossRef]
- Oros, D.; Figueras, F.; Padilla, N.; Meler, E.; Gratacos, E.; Cruz-Martinez, R.; Hernandez-Andrade, E. Middle versus anterior cerebral artery Doppler for the prediction of perinatal outcome and neonatal neurobehavior in term small-for-gestational-age fetuses with normal umbilical artery Doppler. Ultrasound Obstet. Gynecol. 2010, 35, 456–461. [Google Scholar] [CrossRef]
- Lees, C.C.; Stampalija, T.; Baschat, A.; da Silva Costa, F.; Ferrazzi, E.; Figueras, F.; Hecher, K.; Kingdom, J.; Poon, L.C.; Salomon, L.J.; et al. ISUOG Practice Guidelines: Diagnosis and management of small-for-gestational-age fetus and fetal growth restriction. Ultrasound Obstet. Gynecol. 2020, 56, 298–312. [Google Scholar] [CrossRef]
- Ebbing, C.; Kessler, J.; Moster, D.; Rasmussen, S. Single umbilical artery and risk of congenital malformation: Population-based study in Norway. Ultrasound Obstet. Gynecol. 2020, 55, 510–515. [Google Scholar] [CrossRef]
- Ebbing, C.; Kessler, J.; Moster, D.; Rasmussen, S. Isolated single umbilical artery and the risk of adverse perinatal outcome and third stage of labor complications: A population-based study. Acta Obstet. Gynecol. Scand. 2020, 99, 374–380. [Google Scholar] [CrossRef]
- Chen, W.; Liu, N.; Shen, S.; Zhu, W.; Qiao, J.; Chang, S.; Dong, J.; Bai, M.; Ma, L.; Wang, S.; et al. Fetal growth restriction impairs hippocampal neurogenesis and cognition via Tet1 in offspring. Cell Rep. 2021, 37, 109912. [Google Scholar] [CrossRef] [PubMed]
- Baschat, A.A. Neurodevelopment following fetal growth restriction and its relationship with antepartum parameters of placental dysfunction. Ultrasound Obstet. Gynecol. 2011, 37, 501–514. [Google Scholar] [CrossRef]
- Baschat, A.A. Neurodevelopment after Fetal Growth Restriction. Fetal Diagn. Ther. 2014, 36, 136–142. [Google Scholar] [CrossRef]
- Rock, C.R.; White, T.A.; Piscopo, B.R.; Sutherland, A.E.; Miller, S.L.; Camm, E.J.; Allison, B.J. Cardiovascular and cerebrovascular implications of growth restriction: Mechanisms and potential treatments. Int. J. Mol. Sci. 2021, 22, 7555. [Google Scholar] [CrossRef]
- Masoumy, E.P.; Sawyer, A.A.; Sharma, S.; Patel, J.A.; Gordon, P.M.K.; Regnault, T.R.H.; Matushewski, B.; Weintraub, N.L.; Richardson, B.; Thompson, J.A.; et al. The lifelong impact of fetal growth restriction on cardiac development. Pediatr. Res. 2018, 84, 537–544. [Google Scholar] [CrossRef]
- Jauniaux, E.; Englert, Y.; Vanesse, M.; Hiden, M.; Wilkin, P. Pathologic features of placentas from singleton pregnancies obtained by in vitro fertilization and embryo transfer. Obstet. Gynecol. 1990, 76, 61–64. [Google Scholar] [PubMed]
- Matsuzaki, S.; Nagase, Y.; Takiuchi, T.; Kakigano, A.; Mimura, K.; Lee, M.; Matsuzaki, S.; Ueda, Y.; Tomimatsu, T.; Endo, M.; et al. Antenatal diagnosis of placenta accreta spectrum after in vitro fertilization-embryo transfer: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 9205. [Google Scholar] [CrossRef]
- Kamijo, K.; Miyamoto, T.; Ando, H.; Tanaka, Y.; Kikuchi, N.; Shinagawa, M.; Yamada, S.; Asaka, R.; Fuseya, C.; Ohira, S.; et al. Clinical characteristics of a novel “Type 3” vasa previa: Case series at a single center. J. Matern. Neonatal Med. 2021, 35, 7730–7736. [Google Scholar] [CrossRef]
- Ruiter, L.; Kok, N.; Limpens, J.; Derks, J.B.; de Graaf, I.M.; Mol, B.; Pajkrt, E. Incidence of and risk indicators for vasa praevia: A systematic review. BJOG Int. J. Obstet. Gynaecol. 2016, 123, 1278–1287. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author | Year | Total | n | Prevalence | ART | CD | ID | PTB | FGR & | PA |
|---|---|---|---|---|---|---|---|---|---|---|
| Swanson K. [24] | 2021 | 311 | 3 | 1.0% | 3 | -- | -- | -- | -- | -- |
| Celik O.Y. [26] # | 2021 | 154 | 77 | -- | -- | 29 | -- | 11 | 14 | 2 |
| Volodarsky A. [28] | 2021 | 677 | 8 | 1.2% | 8 | -- | -- | -- | -- | -- |
| Volodarsky A. [31] | 2020 | 1057 | 11 | 1.0% | 11 | -- | -- | -- | -- | -- |
| Sacha C.R. [30] $ | 2020 | 1140 | 62 * | -- | 62 | -- | -- | -- | -- | -- |
| Suzuki S. [9] | 2015 | 16,965 | 217 | 1.3% | -- | -- | -- | -- | -- | -- |
| Taniguchi H. [11] | 2014 | 9149 | 92 | 1.0% | 4 | 46 | 3 | 59 | -- | 10 |
| Suzuki S. [44] | 2010 | 11,311 † | 215 | 1.9% | -- | -- | -- | -- | -- | 10 |
| Suzuki S. [45] | 2008 | 722 | 11 | 1.5% | -- | -- | -- | 3 | 2 | 1 |
| Suzuki S. [12] | 2008 | 7930 | 139 | 1.8% | 1 | 33 | 10 | 30 | 17 | 7 |
| Ventolini G. [10] | 2004 | 88 | 3 | 3.4% | -- | -- | -- | -- | -- | -- |
| Harris R.D. [52] | 1997 | 62 | 1 | 1.6% | -- | -- | -- | -- | -- | -- |
| McCarthy J. [54] | 1995 | -- | 6 | -- | -- | -- | -- | 1 | -- | 1 |
| Sistrom C.L. [55] | 1993 | 1784 | 3 | 0.2% | -- | -- | -- | 1 | -- | -- |
| Rolschau J. [62] | 1978 | 447 | 19 | 4.3% | -- | -- | -- | 6 | 11 | -- |
| Author | Year | Total | Control | n | Em CD | PTB | FGR & | PA |
|---|---|---|---|---|---|---|---|---|
| Celik OY [26] | 2021 | 154 | 77 | 77 | -- | 4.11 (1.10, 15.37) | 3.20 (1.09, 9.38) | 5.13 (0.24, 108.68) |
| Taniguchi H [11] | 2014 | 9149 | 9057 | 92 | 5.61 (3.70–8.49) | 13.36 (8.68, 20.55) | 4.64 (3.02, 7.12) | 9.08 (4.60, 17.94) |
| Suzuki S [44] | 2010 | 11,311 | 11,096 | 215 | -- | -- | -- | 15.42 (7.53, 31.55) |
| Suzuki S [45] * | 2008 | 722 | 711 | 11 | -- | -- | -- | -- |
| Suzuki S [12] | 2008 | 7930 | 7666 | 139 | 2.22 (1.40–3.52) | 2.89 (1.91, 4.36) | 1.46 (0.87, 2.44) | -- |
| Rolschau J [62] | 1978 | 447 | 426 | 19 | -- | 11.61 (3.77, 35.76) | 8.39 (3.24, 21.70) | -- |
| Author | Year | Total | n | Exp. | Cont. | Exp. vs. Cont. | OR (95%CI) |
|---|---|---|---|---|---|---|---|
| Swanson K. [24] | 2021 | 311 | 3 | 1/158 | 2/153 | PGT vs non-PGT | 0.48 (0.04, 5.36) |
| Volodarsky A. [28] | 2021 | 679 | 8 | 1/252 | 7/425 | Cleavage vs Blastocyst | 0.24 (0.03, 1.94) |
| Volodarsky A. [31] | 2020 | 1057 | 11 | 5/527 | 6/530 | ART: Male vs Female | 0.84 (0.25, 2.76) |
| Sacha C.R. [30] | 2020 | 1140 | 62 * | 56/929 | 6/211 | Fresh vs Frozen | 2.19 (0.93, 5.16) |
| Taniguchi H. [11] | 2014 | 9149 | 92 | 4/359 | 88/8790 | ART vs Non-ART | 1.11 (0.41, 3.05) |
| Suzuki S. [12] | 2008 | 7930 | 139 | 1/102 | 101/7703 | ART vs Non-ART | 0.75 (0.10, 5.39) |
| Author | Year | Total | n | Prev. | ART | CD | PTB | FGR & | PA | PP |
|---|---|---|---|---|---|---|---|---|---|---|
| Swanson K. [24] | 2021 | 313 | 6 | 1.9% | 6 | -- | -- | -- | -- | -- |
| Volodarsky A. [28] | 2021 | 677 | 6 | 0.9% | 6 | -- | -- | -- | -- | -- |
| Volodarsky A. [31] | 2020 | 1057 | 13 | 1.2% | 13 | -- | -- | -- | -- | -- |
| Sacha C.R. [30] | 2020 | 1030 | 70 | -- | 70 | -- | -- | -- | -- | -- |
| Ma J.S. [13] | 2016 | 28,256 | 294 | 1.0% | 15 | 130 | 45 | 23 | 2 | 4 |
| Suzuki S. [9] | 2015 | 16,965 | 114 | 0.7% | -- | -- | -- | -- | -- | -- |
| Suzuki S. [44] | 2010 | 11,311 | 83 | 0.7% | -- | -- | -- | -- | -- | 2 |
| Suzuki S. [46] | 2008 | 7713 | 47 | 0.6% | 4 | 12 | 5 | 0 | * |
| Author | Year | Total | n | Em CD | PTB | PA | PP |
|---|---|---|---|---|---|---|---|
| Ma J.S. [13] | 2016 | 28,256 | 294 | 2.50 (1.91, 3.26) | 2.95 (2.16, 4.04) | 1.36 (0.34, 5.52) | 1.71 (0.63, 4.62) |
| Suzuki S. [44] | 2010 | 11,311 | 83 | -- | -- | -- | 3.44 (0.83, 14.24) |
| Suzuki S. [46] | 2008 | 7703 | 47 | 1.40 (0.55, 3.56) | 1.23 (0.48, 3.11) | 2.55 (0.15, 42.31) | -- |
| Pooled | 2.37 (1.83, 3.07) | 2.13 (0.92, 4.92) | 1.50 (0.43, 5.26) | 2.05 (0.91, 4.64) |
| Author | Year | Total | n | Age | Abortion | CD | PPH | FGR | PTB | PA | IUFD | PAS |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tang L. [34] | 2019 | 79,862 | 3 | 24 | -- | Yes | -- | -- | -- | -- | -- | Yes |
| 29 | -- | -- | -- | Yes | 28 wk | -- | Yes | Yes | ||||
| 20 | -- | -- | -- | -- | 25 wk | -- | Yes | -- | ||||
| Ravangard S.F. [42] | 2013 | -- | 1 | 35 | -- | Yes | -- | -- | 25 wk | Yes | -- | -- |
| Dinh T.V. [56] | 1992 | -- | 1 | 34 | -- | Yes | Yes | -- | -- | -- | -- | Yes |
| Greenberg J.A. [58] | 1991 | -- | 1 | 33 | -- | Yes | Yes | -- | 32 wk | -- | -- | Yes |
| Wilkins B.S. [59] | 1991 | -- | 7 | Unk | -- | -- | -- | -- | 24 wk | -- | -- | -- |
| Unk | 19 wk | -- | -- | -- | -- | -- | -- | Yes | ||||
| Unk | 18 wk | -- | -- | -- | -- | -- | -- | -- | ||||
| Unk | 23 wk | -- | -- | -- | -- | -- | -- | -- | ||||
| Unk | 17 wk | -- | -- | -- | -- | -- | -- | -- | ||||
| Unk | 17 wk | -- | -- | -- | -- | -- | -- | Yes | ||||
| Unk | -- | Yes | -- | -- | 30 wk | -- | -- | -- | ||||
| Wladimiroff J.W. [64] | 1976 | -- | 1 | 28 | -- | -- | -- | -- | 26 wk | -- | Yes | -- |
| Mathews J. [65] | 1974 | -- | 1 | 19 | 20 wk | -- | -- | -- | -- | -- | -- | -- |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsuzaki, S.; Ueda, Y.; Matsuzaki, S.; Sakaguchi, H.; Kakuda, M.; Lee, M.; Takemoto, Y.; Hayashida, H.; Maeda, M.; Kakubari, R.; et al. Relationship between Abnormal Placenta and Obstetric Outcomes: A Meta-Analysis. Biomedicines 2023, 11, 1522. https://doi.org/10.3390/biomedicines11061522
Matsuzaki S, Ueda Y, Matsuzaki S, Sakaguchi H, Kakuda M, Lee M, Takemoto Y, Hayashida H, Maeda M, Kakubari R, et al. Relationship between Abnormal Placenta and Obstetric Outcomes: A Meta-Analysis. Biomedicines. 2023; 11(6):1522. https://doi.org/10.3390/biomedicines11061522
Chicago/Turabian StyleMatsuzaki, Shinya, Yutaka Ueda, Satoko Matsuzaki, Hitomi Sakaguchi, Mamoru Kakuda, Misooja Lee, Yuki Takemoto, Harue Hayashida, Michihide Maeda, Reisa Kakubari, and et al. 2023. "Relationship between Abnormal Placenta and Obstetric Outcomes: A Meta-Analysis" Biomedicines 11, no. 6: 1522. https://doi.org/10.3390/biomedicines11061522