
A Systematic Review and Meta-Analysis of the Incidence and Risk Factors for Major Adverse Cardiovascular Events in Patients with Unrepaired Abdominal Aortic Aneurysms
 , ,
, , 
Abstract
:1. Introduction
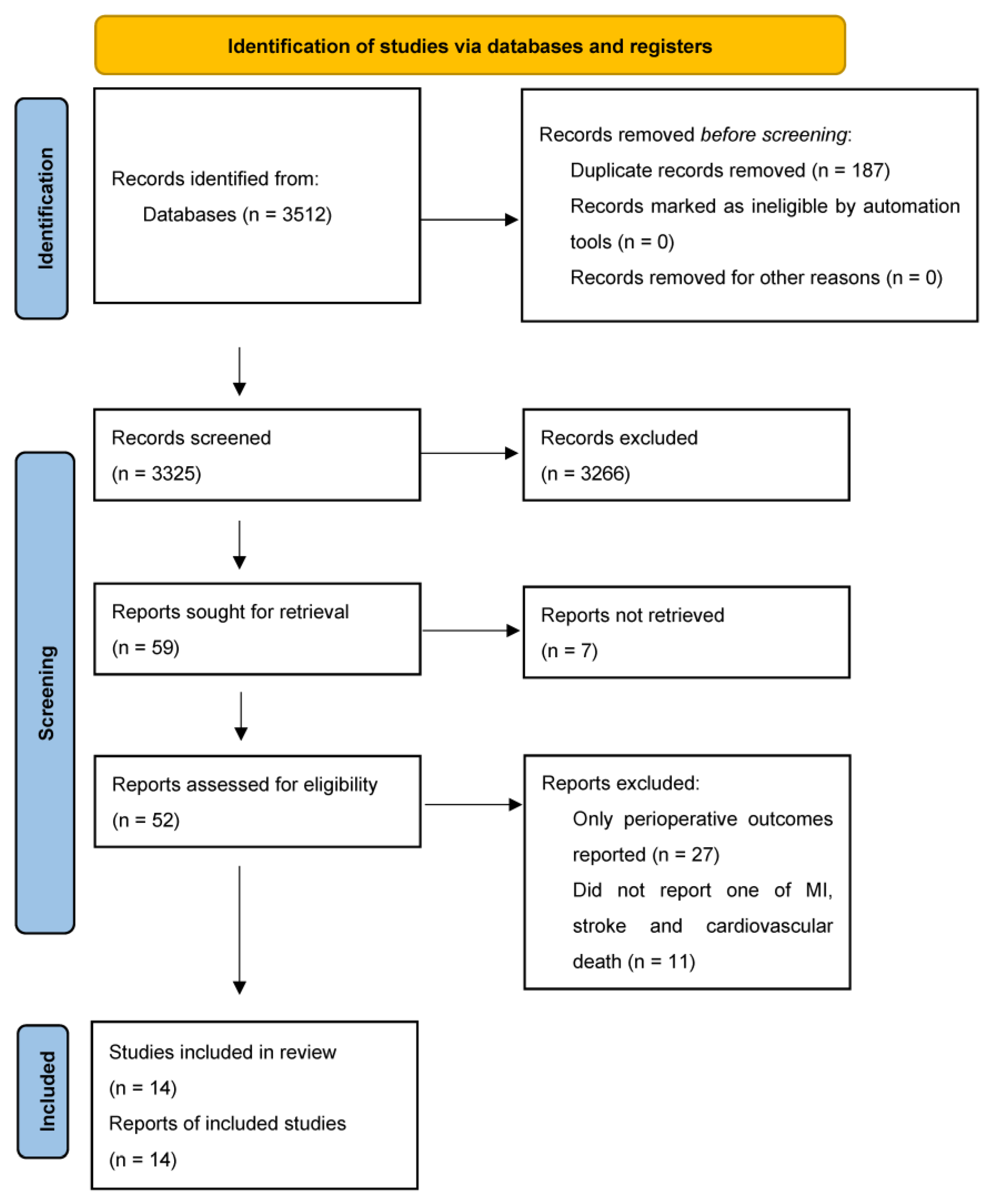
2. Methods
2.1. Search Strategy
2.2. Data Extraction and Outcomes
2.3. Quality Assessment
2.4. Data Analysis
3. Results
3.1. Characteristics of Studies and Included Participants
3.2. Risk of Bias of Included Studies
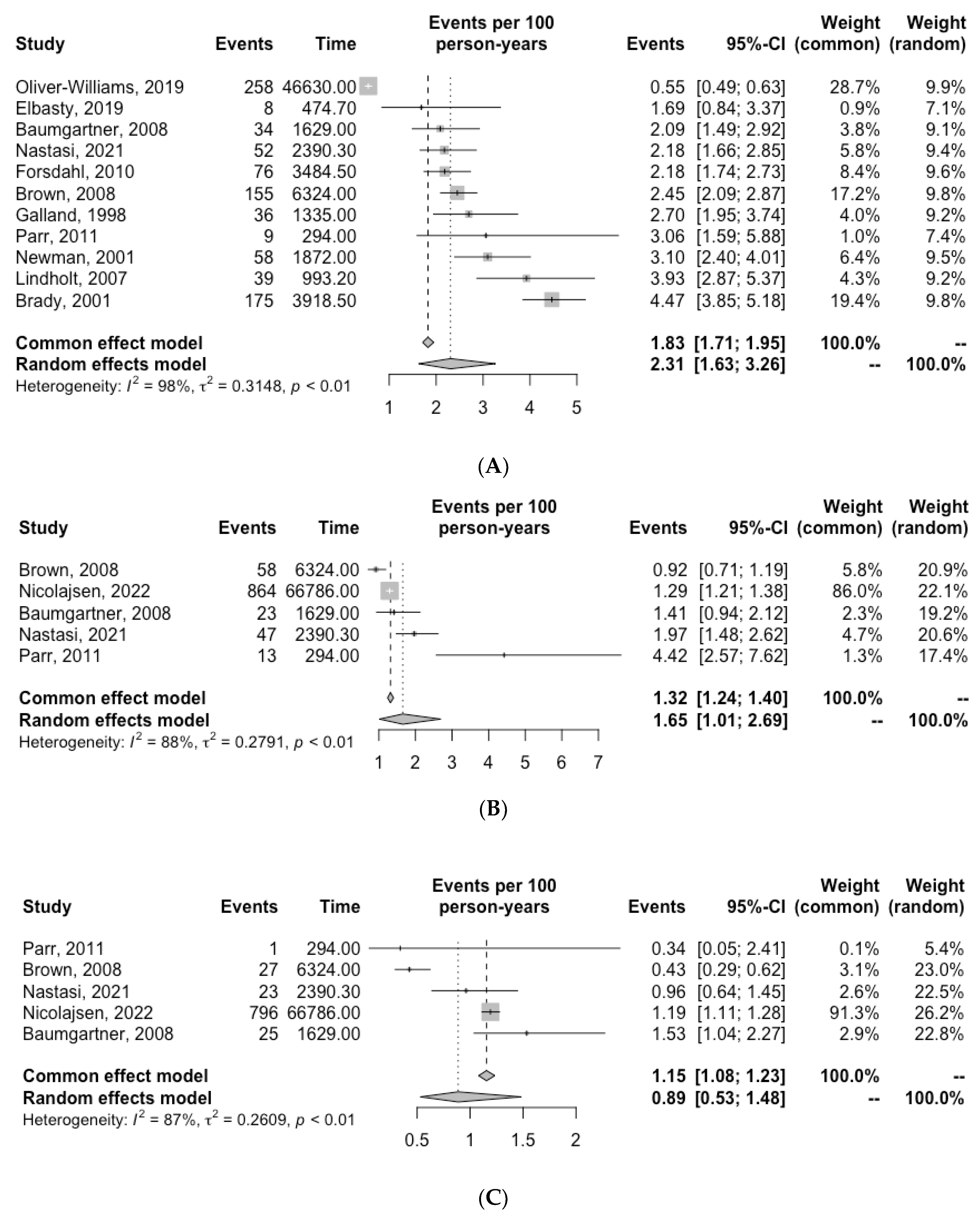
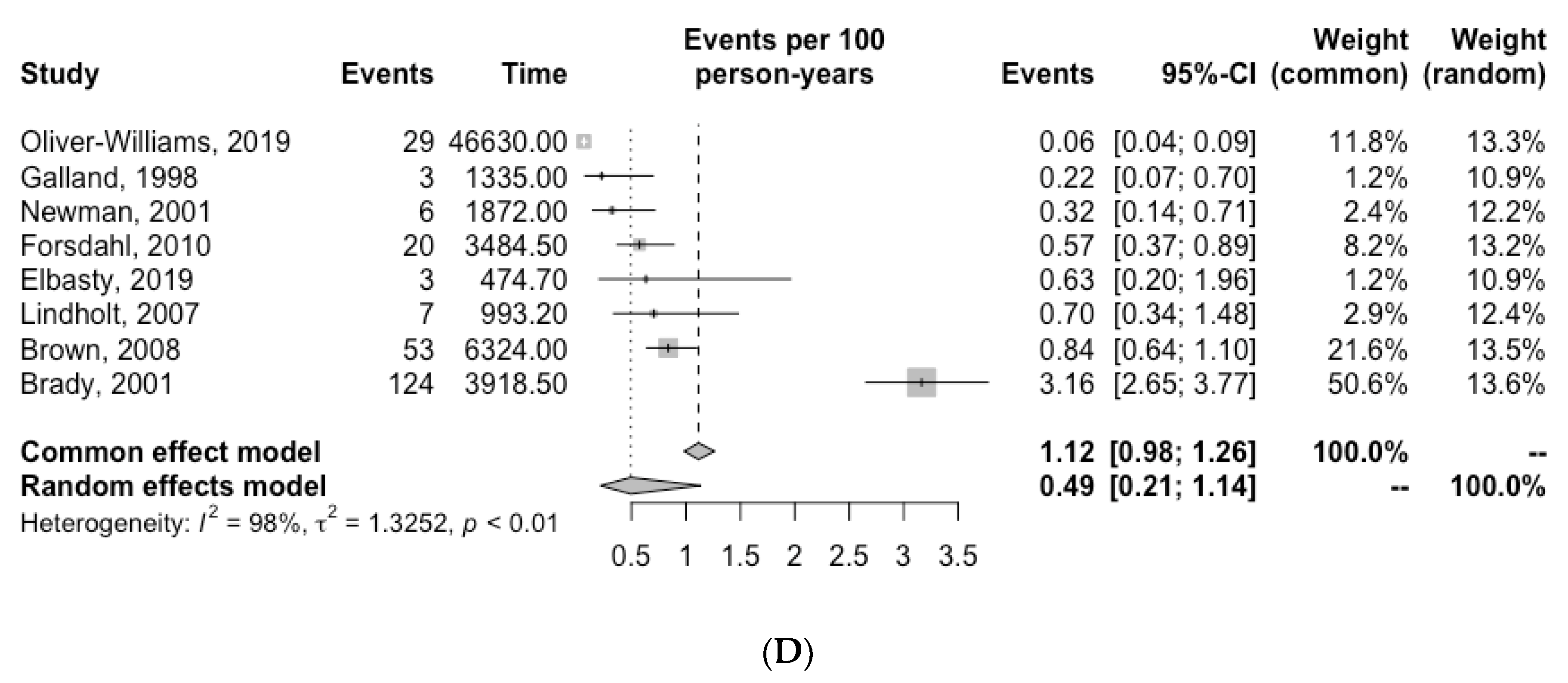
3.3. Incidence of Cardiovascular Death, MI and Stroke
3.4. Risk Factors for Events
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Golledge, J. Abdominal aortic aneurysm: Update on pathogenesis and medical treatments. Nat. Rev. Cardiol. 2019, 16, 225–242. [Google Scholar] [CrossRef] [PubMed]
- Wanhainen, A.; Verzini, F.; Van Herzeele, I.; Allaire, E.; Bown, M.; Cohnert, T.; Dick, F.; van Herwaarden, J.; Karkos, C.; Koelemay, M.; et al. Editor’s Choice—European Society for Vascular Surgery (ESVS) 2019 Clinical Practice Guidelines on the Management of Abdominal Aorto-iliac Artery Aneurysms. Eur. J. Vasc. Endovasc. Surg. 2019, 57, 8–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aboyans, V.; Guessous, I.; Leclerc, A.; Lacroix, P. From guidelines for screening to their (poor) implementation: The case of the abdominal aortic aneurysm. Rev. Med. Suisse 2010, 6, 1405–1409. [Google Scholar] [PubMed]
- Guirguis-Blake, J.M.; Beil, T.L.; Senger, C.A.; Coppola, E.L. Primary Care Screening for Abdominal Aortic Aneurysm: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2019, 322, 2219–2238. [Google Scholar] [CrossRef] [Green Version]
- Bath, M.F.; Gokani, V.J.; Sidloff, D.A.; Jones, L.R.; Choke, E.; Sayers, R.D.; Bown, M.J. Systematic review of cardiovascular disease and cardiovascular death in patients with a small abdominal aortic aneurysm. Br. J. Surg. 2015, 102, 866–872. [Google Scholar] [CrossRef]
- Nastasi, D.R.; Norman, R.; Moxon, J.V.; Quigley, F.; Velu, R.; Jenkins, J.; Golledge, J. The Potential Benefits and Costs of an Intensified Approach to Low Density Lipoprotein Cholesterol Lowering in People with Abdominal Aortic Aneurysm. Eur. J. Vasc. Endovasc. Surg. 2021, 62, 643–650. [Google Scholar] [CrossRef]
- Parr, A.; McCann, M.; Bradshaw, B.; Shahzad, A.; Buttner, P.; Golledge, J. Thrombus volume is associated with cardiovascular events and aneurysm growth in patients who have abdominal aortic aneurysms. J. Vasc. Surg. 2011, 53, 28–35. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Singh, T.P.; Wong, S.A.; Moxon, J.V.; Gasser, T.C.; Golledge, J. Systematic review and meta-analysis of the association between intraluminal thrombus volume and abdominal aortic aneurysm rupture. J. Vasc. Surg. 2019, 70, 2065–2073.e2010. [Google Scholar] [CrossRef]
- Oliver-Williams, C.; Sweeting, M.J.; Jacomelli, J.; Summers, L.; Stevenson, A.; Lees, T.; Earnshaw, J.J. Safety of Men With Small and Medium Abdominal Aortic Aneurysms Under Surveillance in the NAAASP. Circulation 2019, 139, 1371–1380. [Google Scholar] [CrossRef]
- Elbasty, A.; Nickinson, A.T.O.; Delaney, C.; Stather, P.W.; Burrows, M.; Delbridge, M.; Al-Jundi, W. Outcomes of Sub-threshold Abdominal Aortic Aneurysms Undergoing Surveillance in Patients Aged 85 Years or Over. Eur. J. Vasc. Endovasc. Surg. 2019, 58, 357–361. [Google Scholar] [CrossRef] [PubMed]
- Forsdahl, S.H.; Solberg, S.; Singh, K.; Jacobsen, B.K. Abdominal aortic aneurysms, or a relatively large diameter of non-aneurysmal aortas, increase total and cardiovascular mortality: The Tromso study. Int. J. Epidemiol. 2010, 39, 225–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, L.C.; Thompson, S.G.; Greenhalgh, R.M.; Powell, J.T.; Participants, U.K.S.A.T. Fit patients with small abdominal aortic aneurysms (AAAs) do not benefit from early intervention. J. Vasc. Surg. 2008, 48, 1375–1381. [Google Scholar] [CrossRef] [Green Version]
- Baumgartner, I.; Hirsch, A.T.; Abola, M.T.B.; Cacoub, P.P.; Poldermans, D.; Steg, P.G.; Creager, M.A.; Bhatt, D.L.; Investigators, R.R. Cardiovascular risk profile and outcome of patients with abdominal aortic aneurysm in out-patients with atherothrombosis: Data from the Reduction of Atherothrombosis for Continued Health (REACH) Registry. J. Vasc. Surg. 2008, 48, 808–814. [Google Scholar] [CrossRef] [Green Version]
- Newman, A.B.; Arnold, A.M.; Burke, G.L.; O’Leary, D.H.; Manolio, T.A. Cardiovascular disease and mortality in older adults with small abdominal aortic aneurysms detected by ultrasonography: The cardiovascular health study. Ann. Intern. Med. 2001, 134, 182–190. [Google Scholar] [CrossRef]
- Galland, R.B.; Whiteley, M.S.; Magee, T.R. The fate of patients undergoing surveillance of small abdominal aortic aneurysms. Eur. J. Vasc. Endovasc. Surg. 1998, 16, 104–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, K.J.; Yoo, J.H.; Cho, H.J.; Kim, M.H.; Jun, K.W.; Han, K.D.; Hwang, J.K. The Impact of Abdominal Aortic Aneurysm on Cardiovascular Diseases. Int. Heart J. 2021, 62, 1235–1240. [Google Scholar] [CrossRef] [PubMed]
- Nicolajsen, C.W.; Søgaard, M.; Eldrup, N.; Jensen, M.; Larsen, T.B.; Goldhaber, S.Z.; Nielsen, P.B. Temporal trends in abdominal aortic aneurysmal disease: A nationwide cohort study on cardiovascular morbidity and medical cardioprotective therapy. Eur. J. Prev. Cardiol. 2022, 29, 1957–1964. [Google Scholar] [CrossRef]
- Takigawa, M.; Yoshimuta, T.; Akutsu, K.; Takeshita, S.; Yokoyama, N. Prevalence and predictors of coexistent silent atherosclerotic cardiovascular disease in patients with abdominal aortic aneurysm without previous symptomatic cardiovascular diseases. Angiology 2012, 63, 380–385. [Google Scholar] [CrossRef]
- Lindholt, J.S. Relatively high pulmonary and cardiovascular mortality rates in screening-detected aneurysmal patients without previous hospital admissions. Eur. J. Vasc. Endovasc. Surg. 2007, 33, 94–99. [Google Scholar] [CrossRef] [Green Version]
- Brady, A.R.; Fowkes, F.G.; Thompson, S.G.; Powell, J.T. Aortic aneurysm diameter and risk of cardiovascular mortality. Arter. Thromb. Vasc. Biol. 2001, 21, 1203–1207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mortality results for randomised controlled trial of early elective surgery or ultrasonographic surveillance for small abdominal aortic aneurysms. Lancet 1998, 352, 1649–1655. [CrossRef]
- Amini, M.; Zayeri, F.; Salehi, M. Trend analysis of cardiovascular disease mortality, incidence, and mortality-to-incidence ratio: Results from global burden of disease study 2017. BMC Public Health 2021, 21, 401. [Google Scholar] [CrossRef] [PubMed]
- Golledge, J. Update on the pathophysiology and medical treatment of peripheral artery disease. Nat. Rev. Cardiol. 2022, 19, 456–474. [Google Scholar] [CrossRef]
- Baigent, C.; Blackwell, L.; Collins, R.; Emberson, J.; Godwin, J.; Peto, R.; Buring, J.; Hennekens, C.; Kearney, P.; Meade, T. Aspirin in the primary and secondary prevention of vascular disease: Collaborative meta-analysis of individual participant data from randomised trials. Lancet 2009, 373, 1849–1860. [Google Scholar]
- Cannon, C.P.; Steinberg, B.A.; Murphy, S.A.; Mega, J.L.; Braunwald, E. Meta-analysis of cardiovascular outcomes trials comparing intensive versus moderate statin therapy. J. Am. Coll. Cardiol. 2006, 48, 438–445. [Google Scholar] [CrossRef] [Green Version]
- Bahia, S.S.; Vidal-Diez, A.; Seshasai, S.R.K.; Shpitser, I.; Brownrigg, J.R.; Patterson, B.O.; Ray, K.K.; Holt, P.J.; Thompson, M.M.; Karthikesalingam, A. Cardiovascular risk prevention and all-cause mortality in primary care patients with an abdominal aortic aneurysm. Br. J. Surg. 2016, 103, 1626–1633. [Google Scholar] [CrossRef]
- Lloyd, G.M.; Newton, J.D.; Norwood, M.G.A.; Franks, S.C.; Bown, M.J.; Sayers, R.D. Patients with abdominal aortic aneurysm: Are we missing the opportunity for cardiovascular risk reduction? J. Vasc. Surg. 2004, 40, 691–697. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Reference | N | Age, Mean ± SD | Male Gender (%) | Nationality | AAA Diameter (mm), Mean ± SD | Hypertension (%) | Diabetes (%) | Ever Smoked (%) | Current Smoker (%) | Statins (%) | Aspirin (%) | sBP, Mean ± SD | dBP, Mean ± SD | LDL-c, Mean ± SD |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Nicolajsen, 2022 [18] | 33,393 | 73.6 @ | 25,353 (75.9) | Danish | NR | 27.3 | 7.7 | NR | NR | 54.8 # | 60.8 ^# | NR | NR | NR |
| Nastasi, 2021 [6] | 583 | 73.5 (67.8–78.3) * | 476 (82.0) | Australian | 42 (36.0–48.0) * | 77.4 | 24.2 | 85.2 | NR | 70.5 | 66.6 ^ | NR | NR | 2.4 (1.8–3.0) * |
| Ko, 2021 [17] | 10,822 | 63.9 ± 11.7 | 6925 (64.0) | Korean | NR | 73.8 | 18.1 | 49.4 | 27.1 | NR | NR | 127.89 ± 16.6 | 78.3 ± 10.9 | 3.0 ± 1.3 |
| Oliver-Williams, 2019 [10] | 18,652 | 66.8 ° | 18,652 (100.0) | British | NR | NR | NR | 89.8 | 35 | 62.4 | 39.5 | 142.3 ° | 83.0 ° | NR |
| Elbasty, 2019 [11] | 101 | 85–89 $ | 88 (87.1) | British | 45 ± 9.2 | 55.5 | 14.9 | 48.5 | NR | 85.1 | 51.5 | NR | NR | NR |
| Takigawa, 2012 [19] | 157 | 72.7 ± 7.5 | 128 (82.0) | Japanese | 50.1 ± 8.8 | 77.0 | 11.0 | 77.0 | NR | 31.0 | NR | 137.5 ± 16.2 | 75.6 ± 10.4 | 3.4 ± 0.9 |
| Parr, 2011 [7] | 98 | 73 (67–77) * | 75 (76.5) | Australian | 47.2 (34.9–54.6) * | 76.5 | 20.4 | 87.8 | NR | 66.3 | 63.3 | NR | NR | NR |
| Forsdahl, 2010 [12] | 345 | NR | NR | Norwegian | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| Brown, 2008 ! [13] | 527 | 69.2 ± 4.4 | 434 (82.0) | British | 46.1 ± 3.7 | 40.0 | 3.0 | 94.0 | 34.0 | NR | 29.0 | 156.7 ± 26.6 | NR | NR |
| Baumgartner, 2008 [14] | 1722 | 73.4 ±7.8 | 1389 (80.7) | Multinational ∍ | NR | 83.5 | 29.4 | 81.0 | 20.9 | 71.2 | 65.2 | 135.9 ± 19.0 | 76.2 ± 11.2 | NR |
| Lindholt, 2007 [20] | 191 | 65.3–70.7 * | 191 (100.0) | Danish | 31–41 * | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| Newman, 2001 [15] | 416 | 75 (65–93) * | 252 (61.0) | American | NR | 45.0 | 10.0 | NR | 14.7 | NR | NR | NR | NR | NR |
| Brady, 2001 [21] | 2305 | NR | NR | British | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| Galland, 1998 [16] | 267 | NR | NR | British | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR |
| Weighted average | - | 70.1 | 81.0 | - | 43.9 | 41.1 | 11.1 | 75.7 | 27.4 | 58.1 | 53.5 | 136.9 | 80.9 | 3.0 |
| Reference | Objective Defined | Study Design | Sample Size Estimation | Unrepaired AAA | MACE Reporting | Primary Outcome | Participant Characteristics | Follow Up | Statistical Methods | Total | Percentage | Risk of Bias |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Nicolajsen, 2022 [18] | 2 | 1 | 0 | 0 | 1 | 0 | 2 | 1 | 2 | 9 | 50.0% | Moderate |
| Nastasi, 2021 [6] | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 2 | 2 | 16 | 88.9% | Low |
| Ko, 2021 [17] | 2 | 1 | 0 | 0 | 1 | 1 | 2 | NR | 2 | 9 | 50.0% | Moderate |
| Oliver-Williams, 2019 [10] | 2 | 2 | 0 | 2 | 0 | 2 | 1 | 2 | 1 | 12 | 66.7% | Moderate |
| Elbasty, 2019 [11] | 2 | 2 | 0 | 2 | 1 | 2 | 2 | 2 | 0 | 13 | 72.2% | Low |
| Takigawa, 2012 [19] | 2 | 1 | 0 | 0 | 1 | 1 | 2 | NR | 2 | 9 | 50.0% | Moderate |
| Parr, 2011 [7] | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 1 | 2 | 15 | 83.3% | Low |
| Forsdahl, 2010 [12] | 2 | 2 | 0 | 2 | 0 | 2 | 0 | 2 | 2 | 12 | 66.7% | Moderate |
| Brown, 2008 [13] | 2 | 2 | 0 | 2 | 2 | 2 | 0 | 2 | 1 | 13 | 72.2% | Low |
| Baumgartner, 2008 [14] | 2 | 2 | 0 | 0 | 2 | 2 | 2 | 1 | 1 | 12 | 66.7% | Moderate |
| Lindholt, 2007 [20] | 2 | 1 | 0 | 0 | 0 | 1 | 0 | 2 | 1 | 7 | 38.9% | High |
| Newman, 2001 [15] | 2 | 2 | 0 | 2 | 0 | 2 | 2 | 2 | 1 | 13 | 72.2% | Low |
| Brady, 2001 [21] | 2 | 1 | 0 | 2 | 2 | 2 | 0 | 1 | 2 | 12 | 66.7% | Moderate |
| Galland, 1998 [16] | 2 | 2 | 0 | 2 | 2 | 2 | 0 | 2 | 0 | 12 | 66.7% | Moderate |
| Study | N | Duration of Follow Up (years) | MI, n (%) | Stroke, n (%) | CV Death, n (%) | AAA Rupture, n (%) | Surgery Related Death, n (%) | Total AAA Death, n (%) | All Cause Mortality, n (%) |
|---|---|---|---|---|---|---|---|---|---|
| Nicolajsen, 2022 [18] | 33,393 | 2.0 | 864 (2.6) | 796 (2.4) | NR | NR | NR | NR | 8404 (25.2) |
| Nastasi, 2021 [6] | 583 | 4.1 | 47 (8.1) | 23 (3.9) | 52 (8.9) | NR | NR | NR | NR |
| Ko, 2021 ! [17] | 10,822 | NR | NR | NR | 793 (7.3) | NR | NR | NR | 1677 (15.5) |
| Oliver-Williams, 2019 [10] | 18,652 | 2.5 | NR | NR | 258 (1.4) | 31 (0.2) | NR | 29 (0.2) | 980 (5.3) |
| Elbasty, 2019 [11] | 101 | 4.7 | NR | NR | 8 (7.9) | 2 (2.0) | 1 (1.0) | 3 (3.0) | 26 (25.7) |
| Takigawa, 2012 * [19] | 157 | NR | 46 (29.3) | 40 (25.5) | NR | NR | NR | NR | NR |
| Parr, 2011 [7] | 98 | 3.0 | 13 (13.3) | 1 (1.0) | 9 (9.2) | NR | NR | NR | NR |
| Forsdahl, 2010 [12] | 345 | 10.1 | NR | NR | 76 (22.0) | NR | NR | 20 (5.5) | 130 (36.0) |
| Brown, 2008 @ [13] | 527 | 12.0 | 58 (11.0) | 27 (5.1) | 155 (29.4) | 23 (4.4) | 30 (5.7) | 53 (10.1) | 352 (66.8) |
| Baumgartner, 2008 # [14] | 1629 * | 1.0 | 23 (1.4) | 25 (1.5) | 34 (2.1) | NR | NR | NR | NR |
| Lindholt, 2007 [20] | 191 | 5.2 | NR | NR | 39 (20.4) | NR | NR | 7 (3.7) | 49 (25.7) |
| Newman, 2001 [15] | 416 | 4.5 | NR | NR | 58 (13.9) | 6 (1.4) | NR | 6 (1.4) | 110 (26.4) |
| Brady, 2001 [21] | 2305 | 1.7 | NR | NR | 175 (7.6) | 40 (1.7) | 84 (3.6) | 40 (1.7) | 259 (11.2) |
| Galland, 1998 [16] | 267 | 5.0 | NR | NR | 36 (13.5) | 1 (0.4) | 2 (0.8) | 3 (1.1) | NR |
| Study Omitted | Incidence Rate (95% CI) | Cook.d |
|---|---|---|
| Omitting Nastasi, 2021 [6] | 2.32 (1.58–3.40) | 0.001 |
| Omitting Oliver-Williams, 2019 [10] | 2.74 (2.27–3.32) | 0.958 |
| Omitting Elbasty, 2019 [11] | 2.36 (1.63–3.43) | 0.019 |
| Omitting Parr, 2011 [7] | 2.25 (1.55–3.27) | 0.016 |
| Omitting Forsdahl, 2010 [12] | 2.32 (1.58–3.41) | 0.001 |
| Omitting Brown, 2008 [13] | 2.29 (1.56–3.67) | 0.001 |
| Omitting Baumgartner, 2008 [14] | 2.33 (1.59–3.41) | 0.003 |
| Omitting Lindholt, 2007 [20] | 2.18 (1.52–3.15) | 0.093 |
| Omitting Newman, 2001 [15] | 2.24 (1.53–3.27) | 0.030 |
| Omitting Brady, 2001 [21] | 2.14 (1.50–3.06) | 0.167 |
| Omitting Galland, 1998 [16] | 2.27 (1.55–3.32) | 0.008 |
| Metaregression | Intercept | SE | p Value | |
|---|---|---|---|---|
| Cardiovascular death | Diabetes | −3.61 | 0.01 | 0.35 |
| HTN | −3.46 | 0.004 | 0.27 | |
| Aspirin | −4.83 | 0.02 | 0.77 | |
| Statin | −5.74 | 0.05 | 0.62 | |
| Year | −95.5 | 0.02 | 0.01 | |
| Myocardial infarction | Diabetes | −5.16 | 0.02 | 0.23 |
| HTN | −5.05 | 0.01 | 0.66 | |
| Aspirin | −6.27 | 0.01 | <0.01 | |
| Year | −14.53 | 0.05 | 0.91 | |
| Stroke | Diabetes | −4.54 | 0.02 | 0.27 |
| HTN | −4.88 | 0.01 | 0.19 | |
| Aspirin | −3.12 | 0.02 | 0.17 | |
| Year | −58.95 | 0.04 | 0.55 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharma, C.; Singh, T.P.; Thanigaimani, S.; Nastasi, D.; Golledge, J. A Systematic Review and Meta-Analysis of the Incidence and Risk Factors for Major Adverse Cardiovascular Events in Patients with Unrepaired Abdominal Aortic Aneurysms. Biomedicines 2023, 11, 1178. https://doi.org/10.3390/biomedicines11041178
Sharma C, Singh TP, Thanigaimani S, Nastasi D, Golledge J. A Systematic Review and Meta-Analysis of the Incidence and Risk Factors for Major Adverse Cardiovascular Events in Patients with Unrepaired Abdominal Aortic Aneurysms. Biomedicines. 2023; 11(4):1178. https://doi.org/10.3390/biomedicines11041178
Chicago/Turabian StyleSharma, Chinmay, Tejas P. Singh, Shivshankar Thanigaimani, Domenico Nastasi, and Jonathan Golledge. 2023. "A Systematic Review and Meta-Analysis of the Incidence and Risk Factors for Major Adverse Cardiovascular Events in Patients with Unrepaired Abdominal Aortic Aneurysms" Biomedicines 11, no. 4: 1178. https://doi.org/10.3390/biomedicines11041178