
Quantitative Ultrasound and Bone Health in Elderly People, a Systematic Review
 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Eligible Criteria
2.2. Study Selection
2.3. Data Sources
2.4. Methodological Quality Assessment and evaluation of the Risk of Bias in the Included Studies
3. Results
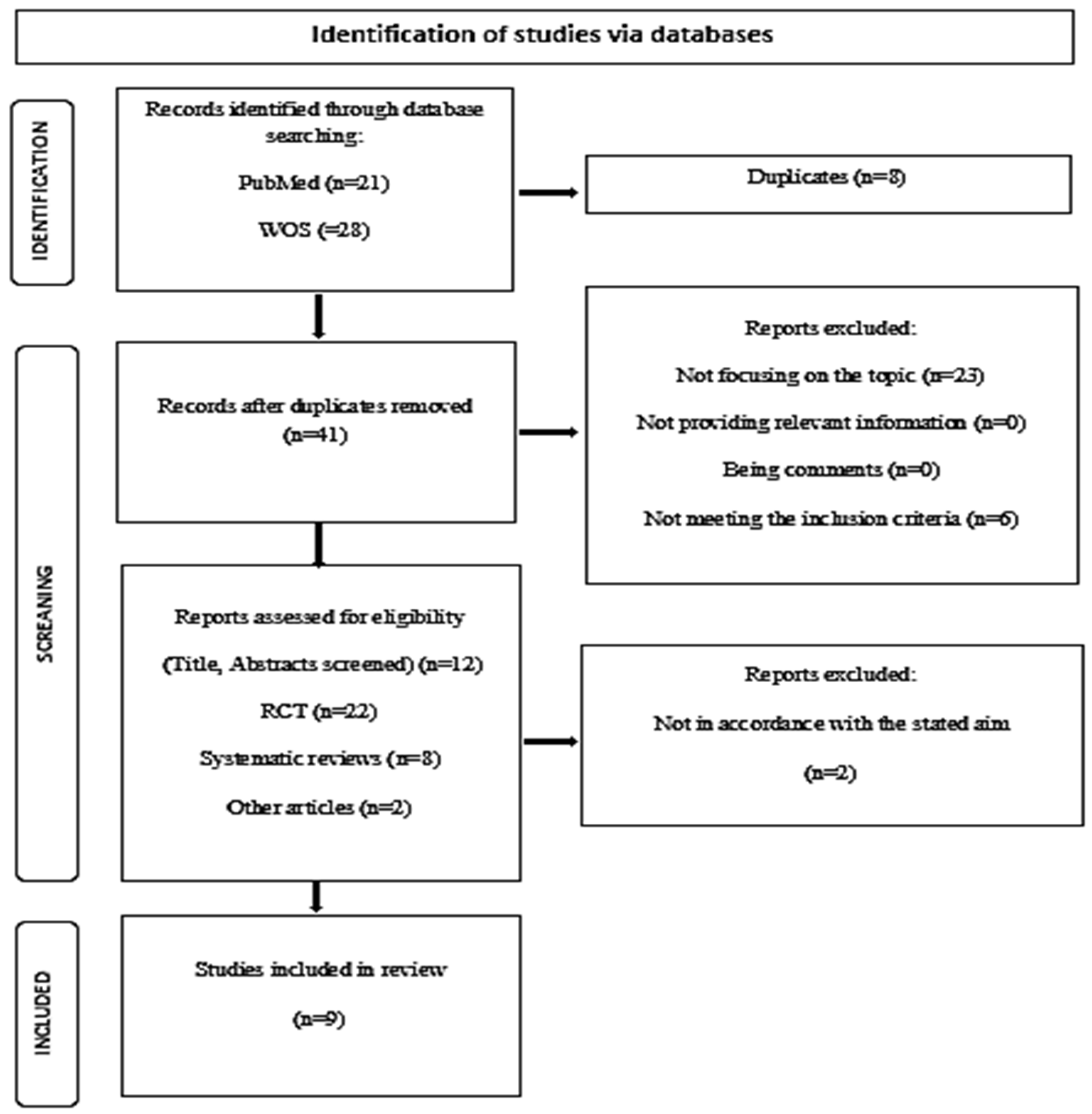
Selection of Studies
- PubMed: 21 articles
- WOS: 28 articles

{kind=link}
| Author | Type of Study | Participant Profile | Intervention | Variables | Results | Conclusions and Limitations |
|---|---|---|---|---|---|---|
| Chan M.Y., et al., 2012 [28] | EP | 454 W 445 M 62–89 years | 1989–2009 DXA QUS: BUA CUBA RX | DMO femoral neck: DXA CQUS (BUA): CUBA Fx for fragility: X-ray | 75 M +154 W with fx for fragility W model BMD of the femoral neck and BUA had a higher AUC compared to the model without BUA Reclassification analysis showed: 7.3%, 11.1% and 5.2% for any fx. | CQUS: independent predictor of fx risk. QUS + BMD measurement could improve the predictive accuracy of fx risk in M AM. |
| Hadyi P., et al., 2015 [29] | ECC | 205 W postMP 68–95 years (hip fx by OsP) 109 GC HM age 75.7 years | DXA 6 different QUS: Ach; Sh; IS; DMB; Omn; QUS-2 | The outcomes of both groups were compared | T scores in W hip fx than matched controls: −2.38 vs. −1.64 (p < 0.001), −2.36 vs. −1.44 (p < 0.001) and −2.05 vs. −1.50 (p = 0.41). Ach, Sh, IS, and Omn QUS T-scores were also lower in W with hip fx compared to matched controls −3.20 vs. −2.36 (p < 0.001), −2.196 vs. −1.761 (p = 0.005), −2.631 vs. −1.849(0 < 0.001), −3.707 vs. −3.030 (p = 0.032). However, DBM and QUS-2 T-scores did not differ between groups. Compared with DXA (hip), the odds ratios of Ach, IS, and Sh were similar, while the odds ratios of DBM, Omn, and QUS-2 were significantly lower (p < =0.05). | Compared with DXA, Ach, Sh and IS can identify a clinically significant risk factor in W with high risk of hip FX. |
| Zha X.Y., et al., 2015 [31] | RCT | 472 M over 60 years (78 years middle ages) | BMD in left hip and lumbar spine: DXA DMO CQUS Curve AUC | Evaluation of the OSTA/QUS; OSTA + QUS. Receiver operational characteristics analysis: SnD and EpD. AUC was compared. | -Prevalence of OsP 27.7% -Optimal cut for OSTA: −3.5 to predict M with OsP anywhere, with SnD= 47.3% and EpD= 76.8% The AUC for OSTA = 0.676 -Optimal cutting for QUS-T score: −1.25, with SnD = 80.4% and EpD = 59.7% AUC for QUS-T = 0.762 - QUS + OSTA Combination improved EpD = 92.9%, but reduced SnD = 36.1%. | OSTA and QUS, respectively, and OSTA + QUS may help find populations at high risk of OsP, which could be an alternative method for their diagnosis, especially in areas where DXA is not accessible. |
| Zhang L.C., et al., 2015 [30] | ETP | 53 W OsP with femoral fx | CQUS DXA HSA | Surgery for femoral heads PCT Pearson correlation: QUS measured/DXA HSA Parameters Ym to evaluate the specific association: QUS (hip), femoral neck, trochanteric + Ward’s area, and femoral diaphysis. | Trochanteric area correlation coefficient (r = 0.356, p = 0.009) was >the neck area (r = 0.297, p = 0.031) and the total prox femur (r = 0.291, p = 0.034). QUS index was significantly correlated with HSA-derived parameters of the trochanteric area (r:0.315–0.356, all p < 0.05), as well as Ym of PCT of the femoral head (r = 0.589, p < 0.001). | The calcaneal bone and the trochanteric spongy bone showed a strong correlation. CQUS parameters may reflect the characteristics of the trochanteric area of the proximal hip, although it does NOT specifically reflect those of the neck or femoral shaft. |
| Cesme F., et al., 2016 [32] | ECC | 20 M with fx hip 18 H with fx distal forearm 38 GC = age | DXA, DMO (CV and hip) CQUS | AUC to assess the discriminatory power of DXA FX and variable QUS | QUS T-score and SOS proved to be the best parameters for the identification of fx of hip and distal forearm. AUC is greater than DXA BMDs and other QUS parameters. QUS T of <= −1.18 could identify and rule out cases of hip FX approx. 80% of SnD and EpD, SOS <= 1529.75 reached almost 90% to rule out distal forearm fx. | The discrimination between M fx and non-fx with QUS variables was as good as DXA’s and even better. |
| Esmaeilzadeh S., et al., 2016 [36] | ECC | 20 W with distal forearm fx and 18 M with hip fx 76 M = age as GC | DXA: measured BMD in CV, proximal femur and radius CQUS: measured bone acoustic parameters FRAX: calculated the probability of fx at 10 years. ORAI: in all participants ROC: evaluated the discriminatory power of fx of all tools | All variables’ probabilities demonstrated significant areas under the ROC curves for W discrimination with hip fx and those without fx. Only 33% of radium BMD, BUA attenuation, and FRAX.® The highest probability of fx OsT calculated without BMD showed significant discriminatory power for distal forearm fx. | The QUS variables (BUA and FRAX®) are good candidates for the identification of both hip and distal radius fx. | |
| Su Y., et al., 2018 [33] | ECC (Tree modeling study) | M&W > 65 years | QALY of the different OsP detection strategies, followed by a subsequent 5 years tto with alendronate/to no detection | DXA to all FRAX® at specific thresholds QUS before DXA No screening | All screening strategies were systematically + cost-effective than the absence of detection in AM >65 years. One-way sensitivity analysis did not change results substantially. Probabilistic sensitivity analyses showed a dominant role of prescreening with FRAX followed by subsequent treatment with OsP drugs in people aged 70 years or +. | DXA-based OsP detection strategies with or without pre-detection (performed with FRAX QUS prior to DXA) are cost-effective + compared to the absence of detection in Chinese people over 65 years. |
| Fitzgerald G.E., et al., 2020 [21] | ETO | 56 total. W post-MP 77% M > 50 58(7.2) years with axSpA | DXA: BMD of QoL and hip CQUS: BUA, SOS, SI and T scores. ROC analysis determined QUS’ ability to discriminate between low and normal BMD. | Calculate: nº of DXA that could be avoided. BASDAI BASFI ASQoL HAQ | BUA, SI and QUS T-score parameters correlated with BMD by DXA SOS did not All QUS parameters had the ability to discriminate between low and normal BMD (the area under the curve ranged from 0.695 to 0.779) QUS identified individuals without low BMD with 90% confidence, with BUA functioning better (SnD = 93%, negative predictive value = 86%). | Using QUS as a triage tool, up to 27% of DXA assessments could have been avoided. QUS could not confidently identify people with OsP. QUS is a promising NON-invasive classification tool in the evaluation of AM OsP with axSpa. |
| Li C.Z., et al., 2022 [35] | EO | 82 p. > 50 years 12 M (62.3 ± 11.6 years) 70 W (63.9 ± 9.2 years) | BMD of the femoral and intertrochanteric neck of the left hip and lumbar spine (L1-L4) with DXA QUS parameters of the right and left calcaneus | DXA: lumbar spine+ left hip. BMD: T-scores; QUS (SONOS 3000):BQI +bilateral CQUS-T. (BQI = SOS and BUA) The mean value of both CQUS parameters. QUS T-score + BQI correlation of calcaneus + DXA parameters Lumbar spine and s.a. (software SPSS20.0) Was generated: receiver’s operating characteristic curve. Were evaluated: areas under the curves. Values for QUS were defined. | In M there was a moderate correlation between CQUS and prox femoral BMD (p < 0.05), no significant correlation between BMD of CQUS and lumbar BMD (p > 0.05). In W, CQUS were moderately correlated with BMD of the lumbar spine and prox femur (p < 0.05) DXA was used: Precision = 90.2%; SnD = 89.2%; EpD = 100%, Predictive value + =100%, Predictive value− =50%of CQUS in the diagnosis of OsP When the CQUS T-score was 1–1.8, the area under the curve =0.888, SnD = 73.21%, and EPD = 92.31% (p < 0.05). When the CQUS T-score was −2.35, SnD = 37.2%, and EpD = 100%. | QUS can be used to predict femoral BMD in middle-aged and elderly people, as well as lumbar to predict BMD in M. Calcaneal QUS has a good EpD as a screening method for OsP. It may be recommended for use as a pre-screening tool to reduce the number of DXAs. If the CQUS T score is −1.8, it has the highest diagnostic efficiency for OsP. When the CQUS T-score is <−2.35, it can be diagnosed as OsP. |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Data Base | Search Strategy |
|---|---|
| PUBMED (RCTs from 2012 to October 2022) | [MeSh terms]: “bone density” AND “elderly” AND “ultrasonography” [MeSh terms]: “bone density” AND “elderly” AND “DXA” [MeSh terms]: “bone density2 AND “elderly” AND “DXA” AND “ultrasonography” |
| Web of Science (WOS) (RCTs from 2012 to October 2022) | [MeSh terms]: “elderly” AND “DXA” AND “QUS” [MeSh terms]: “bone density” AND “elderly” AND “DXA” AND “QUS” |
Appendix B
| 1 * | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Chan M.Y., et al., 2012 [28] | 1 | 1 | - | 1 | 1 | 1 | 1 | 1 | - | 1 | - | 7 |
| Zha X.Y., et al., 2015 [31] | 1 | 1 | - | 1 | - | 1 | - | 1 | 1 | 1 | 1 | 7 |
| Hadyi P., et al., 2015 [29] | 1 | 1 | - | 1 | - | - | - | 1 | 1 | 1 | 1 | 6 |
| Zhang L.C., et al., 2015 [30] | 1 | 1 | 1 | 1 | 1 | - | 1 | 1 | 1 | - | 1 | 8 |
| Cesme F., et al., 2016 [32] | 1 | 1 | - | 1 | - | - | - | 1 | 1 | 1 | 1 | 6 |
| Esmaeilzadeh S., et al., 2016 [36] | 1 | 1 | - | 1 | - | - | - | 1 | 1 | 1 | 1 | 6 |
| Su Y., et al., 2018 [33] | 1 | 1 | 1 | 1 | - | - | - | 1 | 1 | 1 | - | 6 |
| Fitgerald G.E., et al., 2020 [21] | 1 | 1 | - | 1 | - | - | - | 1 | 1 | 1 | 1 | 6 |
| Li C.Z., et al., 2022 [35] | 1 | 1 | 1 | 1 | - | 1 | - | 1 | 1 | 1 | 1 | 8 |
Appendix C
| Reference | Sample Randomization | Concealed Allocation | Blinding of Participants | Blinding of Outcome Measures | Loss of Results | Partial Information of the Results | Other Biases |
|---|---|---|---|---|---|---|---|
| [28] | Yes | Yes | NR | NR | Yes | No | No |
| [31] | Yes | Yes | NR | Yes | Yes | No | No |
| [29] | Yes | Yes | Yes | Yes | Yes | No | No |
| [30] | Yes | Yes | NR | No | Yes | No | No |
| [32] | Yes | Yes | NR | No | No | No | No |
| [36] | Yes | Yes | NR | No | No | No | No |
| [33] | Yes | Yes | NR | No | No | No | No |
| [21] | Yes | Yes | NR | No | No | No | No |
| [35] | Yes | Yes | NR | NR | No | No | No |
References
- Narkauskaitė, L.; Samsonienė, L.; Karanauskien, D.; Stankutė, V. Psychomotor abilities of elderly people and their motivation to partipate in organized physical activity. Exp. Aging Res. 2020, 46, 257–271. [Google Scholar] [CrossRef] [PubMed]
- Organización Mundial de la Salud (OMS), Envejecimiento y Salud. Available online: https://www.who.int/es/news-room/fact-sheets/detail/ageing-and-health (accessed on 20 October 2022).
- Proietti, M.; Cesari, M. Frailty: What is it? Adv. Exp. Med. Biol. 2020, 1216, 1–7. [Google Scholar] [PubMed]
- Karma, B.; Ada-Katrin, B.; Händler-Schuster, D. Exploring health-related needs of elderly people (70+) at home: A qualitative study from switzerland. J. Prim. Care Community Health 2021, 12, 21501327211055635. [Google Scholar] [CrossRef] [PubMed]
- Activo, V.L.J.E. Ministerio de Sanidad, Política Social e Igualdad. Secretaría General de Política Social y Consumo, 1st ed.; Instituto de Mayores y Servicios Sociales (IMSERSO): Madrid, Spain, 2011; Available online: https://www.8088_8089libroblancoenv.pdf(imserso.es) (accessed on 20 October 2022).
- Muñoz Silva, C.A.; Rojas Orellana, P.A.; Marzuca-Nassr, G.N. Criterios de valoración geriátrica integral en adultos mayors con dependencia moderada y severa en Centros de Atención Primaria en Chile. Rev. Med. Chil. 2015, 143, 612–618. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Velilla, N.; Tarazona-Santabalbina, F.J.; Vidán Astiz, M.T.; García Navarro, J.A. Valoración integral y multidimensional del anciano vs. valoración geriátrica integral. Rev. Esp. Geriatr. Gerontol. 2021, 56, 183. [Google Scholar] [CrossRef]
- So, E.; Rushing, C.; Prissel, M.A.; Berlet, G.C. The Role of Secondary Imaging Techniques for Assessing Bone Mineral Density in Elderly Ankle Fractures. J. Foot Ankle Surg. 2022, 61, 149–156. [Google Scholar] [CrossRef]
- World Health Organization. World Report on Aging and Health. 2015. Available online: https://apps.who.int/iris/bitstream/handle/10665/186463/9789240694811eng.pdf;jsessionid=79B5350EF62B5A48500DE81E6B760688?sequence=1 (accessed on 20 October 2022).
- Alonso Bouzón, C. La valoración geriátrica integral. Posicionamiento Soc. Española Med. Geriátrica. Rev. Esp. Geriatr. Gerontol. 2021, 56, 248–249. [Google Scholar] [CrossRef]
- Frost, M.L.; Blake, G.M.; Fogelman, I. Quantitative ultrasound and bone mineral density are equally strongly associated with risk factors for osteoporosis. J Bone Miner. Res. 2001, 16, 406–416. [Google Scholar] [CrossRef]
- Moayyeri, A.; Adams, J.E.; Adler, R.A.; Krieg, M.A.; Hans, D.; Compston, J.; Lewiecki, E.M. Quantitative ultrasound of the heel and fracture risk assessment: An updated meta-analysis. Osteop. Int. 2012, 23, 143–153. [Google Scholar] [CrossRef]
- Abizanda Soler, P.; Rodriguez Mañas, L. Tratado de Medicina Geriátrica: Fundamentos de la Atención Sanitaria a Los Mayores, 2nd ed.; Elsevier: Barcelona, Spain, 2020. [Google Scholar]
- Peck, W.A. Consensus development Conference: Diagnosis, Prophylaxis and Treatment of osteoporosis. Am. J. Med. 1993, 94, 646–650. [Google Scholar]
- Langton, C.M.; Palmer, S.B.; Porter, S.W. The measurement of broadband ultrasonic attenuation in cancellous bone. Eng. Med. 1984, 13, 89–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, J.; Liu, B.; Qin, M.Z.; Liu, J.P. Fall Prevention and Anti-Osteoporosis in Osteopenia Patients of 80 Years of Age and Older: A Randomized Controlled Study. Orthop. Surg. 2020, 12, 890–899. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.H.; Hong, S.W. Risk Factors of Frailty in Patients with Distal Radius Fractures. Ger. Ortho. Surg. Rehab. 2022, 13, 21514593221094736. [Google Scholar] [CrossRef] [PubMed]
- Williams, L.J.; Pasco, J.A.; Jacka, F.N.; Hodge, J.M.; Kotowicz, M.A.; Berk, M. Quantitative heel ultrasound (qus) measures of bone quality in association with mood and anxiety disorders. J. Affect. Disord. 2013, 146, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Luo, W.; Zhang, Q.; Lei, B.; Wang, T.; Chen, Z.; Fu, Y.; Guo, P.; Li, C.; Ma, T.; et al. Osteoporosis diagnosis based on ultrasound radio frequency signal via multi-channel convolutional neural network. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Guadalajara, Mexico, 1–5 November 2021; pp. 832–835. [Google Scholar]
- Diez-Perez, A.; Brandi, M.L.; Al-Daghri, N.; Branco, J.C.; Bruyère, O.; Cavalli, L.; Cooper, C.; Cortet, B.; Dawson-Hughes, B.; Dimai, H.P.; et al. Radiofrequency echographic multi-spectrometry for the in-vivo assessment of bone strength: State of the art-outcomes of an expert consensus meeting organized by the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO). Aging Clin. Exp. Res. 2019, 31, 1375–1389. [Google Scholar] [CrossRef] [Green Version]
- Fitzgerald, G.E.; Anachebe, T.; McCarroll, K.G.; O’Shea, F. Calcaneal quantitative ultrasound has a role in out ruling low bone mineral density in axial spondyloarthropathy. Clin. Rheumatol. 2020, 39, 1971–1979. [Google Scholar] [CrossRef]
- Blake, G.M.; Fogelman, I. Methods and Clinical Issues in Bone Densitometry; Academic Press: New York NY, USA, 2008. [Google Scholar]
- He, Y.Q.; Fan, B.; Hans, D.; Li, J.; Wu, C.Y.; Njeh, C.F.; Zhao, S.; Lu, Y.; Tsuda-Futami, E.; Fuerst, T.; et al. Assessment of a new quantitative ultrasound calcaneus measurement precision and discrimination of hip fractures in elderly women compared with dual x-ray absorptiometry. Osteoporos. Int. 2000, 11, 354–360. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021, 88, 18. [Google Scholar]
- Stone, P.W. Popping the (PICO) question in research and evidence-based practice. Appl. Nurs. Res. 2002, 15, 197–198. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- McCormack, H.M.; De LHorne, D.J.; Sheather, S. Clinical applications of visual analogue scales: A critical review. Psychol. Med. 1988, 18, 1007–1019. [Google Scholar] [CrossRef]
- Verhagen, A.P.; De Vet, H.C.W.; De Bie, R.A.; Boers, M.; Van Den Brandt, P.A. The art of quality assessment of RCTs included in systematic reviews. J. Clin. Epidemiol. 2001, 54, 651–654. [Google Scholar] [CrossRef]
- Chan, M.Y.; Nguyen, N.D.; Center, J.R.; Eisman, J.A.; Nguyen, T.V. Absolute fracture-risk prediction by a combination of calcaneal quantitative ultrasound and bone mineral density. Calcif. Tissue Int. 2012, 90, 128–136. [Google Scholar] [CrossRef]
- Hadji, P.; Imani, P.; Wüster, C.; Hars, O.; Albert, U.-S.; Kyvernitakis, I. Comparison of dual-energy X-ray absorptiometry with six quantitative ultrasonometry devices in women with hip fractures. Climateric 2015, 18, 411–418. [Google Scholar] [CrossRef]
- Zha, X.Y.; Hu, Y.; Pang, X.N.; Chang, G.-L.; Li, L. Diagnostic value of the osteoporosis self-assessment tool for Asians (OSTA) and quantitative bone ultrasound (QUS) in Screening high-risk. J. Bone Miner. Metab. 2015, 33, 230–238. [Google Scholar] [CrossRef]
- Zhang, L.C.; Lv, H.C.; Zheng, H.L.; Li, M.; Yin, P.B.; Peng, Y.; Gao, Y.; Zhang, L.H.; Tang, P.F. Correlation between parameters of calcaneal quantitative ultrasound and Hip structural analysis in Osteoporotic fracture patients. PLoS ONE 2015, 10, e0145879. [Google Scholar] [CrossRef] [Green Version]
- Esmaeilzadeh, S.; Cesme, F.; Oral, A.; Yaliman, A.; Sindel, D. The utility of dual-energy X-ray absorptiometry, calcaneal quantitative ultrasound, and fracture risk indices (FRAX® and Osteoporosis Risk Assessment Instrument) for the identification of women with distal forearm or hip fractures: A pilot study. Endocr. Res. 2016, 41, 248–260. [Google Scholar] [CrossRef]
- Li, C.; Sun, J.; Yu, l. Diagnostic value of calcaneal quantitative ultrasound in the evaluation of osteoporosis in middle-aged and elderly patients. Medicine 2022, 101, e28325. [Google Scholar] [CrossRef]
- Su, Y.; Lai, F.; Yip, B.; Leung, J.; Kwok, T. Cost-effectiveness of osteoporosis screening strategies for hip fracture prevention in older Chinese people: A decision tree modeling study in the Mr. OS and Ms. OS cohort in Hong Kong. Osteoporos Int. 2018, 29, 1793–1805. [Google Scholar] [CrossRef]
- Cesme, F.; Esmaeilzadeh, S.; Oral, A. Discriminative ability of calcaneal quantitative ultrasound compared with dual-energy X-ray absorptiometry in men with hip or distal forearm fractures. Acta Orthop. Et Traumatol. Turc. 2016, 50, 548–553. [Google Scholar] [CrossRef] [Green Version]
- McCloskey, E.V.; Kanis, J.A.; Odén, A.; Harvey, N.C.; Bauer, D.; González-Macias, J.; Hans, D.; Kaptoge, S.; Krieg, M.A.; Kwok, T.; et al. Predictive ability of heel quantitative ultrasound for incident fractures: An individual-level meta-analysis. Osteoporos Int. 2015, 26, 1979–1987. [Google Scholar] [CrossRef]
- Hans, D.B.; Shepherd, J.A.; Schwartz, E.N.; Reid, D.M.; Blake, G.M.; Fordham, J.N.; Fuerst, T.; Hadji, P.; Itabashi, A.; Krieg, M.A.; et al. Peripheral dual-energy X-ray absorptiometry in the management of osteoporosis: The 2007 ISCD Official Positions. J Clin. Densitom. 2008, 11, 188–206. [Google Scholar] [CrossRef] [PubMed]
- Raum, K.; Laugier, P. Clinical devices for bone assessment. Adv. Exp. Med. Biol. 2022, 1364, 35–53. [Google Scholar] [PubMed]
- Cosman, F.; de Beur, S.J.; LeBoff, M.S.; Lewiecki, E.M.; Tanner, B.; Randall, S.; Lindsay, R.; National Osteoporosis Foundation. Clinician’s Guide to Prevention and Treatment of Osteoporosis. Osteoporos Int. 2014, 25, 2359–2381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hans, D.; Baim, S. Quantitative ultrasound (QUS) in the management of osteoporosis and assessment of fracture risk. J. Clin. Densitom. 2017, 20, 322–333. [Google Scholar] [CrossRef]
- NICE. Osteoporosis Secondary Prevention Including Strontium Ranelate. Available online: http://guidance.nice.org.uk/TA161 (accessed on 20 October 2022).
- Thomsen, K.; Jepsen, D.B.; Matzen, L.; Hermann, A.P.; Masud, T.; Ryg, J. Is calcaneal quantitative ultrasoun useful as a prescreen stratification tool for osteoporosis? Osteoporos Int. 2015, 26, 1459–1475. [Google Scholar] [CrossRef]
- Clowes, J.A.; Peel, N.F.; Eastell, R. Device-specific thresholds to diagnose osteoporosis at the proximal femur: An approach to interpreting peripheral bone measurements in Clinical practice. Osteoporos Int. 2006, 17, 1293–1302. [Google Scholar] [CrossRef]
- Dontas, I.A.; Yiannakopoulos, C.K. Risk factors and prevention of osteoporosis-related fractures. J. Musculoskelet. Neuronal. Interact. 2007, 7, 268–272. [Google Scholar]
- Kanis, J.A.; Gluer, C.C. An update on the diagnosis and assessment of osteoporosis with densitometry. Osteoporos Int. 2000, 11, 192–202. [Google Scholar] [CrossRef]
- Nayak, S.; Roberts, M.S.; Greenspan, S.L. Cost-effectiveness of different Screening strategies for osteoporosis in postmenopaual women. Ann. Intern. Med. 2011, 155, 751–761. [Google Scholar] [CrossRef]
- Caulin, F.; Kanis, J.A.; Johnell, O.; Oden, A. Optimal age for preventing osteoporosis after menopause depends on Effects of stopping treatment. Bone 2002, 30, 754–758. [Google Scholar] [CrossRef]
- Bauer, D.C.; Ewing, S.K.; Cauley, J.A.; Ensrud, K.E.; Cummings, S.R.; Orwoll, E.S. Osteoporotic Fractures in Men (MrOS) Research Group. Quantitative ultrasound predicts hip and non-spine fracture in men: The MrOS study. Osteoporos Int. 2007, 18, 771–777. [Google Scholar] [CrossRef]
- Pluskiewicz, W.; Wilk, R.; Wielg_orecki, A.; Golba, K.S.; Drozdzowska, B. Fracture status in men assessed by quantitative ultrasound measurements at the calcaneus. J. Ultrasound. Med. 2011, 30, 877–882. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.-M.; Ma, L.-Y.; Bi, Y.-f.; Xu, Y.; Huang, Y.; Xu, M.; Zhao, H.-Y.; Sun, L.-H.; Tao, B.; Li, X.-y.; et al. A population-based study examining calcaneus quantitative ultrasound and its optimal cut-points to discriminate osteoporotic fractures among 9352 Chinese women and men. J. Clin. Endocrinol. Metab. 2012, 97, 800–809. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Zhou, W.; Hao, Y.J.; Li, G.T.; Deng, X.R.; Zhao, J.; Zhang, Z.L. Quantitative ultrasound scans of the calcaneus: A useful tool for screening osteoporosis in patients with connective tissue disease. Beijing Da Xue Xue Bao. Yi Xue Ban J. Peking Univ. Health Sci. 2013, 45, 766–769. [Google Scholar]
- Nwawka, O.K. Update in Musculoskeletal Ultrasound Research. Sport. Health 2016, 8, 429–437. [Google Scholar] [CrossRef] [Green Version]
- Kwok, T.; Khoo, C.C.; Leung, J.; Kwok, A.; Qin, L.; Woo, J.; Leung, P.C. Predictive values of calcaneal quantitative ultrasound and dual energy X ray absorptiometry for non-vertebral fracture in older men: Results from the MrOS study (Hong Kong). Osteoporos. Int. 2012, 23, 1001–1006. [Google Scholar] [CrossRef]
- Schott, A.M.; Hans, D.; Duboeuf, F. Quantitative ultrasound parameters as well as bone mineral density are better predictors of trochanteric than cervical hip fractures in elderly women. Results from the EPIDOS study. Bone 2005, 37, 858–863. [Google Scholar] [CrossRef]

| Variables | |
|---|---|
| Primary Measures | Secondary Measures |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Escobio-Prieto, I.; Blanco-Díaz, M.; Pinero-Pinto, E.; Rodriguez-Rodriguez, A.M.; Ruiz-Dorantes, F.J.; Albornoz-Cabello, M. Quantitative Ultrasound and Bone Health in Elderly People, a Systematic Review. Biomedicines 2023, 11, 1175. https://doi.org/10.3390/biomedicines11041175
Escobio-Prieto I, Blanco-Díaz M, Pinero-Pinto E, Rodriguez-Rodriguez AM, Ruiz-Dorantes FJ, Albornoz-Cabello M. Quantitative Ultrasound and Bone Health in Elderly People, a Systematic Review. Biomedicines. 2023; 11(4):1175. https://doi.org/10.3390/biomedicines11041175
Chicago/Turabian StyleEscobio-Prieto, Isabel, María Blanco-Díaz, Elena Pinero-Pinto, Alvaro Manuel Rodriguez-Rodriguez, Francisco Javier Ruiz-Dorantes, and Manuel Albornoz-Cabello. 2023. "Quantitative Ultrasound and Bone Health in Elderly People, a Systematic Review" Biomedicines 11, no. 4: 1175. https://doi.org/10.3390/biomedicines11041175