
Colostrum and Lactoferrin Protect against Side Effects of Therapy with Antibiotics, Anti-inflammatory Drugs and Steroids, and Psychophysical Stress: A Comprehensive Review

Abstract
:1. Introduction
2. Bovine Colostrum
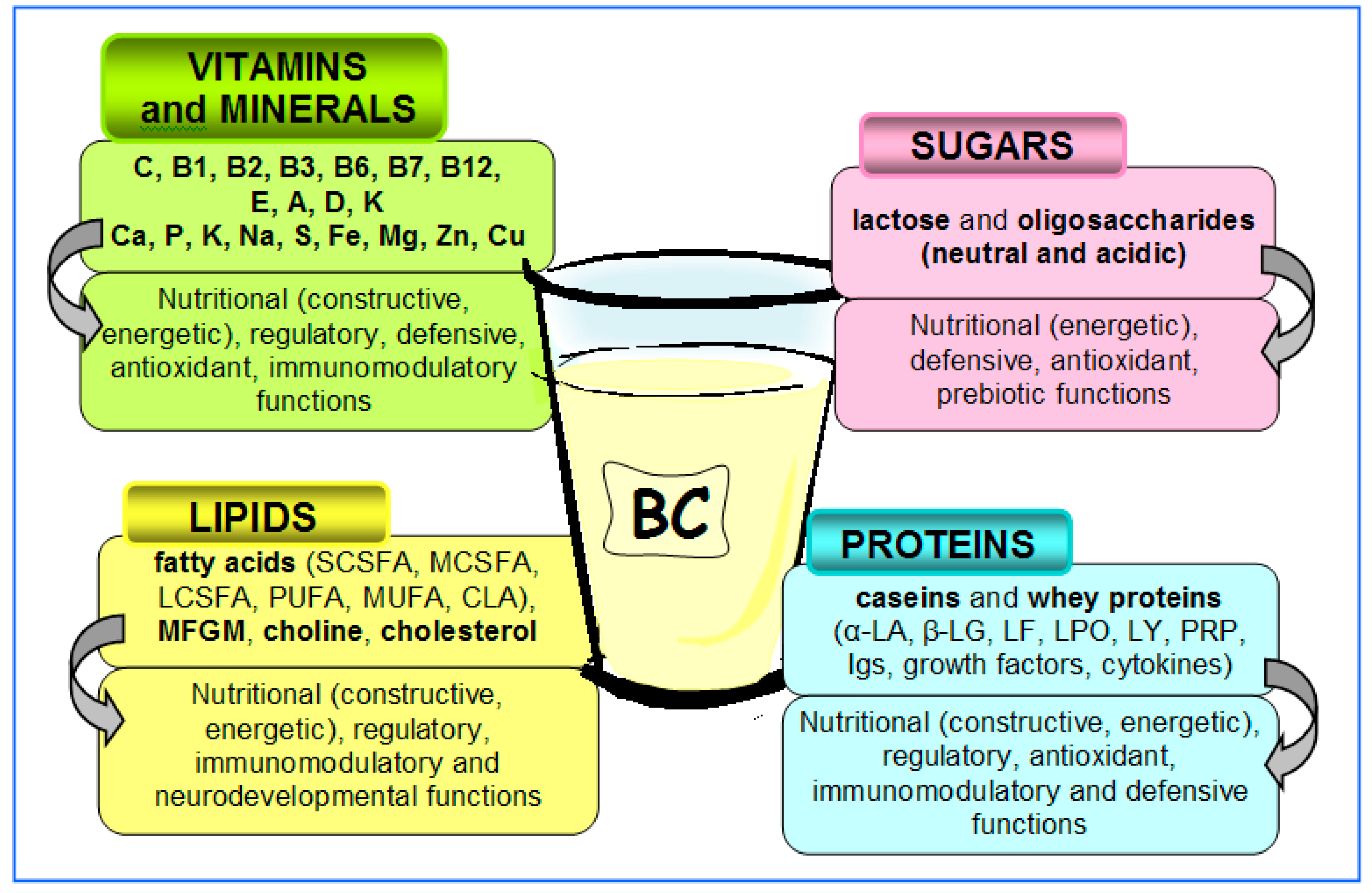
- (1)
- Nutrients: building proteins (caseins, α-lactoalbumin (α-LA), β-lactoglobulin/β-LG/), amino acids, milk sugar (lactose), fats (triglycerides), fatty acids, minerals and vitamins; their purpose is to provide energy and building materials for the fast-growing organism and to regulate the various metabolic processes;
- (2)
- Antimicrobial and immunoregulatory factors: immunoglobulins (Igs), lactoferrin (LF), lactoperoxidase (LPO), lysozyme (LY), antioxidant substances, nucleotides/nucleosides, gangliosides, oligosaccharides/glycoconjugates, phospholipids, colostrinin (proline rich polypeptide (PRP)), cytokines and maternal leukocytes; their purpose is to directly destroy pathogenic microorganisms, promote the growth of symbiotic (beneficial) microorganisms and regulate the maturation and function of the immune system;
- (3)
- Growth factors: insulin-like growth factor (IGF), epidermal growth factor (EGF), transforming growth factor (TGF), platelet-derived growth factor (PDGF), vascular endothelial growth factor (VEGF) and hormones (prolactin, calcitonin, thyroxine, insulin and growth hormone); their function is to regulate the growth, maturation and function of various tissues, such as bone, muscle, connective tissue, nerve tissue, skin and especially the gastrointestinal mucosa; they act both locally (in the intestine) and systemically, after absorption into the circulation.
3. Lactoferrin
4. Lactoferrin as Supportive Therapy in Antibiotic Treatment
4.1. Antibiotic Treatment in In Vitro and Animal Models
4.2. Antibiotic Treatment in Clinics
5. Bovine Colostrum and Lactoferrin as a Supportive Therapy in NSAID Therapy
5.1. NSAID Therapy in Animal Models
5.2. NSAID Therapy in Clinics
6. Bovine Colostrum and Lactoferrin as Supportive Therapy in Steroid Treatment and Psychophysical Stress
6.1. Steroid Therapy and Endogenous Stress in Animal Models
6.2. Endogenous Stress in Clinics
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bindu, S.; Mazumder, S.; Bandyopadhyay, U. Non-steroidal anti-inflammatory drugs (NSAIDs) and organ damage: A current perspective. Biochem. Pharmacol. 2020, 180, 114147. [Google Scholar] [CrossRef] [PubMed]
- Galmarini, D.; Galmarini, C.M.; Galmarini, F.C. Cancer chemotherapy: A critical analysis of its 60 years of history. Crit. Rev. Oncol. Hematol. 2012, 84, 181–199. [Google Scholar] [CrossRef] [PubMed]
- Hutchings, M.I.; Truman, A.W.; Wilkinson, B. Antibiotics: Past, present and future. Curr. Opin. Microbiol. 2019, 51, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Scherholz, M.L.; Schlesinger, N.; Androulakis, I.P. Chronopharmacology of glucocorticoids. Adv. Drug Deliv. Rev. 2019, 151-152, 245–261. [Google Scholar] [CrossRef]
- Akram, F.; Imtiaz, M.; Ul Haq, I. Emergent crisis of antibiotic resistance: A silent pandemic threat to 21st century. Microb. Pathog. 2022, 174, 105923. [Google Scholar] [CrossRef]
- Górski, A.; Miedzybrodzki, R.; Borysowski, J.; Weber-Dabrowska, B.; Lobocka, M.; Fortuna, W.; Letkiewicz, S.; Zimecki, M.; Filby, G. Bacteriophage therapy for the treatment of infections. Curr. Opin. Investig. Drugs 2009, 10, 766–774. [Google Scholar]
- Glaser, R.; Kiecolt-Glaser, J.K.; Malarkey, W.B.; Sheridan, J.F. The influence of psychological stress on the immune response to vaccines. Ann. N. Y. Acad. Sci. 1998, 840, 649–655. [Google Scholar] [CrossRef]
- Li, T.; Harada, M.; Tamada, A.; Abe, K.; Nomoto, K. Repeated restraint stress impairs the antitumor T cell response through its suppressive effect on Th1-type CD4+ T cells. Anticancer Res. 1997, 17, 4259–4268. [Google Scholar]
- Artym, J.; Zimecki, M. The effect of psychic stress on the immune response. Postepy Hig. Med. Dosw. 2004, 58, 166–175. [Google Scholar]
- Campos-Rodríguez, R.; Godínez-Victoria, M.; Abarca-Rojano, E.; Pacheco-Yépez, J.; Reyna-Garfias, H.; Barbosa-Cabrera, R.E.; Drago-Serrano, M.E. Stress modulates intestinal secretory immunoglobulin A. Front. Integr. Neurosci. 2013, 7, 86. [Google Scholar] [CrossRef]
- Artym, J.; Zimecki, M. Colostrum Proteins in Protection against Therapy-Induced Injuries in Cancer Chemo- and Radiotherapy: A Comprehensive Review. Biomedicines 2023, 11, 114. [Google Scholar] [CrossRef] [PubMed]
- Lopez, A.J.; Heinrichs, A.J. Invited review: The importance of colostrum in the newborn dairy calf. J. Dairy Sci. 2022, 105, 2733–2749. [Google Scholar] [CrossRef] [PubMed]
- Tlaskalová-Hogenová, H.; Kverka, M.; Hrdý, J. Immunomodulatory Components of Human Colostrum and Milk. Nestle Nutr. Inst. Workshop Ser. 2020, 94, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Arslan, A.; Kaplan, M.; Duman, H.; Bayraktar, A.; Ertürk, M.; Henrick, B.M.; Frese, S.A.; Karav, S. Bovine Colostrum and Its Potential for Human Health and Nutrition. Front. Nutr. 2021, 8, 651721. [Google Scholar] [CrossRef]
- Mehra, R.; Singh, R.; Nayan, V.; Buttar, H.S.; Kumar, N.; Kumar, S.; Bhardwaj, A.; Kaushik, R.; Kumar, H. Nutritional attributes of bovine colostrum components in human health and disease: A comprehensive review. Food Biosci. 2021, 40, 100907. [Google Scholar] [CrossRef]
- Mehra, R.; Garhwal, R.; Sangwan, K.; Guiné, R.P.F.; Lemos, E.T.; Buttar, H.S.; Visen, P.K.S.; Kumar, N.; Bhardwaj, A.; Kumar, H. Insights into the research trends on bovine colostrum: Beneficial health perspectives with special reference to manufacturing of functional foods and feed supplements. Nutrients 2022, 14, 659. [Google Scholar] [CrossRef]
- Playford, R.J.; Weiser, M.J. Bovine Colostrum: Its Constituents and Uses. Nutrients 2021, 13, 265. [Google Scholar] [CrossRef]
- Bagwe-Parab, S.; Yadav, P.; Kaur, G.; Tuli, H.S.; Buttar, H.S. Therapeutic Applications of Human and Bovine Colostrum in the Treatment of Gastrointestinal Diseases and Distinctive Cancer Types: The Current Evidence. Front. Pharmacol. 2020, 11, 01100. [Google Scholar] [CrossRef]
- Sangild, P.T.; Vonderohe, C.; Hebib, V.M.; Burrin, D.G. Potential Benefits of Bovine Colostrum in Pediatric Nutrition and Health. Nutrients 2021, 13, 2551. [Google Scholar] [CrossRef]
- Stelwagen, K.; Carpenter, E.; Haigh, B.; Hodgkinson, A.; Wheeler, T.T. Immune components of bovine colostrum and milk. J. Anim. Sci. 2009, 87 (Suppl. 13), 3–9. [Google Scholar] [CrossRef]
- Zimecki, M. A proline-rich polypeptide from ovine colostrum: Colostrinin with immunomodulatory activity. Adv. Exp. Med. Biol. 2008, 606, 241–250. [Google Scholar] [CrossRef]
- Rathe, M.; Müller, K.; Sangild, P.T.; Husby, S. Clinical applications of bovine colostrum therapy: A systematic review. Nutr. Rev. 2014, 72, 237–254. [Google Scholar] [CrossRef] [PubMed]
- Silva, E.G.; Rangel, A.H.; Murmam, L.; Bezerra, M.F.; de Oliveira, J.P. Bovine colostrum: Benefits of its use in human food. Food Sci. Technol. 2019, 39 (Suppl. 2), 355–362. [Google Scholar] [CrossRef]
- Kaplan, M.; Arslan, A.; Duman, H.; Karyelioğlu, M.; Baydemir, B.; Günar, B.B.; Alkan, M.; Bayraktar, A.; Tosun, H.I.; Ertürk, M.; et al. Production of Bovine Colostrum for Human Consumption to Improve Health. Front. Pharmacol. 2022, 12, 796824. [Google Scholar] [CrossRef]
- Afzal, I.; Khan, A.A.; Khaliq, T.; Hamadani, H.; Shafi, M.; Raja, T.A. Effect of Bovine Colostrum Supplemented Diets on Performance of Broiler Chicken. Indian J. Poult. Sci. 2017, 52, 157–160. [Google Scholar] [CrossRef]
- Fenger, C.K.; Tobin, T.; Caseyc, P.J.; Roualdesd, E.A.; Langemeiera, J.L.; Cowlese, R.; Haines, D.M. Enhanced bovine colostrum supplementation shortens the duration of respiratory disease in thoroughbred yearlings. J. Equine Vet. Sci. 2016, 42, 77–81. [Google Scholar] [CrossRef]
- Guberti, M.; Botti, S.; Capuzzo, M.T.; Nardozi, S.; Fusco, A.; Cera, A.; Dugo, L.; Piredda, M.; De Marinis, M.G. Bovine Colostrum Applications in Sick and Healthy People: A Systematic Review. Nutrients 2021, 13, 2194. [Google Scholar] [CrossRef]
- Patiroglu, T.; Kondolot, M. The effect of bovine colostrum on viral upper respiratory tract infections in children with immunoglobulin A deficiency. Clin. Respir. J. 2013, 7, 21–26. [Google Scholar] [CrossRef]
- Nigro, A.; Nicastro, A.; Trodella, R. Retrospective observational study to investigate Sinerga, a multifactorial nutritional product, and bacterial extracts in the prevention of recurrent respiratory infections in children. Int. J. Immunopathol. Pharmacol. 2014, 27, 455–460. [Google Scholar] [CrossRef]
- Oloroso-Chavez, K.; Andaya, P.; Wong, C. OR082 bovine colostrum supplementation in respiratory allergies according to sensitization: Subgroup analysis of randomized controlled trial. Ann. Allergy Asthma Immunol. 2017, 119, S11–S12. [Google Scholar] [CrossRef]
- Ebina, T.; Sato, A.; Umezu, K.; Ishida, N.; Ohyama, S.; Ohizumi, A.; Aikawa, K.; Katagiri, S.; Katsushima, N.; Imai, A.; et al. Prevention of rotavirus infection by cow colostrum antibody against human rotaviruses. Lancet 1983, 2, 1029–1030. [Google Scholar] [CrossRef] [PubMed]
- Sarker, S.A.; Casswall, T.H.; Mahalanabis, D.; Alam, N.H.; Albert, M.J.; Brussow, H.; Fuchs, G.J.; Hammerstrom, L. Successful treatment of rotavirus diarrhea in children with immunoglobulin from immunized bovine colostrum. Pediatr. Infect. Dis. J. 1998, 17, 1149–1154. [Google Scholar] [CrossRef]
- Patel, K.; Rana, R. Pedimune in recurrent respiratory infection and diarrhoea—The Indian experience—The pride study. Indian J. Pediatr. 2006, 73, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Huppertz, H.I.; Rutkowski, S.; Busch, D.H.; Eisebit, R.; Lissner, R.; Karch, H. Bovine colostrum ameliorates diarrhea in infection with diarrheagenic Escherichia coli, shiga toxin-producing E. coli, and E. coli expressing intimin and hemolysin. J. Pediatr. Gastroenterol. Nutr. 1999, 29, 452–456. [Google Scholar] [CrossRef] [PubMed]
- Suwarba, I.G.; Sudaryat, S.; Hendra, S.; Suandi, I.K.G.; Widiana, R. The role of bovine colostrum on recovery time and length of hospital stay of acute diarrhea in infants and children: A double-blind randomized controlled trial. Paediatr. Indones. 2006, 46, 127–133. [Google Scholar] [CrossRef]
- Li, J.; Xu, Y.W.; Jiang, J.J.; Song, Q.K. Bovine colostrum and product intervention associated with relief of childhood infectious diarrhea. Sci. Rep. 2019, 9, 3093. [Google Scholar] [CrossRef] [PubMed]
- Barakat, S.H.; Meheissen, M.A.; Omar, O.M.; Elbana, D.A. Bovine colostrum in the treatment of acute diarrhea in children: A double-blinded randomized controlled trial. J. Trop. Pediatr. 2020, 66, 46–55. [Google Scholar] [CrossRef]
- Bierut, T.; Duckworth, L.; Grabowsky, M.; Ordiz, M.I.; Laury, M.L.; Callaghan-Gillespie, M.; Maleta, K.; Manary, M.J. The effect of bovine colostrum/egg supplementation compared with corn/soy flour in young Malawian children: A randomized, controlled clinical trial. Am. J. Clin. Nutr. 2021, 113, 420–427. [Google Scholar] [CrossRef]
- Ismail, R.I.H.; Awad, H.A.; Imam, S.S.; Gad, G.I.; Aboushady, N.M.; Abdou, R.M.; Eissa, D.S.; Azzam, N.T.; Barakat, M.M.; Yassin, M.M.; et al. Gut priming with bovine colostrum and T regulatory cells in preterm neonates: A randomized controlled trial. Pediatr. Res. 2021, 90, 650–656. [Google Scholar] [CrossRef]
- Sanctuary, M.R.; Kain, J.N.; Chen, S.Y.; Kalanetra, K.; Lemay, D.G.; Rose, D.R.; Yang, H.T.; Tancredi, D.J.; German, J.B.; Slupsky, C.M.; et al. Pilot study of probiotic/colostrum supplementation on gut function in children with autism and gastrointestinal symptoms. PLoS ONE 2019, 14, e0210064. [Google Scholar] [CrossRef]
- Rathe, M.; De Pietri, S.; Wehner, P.S.; Frandsen, T.L.; Grell, K.; Schmiegelow, K.; Sangild, P.T.; Husby, S.; Muller, K. Bovine colostrum against chemotherapy-induced gastrointestinal toxicity in children with acute lymphoblastic leukemia: A randomized, double-blind, placebo-controlled trial. J. Parenter. Enter. Nutr. 2020, 44, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Nappi, R.E.; Benedetto, C.; Campolo, F.; Martella, S.; Tosti, C.; Cianci, A.; Caruso, S.; Guaschino, S.; Grimaldi, E.; Bagolan, M.; et al. Efficacy, tolerability and safety of a new medical device, Monurelle Biogel® vaginal gel, in the treatment of vaginal dryness: A randomized clinical trial in women of reproductive age. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 203, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Brinkworth, G.D.; Buckley, J.D. Concentrated bovine colostrum protein supplementation reduces the incidence of self-reported symptoms of upper respiratory tract infection in adult males. Eur. J. Nutr. 2003, 42, 228–232. [Google Scholar] [CrossRef]
- Chandwe, K.; Kelly, P. Colostrum therapy for human gastrointestinal health and disease. Nutrients 2021, 13, 1956. [Google Scholar] [CrossRef]
- Gomes, R.D.S.; Anay, K.; Galdino, A.B.S.; Oliveira, J.P.F.; Gama, M.A.S.; Medeiros, C.A.; Gavioli, E.C.; Porto, A.L.; Rangel, A.H. Bovine colostrum: A source of bioactive compounds for prevention and treatment of gastrointestinal disorders. NFS J. 2021, 25, 1–11. [Google Scholar] [CrossRef]
- Hałasa, M.; Baśkiewicz-Hałasa, M.; Jamioł-Milc, D.; Maciejewska-Markiewicz, D.; Skonieczna-Żydecka, K. Bovine colostrum supplementation in prevention of upper respiratory tract infections—Systematic review, meta-analysis and meta-regression of randomized controlled trials. J. Funct. Foods 2022, 99, 105316. [Google Scholar] [CrossRef]
- Sienkiewicz, M.; Szymańska, P.; Fichna, J. Supplementation of Bovine Colostrum in Inflammatory Bowel Disease: Benefits and Contraindications. Adv. Nutr. 2021, 12, 533–545. [Google Scholar] [CrossRef]
- Playford, R.J.; MacDonald, C.E.; Calnan, D.P.; Floyd, D.N.; Podas, T.; Johnson, W.; Wicks, A.C.; Bashir, O.; Marchbank, T. Co-administration of the health food supplement, bovine colostrum, reduces the acute non-steroidal anti-inflammatory drug-induced increase in intestinal permeability. Clin. Sci. 2001, 100, 627–633. [Google Scholar] [CrossRef]
- Kazimierska, K.; Kalinowska-Lis, U. Milk proteins—Their biological activities and use in cosmetics and dermatology. Molecules 2021, 26, 3253. [Google Scholar] [CrossRef]
- Eslamian, G.; Ardehali, S.H.; Baghestani, A.R.; Vahdat Shariatpanahi, Z. Effects of early enteral bovine colostrum supplementation on intestinal permeability in critically ill patients: A randomized, double-blind, placebo-controlled study. Nutrition 2019, 60, 106–111. [Google Scholar] [CrossRef]
- Jones, A.W.; March, D.S.; Curtis, F.; Bridle, C. Bovine colostrum supplementation and upper respiratory symptoms during exercise training: A systematic review and meta-analysis of randomised controlled trials. BMC Sports Sci. Med. Rehabil. 2016, 8, 21. [Google Scholar] [CrossRef] [PubMed]
- Główka, N.; Woźniewicz, M. Potential use of Colostrum Bovinum supplementation in athletes—A review. Acta Sci. Pol. Technol. Aliment. 2019, 18, 115–123. [Google Scholar] [CrossRef]
- Davison, G. The use of bovine colostrum in sport and exercise. Nutrients 2021, 13, 1789. [Google Scholar] [CrossRef] [PubMed]
- Dziewiecka, H.; Buttar, H.S.; Kasperska, A.; Ostapiuk-Karolczuk, J.; Domagalska, M.; Cichoń, J.; Skarpańska-Stejnborn, A. A Systematic Review of the Influence of Bovine Colostrum Supplementation on Leaky Gut Syndrome in Athletes: Diagnostic Biomarkers and Future Directions. Nutrients 2022, 14, 2512. [Google Scholar] [CrossRef] [PubMed]
- Puppel, K.; Gołębiewski, M.; Grodkowski, G.; Slósarz, J.; Kunowska-Slósarz, M.; Solarczyk, P.; Łukasiewicz, M.; Balcerak, M.; Przysucha, T. Composition and Factors Affecting Quality of Bovine Colostrum: A Review. Animals 2019, 9, 1070. [Google Scholar] [CrossRef]
- Artym, J.; Zimecki, M. The effects of lactoferrin on myelopoiesis: Can we resolve the controversy? Postepy Hig. Med. Dosw. Online 2007, 61, 129–150. [Google Scholar]
- Artym, J.; Zimecki, M. Milk-derived proteins and peptides in clinical trials. Postepy Hig. Med. Dosw. Online 2013, 67, 800–816. [Google Scholar] [CrossRef]
- Artym, J.; Zimecki, M. Beneficial effect of lactoferrin on the microbiota from gastrointestinal tract. Adv. Microbiol. 2020, 59, 277–290. [Google Scholar] [CrossRef]
- Bagwe, S.; Tharappel, L.J.P.; Kaur, G.; Buttar, H.S. Bovine colostrum: An emerging nutraceutical. J. Complement. Integr. Med. 2015, 12, 175–185. [Google Scholar] [CrossRef]
- Bukowska-Osko, I.; Sulejczak, D.; Kaczynska, K.; Kleczkowska, P.; Kramkowski, K.; Popiel, M.; Wietrak, E.; Kowalczyk, P. Lactoferrin as a Human Genome “Guardian”—An Overall Point of View. Int. J. Mol. Sci. 2022, 23, 5248. [Google Scholar] [CrossRef]
- Cutone, A.; Rosa, L.; Ianiro, G.; Lepanto, M.S.; Bonaccorsi di Patti, M.C.; Valenti, P.; Musci, G. Lactoferrin’s Anti-Cancer Properties: Safety, Selectivity, and Wide Range of Action. Biomolecules 2020, 10, 456. [Google Scholar] [CrossRef] [PubMed]
- Drago-Serrano, M.E.; Campos-Rodríguez, R.; Carrero, J.C.; de la Garza, M. Lactoferrin: Balancing Ups and Downs of Inflammation Due to Microbial Infections. Int. J. Mol. Sci. 2017, 18, 501. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.; Iacucci, M. Diverse immune effects of bovine colostrum and benefits in human health and disease. Nutrients 2021, 13, 3798. [Google Scholar] [CrossRef]
- Gruden, S.; Ulrih, N.P. Diverse mechanisms of antimicrobial activities of lactoferrins, lactoferricins, and other lactoferrin-derived peptides. Int. J. Mol. Sci. 2021, 22, 11264. [Google Scholar] [CrossRef]
- Hao, L.; Shan, Q.; Wei, J.; Ma, F.; Sun, P. Lactoferrin: Major Physiological Functions and Applications. Curr. Protein Pept. Sci. 2019, 20, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Kowalczyk, P.; Kaczyńska, K.; Kleczkowska, P.; Bukowska-Ośko, I.; Kramkowski, K.; Sulejczak, D. The Lactoferrin Phenomenon—A Miracle Molecule. Molecules 2022, 27, 2941. [Google Scholar] [CrossRef]
- Kruzel, M.L.; Zimecki, M.; Actor, J.K. Lactoferrin in a Context of Inflammation-Induced Pathology. Front. Immunol. 2017, 8, 1438. [Google Scholar] [CrossRef]
- Lepanto, M.S.; Rosa, L.; Paesano, R.; Valenti, P.; Cutone, A. Lactoferrin in Aseptic and Septic Inflammation. Molecules 2019, 24, 1323. [Google Scholar] [CrossRef]
- McGrath, B.A.; Fox, P.F.; McSweeney, P.L.; Kelly, A.L. Composition and properties of bovine colostrum: A review. Dairy Sci. Technol. 2015, 96, 133–158. [Google Scholar] [CrossRef]
- Zarzosa-Moreno, D.; Avalos-Gómez, C.; Ramírez-Texcalco, L.S.; Torres-López, E.; Ramírez-Mondragón, R.; Hernández-Ramírez, J.O.; Serrano-Luna, J.; de la Garza, M. Lactoferrin and its derived peptides: An alternative for combating virulence mechanisms developed by pathogens. Molecules 2020, 25, 5763. [Google Scholar] [CrossRef]
- Davis, P.F.; Greenhill, N.S.; Rowan, A.M.; Schollum, L.M. The safety of New Zealand bovine colostrum: Nutritional and physiological evaluation in rats. Food Chem. Toxicol. 2007, 45, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Thiel, A.; Glávits, R.; Murbach, T.S.; Endres, J.R.; Reddeman, R.; Hirka, G.; Vértesi, A.; Béres, E.; Szakonyiné, I.P. Toxicological evaluations of colostrum ultrafiltrate. Regul. Toxicol. Pharmacol. 2019, 104, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Jańczuk, A.; Brodziak, A.; Czernecki, T.; Król, J. Lactoferrin-The Health-Promoting Properties and Contemporary Application with Genetic Aspects. Foods 2022, 12, 70. [Google Scholar] [CrossRef] [PubMed]
- Takayama, Y.; Aoki, R. Roles of lactoferrin on skin wound healing. Biochem. Cell Biol. 2012, 90, 497–503. [Google Scholar] [CrossRef]
- Wang, B.; Timilsena, Y.P.; Blanch, E.; Adhikari, B. Lactoferrin: Structure, function, denaturation and digestion. Crit. Rev. Food Sci. Nutr. 2019, 59, 580–596. [Google Scholar] [CrossRef]
- Drago-Serrano, M.E.; Rafael Campos-Rodriguez, R.; Carrero, J.C.; de la Garza, M. Lactoferrin and Peptide-derivatives: Antimicrobial Agents with Potential Use in Nonspecific Immunity Modulation. Curr. Pharm. Des. 2018, 24, 1067–1078. [Google Scholar] [CrossRef]
- Ochoa, T.J.; Pezo, A.; Cruz, K.; Chea-Woo, E.; Cleary, T.G. Clinical studies of lactoferrin in children. Biochem. Cell Biol. 2012, 90, 457–467. [Google Scholar] [CrossRef]
- Kaczyńska, K.; Jampolska, M.; Wojciechowski, P.; Sulejczak, D.; Andrzejewski, K.; Zając, D. Potential of Lactoferrin in the Treatment of Lung Diseases. Pharmaceuticals 2023, 16, 192. [Google Scholar] [CrossRef]
- Santos-Pereira, C.; Andrés, M.T.; Fierro, J.F.; Rodrigues, L.R.; Côrte-Real, M. A review on lactoferrin as a proton pump inhibitor. Int. J. Biol. Macromol. 2022, 202, 309–317. [Google Scholar] [CrossRef]
- Liu, N.; Feng, G.; Zhang, X.; Hu, Q.; Sun, S.; Sun, J.; Sun, Y.; Wang, R.; Zhang, Y.; Wang, P.; et al. The Functional Role of Lactoferrin in Intestine Mucosal Immune System and Inflammatory Bowel Disease. Front. Nutr. 2021, 8, 759507. [Google Scholar] [CrossRef]
- Liao, Y.; Jiang, R.; Lönnerdal, B. Biochemical and molecular impacts of lactoferrin on small intestinal growth and development during early life. Biochem. Cell Biol. 2012, 90, 476–484. [Google Scholar] [CrossRef] [PubMed]
- Ramirez-Rico, G.; Drago-Serrano, M.E.; Leon-Sicairos, N.; de la Garza, M. Lactoferrin: A nutraceutical with activity against colorectal cancer. Front. Pharmacol. 2022, 13, 855852. [Google Scholar] [CrossRef] [PubMed]
- Tamano, S.; Sekine, K.; Takase, M.; Yamauchi, K.; Iigo, M.; Tsuda, H. Lack of chronic oral toxicity of chemopreventive bovine lactoferrin in F344/DuCrj rats. Asian Pac. J. Cancer Prev. 2008, 9, 313–316. [Google Scholar] [PubMed]
- Yamauchi, K.; Toida, T.; Nishimura, S.; Nagano, E.; Kusuoka, O.; Teraguchi, S.; Hayasawa, H.; Shimamura, S.; Tomita, M. 13-Week oral repeated administration toxicity study of bovine lactoferrin in rats. Food Chem. Toxicol. 2000, 38, 503–512. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, H.; Yamauchi, K.; Abe, F. Quality control of commercial bovine lactoferrin. Biometals 2018, 31, 313–319. [Google Scholar] [CrossRef]
- European Food Safety Authority, EFSA Panel on Dietetic Products, Nutrition and Allergies, Scientific opinion on bovine lactoferrin. EFSA J. 2012, 10, 2811–2825. [CrossRef]
- US Food and Drug Administration. GRAS Notice No. GRN 669. 2016. Available online: https://www.fda.gov/media/124472/download (accessed on 20 February 2023).
- Kruzel, M.L.; Olszewska, P.; Pazdrak, B.; Krupinska, A.M.; Actor, J.A. New insights into the systemic effects of oral lactoferrin: Transcriptome profiling. Biochem. Cell Biol. 2021, 99, 47–53. [Google Scholar] [CrossRef]
- Kruzel, M.L.; Actor, J.K.; Boldogh, I.; Zimecki, M. Lactoferrin in health and disease. Postepy Hig. Med. Dosw. 2007, 61, 261–267. [Google Scholar]
- Mulder, A.M.; Connellan, P.A.; Oliver, C.J.; Morris, C.A.; Stevenson, L.M. Bovine lactoferrin supplementation supports immune and antioxidant status in healthy human males. Nutr. Res. 2008, 28, 583–589. [Google Scholar] [CrossRef]
- Nguyen, T.K.T.; Niaz, Z.; Kruzel, M.L.; Actor, J.K. Recombinant Human Lactoferrin Reduces Inflammation and Increases Fluoroquinolone Penetration to Primary Granulomas During Mycobacterial Infection of C57Bl/6 Mice. Arch. Immunol. Ther. Exp. 2022, 70, 9. [Google Scholar] [CrossRef]
- Ordaz-Pichardo, C.; León-Sicairos, N.; Hernández-Ramírez, V.I.; Talamás-Rohana, P.; de la Garza, M. Effect of bovine lactoferrin in a therapeutic hamster model of hepatic amoebiasis. Biochem. Cell Biol. 2012, 90, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Jeong, G.-J.; Khan, F.; Khan, S.; Tabassum, N.; Mehta, S.; Kim, Y.-M. Pseudomonas aeruginosa virulence attenuation by inhibiting siderophore functions. Appl. Microbiol. Biotechnol. 2023, 107, 1019–1038. [Google Scholar] [CrossRef] [PubMed]
- Döring, G.; Pfestorf, M.; Botzenhart, K.; Abdallah, M.A. Impact of proteases on iron uptake of Pseudomonas aeruginosa pyoverdin from transferrin and lactoferrin. Infect. Immun. 1988, 56, 291–293. [Google Scholar] [CrossRef] [PubMed]
- Britigan, B.E.; Hayek, M.B.; Doebbeling, B.N.; Fick, R.B., Jr. Transferrin and lactoferrin undergo proteolytic cleavage in the Pseudomonas aeruginosa-infected lungs of patients with cystic fibrosis. Infect. Immun. 1993, 61, 5049–5055. [Google Scholar] [CrossRef]
- Moreau-Marquis, S.; Coutermarsh, B.; Stanton, B.A. Combination of Hypothiocyanite and Lactoferrin (ALX-109) Enhances the Ability of Tobramycin and Aztreonam to Eliminate Pseudomonas Aeruginosa Biofilms Growing on Cystic Fibrosis Airway Epithelial Cells. J. Antimicrob. Chemother. 2015, 70, 160–166. [Google Scholar] [CrossRef]
- Tunney, M.M.; Payne, J.E.; McGrath, S.J.; Einarsson, G.G.; Ingram, R.J.; Gilpin, D.F.; Juarez-Perez, V.; Elborn, J.S. Activity of Hypothiocyanite and Lactoferrin (ALX-009) against Respiratory Cystic Fibrosis Pathogens in Sputum. J. Antimicrob. Chemother. 2018, 73, 3391–3397. [Google Scholar] [CrossRef]
- Chilton, C.H.; Crowther, G.S.; Śpiewak, K.; Brindell, M.; Singh, G.; Wilcox, M.H.; Monaghan, T.M. Potential of lactoferrin to prevent antibiotic-induced Clostridium difficile infection. J. Antimicrob. Chemother. 2016, 71, 975–985. [Google Scholar] [CrossRef]
- Laffan, A.M.; McKenzie, R.; Forti, J.; Conklin, D.; Marcinko, R.; Shrestha, R.; Bellantoni, M.; Greenough, W.B. 3rd Lactoferrin for the prevention of post-antibiotic diarrhea. J. Health Popul. Nutr. 2011, 29, 547–551. [Google Scholar] [CrossRef]
- Lai, Y.-W.; Campbell, L.T.; Wilkins, M.R.; Pang, C.N.I.; Chen, S.; Carter, D.A. Synergy and antagonism between iron chelators and antifungal drugs in Cryptococcus. Int. J. Antimicrob. Agents 2016, 48, 388–394. [Google Scholar] [CrossRef]
- Weber-Dabrowska, B.; Zimecki, M.; Kruzel, M.; Kochanowska, I.; Lusiak-Szelachowska, M. Alternative therapies in antibiotic-resistant infection. Adv. Med. Sci. 2006, 51, 242–244. [Google Scholar]
- Barone, A.; Marchionni, F.S.; Cinquini, C.; Panattoni, A.C.; Toti, P.; Marconcini, S.; Covani, U.; Gabriele, M. Antibiotic treatment to prevent postextraction complications: A monocentric, randomized clinical trial. Preliminary outcomes. Minerva Stomatol. 2017, 66, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Wronowski, M.F.; Kotowska, M.; Banasiuk, M.; Kotowski, A.; Kuzmicka, W.; Albrecht, P. Bovine Lactoferrin in the Prevention of Antibiotic-Associated Diarrhea in Children: A Randomized Clinical Trial. Front. Pediatr. 2021, 9, 675606. [Google Scholar] [CrossRef] [PubMed]
- Tolone, S.; Pellino, V.; Vitaliti, G.; Lanzafame, A.; Tolone, C. Evaluation of Helicobacter pylori eradication in pediatric patients by triple therapy plus lactoferrin and probiotics compared to triple therapy alone. Ital. J. Pediatr. 2012, 38, 63. [Google Scholar] [CrossRef]
- de Bortoli, N.; Leonardi, G.; Ciancia, E.; Merlo, A.; Bellini, M.; Costa, F.; Mumolo, M.G.; Ricchiuti, A.; Cristiani, F.; Santi, S.; et al. Helicobacter pylori eradication: A randomized prospective study of triple therapy versus triple therapy plus lactoferrin and probiotics. Am. J. Gastroenterol. 2007, 102, 951–956. [Google Scholar] [CrossRef]
- Tursi, A.; Elisei, W.; Brandimarte, G.; Giorgetti, G.M.; Modeo, M.E.; Aiello, F. Effect of lactoferrin supplementation on the effectiveness and tolerability of a 7-day quadruple therapy after failure of a first attempt to cure Helicobacter pylori infection. Med. Sci. Monit. 2007, 13, CR187–CR190. [Google Scholar] [PubMed]
- Hablass, F.H.; Lashen, S.A.; Alsayed, E.A. Efficacy of lactoferrin with standard triple therapy or sequential therapy for Helicobacter pylori eradication: A randomized controlled trial. Turk. J. Gastroenterol. 2021, 32, 742–749. [Google Scholar] [CrossRef]
- Andres, M.T.; Fierro, J.F. Antimicrobial mechanism of action of transferrins: Selective inhibition of H+-ATPase. Antimicrob. Agents Chemother. 2010, 54, 4335–4342. [Google Scholar] [CrossRef]
- Playford, R.J.; MacDonald, C.E.; Johnson, W.S. Colostrum and milk-derived peptide growth factors for the treatment of gastrointestinal disorders. Am. J. Clin. Nutr. 2000, 72, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Playford, R.J.; Choudhry, N.; Kelly, P.; Marchbank, T. Effects of bovine colostrum with or without egg on in vitro bacterial-induced intestinal damage with relevance for SIBO and infectious diarrhea. Nutrients 2021, 13, 1024. [Google Scholar] [CrossRef]
- Hung, Y.-P.; Yang, Y.-P.; Wang, H.-C.; Liao, J.-W.; Hsu, W.-L.; Chang, C.-C.; Chang, S.-C. Bovine lactoferrin and piroxicam as an adjunct treatment for lymphocytic-plasmacytic gingivitis stomatitis in cats. Vet. J. 2014, 202, 76–82. [Google Scholar] [CrossRef]
- Dial, E.J.; Dohrman, A.J.; Romero, J.J.; Lichtenberger, L.M. Recombinant human lactoferrin prevents NSAID-induced intestinal bleeding in rodents. J. Pharm. Pharmacol. 2005, 57, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Mir, R.; Singh, N.; Vikram, G.; Kumar, R.P.; Sinha, M.; Bhushan, A.; Kaur, P.; Srinivasan, A.; Sharma, S.; Singh, T.P. The structural basis for the prevention of nonsteroidal antiinflammatory drug-induced gastrointestinal tract damage by the C-lobe of bovine colostrum lactoferrin. Biophys. J. 2009, 97, 3178–3186. [Google Scholar] [CrossRef] [PubMed]
- Fornai, M.; Pellegrini, C.; Benvenuti, L.; Tirotta, E.; Gentile, D.; Natale, G.; Ryskalin, L.; Colucci, R.; Piccoli, E.; Ghelardi, E.; et al. Protective effects of the combination Bifidobacterium longum plus lactoferrin against NSAID-induced enteropathy. Nutrition 2020, 70, 110583. [Google Scholar] [CrossRef] [PubMed]
- Playford, R.J.; Floyd, D.N.; Macdonald, C.E.; Calnan, D.P.; Adenekan, R.O.; Johnson, W.; Goodlad, R.A.; Marchbank, T. Bovine colostrum is a health food supplement which prevents NSAID induced gut damage. Gut 1999, 44, 653–658. [Google Scholar] [CrossRef]
- Playford, R.J.; Garbowsky, M.; Marchbank, T. Pasteurized chicken egg powder stimulates proliferation and migration of AGS, RIE1, and Caco-2 cells and reduces NSAID-induced injury in mice and colitis in rats. J. Nutr. 2020, 150, 1434–1442. [Google Scholar] [CrossRef]
- Playford, R.J.; Cattell, M.; Marchbank, T. Marked variability in bioactivity between commercially available bovine colostrum for human use; implications for clinical trials. PLoS ONE 2020, 15, e0234719. [Google Scholar] [CrossRef]
- Troost, F.J.; Saris, W.H.M.; Brummer, R.-J.M. Recombinant human lactoferrin ingestion attenuates indomethacin-induced enteropathy in vivo in healthy volunteers. Eur. J. Clin. Nutr. 2003, 57, 1579–1585. [Google Scholar] [CrossRef]
- Shimba, A.; Ikuta, K. Control of immunity by glucocorticoids in health and disease. Semin. Immunopathol. 2020, 42, 669–680. [Google Scholar] [CrossRef]
- Shimizu, T.; Kawamura, T.; Miyaji, C.; Oya, H.; Bannai, M.; Yamamoto, S.; Weerasinghe, A.; Halder, R.C.; Watanabe, H.; Hatakeyama, K.; et al. Resistance of extrathymic T cells to stress and the role of endogenous glucocorticoids in stress associated immunosuppression. Scand. J. Immunol. 2000, 51, 285–292. [Google Scholar] [CrossRef]
- Zimecki, M.; Artym, J.; Kocięba, M. Endogenous steroids are responsible for lactoferrin-induced myelopoiesis in mice. Pharmacol. Rep. 2009, 61, 705–710. [Google Scholar] [CrossRef]
- Zimecki, M.; Artym, J.; Chodaczek, G.; Kocięba, M.; Kruzel, M. Effects of lactoferrin on the immune response modified by the immobilization stress. Pharmacol. Rep. 2005, 57, 811–817. [Google Scholar] [PubMed]
- Peña-Juárez, M.C.; Campos-Rodríguez, R.; Godínez-Victoria, M.; Cruz-Hernández, T.R.; Reyna-Garfias, H.; Barbosa-Cabrera, R.E.; Drago-Serrano, M.E. Effect of Bovine Lactoferrin Treatment Followed by Acute Stress on the IgA-Response in Small Intestine of BALB/c mice. Immunol. Investig. 2016, 45, 652–667. [Google Scholar] [CrossRef]
- Cruz-Hernández, T.R.; Gómez-Jiménez, D.C.; Campos-Rodríguez, R.; Godínez-Victoria, M.; Drago-Serrano, M.E. Analysis of the intestinal IgA response in mice exposed to chronic stress and treated with bovine lactoferrin. Mol. Med. Rep. 2021, 23, 126. [Google Scholar] [CrossRef] [PubMed]
- Noda, N.; Aoki, M.; Akiyoshi, H.; Asaki, H.; Ogata, T.; Yamauchi, K.; Shimada, T.; Ohashi, F. Effect of bovine lactoferrin on the immune responses of captive bottlenosed dolphins (Tursiops truncatus) being transported over long distances. Vet. Rec. 2006, 159, 885–888. [Google Scholar] [PubMed]
- Maekawa, Y.; Sugiyama, A.; Takeuchi, T. Lactoferrin ameliorates corticosterone-related acute stress and hyperglycemia in rats. J. Vet. Med. Sci. 2017, 79, 412–417. [Google Scholar] [CrossRef]
- Kamemori, N.; Takeuchi, T.; Hayashida, K.-I.; Harada, E. Suppressive effects of milk-derived lactoferrin on psychological stress in adult rats. Brain Res. 2004, 1029, 34–40. [Google Scholar] [CrossRef]
- Takeuchi, T.; Hayashida, K.I.; Inagaki, H.; Kuwahara, M.; Tsubone, H.; Harada, E. Opioid mediated suppressive effect of milk-derived lactoferrin on distress induced by maternal separation in rat pups. Brain Res. 2003, 979, 216–224. [Google Scholar] [CrossRef]
- Takakura, N.; Wakabayashi, H.; Ishibashi, H.; Yamauchi, K.; Teraguchi, S.; Tamura, Y.; Yamaguchi, H.; Abe, S. Effect of orally administered bovine lactoferrin on the immune response in the oral candidiasis murine model. J. Med. Microbiol. 2004, 53, 495–500. [Google Scholar] [CrossRef]
- Rayner, T.E.; Cowin, A.J.; Robertson, J.G.; Cooter, R.D.; Harries, R.C.; Regester, G.O.; Smithers, G.W.; Goddard, C.; Belford, D.A. Mitogenic whey extract stimulates wound repair activity in vitro and promotes healing of rat incisional wounds. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2000, 278, R1651–R1660. [Google Scholar] [CrossRef]
- Shinjo, T.; Sakuraba, K.; Nakaniida, A.; Ishibashi, T.; Kobayashi, M.; Aono, Y.; Suzuki, Y. Oral lactoferrin influences psychological stress in humans: A single-dose administration crossover study. Biomed. Rep. 2018, 8, 426–432. [Google Scholar] [CrossRef]
- Yoshise, R.E.; Matsuyama, H.; Hosoya, T.; Ogawa, A.; Kadooka, Y. Effects of Fe-lactoferrin via oral administration on mental stress. Milk Sci. 2010, 59, 93–101. [Google Scholar] [CrossRef]
- Costa, R.J.S.; Snipe, R.M.J.; Kitic, C.M.; Gibson, P.R. Systematic review: Exercise-induced gastrointestinal syndrome-implications for health and intestinal disease. Aliment. Pharmacol. Ther. 2017, 46, 246–265. [Google Scholar] [CrossRef] [PubMed]
- Davison, G.; Marchbank, T.; March, D.S.; Thatcher, R.; Playford, R.J. Zinc carnosine works with bovine colostrum in truncating heavy exercise-induced increase in gut permeability in healthy volunteers. Am. J. Clin. Nutr. 2016, 104, 526–536. [Google Scholar] [CrossRef] [PubMed]
- Hałasa, M.; Maciejewska, D.; Baśkiewicz-Hałasa, M.; Machaliński, B.; Safranow, K.; Stachowska, E. Oral supplementation with bovine colostrum decreases intestinal permeability and stool concentrations of zonulin in athletes. Nutrients 2017, 9, 370. [Google Scholar] [CrossRef] [PubMed]
- Hałasa, M.; Maciejewska-Markiewicz, D.; Baskiewicz-Hałasa, M.; Safranow, K.; Stachowska, E. Post-Delivery Milking Delay Influence on the Effect of Oral Supplementation with Bovine Colostrum as Measured with Intestinal Permeability Test. Medicina 2020, 56, 495. [Google Scholar] [CrossRef]
- March, D.S.; Marchbank, T.; Playford, R.J.; Jones, A.; Thatcher, R.; Davison, G. Intestinal fatty acid-binding protein and gut permeability responses to exercise. Eur. J. Appl. Physiol. 2017, 117, 931–941. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Model | Application of Colostrum Proteins | Therapeutic Laboratory or Clinical Effects | Reference |
|---|---|---|---|
| Antibiotic therapy in in vitro and animal models | |||
| Mice infected with Mycobacterium tuberculosis and treated with ofloxacin fluoroquinolone | Orally applied rhLF | LF enabled penetration of the antibiotic to the sites of pathological disruption, increase in macrophage phenotype in the granulomas to M-2-like phenotype | Nguyen T.K.T. et al. (2022) [91] |
| Hamsters infected with amoebae | Intragastrically given bLF (2.5 mg/100 g mass) for 8 days | Prevention of disease symptoms, the liver functions and blood parameters return to normal levels | Ordaz-Pichardo C et al. (2012) [92] |
| Six clinical isolates of P. aeruginosa biofilm grown at the apical surface of human CF airway epithelial cells | bLF-hypothiocyanite combination (ALX-109) combined with tobramycin or aztreonam | ALX-109 alone reduced bacterial biofilm formation but did not disturb the biofilms already formed, enhancement of tobramycin and aztreonam ability to reduce biofilm formation and disrupt existing ones | Morceau-Marquis S. et al. (2015) [96] |
| Sputum from CF patients containing P. aeruginosa and Burkholderia cepacia complex (Bcc) | bLF-hypothiocyanite combination (ALX-009) alone or combined with tobramycin | ALX-009 alone had a bactericidal effect against P. aeruginosa but was more effective in combination with tobramycin | Tunney M.M. (2018) [97] |
| C. difficile infection in triple-stage chemostat gut model inoculated with human feces | Holo-bLF and apo-bLF instilled in the chemostat with simulated CDI, 7 days later clindamycin was instilled | Holo-bLF, but not apo-bLF, delayed growth of C. difficile and prevented toxin production | Chilton C.H. et al. (2016) [98] |
| Cryptococcus strains in in vitro cultures | bLF (and other iron chelators) with antifungal agents (among others, amphotericin B, fluconazole and itraconazole) | Significant synergy between LF and amphotericin B for all Cryptococcus strains, not primarily due to iron chelation but to other properties of LF that were raised in the presence of amphotericin B | Lai Y.-W. et al. (2016) [100] |
| Antibiotic therapy in clinics | |||
| Case study; patient with ineffective treatment of post-influenza otitis with antibiotics and specific bacteriophages | Orally applied bLF (50 mg daily) for 7 days, with two-week intervals | Complete eradication of the inflammation, complete clearance of both bacterial strains (Staphylococcus homis and Staphylococcus epidermidis), increased myelopoiesis and elevated serum LF concentration, and full recovery of the patient | Weber-Dabrowska B. et al. (2006) [101] |
| Monocentric RCT; patients with tooth post-extraction complications; n = 111 | Amoxicillin + clavulanic acid (#1) for 6 days after extraction versus the antibiotics + Bifidobacterium longum + LF (#2) and no antibiotic therapy (#3) | Pain at surgical site relief (pain was present in 48%, 30% and 71.4% of the respective groups #1, 2 and 3) Protection from diarrhea (was recorded in 5 patients in group #1 and in none of the patients in groups #2 and #3) and intestinal distention (in 9 patients in group #1 and 1 patient in group #2) | Barone A. et al. (2017) [102] |
| Double-blind RCT; tube-fed long-term-care adult patients with AAD; n = 30 (males and females) | Orally given (by gastric tube), rhLF (3 g daily) for 8 weeks versus antibiotics only | Fewer patients experienced AAD (including Clostridium difficile diarrhea) Reduced mean number of diarrhea days and the percentage of the study days with AAD Shorter time to first episode of ADD | Laffan A.M. et al. (2011) [99] |
| Randomized clinical trial; children (8.3 ± 3.4 years) treated for Helicobacter pylori infection with standard triple treatment; n = 68 (males and females) | Omeprazole + amoxicillin + clarithromycin (#1), additional probiotic + bLF (no dose specified) (#2) | Alleviation of antibiotic therapy side effects: epigastric pain in 17.6% versus 5.8% of patients, nausea in 8.8% versus 2.9%, vomiting and diarrhea in 5.8% versus 23.5% (group #1 versus group #2) | Tolone S. et al. (2012) [104] |
| Open, prospective, randomized study; adult patients treated for H. pylori infection with standard triple treatment; n = 206 (males and females) | Esomeprazole + clarithromycin + amoxicillin + bLF (400 mg daily) + probiotics for 7 days versus antibiotics only as control | Eradication of H. pylori in 88.6% of the LF + probiotics group and 72.3% of the control group, in 13C-urea breath test Fewer adverse side effects in the LF + probiotics group (in 9.5%) versus control group (in 49.6%) | de Bortoli N. et al. (2007) [105] |
| Prospective, randomized study; adult patients with persistent H. pylori infection, with peptic ulcer or gastritis with severe histological abnormalities failure of the first standard treatment schedule; n = 70 (males and females) | Ranitidine bismuth citrate + esomeprazole + amoxicillin + tinidazole + bLF (400 mg daily) for 7 days versus antibiotics only as control | Eradication of H. pylori in 94.3% of the LF group and 88.6% of the control group, in 13C-urea breath test and histological evaluation Adverse side effects in 17.6% of patients in the LF group and 29.4% of the control group | Tursi A. et al. (2007) [106] |
| Parallel randomized study; adult patients with H. pylori infection with standard triple treatment or standard sequential treatment; n = 400 (males and females) | Esomeprazole + clarithromycin + amoxicillin + bLF (400 mg daily) or esomeprazole + amoxicillin and then esomeprazole + metronidazole + clarithromycin + bLF (400 mg daily) for 15 days | H. pylori eradication in groups without LF: 70.3% and 82.8%; in groups with LF: 85.6% and 94.5% No differences in the frequency of side effects of therapy | Hablass F.H. et al. (2021) [107] |
| NSAID therapy in animal models | |||
| Double-blind RCT, cats with caudal stomatitis treated with piroxicam; n = 13 | bLF in oral spray (2 sprays, 3 mg/spray, 6 mg/cat) with oral piroxicam versus piroxicam alone | Better reduction in oral lesions closely correlated with decreased number of macrophages and improvement of clinical symptoms, quality of life and weight gain | Hung Y.-P. et al. (2014) [111] |
| Rats and mice with NSAID-induced increases in gut bleeding after treating with indomethacin, naproxen and diclophenac | Orally or intraperitoneally applied rhLF (30, 100, 200 or 400 mg/kg b.w.) | Prevention of drug-induced bleeding, inflammation, inhibition of myeloperoxidase activity and neutrophil migration to the intestine; LF activity is independent of prostaglandins and nitric oxide; LF does not bind to the NSAIDs or interfere with the NSAID biological activity | Dial E.J. et al. (2005) [112] |
| Mice with gastrointestinal damage after treatment with indomethacin, diclofenac, aspirin or ibuprofen | Orally applied C lobes (C-terminal half) of bLF prepared proteolytically (200 mg.kg b.w.) | Partial reduction in NSAID-induced injuries (gastropathy) by C lobes of LF applicated after NSAIDs, but better results with co-administration with NSAIDs; NSAID binding to C lobes was demonstrated | Mir R. et al. (2009) [113] |
| Rats with enteropathy after treatment with diclophenac | Orally given LF (100, 200 or 400 mg/kg b.w.) with Bifidobacterium longum versus B. longum alone | LF or Bifidobacterium alone were effective, but the combinatory treatment was more effective in reducing altered parameters in enteropathy, such as histological picture, MPO and MDA levels, TLR2 and TLR4 expression, activation of MyD88 and NFκB p65, blood hemoglobin and fecal calprotectin levels | Fornai M. et al. (2020) [114] |
| Rats and mice with gastro- and enteropathy after treatment with indomethacin; in vitro test | Rat model: Oral pretreatment with BC (0.5 or 1 mg) Mouse model: Addition of BC to drinking water (10% v/v) | Rat model: Reduction in gastric injury by 30% and 60%, respectively, for the doses Mouse model: Reduction in villus shortening in small intestine In in vitro test: Increased proliferation and migration of intestinal epithelial cell lines: human HT-29 and rat RIE-1 | Playford R.J. et al. (1999) [115] |
| Mice with enteropathy after treatment with indomethacin Rats with chemically induced colitis | Mouse model: Oral pretreatment with BC (20 mg/kg b.w.) for 7 days Rat model: Oral pretreatment with BC (20 mg/kg b.w.) for 9 days | Reduced shortening of intestinal villi in mice by 34% and colonic damage in rats by 44–61% In in vitro test, 3-fold increase in epithelial cell (Caco-2, RIE-1 and AGS) proliferation and migration | Playford R.J., Garbowsky M., Marchbank T. (2020) [116] |
| Rats with gastric damage after indomethacin and short-term (3 h) restraint stress; in vitro test | Oral pretreatment with BC (14 mg/rat, 20 commercial BC products) in single dose 30 min. before indomethacin application and placement in restraint cages | Reduced macroscopic gastric injures by 48% and 86%, for least active and most active BC samples Reduced microscopic injures (histological ulcer score) by 15% and 74%, for least active and most active BC samples In in vitro test, increase in epithelial cell (Caco-2, RIE-1 and AGS) proliferation and migration | Playford R.J., Cattell M., Marchbank T. (2020) [117] |
| NSAID therapy in clinics | |||
| A randomized cross-over, double-blind trial: Healthy volunteers treated with indomethacin for 5 days; n = 7 (males) Adult patients taking a substantial, regular dose of an NSAID for clinical reasons; n = 15 (male and female) | Healthy volunteers: Orally applied BC (125 mL, three times daily) with indomethacin for 7 days; Patients: Orally applied BC (125 mL, three times daily) for 7 days In both studies, whey protein as control | Healthy volunteers: 3-fold increase in gut permeability (lactulose/rhamnose test) in the control arm and no significant increase in permeability when BC was co-administered Patients: Initial gut permeability was low despite continuing with the drug, and was not influenced by co-administration of BC (possibly as an adaptation to long-term NSAID therapy) | Playford R.J. et al. (2001) [48] |
| A randomized cross-over dietary intervention; human volunteers given indomethacin versus placebo; n = 15 (males) | Orally applied rhLF (5 g in single dose) before indomethacin application | Small intestine permeability in lactulose/rhamnose test lower in LF group versus the placebo group | Troost F.J. (2003) [118] |
| Steroid therapy and psychic stress in animal models | |||
| Mice under long-term (5 h daily for 5 days) and short-term (5 h) immobilization stress | 0.5% bLF in drinking water | Restoration of DTH to OVA and HIR to SRBCs in long-term stress, reduced production of TGF-β by mesenteric lymph node lymphocytes Reduction in DTH in short-term stress | Zimecki M. et al. (2005) [122] |
| Mice under acute immobilization stress | Orally applied bLF (0.05, 0.5 or 5 mg) for 7 days before stress | Induction of higher levels of IgA, sIgA, pIgR, IL-4 and IL-6 in the intestine, higher levels of plasma cortisone in LF- and LF/stressed mice | Pena-Juarez M.C. et al. (2016) [123] |
| Mice under chronic (7-day) immobilization stress | Orally applied bLF (0.05, 0.5 or 5 mg) for 7 days before stress | Suppression of total antibody levels, α-chain, expression of polymeric IgR and IL-6 | Cruz-Hernandez T.R. et al. (2021) [124] |
| Captive dolphins under 6h-transport as a source of stress | bLF (40 mg/kg b.w.) in feed before transportation | No effect on serum cortisol or lymphopenia, but lower eosinophilia in circulating blood | Noda N. et al. (2006) [125] |
| Rats under short immobilization stress | bLF (100 mg/kg b.w.) given i.p. before the stress | Stress significantly increased plasma glucose levels Plasma glucose levels in the oral glucose tolerance test were significantly decreased in the LF group Lowering increased plasma corticosterone levels during stress; no effect on insulin, epinephrine or glucagon levels | Maekawa Y. et al. (2017) [126] |
| 5-8-day-old rat pups under maternal separation stress | bLF (100 mg/kg b.w.) i.p. 30 min. before the behavioral separation test | Suppression of distress activity (body movements and ultrasonic vocalizations), LF effects in CNS are opioid- and NO-mediated | Takeuchi T. et al. (2003) [128] |
| Adult rats under stress in freezing test and maze test | bLF (30 or 100 mg/kg b.w.) i.p. | Suppression of distress activity, LF effects in CNS are opioid- and NO-mediated | Kamemori N. et al. (2004) [127] |
| Mice with oral candidasis after immunosuppression with prednisolone Ex vivo tests in lymph node lymphocytes | 0.3% bLF (equivalent of 0.5 g/kg b.w.) in drinking water | Prevention of decline in peripheral blood leukocyte number Increased antigen-specific production of IL-12, IFN-γ and TNF-α by cervical lymph node lymphocytes from LF-treated mice inversely correlated with Candida albicans load in oral cavity | Takakura N. et al. (2004) [129] |
| Methylprednisolone-treated rats with experimentally induced wounds | Bovine-milk-derived growth-factor-enriched preparation applicated to wounds | Promotion of cutaneous repair in normal and steroid-treated rats Increase in the cellular infiltrate and fibroblast activity, but not the inflammatory scores in wounds in both normal and steroid-treated rats | Rayner T.E. et al. (2000) [130] |
| Psychic and psychophysical stress in clinics | |||
| Placebo-controlled cross-over study; adult subjects under mental stress when solving a calculation task; n = 24 | Orally applied bLF (0.8 g) in single dose | Improvements in CNS, AUS and immune response: normalization of brain waves, improvement of scores in calculation tests, reduction in POMS scores (anger–hostility, vigor, fatigue, confusion) Increase in salivary sIgA level | Yoshise R.E. et al. (2010) [132] |
| Single-dose, double-blind, placebo-controlled cross-over RCT; college students who solved a calculation task; n = 16 (female) | Orally applied bLF (0.8 g) in single dose versus placebo (soy milk) as control | Normalization of the activity of parasympathetic and sympathetic neural system | Shinjo T. et al. (2018) [131] |
| Double-blind cross-over RCT; actively training healthy adult volunteers; n = 8 (males) In vitro test | Orally applied commercial BC preparation (20 g) plus zinc carnosine daily for 2 weeks versus isocaloric milk protein preparation as control | Reduced increased intestinal permeability (as measured by the lactulose/rhamnose test) In in vitro tests, increased the tightness of the intestinal epithelium Caco-2 and HT-29 cell lines Increase in Hsp7 protein and total occludin, decrease in phosphorylated ZO-1 and occludin, decrease in proapoptotic proteins (Bax and caspase-3 and -9) | Davison G. et al. (2016) [134] |
| Double-blind and open-label cross-over RCT; healthy adult athletes; n = 16 (males) | Orally applied commercial 2 h BC preparation (1 g) daily for 3 weeks versus isocaloric whey protein preparation as control | Reduced intestinal permeability (as measured by the lactulose/mannitol differential sugar absorption test) Lower levels of zonulin in the circulation, reflecting less damage to the intestinal epithelium Fewer cases of URTIs | Hałasa (2017) [135] |
| Double-blind RCT; healthy adult athletes; n = 31 (males and females) | Orally applied commercial 2 h BC preparation (1 g) daily for 3 weeks versus 24 h BC, 72 h BC and isocaloric whey protein preparation as control | Reduced intestinal permeability (as measured by the lactulose/mannitol differential sugar absorption test) only in 2 h BC and 24 h BC groups | Hałasa (2020) [136] |
| Double-blind cross-over RCT; healthy adult athletes; n = 18 (males) | Orally applied commercial BC preparation (20 g) daily for 2 weeks versus isocaloric protein preparation as control | Reduced intestinal permeability (as measured by the lactulose/rhamnose test) increased after an intensive run for 1 h Smaller increase in serum protein I-FABP, a marker of intestinal epithelial damage | March D.S. et al. (2017) [137] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Artym, J.; Zimecki, M. Colostrum and Lactoferrin Protect against Side Effects of Therapy with Antibiotics, Anti-inflammatory Drugs and Steroids, and Psychophysical Stress: A Comprehensive Review. Biomedicines 2023, 11, 1015. https://doi.org/10.3390/biomedicines11041015
Artym J, Zimecki M. Colostrum and Lactoferrin Protect against Side Effects of Therapy with Antibiotics, Anti-inflammatory Drugs and Steroids, and Psychophysical Stress: A Comprehensive Review. Biomedicines. 2023; 11(4):1015. https://doi.org/10.3390/biomedicines11041015
Chicago/Turabian StyleArtym, Jolanta, and Michał Zimecki. 2023. "Colostrum and Lactoferrin Protect against Side Effects of Therapy with Antibiotics, Anti-inflammatory Drugs and Steroids, and Psychophysical Stress: A Comprehensive Review" Biomedicines 11, no. 4: 1015. https://doi.org/10.3390/biomedicines11041015