

Frequency of Vitamin D Receptor Gene Polymorphisms in a Population with a very High Prevalence of Vitamin D Deficiency, Obesity, Diabetes and Hypertension

Abstract
:1. Introduction
2. Materials and Methods
2.1. The Measurements
2.2. Biochemical and Urine Analysis
2.3. DNA Preparation and VDR SNPs Genotyping Analysis
2.4. Statistical Power of the Study
2.5. Statistical Analysis
3. Results
3.1. Baseline Charachteristics
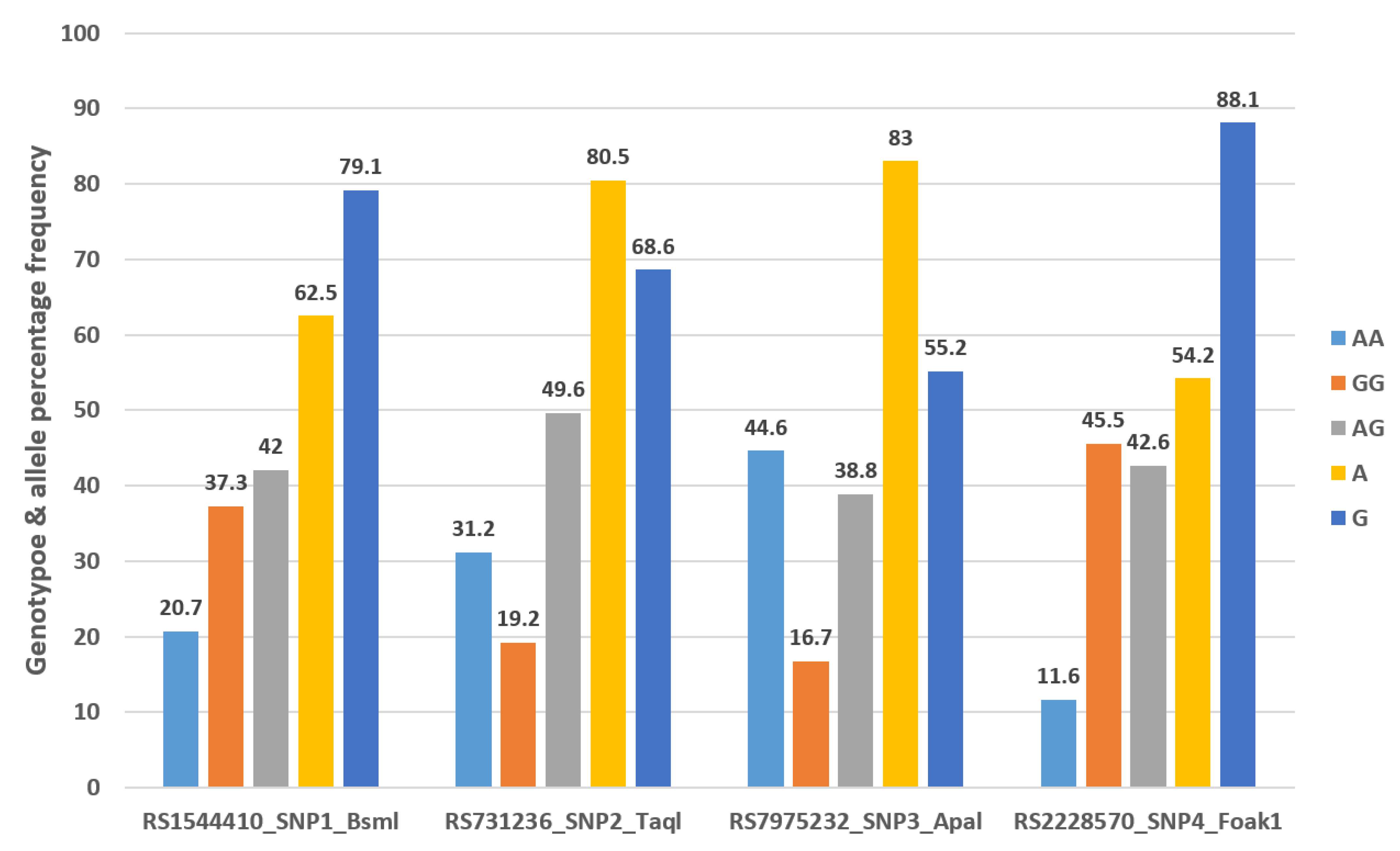
3.2. Distribution of four VDR Gene Polymorphisms in Group of 277 from Emirati Population
3.3. Vitamin D Concentrations According to Distribution and Presence or Absence of Genotypes and Alleles of Four VDR Gene Polymorphisms
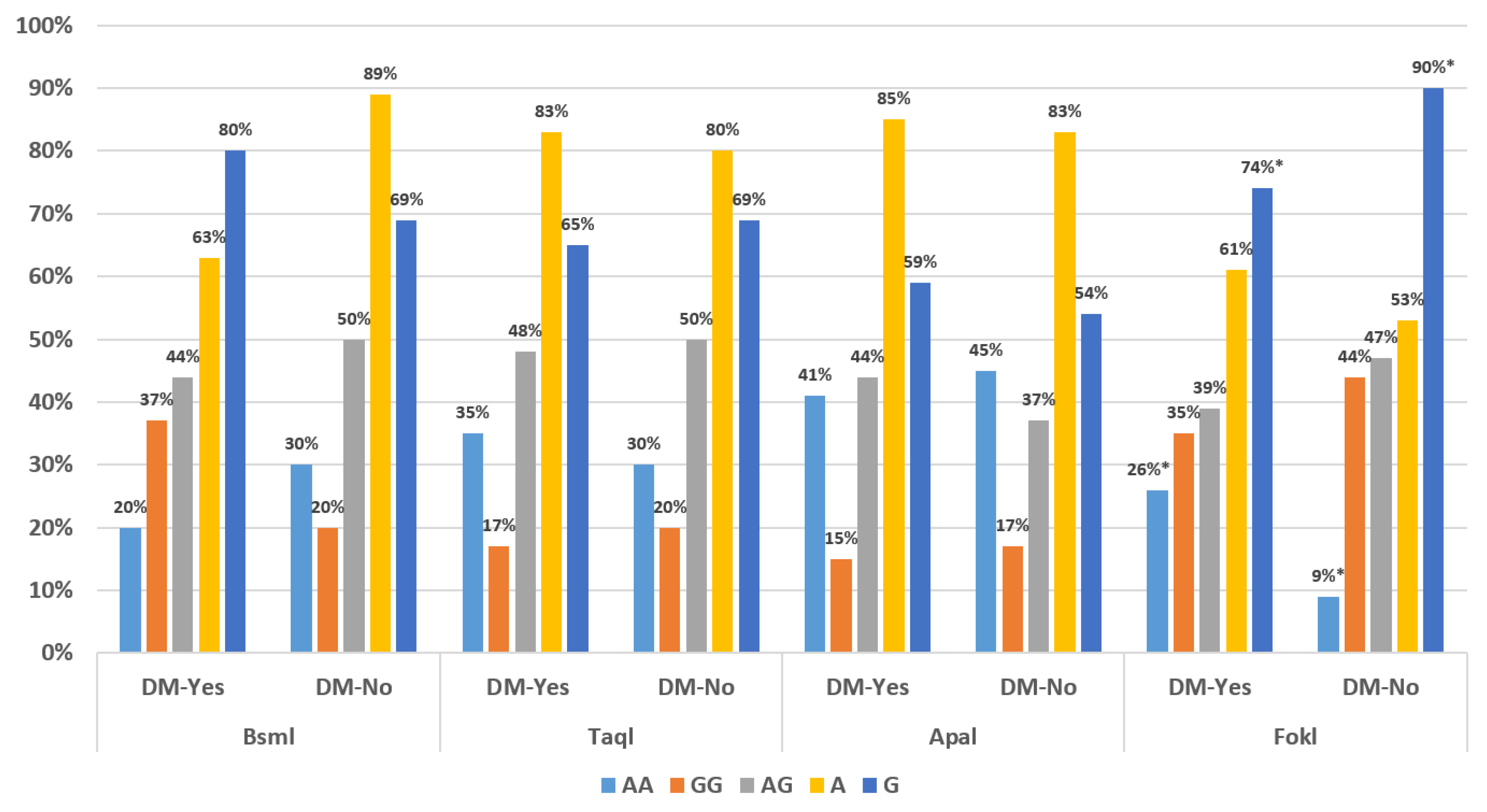
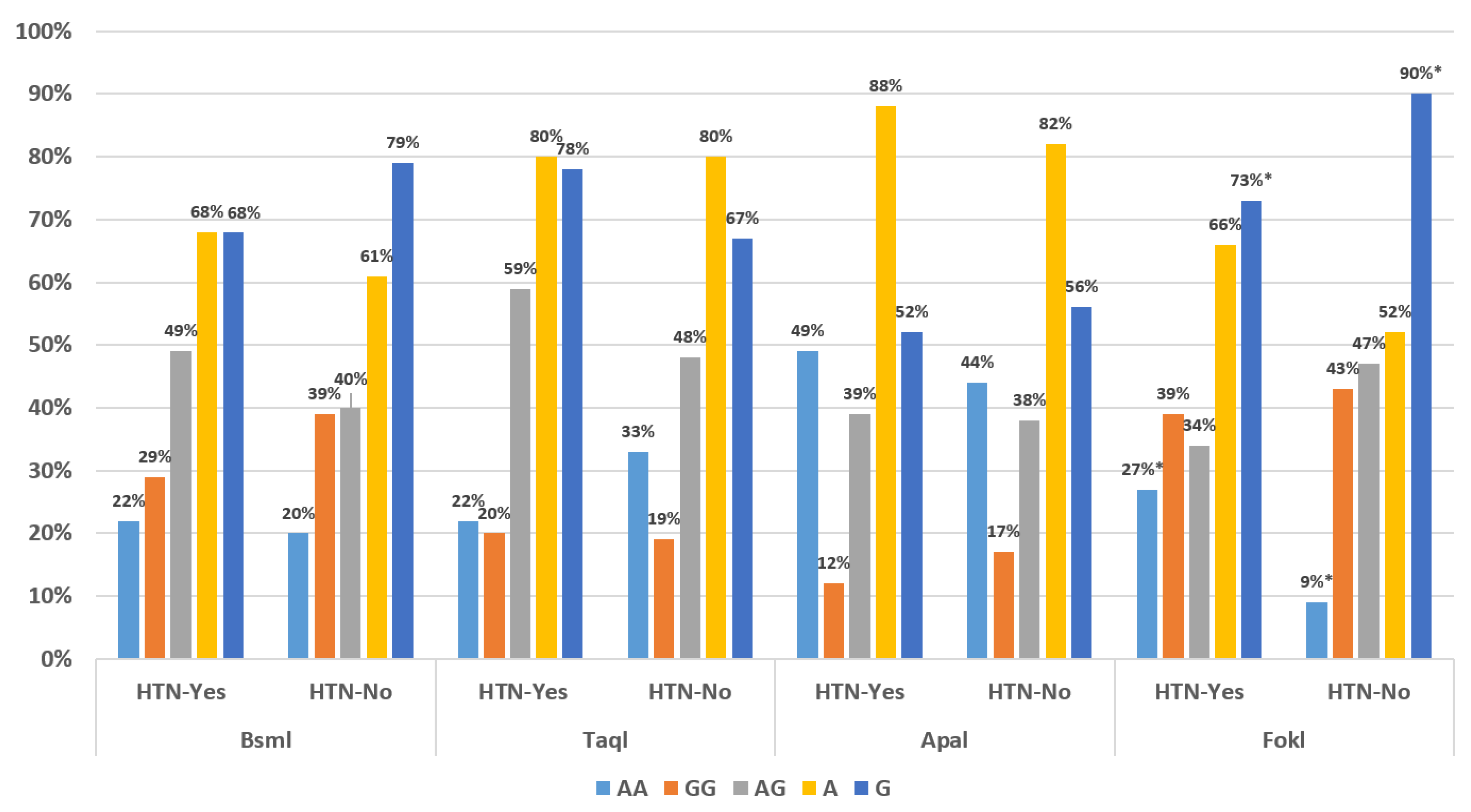
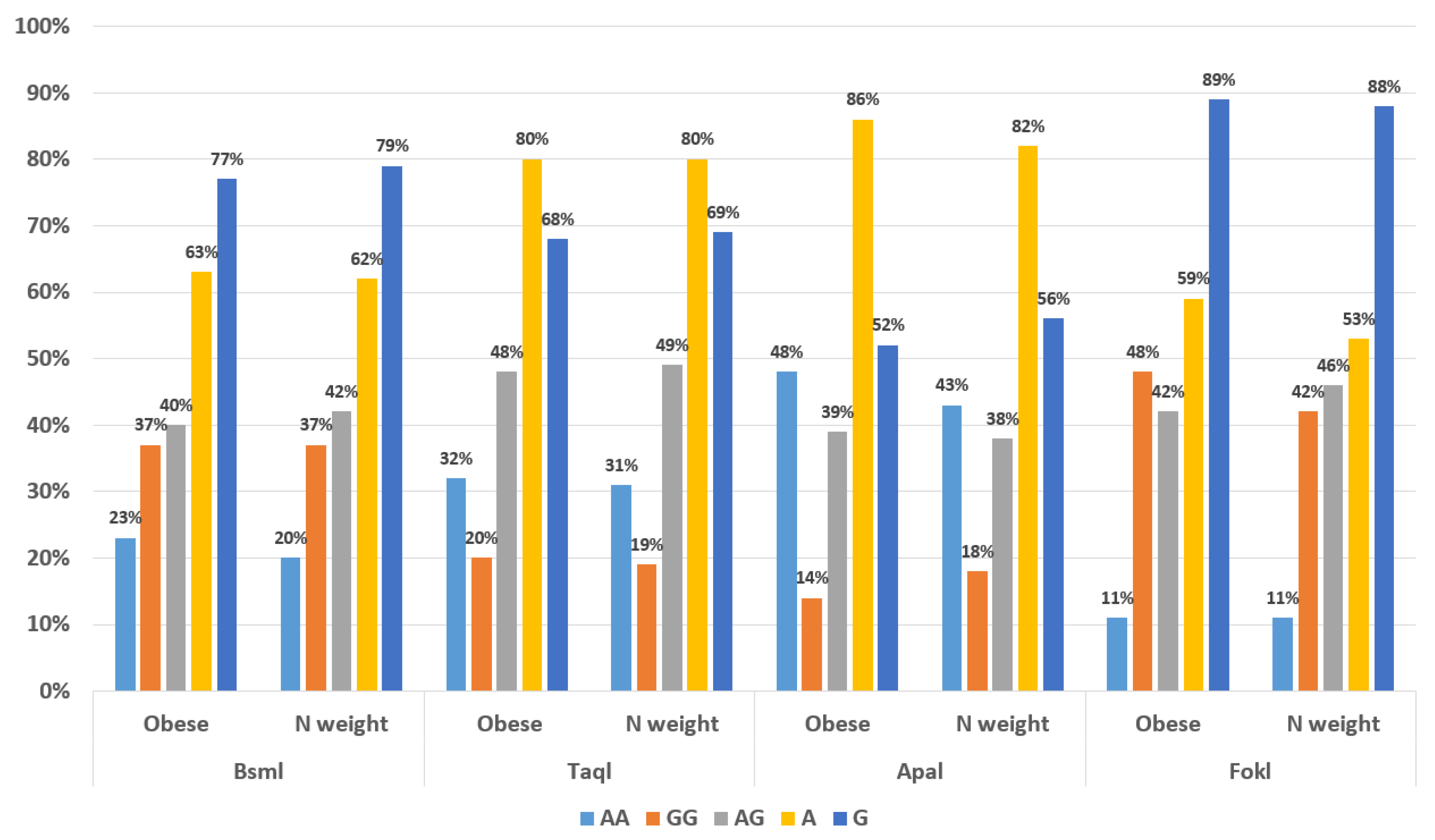
3.4. Genotype Distribution Based on Gender, BMI and Diabetes, Hypertension
4. Discussion
4.1. Genotypes and Allele Percentage Frequency Distribution Compared to Previous Studies
4.2. Vitamin D Concentrations According to the Presence or Absence of Genotypes and Allele Distribution of Four VDR Gene Polymorphism
4.3. The Prevalence of Vitamin D VDR Receptor Genotypes and Alleles in Subjects with Obesity, Diabetes Mellitus and Hypertension Compared to Those without These Conditions
4.4. Strengths and Weakness
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BMI = body mass index |
| CVS = cardiovascular disease |
| ECL = chemiluminescence |
| LDL = Low density lipoprotein |
| SNPs = single nucleotide polymorphism |
| T2DM = type 2 diabetes mellitus |
| UAE = United Arab Emirates |
| VDR = vitamin D receptor |
| MetS = metabolic syndrome |
References
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Uitterlinden, A.G.; Fang, Y.; Van Meurs, J.B.; Pols, H.A.; Van Leeuwen, J.P. Genetics and biology of vitamin D receptor polymorphisms. Gene 2004, 338, 143–156. [Google Scholar] [CrossRef] [PubMed]
- Rezende, V.B.; Barbosa, F.; Montenegro, M.F.; Sandrim, V.C.; Gerlach, R.F.; Tanus-Santos, J.E. An interethnic comparison of the distribution of vitamin D receptor genotypes and haplotypes. Clin. Chim. Acta 2007, 384, 155–159. [Google Scholar] [CrossRef]
- Qin, W.H.; Wang, H.X.; Qiu, J.L.; Huang, X.B.; Huang, Y.; Wu, N.R.; Liang, H.S. A meta-analysis of association of vitamin D receptor BsmI gene polymorphism with the risk of type 1 diabetes mellitus. J. Recept. Signal Transduct. Res. 2014, 34, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Al-Daghri, N.M.; Al-Attas, O.S.; Alkharfy, K.M.; Khan, N.; Mohammed, A.K.; Vinodson, B.; Ansari, M.G.A.; Alenad, A.; Alokail, M.S. Association of VDR-gene variants with factors related to the metabolic syndrome, type 2 diabetes and vitamin D deficiency. Gene 2014, 542, 129–133. [Google Scholar] [CrossRef]
- Mosaad, Y.M.; Hammad, E.M.; Fawzy, Z.; Aal, I.A.A.; Youssef, H.M.; ElSaid, T.O.; Monir, R.; El-Deek, B.S. Vitamin D receptor gene polymorphism as possible risk factor in rheumatoid arthritis and rheumatoid related osteoporosis. Hum. Immunol. 2014, 75, 452–461. [Google Scholar] [CrossRef]
- Neela, V.S.K.; Suryadevara, N.C.; Shinde, V.G.; Pydi, S.S.; Jain, S.; Jonnalagada, S.; Singh, S.S.; Valluri, V.L.; Anandaraj, M. Association of Taq I, Fok I and Apa I polymorphisms in Vitamin D Receptor (VDR) gene with leprosy. Hum. Immunol. 2015, 76, 402–405. [Google Scholar] [CrossRef]
- Bhanushali, A.A.; Lajpal, N.; Kulkarni, S.S.; Chavan, S.S.; Bagadi, S.S.; Das, B.R. Frequency of fokI and taqI polymorphism of vitamin D receptor gene in Indian population and its association with 25-hydroxyvitamin D levels. Indian J. Hum. Genet. 2009, 15, 108–113. [Google Scholar] [CrossRef]
- McKinsey Global Institute. Overcoming Obesity: An Initial Economic Analysis. 2021. Available online: http://www.mckinsey.com/insights/economic_studies/how_the_world_could_better_fight_obesity (accessed on 1 March 2023).
- Fu, J.; Han, L.; Zhao, Y.; Li, G.; Zhu, Y.; Li, Y.; Li, M.; Gao, S.; Willi, S.M. 25(OH) D levels are associated with metabolic syndrome in adolescents and young adults: The BCAMS study. Clin. Nutr. 2019, 38, 2161–2167. [Google Scholar] [CrossRef] [PubMed]
- Palaniswamy, S.; Gill, D.; De Silva, N.M.; Lowry, E.; Jokelainen, J.; Karhu, T.; Mutt, S.J.; Dehghan, A.; Sliz, E.; Chasman, D.I.; et al. Could vitamin D reduce obesity-associated inflammation? Observational and Mendelian randomization study. Am. J. Clin. Nutr. 2020, 111, 1036–1047. [Google Scholar] [CrossRef]
- Cade, C.; Norman, A.W. Vitamin D3 improves impaired glucose tolerance and insulin secretion in the vitamin D-deficient rat in vivo. Endocrinology 1986, 119, 84–90. [Google Scholar] [CrossRef]
- Earthman, C.P.; Beckman, L.M.; Masodkar, K.; Sibley, S.D. The link between obesity and low circulating 25-hydroxyvitamin D concentrations: Considerations and implications. Int. J. Obes. 2012, 36, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Wu, L.; Fan, Y.; Ma, J. Associations among Four Polymorphisms (BsmI, FokI, TaqI and ApaI) of Vitamin D Receptor Gene and End-stage Renal Disease: A Meta-Analysis. Arch. Med. Res. 2015, 46, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Osman, E.; Al Anouti, F.; El Ghazali, G.; Haq, A.; Mirgani, R.; Al Safar, H. Frequency of rs731236 (Taql), rs2228570 (Fok1) of Vitamin-D Receptor (VDR) gene in Emirati healthy population. Meta Gene 2015, 6, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A. Vitamin D deficiency in India: Prevalence, causalities and interventions. Nutrients 2014, 6, 729–775. [Google Scholar] [CrossRef]
- Saadi, H.F.; Nagelkerke, N.; Benedict, S.; Qazaq, H.S.; Zilahi, E.; Mohamadiyeh, M.K.; Al-Suhaili, A.I. Predictors and relationship of serum 25 hydroxyvitamin D concentration with bone turnover markers, bone mineral density and vitamin D receptor genotype in Emirati women. Bone 2006, 39, 1136–1143. [Google Scholar] [CrossRef] [PubMed]
- Holvik, K.; Meyer, H.E.; Søgaard, A.J.; Selmer, R.; Haug, E.; Falch, J.A. Biochemical markers of bone turnover and their relation to forearm bone mineral density in persons of Pakistani and Norwegian background living in Oslo, Norway: The Oslo Health Study. Eur. J. Endocrinol. 2006, 155, 693–699. [Google Scholar] [CrossRef]
- Lowe, N.M.; Mitra, S.R.; Foster, P.C.; Bhojani, I.; McCann, J.F. Vitamin D status and markers of bone turnover in Caucasian and Southy Asian postmenopausal women living in the UK. Br. J. Nutr. 2010, 103, 1706–1710. [Google Scholar] [CrossRef]
- Farrar, M.D.; Kift, R.; Felton, S.J.; Berry, J.L.; Durkin, M.T.; Allan, D.; Vail, A.; Webb, A.R.; Rhodes, L.E. Recommended summer sunlight exposure amounts fail to produce sufficient vitamin D status in UK adults of South Asian origin. Am. J. Clin. Nutr. 2011, 94, 1219–1224. [Google Scholar] [CrossRef] [PubMed]
- Saadi, H.F.; Dawodu, A.; Afandi, B.O.; Zayed, R.; Benedict, S.; Nagelkerke, N. Efficacy of daily and monthly high-dose calciferol in vitamin D–deficient nulliparous and lactating women. Am. J. Clin. Nutr. 2007, 85, 1565–1571. [Google Scholar] [CrossRef]
- Laaksonen, M.; Kärkkäinen, M.; Outila, T.; Vanninen, T.; Ray, C.; Lamberg-Allardt, C. Vitamin D receptor gene BsmI-polymorphism in Finnish premenopausal and postmenopausal women: Its association with bone mineral density, markers of bone turnover, and intestinal calcium absorption, with adjustment for lifestyle factors. J. Bone Miner. Metab. 2002, 20, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Gariballa, S.; Shah, I.; Yasin, J.; Alessa, A. Vitamin D [25f(OH)D] metabolites and epimers in obese subject: Interaction and correlations with adverse metabolic health risk factors. J. Steroid Biochem. Mol. Biol. 2022, 215, 106023. [Google Scholar] [CrossRef] [PubMed]
- Zmuda, J.M.; Cauley, J.A.; Danielson, M.E.; Wolf, R.L.; Ferrell, R.E. Vitamin D receptor gene polymorphisms, bone turnover, and rates of bone loss in older African-American women. J. Bone Miner. Res. 1997, 12, 1446–1452. [Google Scholar] [CrossRef]
- Abouzid, M.; Kruszyna, M.; Burchardt, P.; Kruszyna, Ł.; Główka, F.K.; Karaźniewicz-Łada, M. Vitamin D Receptor Gene Polymorphism and Vitamin D Status in Population of Patients with Cardiovascular Disease-A Preliminary Study. Nutrients 2021, 13, 3117. [Google Scholar] [CrossRef]
- Hasan, H.A.; Ra’ed, O.A.; Muda, W.A.M.B.W.; Mohamed, H.J.B.J.; Samsudin, A.R. Association of Vitamin D receptor gene polymorphisms with metabolic syndrome and its components among adult Arabs from the United Arab Emirates. Diabetes Metab. Syndr. 2017, 11 (Suppl. S2), S531–S537. [Google Scholar] [CrossRef]
- Al Safar, H.; Chehadeh, S.E.H.; Abdel-Wareth, L.; Haq, A.; Jelinek, H.F.; ElGhazali, G.; Al Anouti, F. Vitamin D receptor gene polymorphisms among Emirati patients with type 2 diabetes mellitus. J. Steroid Biochem. Mol. Biol. 2018, 175, 119–124. [Google Scholar] [CrossRef]
- Li, L.; Wu, B.; Liu, J.Y.; Yang, L.B. Vitamin D receptor gene polymorphisms and type 2 diabetes: A meta-analysis. Arch. Med. Res. 2013, 44, 235–241. [Google Scholar] [CrossRef]
- Al-Hazmi, A.S.; Al-Mehmadi, M.M.; Al-Bogami, S.M.; Shami, A.A.; Al-Askary, A.A.; Alomery, A.M.; Al-Shehri, S.S.; Dahlawi, H.; Abdulrazag, K.; Ali, T.; et al. Vitamin D receptor gene polymorphisms as a risk factor for obesity in Saudi men. Electron. Physician 2017, 9, 5427–5433. [Google Scholar] [CrossRef] [PubMed]
- Rashidi, F.; Ostadsharif, M. Association of VDR gene Apal polymorphism with obesity in Iranian population. Biomedica 2021, 41, 651–659. [Google Scholar] [CrossRef]
- Younes, S.; Ibrahim, A.; Al-Jurf, R.; Zayed, H. Genetic polymorphisms associated with obesity in the Arab world: A systematic review. Int. J. Obes. 2021, 45, 1899–1913. [Google Scholar] [CrossRef]
- Sahakyan, K.R.; Somers, V.K.; Rodriguez-Escudero, J.P.; Hodge, D.O.; Carter, R.E.; Sochor, O.; Coutinho, T.; Jensen, M.D.; Roger, V.L.; Singh, P.; et al. Normal-Weight Central Obesity: Implications for Total and Cardiovascular Mortality. Ann. Intern. Med. 2015, 163, 827–835. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Baseline Clinical, Anthropometric and Metabolic Characteristics of the Study Population | Mean (SD) Unless Otherwise Stated (n = 277) |
|---|---|---|
| Age (years) | 41 (12) | |
| Sex, female n (%) | 204 (74) | |
| Smoking n (%) | ||
| Current | 35 (13) | |
| Ex-smoker | 12 (4) | |
| Never smoked | 225 (81) | |
| Body mass index (BMI) n (%) | ||
| Normal weight (BMI 18.5–25) | 65 (24) | |
| Overweight (BMI 25.1–29.9) | 93 (34) | |
| Obese (BMI ≥ 30) | 108 (39) | |
| Physical activity n (%) | ||
| Not active | 32 (12) | |
| Moderately active | 146 (53) | |
| Very active | 96 (35) | |
| Diabetes n (%) | 46 (17) | |
| Hypertension n (%) | 41 (15) | |
| Hs CRP (mg/L) * | 3.5 mg (3) | |
| Glucose (mmol/L) * | 6.3 (2.5) | |
| Total cholesterol (mmol/L) * | 4.9 (0.9) | |
| Urea (mmol/L) * | 4.1 (1.5) |
| AA | GG | AG | p Value | |
|---|---|---|---|---|
| RS1544410_SNP1_Bsml | 24.5 (11) | 22.1 (11) | 23.9 (10) | 0.046 |
| RS731236_SNP2_Taql | 22.0 (11) | 24.0 (11) | 23.9 (10) | 0.054 |
| RS7975232_SNP3_Apal | 25.0 (11) | 22.3 (11) | 21.7 (9) | 0.008 |
| RS2228570_SNP4_Foak1 | 24.0 (10) | 23.9 (12) | 22.6 (9) | 0.007 |
| AA | GG | AG | A | G | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Yes | No | Yes | No | Yes | No | Yes | No | Yes | No | |
| RS1544410_SNP1_Bsml | 25.5 (11) | 23.2 (10) | 22.1 (11) | 24.2 (10) | 23.9 (10) | 23.1 (11) | 23.9 (10) | 22.7 (12) | 23.0 (10) | 25.0 (12) |
| RS731236_SNP2_Taql | 22.0 (11) | 24.1 (10) | 24.0 (11) | 23.3 (11) | 23.9 (10) | 23.0 (11) | 23.2 (11) | 24.5 (11) | 23.9 (11) | 22.3 (11) |
| RS7975232_SNP3_Apal | 25.1 (11) | 22.1 * (10) | 22.3 (11) | 23.7 (11) | 21.7 (9) | 24.5 * (11) | 23.6 (10) | 22.9 (12) | 21.9 (10) | 25.3 * (12) |
| RS2228570_SNP4_Foak1 | 23.9 (10) | 23.4 (11) | 22.6 (9) | 24.1 (11) | 23.9 (12) | 23.0 (10) | 22.9 (10) | 24.1 (12) | 23.3 (11) | 24.6 (11) |
| Standardized Coefficients B | Standard Error | p Value | Exp (B) | 95.0% Confidence Interval for B | ||
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| Age (years) | 0.018 | 0.008 | 0.022 | 1.018 | 1.003 | 1.034 |
| Gender (male/female) | −0.763 | 0.241 | 0.002 | 0.466 | 0.291 | 0.748 |
| BMI | −0.006 | 0.008 | 0.443 | 0.994 | 0.978 | 1.010 |
| Sun exposure | 0.009 | 0.044 | 0.838 | 1.009 | 0.926 | 1.099 |
| Diet | 0.010 | 0.036 | 0.782 | 1.010 | 0.941 | 1.083 |
| Physical activity | 0.050 | 0.154 | 0.748 | 1.051 | 0.777 | 1.422 |
| Smoking | 0.071 | 0.142 | 0.616 | 1.074 | 0.813 | 1.417 |
| RS1544410_SNP1_Bsm | 0.179 | 0.146 | 0.221 | 1.196 | 0.898 | 1.593 |
| RS731236_SNP2_Taql | −0.067 | 0.127 | 0.598 | 0.935 | 0.730 | 1.199 |
| RS7975232_SNP3_Apal | −0.079 | 0.064 | 0.217 | 0.924 | 0.815 | 1.047 |
| RS2228570_SNP4_ | −0.156 | 0.144 | 0.279 | 0.855 | 0.645 | 1.135 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gariballa, S.; Al-Bluwi, G.S.M.; Yasin, J. Frequency of Vitamin D Receptor Gene Polymorphisms in a Population with a very High Prevalence of Vitamin D Deficiency, Obesity, Diabetes and Hypertension. Biomedicines 2023, 11, 1202. https://doi.org/10.3390/biomedicines11041202
Gariballa S, Al-Bluwi GSM, Yasin J. Frequency of Vitamin D Receptor Gene Polymorphisms in a Population with a very High Prevalence of Vitamin D Deficiency, Obesity, Diabetes and Hypertension. Biomedicines. 2023; 11(4):1202. https://doi.org/10.3390/biomedicines11041202
Chicago/Turabian StyleGariballa, Salah, Ghada S. M. Al-Bluwi, and Javed Yasin. 2023. "Frequency of Vitamin D Receptor Gene Polymorphisms in a Population with a very High Prevalence of Vitamin D Deficiency, Obesity, Diabetes and Hypertension" Biomedicines 11, no. 4: 1202. https://doi.org/10.3390/biomedicines11041202