
Challenging the Pleiotropic Effects of Repetitive Transcranial Magnetic Stimulation in Geriatric Depression: A Multimodal Case Series Study

 , , , , ,
, , , , ,  , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Baseline Assessment
2.3. Laboratory Investigations
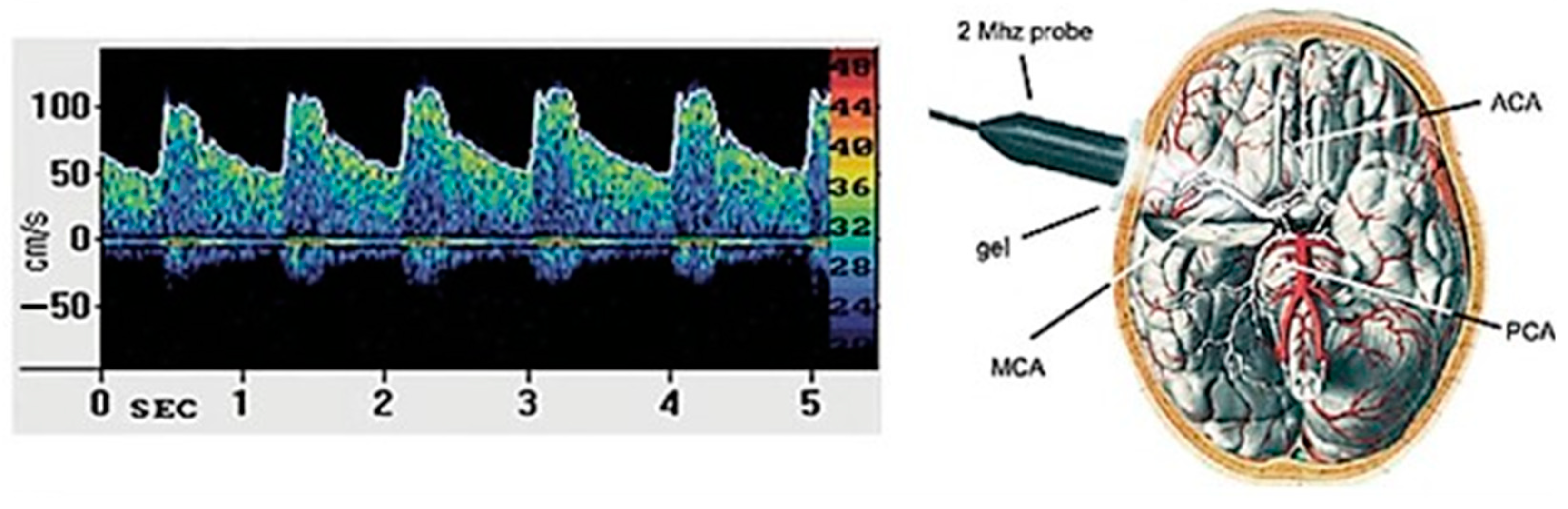
2.4. Transcranial Doppler Sonography
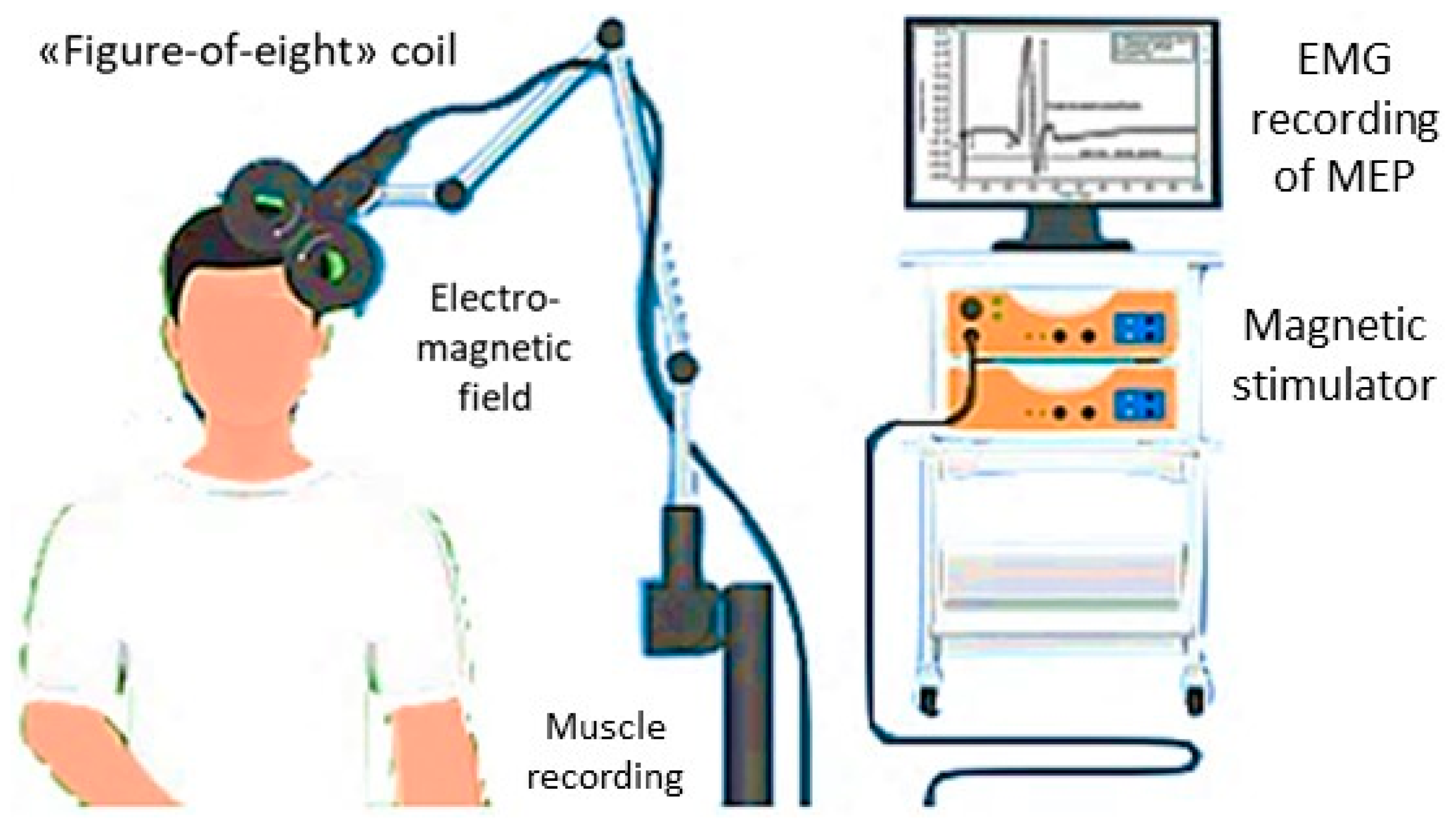
2.5. Transcranial Magnetic Stimulation
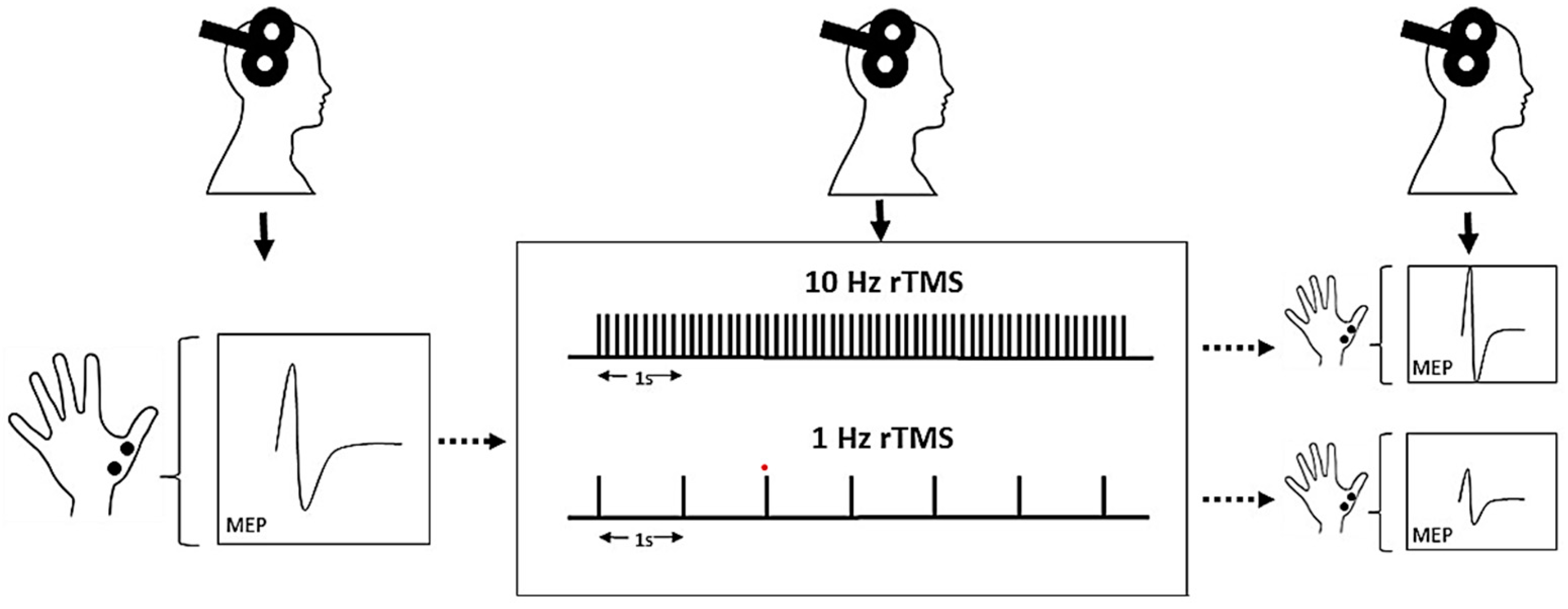
2.6. Repetitive Transcranial Magnetic Stimulation
2.7. Statistical Analysis
3. Results
3.1. Descriptive Data
3.2. General Considerations
4. Discussion
4.1. Proposed Pathomechanisms
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Friedrich, M.J. Depression Is the Leading Cause of Disability Around the World. JAMA 2017, 317, 1517. [Google Scholar] [CrossRef] [PubMed]
- Roberto, N.; Portella, M.J.; Marquié, M.; Alegret, M.; Hernández, I.; Mauleón, A.; Rosende-Roca, M.; Abdelnour, C.; de Antonio, E.E.; Gil, S.; et al. Neuropsychiatric profiles and conversion to dementia in mild cognitive impairment, a latent class analysis. Sci. Rep. 2021, 11, 6448. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, P.E.; Fournier, A.-A.; Sisitsky, T.; Pike, C.T.; Kessler, R.C. The economic burden of adults with major depressive disorder in the United States (2005 and 2010). J. Clin. Psychiatry 2015, 76, 155–162. [Google Scholar] [CrossRef] [Green Version]
- Román, G.C. Vascular depression: An archetypal neuropsychiatric disorder. Biol. Psychiatry 2006, 60, 1306–1308. [Google Scholar] [CrossRef] [PubMed]
- Caruso, P.; Signori, R.; Moretti, R. Small vessel disease to subcortical dementia: A dynamic model, which interfaces aging, cholinergic dysregulation and the neurovascular unit. Vasc. Health Risk Manag. 2019, 15, 259–281. [Google Scholar] [CrossRef] [PubMed]
- Sopova, K.; Gatsiou, K.; Stellos, K.; Laske, C. Dysregulation of Neurotrophic and Haematopoietic Growth Factors in Alzheimer’s Disease: From Pathophysiology to Novel Treatment Strategies. Curr. Alzheimer Res. 2014, 11, 27–39. [Google Scholar] [CrossRef]
- Levy, M.J.F.; Boulle, F.; Steinbusch, H.W.; van den Hove, D.L.A.; Kenis, G.; Lanfumey, L. Neurotrophic factors and neuroplasticity pathways in the pathophysiology and treatment of depression. Psychopharmacology 2018, 235, 2195–2220. [Google Scholar] [CrossRef] [Green Version]
- Cowansage, K.K.; LeDoux, J.E.; Monfils, M.-H. Brain-Derived Neurotrophic Factor: A Dynamic Gatekeeper of Neural Plasticity. Curr. Mol. Pharmacol. 2010, 3, 12–29. [Google Scholar] [CrossRef]
- Gottmann, K.; Mittmann, T.; Lessmann, V. BDNF signaling in the formation, maturation and plasticity of glutamatergic and GABAergic synapses. Exp. Brain Res. 2009, 199, 203–234. [Google Scholar] [CrossRef]
- Ventriglia, M.; Zanardini, R.; Pedrini, L.; Placentino, A.; Nielsen, M.G.; Gennarelli, M.; Bocchio-Chiavetto, L. VEGF serum levels in depressed patients during SSRI antidepressant treatment. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2009, 33, 146–149. [Google Scholar] [CrossRef]
- Mateo, I.; Llorca, J.; Infante, J.; Rodríguez-Rodríguez, E.; Fernández-Viadero, C.; Peña, N.; Berciano, J.; Combarros, O. Low serum VEGF levels are associated with Alzheimer’s disease. Acta Neurol. Scand. 2007, 116, 56–58. [Google Scholar] [CrossRef] [PubMed]
- Diniz, B.S.; Sibille, E.; Ding, Y.; Tseng, G.; Aizenstein, H.J.; Lotrich, F.; Becker, J.T.; Lopez, O.L.; Lotze, M.T.; Klunk, W.E.; et al. Plasma biosignature and brain pathology related to persistent cognitive impairment in late-life depression. Mol. Psychiatry 2015, 20, 594–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnsen, S.P.; Hundborg, H.H.; Sørensen, H.T.; Ørskov, H.; Tjønneland, A.; Overvad, K.; Jørgensen, J.O.L. Insulin-Like Growth Factor (IGF) I, -II, and IGF Binding Protein-3 and Risk of Ischemic Stroke. J. Clin. Endocrinol. Metab. 2005, 90, 5937–5941. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.-K.; Miller, I.; Aja, S.; Landree, L.E.; Pinn, M.; McFadden, J.; Kuhajda, F.P.; Moran, T.H.; Ronnett, G.V. C75, a fatty acid synthase inhibitor, reduces food intake via hypothalamic AMP-activated protein kinase. J. Biol. Chem. 2004, 279, 19970–19976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstead, W.M.; Raghupathi, R. Endothelin and the neurovascular unit in pediatric traumatic brain injury. Neurol. Res. 2011, 33, 127–132. [Google Scholar] [CrossRef] [Green Version]
- Lake, E.M.R.; Bazzigaluppi, P.; Mester, J.; Thomason, L.A.M.; Janik, R.; Brown, M.; McLaurin, J.; Carlen, P.L.; Corbett, D.; Stanisz, G.J.; et al. Neurovascular unit remodelling in the subacute stage of stroke recovery. Neuroimage 2017, 146, 869–882. [Google Scholar] [CrossRef]
- Cantone, M.; Lanza, G.; Fisicaro, F.; Pennisi, M.; Bella, R.; Di Lazzaro, V.; Di Pino, G. Evaluation and Treatment of Vascular Cognitive Impairment by Transcranial Magnetic Stimulation. Neural Plasticity 2020, 2020, 8820881. [Google Scholar] [CrossRef]
- Cantone, M.; Lanza, G.; Ranieri, F.; Opie, G.M.; Terranova, C. Editorial: Non-invasive Brain Stimulation in the Study and Modulation of Metaplasticity in Neurological Disorders. Front. Neurol. 2021, 12, 721906. [Google Scholar] [CrossRef]
- Parkes, I.; Chintawar, S.; Cader, M.Z. Neurovascular dysfunction in dementia—Human cellular models and molecular mechanisms. Clin. Sci. 2018, 132, 399–418. [Google Scholar] [CrossRef]
- Fabiani, M.; Gordon, B.A.; Maclin, E.L.; Pearson, M.A.; Brumback-Peltz, C.R.; Low, K.A.; McAuley, E.; Sutton, B.P.; Kramer, A.F.; Gratton, G. Neurovascular coupling in normal aging: A combined optical, ERP and fMRI study. Neuroimage 2014, 85 Pt 1, 592–607. [Google Scholar] [CrossRef] [Green Version]
- Sorond, F.A.; Hurwitz, S.; Salat, D.H.; Greve, D.N.; Fisher, N.D.L. Neurovascular coupling, cerebral white matter integrity, and response to cocoa in older people. Neurology 2013, 81, 904–909. [Google Scholar] [CrossRef]
- Tarantini, S.; Hertelendy, P.; Tucsek, Z.; Valcarcel-Ares, M.N.; Smith, N.; Menyhart, A.; Farkas, E.; Hodges, E.L.; Towner, R.; Deak, F.; et al. Pharmacologically-induced neurovascular uncoupling is associated with cognitive impairment in mice. J. Cereb. Blood Flow Metab. 2015, 35, 1871–1881. [Google Scholar] [CrossRef] [Green Version]
- Greden, J.F. The burden of disease for treatment-resistant depression. J. Clin. Psychiatry 2001, 62 (Suppl. S16), 26–31. [Google Scholar]
- Rush, A.J.; Trivedi, M.H.; Wisniewski, S.R.; Nierenberg, A.A.; Stewart, J.W.; Warden, D.; Niederehe, G.; Thase, M.E.; Lavori, P.W.; Lebowitz, B.D.; et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: A STAR*D report. Am. J. Psychiatry 2006, 163, 1905–1917. [Google Scholar] [CrossRef]
- Tedeschini, E.; Levkovitz, Y.; Iovieno, N.; Ameral, V.E.; Nelson, J.C.; Papakostas, G.I. Efficacy of antidepressants for late-life depression: A meta-analysis and meta-regression of placebo-controlled randomized trials. J. Clin. Psychiatry 2011, 72, 1660–1668. [Google Scholar] [CrossRef]
- Cantone, M.; Lanza, G.; Vinciguerra, L.; Puglisi, V.; Ricceri, R.; Fisicaro, F.; Vagli, C.; Bella, R.; Ferri, R.; Pennisi, G.; et al. Age, Height, and Sex on Motor Evoked Potentials: Translational Data from a Large Italian Cohort in a Clinical Environment. Front Hum. Neurosci 2019, 13, 185. [Google Scholar] [CrossRef]
- Lanza, G.; Cantone, M.; Puglisi, V.; Vinciguerra, L.; Fisicaro, F.; Vagli, C.; Bella, R.; Pennisi, G.; Di Lazzaro, V.; Pennisi, M. “Mute” plantar response: Does the cortico-spinal tract “speak”? Brain Stimul. 2019, 12, 1579–1580. [Google Scholar] [CrossRef]
- Cantone, M.; Lanza, G.; Le Pira, A.; Barone, R.; Pennisi, G.; Bella, R.; Pennisi, M.; Fiumara, A. Adjunct Diagnostic Value of Transcranial Magnetic Stimulation in Mucopolysaccharidosis-Related Cervical Myelopathy: A Pilot Study. Brain Sci. 2019, 9, 200. [Google Scholar] [CrossRef] [Green Version]
- Lanza, G.; Puglisi, V.; Vinciguerra, L.; Fisicaro, F.; Vagli, C.; Cantone, M.; Pennisi, G.; Pennisi, M.; Bella, R. TMS Correlates of Pyramidal Tract Signs and Clinical Motor Status in Patients with Cervical Spondylotic Myelopathy. Brain Sci. 2020, 10, 806. [Google Scholar] [CrossRef]
- Rossini, P.M.; Burke, D.; Chen, R.; Cohen, L.G.; Daskalakis, Z.; Di Iorio, R.; Di Lazzaro, V.; Ferreri, F.; Fitzgerald, P.B.; George, M.S.; et al. Non-invasive electrical and magnetic stimulation of the brain, spinal cord, roots and peripheral nerves: Basic principles and procedures for routine clinical and research application. An updated report from an I.F.C.N. Committee. Clin. Neurophysiol. 2015, 126, 1071–1107. [Google Scholar] [CrossRef]
- Bella, R.; Ferri, R.; Lanza, G.; Cantone, M.; Pennisi, M.; Puglisi, V.; Vinciguerra, L.; Spampinato, C.; Mazza, T.; Malaguarnera, G.; et al. TMS follow-up study in patients with vascular cognitive impairment-no dementia. Neurosci. Lett. 2013, 534, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Lanza, G.; Bella, R.; Giuffrida, S.; Cantone, M.; Pennisi, G.; Spampinato, C.; Giordano, D.; Malaguarnera, G.; Raggi, A.; Pennisi, M. Preserved transcallosal inhibition to transcranial magnetic stimulation in nondemented elderly patients with leukoaraiosis. Biomed Res. Int. 2013, 2013, 351680. [Google Scholar] [CrossRef] [PubMed]
- Pennisi, M.; Lanza, G.; Cantone, M.; Ricceri, R.; Ferri, R.; D’Agate, C.C.; Pennisi, G.; Di Lazzaro, V.; Bella, R. Cortical involvement in celiac disease before and after long-term gluten-free diet: A Transcranial Magnetic Stimulation study. PLoS ONE 2017, 12, e0177560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bella, R.; Ferri, R.; Cantone, M.; Pennisi, M.; Lanza, G.; Malaguarnera, G.; Spampinato, C.; Giordano, D.; Raggi, A.; Pennisi, G. Motor cortex excitability in vascular depression. Int. J. Psychophysiol. 2011, 82, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Fisicaro, F.; Lanza, G.; Cantone, M.; Ferri, R.; Pennisi, G.; Nicoletti, A.; Zappia, M.; Bella, R.; Pennisi, M. Clinical and Electrophysiological Hints to TMS in de novo Patients with Parkinson’s Disease and Progressive Supranuclear Palsy. J. Pers. Med. 2020, 10, 274. [Google Scholar] [CrossRef]
- Lanza, G.; Aricò, D.; Lanuzza, B.; Cosentino, F.I.I.; Tripodi, M.; Giardina, F.; Bella, R.; Puligheddu, M.; Pennisi, G.; Ferri, R.; et al. Facilitatory/inhibitory intracortical imbalance in REM sleep behavior disorder: Early electrophysiological marker of neurodegeneration? Sleep 2020, 43, zsz242. [Google Scholar] [CrossRef]
- Lanza, G.; Bella, R.; Cantone, M.; Pennisi, G.; Ferri, R.; Pennisi, M. Cognitive Impairment and Celiac Disease: Is Transcranial Magnetic Stimulation a Trait d’Union between Gut and Brain? Int. J. Mol. Sci. 2018, 19, 2243. [Google Scholar] [CrossRef] [Green Version]
- Fisicaro, F.; Lanza, G.; Bella, R.; Pennisi, M. “Self-Neuroenhancement”: The Last Frontier of Noninvasive Brain Stimulation? J. Clin. Neurol. 2020, 16, 158–159. [Google Scholar] [CrossRef]
- Lanza, G.; Fisicaro, F.; Cantone, M.; Pennisi, M.; Cosentino, F.I.I.; Lanuzza, B.; Tripodi, M.; Bella, R.; Paulus, W.; Ferri, R. Repetitive transcranial magnetic stimulation in primary sleep disorders. Sleep Med. Rev. 2023, 67, 101735. [Google Scholar] [CrossRef]
- Concerto, C.; Lanza, G.; Fisicaro, F.; Pennisi, M.; Rodolico, A.; Torrisi, G.; Bella, R.; Aguglia, E. Repetitive transcranial magnetic stimulation for post-traumatic stress disorder: Lights and shadows. World J. Clin. Cases 2022, 10, 5929–5933. [Google Scholar] [CrossRef]
- George, M.S.; Lisanby, S.H.; Avery, D.; McDonald, W.M.; Durkalski, V.; Pavlicova, M.; Anderson, B.; Nahas, Z.; Bulow, P.; Zarkowski, P.; et al. Daily left prefrontal transcranial magnetic stimulation therapy for major depressive disorder: A sham-controlled randomized trial. Arch. Gen. Psychiatry 2010, 67, 507–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ning, L.; Rathi, Y.; Barbour, T.; Makris, N.; Camprodon, J.A. White matter markers and predictors for subject-specific rTMS response in major depressive disorder. J. Affect. Disord. 2022, 299, 207–214. [Google Scholar] [CrossRef]
- McIntyre, A.; Thompson, S.; Burhan, A.; Mehta, S.; Teasell, R. Repetitive Transcranial Magnetic Stimulation for Depression Due to Cerebrovascular Disease: A Systematic Review. J. Stroke Cerebrovasc. Dis. 2016, 25, 2792–2800. [Google Scholar] [CrossRef] [PubMed]
- Cantone, M.; Bramanti, A.; Lanza, G.; Pennisi, M.; Bramanti, P.; Pennisi, G.; Bella, R. Cortical Plasticity in Depression. ASN Neuro 2017, 9, 1759091417711512. [Google Scholar] [CrossRef] [Green Version]
- Teffer, K.; Semendeferi, K. Human prefrontal cortex: Evolution, development, and pathology. Prog. Brain Res. 2012, 195, 191–218. [Google Scholar] [CrossRef]
- Lefaucheur, J.-P.; Aleman, A.; Baeken, C.; Benninger, D.H.; Brunelin, J.; Di Lazzaro, V.; Filipović, S.R.; Grefkes, C.; Hasan, A.; Hummel, F.C.; et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): An update (2014–2018). Clin. Neurophysiol. 2020, 131, 474–528. [Google Scholar] [CrossRef]
- Oldfield, R.C. The assessment and analysis of handedness: The Edinburgh inventory. Neuropsychologia 1971, 9, 97–113. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Pub: Washington, DC, USA, 2013; ISBN 978-0-89042-557-2. [Google Scholar]
- Sforzini, L.; Worrell, C.; Kose, M.; Anderson, I.M.; Aouizerate, B.; Arolt, V.; Bauer, M.; Baune, B.T.; Blier, P.; Cleare, A.J.; et al. A Delphi-method-based consensus guideline for definition of treatment-resistant depression for clinical trials. Mol. Psychiatry 2022, 27, 1286–1299. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Morris, J.C. Clinical Dementia Rating: A Reliable and Valid Diagnostic and Staging Measure for Dementia of the Alzheimer Type. Int. Psychogeriatr. 1997, 9, 173–176. [Google Scholar] [CrossRef]
- Gagnier, J.J.; Kienle, G.; Altman, D.G.; Moher, D.; Sox, H.; Riley, D.; CARE Group. The CARE guidelines: Consensus-based clinical case reporting guideline development. BMJ Case Rep. 2013, 2013, bcr2013201554. [Google Scholar] [CrossRef] [Green Version]
- Appollonio, I.; Leone, M.; Isella, V.; Piamarta, F.; Consoli, T.; Villa, M.L.; Forapani, E.; Russo, A.; Nichelli, P. The Frontal Assessment Battery (FAB): Normative values in an Italian population sample. Neurol. Sci. 2005, 26, 108–116. [Google Scholar] [CrossRef]
- Caffarra, P.; Vezzadini, G.; Dieci, F.; Zonato, F.; Venneri, A. Una versione abbreviata del test di Stroop: Dati normativi nella popolazione Italiana. Riv. Neurol. 2002, 12, 111–115. [Google Scholar]
- Katz, S. Assessing self-maintenance: Activities of daily living, mobility, and instrumental activities of daily living. J. Am. Geriatr. Soc. 1983, 31, 721–727. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [Green Version]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef]
- Strauss, M.E.; Sperry, S.D. An informant-based assessment of apathy in Alzheimer disease. Cogn. Behav. Neurol. 2002, 15, 176–183. [Google Scholar]
- Fazekas, F.; Chawluk, J.B.; Alavi, A.; Hurtig, H.I.; Zimmerman, R.A. MR signal abnormalities at 1.5 T in Alzheimer’s dementia and normal aging. Am. J. Neuroradiol. 1987, 149, 351–356. [Google Scholar] [CrossRef] [Green Version]
- Sharma, V.K.; Wong, K.S.; Alexandrov, A.V. Transcranial Doppler. Front. Neurol. Neurosci. 2016, 40, 124–140. [Google Scholar] [CrossRef]
- Fisicaro, F.; Lanza, G.; D’Agate, C.C.; Pennisi, M.; Cantone, M.; Pennisi, G.; Hadjivassiliou, M.; Bella, R. Cerebral hemodynamic changes to transcranial Doppler sonography in celiac disease: A pilot study. Front. Hum. Neurosci. 2022, 16. [Google Scholar] [CrossRef] [PubMed]
- Vagli, C.; Fisicaro, F.; Vinciguerra, L.; Puglisi, V.; Rodolico, M.S.; Giordano, A.; Ferri, R.; Lanza, G.; Bella, R. Cerebral Hemodynamic Changes to Transcranial Doppler in Asymptomatic Patients with Fabry’s Disease. Brain Sci. 2020, 10, 546. [Google Scholar] [CrossRef] [PubMed]
- Puglisi, V.; Bramanti, A.; Lanza, G.; Cantone, M.; Vinciguerra, L.; Pennisi, M.; Bonanno, L.; Pennisi, G.; Bella, R. Impaired Cerebral Haemodynamics in Vascular Depression: Insights From Transcranial Doppler Ultrasonography. Front. Psychiatry 2018, 9, 316. [Google Scholar] [CrossRef] [Green Version]
- Vinciguerra, L.; Lanza, G.; Puglisi, V.; Pennisi, M.; Cantone, M.; Bramanti, A.; Pennisi, G.; Bella, R. Transcranial Doppler ultrasound in vascular cognitive impairment-no dementia. PLoS ONE 2019, 14, e0216162. [Google Scholar] [CrossRef] [Green Version]
- Gosling, R.G.; King, D.H. Arterial Assessment by Doppler-shift Ultrasound. Proc. R. Soc. Med. 1974, 67, 447–449. [Google Scholar] [PubMed]
- D’Andrea, A.; Conte, M.; Cavallaro, M.; Scarafile, R.; Riegler, L.; Cocchia, R.; Pezzullo, E.; Carbone, A.; Natale, F.; Santoro, G.; et al. Transcranial Doppler ultrasonography: From methodology to major clinical applications. World J. Cardiol. 2016, 8, 383–400. [Google Scholar] [CrossRef] [PubMed]
- Ziemann, U.; Reis, J.; Schwenkreis, P.; Rosanova, M.; Strafella, A.; Badawy, R.; Müller-Dahlhaus, F. TMS and drugs revisited 2014. Clin. Neurophysiol. 2015, 126, 1847–1868. [Google Scholar] [CrossRef]
- Paulus, W.; Classen, J.; Cohen, L.G.; Large, C.H.; Di Lazzaro, V.; Nitsche, M.; Pascual-Leone, A.; Rosenow, F.; Rothwell, J.C.; Ziemann, U. State of the art: Pharmacologic effects on cortical excitability measures tested by transcranial magnetic stimulation. Brain Stimul. 2008, 1, 151–163. [Google Scholar] [CrossRef]
- Wassermann, E.M.; Fuhr, P.; Cohen, L.G.; Hallett, M. Effects of transcranial magnetic stimulation on ipsilateral muscles. Neurology 1991, 41, 1795–1799. [Google Scholar] [CrossRef]
- Hupfeld, K.E.; Swanson, C.W.; Fling, B.W.; Seidler, R.D. TMS-induced silent periods: A review of methods and call for consistency. J. Neurosci. Methods 2020, 346, 108950. [Google Scholar] [CrossRef]
- Faro, A.; Giordano, D.; Kavasidis, I.; Pino, C.; Spampinato, C.; Cantone, M.G.; Lanza, G.; Pennisi, M. An Interactive Tool for Customizing Clinical Transacranial Magnetic Stimulation (TMS) Experiments. In Proceedings of the XII Mediterranean Conference on Medical and Biological Engineering and Computing 2010, Chalkidiki, Greece, 27–30 May 2010; Bamidis, P.D., Pallikarakis, N., Eds.; Springer: Berlin/Heidelberg, Germany, 2010; pp. 200–203. [Google Scholar]
- Hayasaka, S.; Nakamura, M.; Noda, Y.; Izuno, T.; Saeki, T.; Iwanari, H.; Hirayasu, Y. Lateralized hippocampal volume increase following high-frequency left prefrontal repetitive transcranial magnetic stimulation in patients with major depression. Psychiatry Clin. Neurosci. 2017, 71, 747–758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jorge, R.E.; Moser, D.J.; Acion, L.; Robinson, R.G. Treatment of vascular depression using repetitive transcranial magnetic stimulation. Arch. Gen. Psychiatry 2008, 65, 268–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pascual-Leone, A.; Rubio, B.; Pallardó, F.; Catalá, M.D. Rapid-rate transcranial magnetic stimulation of left dorsolateral prefrontal cortex in drug-resistant depression. Lancet 1996, 348, 233–237. [Google Scholar] [CrossRef]
- Perera, T.; George, M.S.; Grammer, G.; Janicak, P.G.; Pascual-Leone, A.; Wiercki, T.S. The Clinical TMS Society Consensus Review and Treatment Recommendations for TMS Therapy for Major Depressive Disorder. Brain Stimul. 2016, 9, 336–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kricheldorff, J.; Göke, K.; Kiebs, M.; Kasten, F.H.; Herrmann, C.S.; Witt, K.; Hurlemann, R. Evidence of Neuroplastic Changes after Transcranial Magnetic, Electric, and Deep Brain Stimulation. Brain Sci. 2022, 12, 929. [Google Scholar] [CrossRef] [PubMed]
- Pecuch, P.W.; Evers, S.; Folkerts, H.W.; Michael, N.; Arolt, V. The cerebral hemodynamics of repetitive transcranial magnetic stimulation. Eur. Arch Psychiatry Clin. Neurosci. 2000, 250, 320–324. [Google Scholar] [CrossRef]
- Vernieri, F.; Maggio, P.; Tibuzzi, F.; Filippi, M.M.; Pasqualetti, P.; Melgari, J.M.; Altamura, C.; Palazzo, P.; Di Giorgio, M.; Rossini, P.M. High frequency repetitive transcranial magnetic stimulation decreases cerebral vasomotor reactivity. Clin. Neurophysiol. 2009, 120, 1188–1194. [Google Scholar] [CrossRef]
- Fitzgerald, P.B.; Fountain, S.; Daskalakis, Z.J. A comprehensive review of the effects of rTMS on motor cortical excitability and inhibition. Clin. Neurophysiol. 2006, 117, 2584–2596. [Google Scholar] [CrossRef]
- Hinchman, C.A.; Fried, P.J.; Jannati, A.; Press, D.Z.; Pascual-Leone, A.; Stern, A.P. Corticomotor plasticity as a predictor of response to high frequency transcranial magnetic stimulation treatment for major depressive disorder. J. Affect. Disord. 2022, 303, 114–122. [Google Scholar] [CrossRef]
- Noda, Y.; Zomorrodi, R.; Vila-Rodriguez, F.; Downar, J.; Farzan, F.; Cash, R.F.H.; Rajji, T.K.; Daskalakis, Z.J.; Blumberger, D.M. Impaired neuroplasticity in the prefrontal cortex in depression indexed through paired associative stimulation. Depress. Anxiety 2018, 35, 448–456. [Google Scholar] [CrossRef]
- Player, M.J.; Taylor, J.L.; Weickert, C.S.; Alonzo, A.; Sachdev, P.; Martin, D.; Mitchell, P.B.; Loo, C.K. Neuroplasticity in Depressed Individuals Compared with Healthy Controls. Neuropsychopharmacology 2013, 38, 2101–2108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shajahan, P.M.; Glabus, M.F.; Gooding, P.A.; Shah, P.J.; Ebmeier, K.P. Reduced cortical excitability in depression. Impaired post-exercise motor facilitation with transcranial magnetic stimulation. Br. J. Psychiatry 1999, 174, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Fumagalli, F.; Molteni, R.; Roceri, M.; Bedogni, F.; Santero, R.; Fossati, C.; Gennarelli, M.; Racagni, G.; Riva, M.A. Effect of antipsychotic drugs on brain-derived neurotrophic factor expression under reduced N-methyl-D-aspartate receptor activity. J. Neurosci. Res. 2003, 72, 622–628. [Google Scholar] [CrossRef] [PubMed]
- Mosiołek, A.; Mosiołek, J.; Jakima, S.; Pięta, A.; Szulc, A. Effects of Antidepressant Treatment on Neurotrophic Factors (BDNF and IGF-1) in Patients with Major Depressive Disorder (MDD). J. Clin. Med. 2021, 10, 3377. [Google Scholar] [CrossRef]
- Mayberg, H.S. Frontal lobes dysfunction in secondary depression. In The Frontal Lobes and Neuropsychiatric Illness; American Psychiatric Publishing, Inc.: Arlington, VA, USA, 2001; pp. 167–186. ISBN 978-0-88048-800-6. [Google Scholar]
- Pizzagalli, D.A. Frontocingulate dysfunction in depression: Toward biomarkers of treatment response. Neuropsychopharmacology 2011, 36, 183–206. [Google Scholar] [CrossRef]
- Cappon, D.; den Boer, T.; Jordan, C.; Yu, W.; Metzger, E.; Pascual-Leone, A. Transcranial magnetic stimulation (TMS) for geriatric depression. Ageing Res. Rev. 2022, 74, 101531. [Google Scholar] [CrossRef]
- Lindenberger, U. Human cognitive aging: Corriger la fortune? Science 2014, 346, 572–578. [Google Scholar] [CrossRef]
- Fiske, A.; Wetherell, J.L.; Gatz, M. Depression in older adults. Annu. Rev. Clin. Psychol. 2009, 5, 363–389. [Google Scholar] [CrossRef]
- Maydych, V. The Interplay Between Stress, Inflammation, and Emotional Attention: Relevance for Depression. Front. Neurosci. 2019, 13, 384. [Google Scholar] [CrossRef] [Green Version]
- Alexopoulos, G.S.; Murphy, C.F.; Gunning-Dixon, F.M.; Latoussakis, V.; Kanellopoulos, D.; Klimstra, S.; Lim, K.O.; Hoptman, M.J. Microstructural White Matter Abnormalities and Remission of Geriatric Depression. Am. J. Psychiatry 2008, 165, 238–244. [Google Scholar] [CrossRef] [Green Version]
- Gunning-Dixon, F.M.; Brickman, A.M.; Cheng, J.C.; Alexopoulos, G.S. Aging of cerebral white matter: A review of MRI findings. Int. J. Geriatr. Psychiatry 2009, 24, 109–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bella, R.; Pennisi, G.; Cantone, M.; Palermo, F.; Pennisi, M.; Lanza, G.; Zappia, M.; Paolucci, S. Clinical presentation and outcome of geriatric depression in subcortical ischemic vascular disease. Gerontology 2010, 56, 298–302. [Google Scholar] [CrossRef] [PubMed]
- Blumberger, D.M. Can Repetitive Transcranial Magnetic Stimulation Enhance Cognitive Control in Late-Life Depression? Am. J. Geriatr. Psychiatry 2018, 26, 347–349. [Google Scholar] [CrossRef]
- Wagner, T.; Eden, U.; Fregni, F.; Valero-Cabre, A.; Ramos-Estebanez, C.; Pronio-Stelluto, V.; Grodzinsky, A.; Zahn, M.; Pascual-Leone, A. Transcranial magnetic stimulation and brain atrophy: A computer-based human brain model study. Exp. Brain Res. 2008, 186, 539–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabesan, P.; Lankappa, S.; Khalifa, N.; Krishnan, V.; Gandhi, R.; Palaniyappan, L. Transcranial magnetic stimulation for geriatric depression: Promises and pitfalls. World J. Psychiatry 2015, 5, 170–181. [Google Scholar] [CrossRef] [PubMed]
- Iriarte, I.G.; George, M.S. Transcranial Magnetic Stimulation (TMS) in the Elderly. Curr. Psychiatry Rep. 2018, 20, 6. [Google Scholar] [CrossRef] [PubMed]
- van Rooij, S.J.H.; Riva-Posse, P.; McDonald, W.M. The Efficacy and Safety of Neuromodulation Treatments in Late-Life Depression. Curr. Treat. Options Psychiatry 2020, 7, 337–348. [Google Scholar] [CrossRef]
- Manes, F.; Jorge, R.; Morcuende, M.; Yamada, T.; Paradiso, S.; Robinson, R.G. A controlled study of repetitive transcranial magnetic stimulation as a treatment of depression in the elderly. Int. Psychogeriatr. 2001, 13, 225–231. [Google Scholar] [CrossRef]
- Freitas, C.; Perez, J.; Knobel, M.; Tormos, J.M.; Oberman, L.; Eldaief, M.; Bashir, S.; Vernet, M.; Peña-Gómez, C.; Pascual-Leone, A. Changes in cortical plasticity across the lifespan. Front. Aging Neurosci. 2011, 3, 5. [Google Scholar] [CrossRef] [Green Version]
- Pascual-Leone, A.; Freitas, C.; Oberman, L.; Horvath, J.C.; Halko, M.; Eldaief, M.; Bashir, S.; Vernet, M.; Shafi, M.; Westover, B.; et al. Characterizing brain cortical plasticity and network dynamics across the age-span in health and disease with TMS-EEG and TMS-fMRI. Brain Topogr. 2011, 24, 302–315. [Google Scholar] [CrossRef] [Green Version]
- Clark-Raymond, A.; Meresh, E.; Hoppensteadt, D.; Fareed, J.; Sinacore, J.; Garlenski, B.; Halaris, A. Vascular endothelial growth factor: Potential predictor of treatment response in major depression. World J. Biol. Psychiatry 2017, 18, 575–585. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.W.; Madsen, J.R. VEGF Signaling in Neurological Disorders. Int. J. Mol. Sci. 2018, 19, 275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onoda, K.; Ishihara, M.; Yamaguchi, S. Decreased functional connectivity by aging is associated with cognitive decline. J. Cogn. Neurosci. 2012, 24, 2186–2198. [Google Scholar] [CrossRef] [PubMed]
- Coelho, A.; Fernandes, H.M.; Magalhães, R.; Moreira, P.S.; Marques, P.; Soares, J.M.; Amorim, L.; Portugal-Nunes, C.; Castanho, T.; Santos, N.C.; et al. Signatures of white-matter microstructure degradation during aging and its association with cognitive status. Sci. Rep. 2021, 11, 4517. [Google Scholar] [CrossRef]
- Honey, C.J.; Sporns, O.; Cammoun, L.; Gigandet, X.; Thiran, J.P.; Meuli, R.; Hagmann, P. Predicting human resting-state functional connectivity from structural connectivity. Proc. Natl. Acad. Sci. USA 2009, 106, 2035–2040. [Google Scholar] [CrossRef] [Green Version]
- Opie, G.M.; Vosnakis, E.; Ridding, M.C.; Ziemann, U.; Semmler, J.G. Priming theta burst stimulation enhances motor cortex plasticity in young but not old adults. Brain Stimul. 2017, 10, 298–304. [Google Scholar] [CrossRef] [Green Version]
- Galvez-Contreras, A.Y.; Campos-Ordonez, T.; Lopez-Virgen, V.; Gomez-Plascencia, J.; Ramos-Zuniga, R.; Gonzalez-Perez, O. Growth factors as clinical biomarkers of prognosis and diagnosis in psychiatric disorders. Cytokine Growth Factor Rev. 2016, 32, 85–96. [Google Scholar] [CrossRef]
- Xue, Y.; Liang, H.; Yang, R.; Deng, K.; Tang, M.; Zhang, M. The role of pro- and mature neurotrophins in the depression. Behav. Brain Res. 2021, 404, 113162. [Google Scholar] [CrossRef]
- Kim, H.K.; Blumberger, D.M.; Downar, J.; Daskalakis, Z.J. Systematic review of biological markers of therapeutic repetitive transcranial magnetic stimulation in neurological and psychiatric disorders. Clin. Neurophysiol. 2021, 132, 429–448. [Google Scholar] [CrossRef]
- Gedge, L.; Beaudoin, A.; Lazowski, L.; du Toit, R.; Jokic, R.; Milev, R. Effects of electroconvulsive therapy and repetitive transcranial magnetic stimulation on serum brain-derived neurotrophic factor levels in patients with depression. Front. Psychiatry 2012, 3, 12. [Google Scholar] [CrossRef] [Green Version]
- Zhao, X.; Li, Y.; Tian, Q.; Zhu, B.; Zhao, Z. Repetitive transcranial magnetic stimulation increases serum brain-derived neurotrophic factor and decreases interleukin-1β and tumor necrosis factor-α in elderly patients with refractory depression. J. Int. Med. Res. 2019, 47, 1848–1855. [Google Scholar] [CrossRef] [PubMed]
- Valiuliene, G.; Valiulis, V.; Dapsys, K.; Vitkeviciene, A.; Gerulskis, G.; Navakauskiene, R.; Germanavicius, A. Brain stimulation effects on serum BDNF, VEGF, and TNFα in treatment-resistant psychiatric disorders. Eur. J. Neurosci. 2021, 53, 3791–3802. [Google Scholar] [CrossRef]
- Cheng, C.-M.; Hong, C.-J.; Lin, H.-C.; Chu, P.-J.; Chen, M.-H.; Tu, P.-C.; Bai, Y.-M.; Chang, W.-H.; Juan, C.-H.; Lin, W.-C.; et al. Predictive roles of brain-derived neurotrophic factor Val66Met polymorphism on antidepressant efficacy of different forms of prefrontal brain stimulation monotherapy: A randomized, double-blind, sham-controlled study. J. Affect. Disord. 2022, 297, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, A.M.; Hindley, L.E.; Kang, J.W.D.; Tirrell, E.; Tyrka, A.R.; Ayala, A.; Carpenter, L.L. Peripheral vascular endothelial growth factor changes after transcranial magnetic stimulation in treatment-resistant depression. Neuroreport 2020, 31, 1121–1127. [Google Scholar] [CrossRef]
- Elemery, M.; Kiss, S.; Dome, P.; Pogany, L.; Faludi, G.; Lazary, J. Change of Circulating Vascular Endothelial Growth Factor Level and Reduction of Anhedonia Are Associated in Patients With Major Depressive Disorder Treated With Repetitive Transcranial Magnetic Stimulation. Front. Psychiatry 2022, 13, 806731. [Google Scholar] [CrossRef] [PubMed]
- Mondal, A.C.; Fatima, M. Direct and indirect evidences of BDNF and NGF as key modulators in depression: Role of antidepressants treatment. Int. J. Neurosci. 2019, 129, 283–296. [Google Scholar] [CrossRef]
- Bot, M.; Milaneschi, Y.; Penninx, B.W.J.H.; Drent, M.L. Plasma insulin-like growth factor I levels are higher in depressive and anxiety disorders, but lower in antidepressant medication users. Psychoneuroendocrinology 2016, 68, 148–155. [Google Scholar] [CrossRef]
- Ward, R.; Abdul, Y.; Ergul, A. Endothelin-1 inhibition improves the mBDNF/proBDNF ratio in endothelial cells and HT22 neurons under high glucose/palmitate growth conditions. Physiol. Res. 2018, 67, S237–S246. [Google Scholar] [CrossRef]
- Khedr, E.M.; Elserogy, Y.; Fawzy, M.; Abdelrahman, A.A.; Galal, A.M.; Noaman, M.M. Effect of psychotropic drugs on cortical excitability of patients with major depressive disorders: A transcranial magnetic stimulation study. Psychiatry Res. 2020, 291, 113287. [Google Scholar] [CrossRef]
- Minzenberg, M.J.; Leuchter, A.F. The effect of psychotropic drugs on cortical excitability and plasticity measured with transcranial magnetic stimulation: Implications for psychiatric treatment. J. Affect. Disord. 2019, 253, 126–140. [Google Scholar] [CrossRef]
- Di Lazzaro, V.; Oliviero, A.; Meglio, M.; Cioni, B.; Tamburrini, G.; Tonali, P.; Rothwell, J.C. Direct demonstration of the effect of lorazepam on the excitability of the human motor cortex. Clin. Neurophysiol. 2000, 111, 794–799. [Google Scholar] [CrossRef] [PubMed]
- Kimiskidis, V.K.; Papagiannopoulos, S.; Kazis, D.A.; Sotirakoglou, K.; Vasiliadis, G.; Zara, F.; Kazis, A.; Mills, K.R. Lorazepam-induced effects on silent period and corticomotor excitability. Exp. Brain Res. 2006, 173, 603–611. [Google Scholar] [CrossRef] [PubMed]
- Hunter, A.M.; Minzenberg, M.J.; Cook, I.A.; Krantz, D.E.; Levitt, J.G.; Rotstein, N.M.; Chawla, S.A.; Leuchter, A.F. Concomitant medication use and clinical outcome of repetitive Transcranial Magnetic Stimulation (rTMS) treatment of Major Depressive Disorder. Brain Behav. 2019, 9, e01275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deppe, M.; Abdelnaim, M.; Hebel, T.; Kreuzer, P.M.; Poeppl, T.B.; Langguth, B.; Schecklmann, M. Concomitant lorazepam use and antidepressive efficacy of repetitive transcranial magnetic stimulation in a naturalistic setting. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 61–67. [Google Scholar] [CrossRef]
- Minelli, A.; Bortolomasi, M.; Scassellati, C.; Salvoro, B.; Avesani, M.; Manganotti, P. Effects of intravenous antidepressant drugs on the excitability of human motor cortex: A study with paired magnetic stimulation on depressed patients. Brain Stimul. 2010, 3, 15–21. [Google Scholar] [CrossRef]
- Robol, E.; Fiaschi, A.; Manganotti, P. Effects of citalopram on the excitability of the human motor cortex: A paired magnetic stimulation study. J. Neurol. Sci. 2004, 221, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Langguth, B.; Eichhammer, P.; Spranz, C.; Landgrebe, M.; Frick, U.; Sand, P.; Hajak, G. Modulation of human motor cortex excitability by quetiapine. Psychopharmacology 2008, 196, 623–629. [Google Scholar] [CrossRef]
- Hasan, A.; Falkai, P.; Wobrock, T. Transcranial brain stimulation in schizophrenia: Targeting cortical excitability, connectivity and plasticity. Curr. Med. Chem. 2013, 20, 405–413. [Google Scholar]
- Frank, E.; Landgrebe, M.; Poeppl, T.B.; Schecklmann, M.; Kreuzer, P.M.; Prasser, J.; Rupprecht, R.; Eichhammer, P.; Hajak, G.; Langguth, B. Antipsychotic treatment with quetiapine increases the cortical silent period. Schizophr. Res. 2014, 156, 128–132. [Google Scholar] [CrossRef]
- Hebel, T.; Abdelnaim, M.; Deppe, M.; Langguth, B.; Schecklmann, M. Attenuation of antidepressive effects of transcranial magnetic stimulation in patients whose medication includes drugs for psychosis. J. Psychopharmacol. 2020, 34, 1119–1124. [Google Scholar] [CrossRef]
- Schulze, L.; Remington, G.; Giacobbe, P.; Kennedy, S.H.; Blumberger, D.M.; Daskalakis, Z.J.; Downar, J. Effect of antipsychotic pharmacotherapy on clinical outcomes of intermittent theta-burst stimulation for refractory depression. J. Psychopharmacol. 2017, 31, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Costa, M.V.; Diniz, M.F.; Nascimento, K.K.; Pereira, K.S.; Dias, N.S.; Malloy-Diniz, L.F.; Diniz, B.S. Accuracy of three depression screening scales to diagnose major depressive episodes in older adults without neurocognitive disorders. Braz. J. Psychiatry 2016, 38, 154–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 |
|---|---|---|---|---|---|---|
| Sex | Female | Male | Male | Male | Male | Male |
| Age, years | 62 | 81 | 82 | 60 | 72 | 64 |
| Education, years | 18 | 5 | 3 | 13 | 8 | 13 |
| Height, cm | 160 | 165 | 170 | 170 | 168 | 177 |
| Weight, Kg | 57 | 62 | 70 | 63 | 72 | 72 |
| Family history of depression | No | Yes | No | No | No | Yes |
| Current episode duration, months | 9 | 6 | 10 | 7 | 5 | 24 |
| Vascular risk factors | None | Dyslipidemia Diabetes | Hypertension Dyslipidemia Mild bilateral carotid stenosis | Tobacco smoking | Left carotid stenosis | Hypertension |
| Brain MRI | Normal | Mild SCVD | Moderate SCVD | Mild SCVD | Moderate SCVD | Mild SCVD |
| Drug daily dosage(s) | cital 40 mg olanz 5 mg loraz 2.5 mg venla 75 mg | vorti 5 mg | vorti 5 mg queti 25 mg | amitr 50 mg queti 350 mg loraz 5 mg | aripi 5 mg cital 20 mg | diaze 2.5 mg queti 50 mg cital 40 mg amitr 60 mg triaz 0.5 mg |
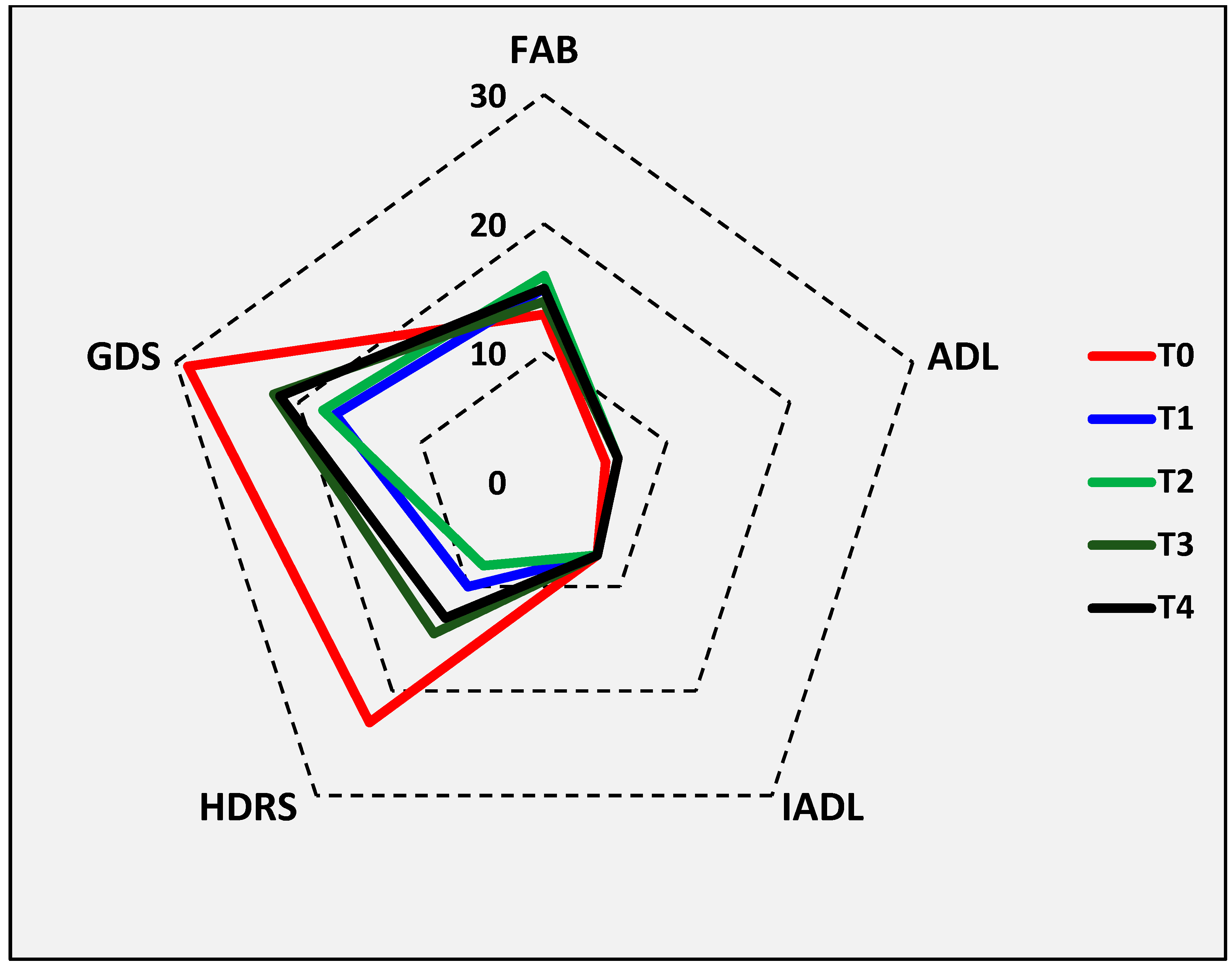
| Variable | Median (IQR) T0 | Median (IQR) T1 | Wilcoxon Z | p Value |
|---|---|---|---|---|
| MMSE | 27.7 (24.0–29.0) | 28.2 (17.5–30.0) | 0.405 | 0.686 |
| FAB | 12.0 (10.0–17.0) | 15.0 (10.0–18.0) | 1.483 | 0.138 |
| Stroop T | 27.6 (22.4–57.7) | 32.3 (28.7–40.0) | 0.314 | 0.753 |
| Stroop E | 2.0 (1.0–3.0) | 1.5 (0.0–3.0) | 0.135 | 0.893 |
| Stroop score | 15.7 (7.3–42.8) | 22.0 (9.1–26.1) | 0.314 | 0.753 |
| ADL | 5.5 (5.0–6.0) | 6.0 (6.0–6.0) | 1.342 | 0.180 |
| IADL | 5.0 (4.0–7.0) | 7.0 (5.0–7.0) | 1.826 | 0.068 |
| HDRS | 23.0 (19.0–24.0) | 10.0 (8.0–16.0) | 2.201 | 0.028 |
| GDS | 22.5 (22.0–26.0) | 17.0 (16.0–27.0) | 1.363 | 0.173 |
| AES | 43.0 (40.0–49.0) | 43.0 (39.0–45.0) | 0.405 | 0.686 |
| Variable | Median (IQR) T0 | Median (IQR) T1 | Wilcoxon Z | p Value |
|---|---|---|---|---|
| Left rMT, % | 40.5 (39.0–42.0) | 40.0 (38.0–41.0) | 1.348 | 0.178 |
| Left MEP latency, ms | 22.0 (20.0–22.5) | 21.7 (20.8–22.0) | 0.405 | 0.686 |
| Left MEP amplitude, mV | 4.1 (3.7–5.3) | 4.7 (3.9–7.0) | 1.153 | 0.249 |
| Left PMS latency, ms | 15.5 (15.1–16.4) | 16.0 (14.1–16.2) | 0.524 | 0.600 |
| Left CMCT, ms | 6.4 (6.1–6.9) | 6.2 (5.4–7.2) | 0.105 | 0.917 |
| Left CMAP latency, ms | 3.2 (2.7–3.9) | 3.1 (2.8–3.4) | 0.730 | 0.465 |
| Left CMAP amplitude, mV | 17.4 (10.3–22.2) | 18.0 (17.2–20.6) | 0.734 | 0.463 |
| Left F wave latency, ms | 30.7 (29.1–31.8) | 31.0 (29.4–31.8) | 0.405 | 0.686 |
| Left F wave amplitude, mV | 0.2 (0.1–0.2) | 0.2 (0.1–0.2) | 0.943 | 0.345 |
| Left amplitude ratio | 0.3 (0.2–0.4) | 0.3 (0.2–0.4) | 0.314 | 0.753 |
| Left CMCT-F, ms | 5.3 (5.0–5.5) | 5.6 (4.4–6.1) | 0.629 | 0.529 |
| Left cSP, ms | 70.6 (59.8–94.0) | 67.2 (48.8–78.0) | 0.734 | 0.463 |
| Left iSP, ms | 17.8 (13.2–19.8) | 16.5 (13.7–17.5) | 0.524 | 0.600 |
| Right rMT, % | 39.5 (35.0–50.0) | 39.0 (36.0–50.0) | 0.000 | 1.000 |
| Right MEP latency, ms | 21.6 (20.7–21.9) | 21.4 (20.1–22.2) | 0.314 | 0.753 |
| Right MEP amplitude, mV | 3.2 (2.5–4.1) | 4.1 (3.4–4.2) | 1.992 | 0.046 |
| Right PMS latency, ms | 15.6 (14.5–16.0) | 15.8 (14.9–16.1) | 0.270 | 0.787 |
| Right CMCT, ms | 6.4 (5.5–6.6) | 6.1 (5.2–6.3) | 0.943 | 0.345 |
| Right CMAP latency, ms | 3.3 (2.8–3.7) | 3.1 (2.7–3.6) | 2.023 | 0.053 |
| Right CMAP amplitude, mV | 15.7 (14.2–16.8) | 17.5 (12.5–21.0) | 0.524 | 0.600 |
| Right F wave latency, ms | 29.7 (28.5–31) | 30.1 (29.5–30.8) | 0.524 | 0.600 |
| Right F wave amplitude, mV | 0.1 (0.1–0.2) | 0.1 (0.1–0.2) | 0.314 | 0.753 |
| Right amplitude ratio | 0.2 (0.2–0.3) | 0.2 (0.2–0.4) | 0.734 | 0.463 |
| Right CMCT-F, ms | 5.5 (4.9–5.8) | 5.2 (5.0–6.1) | 0.405 | 0.686 |
| Right cSP, ms | 77.8 (65.1–109.5) | 72.1 (59.6–85.8) | 0.943 | 0.345 |
| Right iSP, ms | 19.4 (15.7–20.0) | 18.0 (17.2–28.9) | 1.153 | 0.249 |
| Variable | Median (IQR) T0 | Median (IQR) T1 | Wilcoxon Z | p Value |
|---|---|---|---|---|
| Left PSV, cm/s | 62.5 (48.0–65.0) | 75.5 (71.0–85.0) | 1.153 | 0.249 |
| Left EDV, cm/s | 25.5 (18.0–28.0) | 29.5 (20.0–42.0) | 0.314 | 0.753 |
| Left MV, cm/s | 38.0 (35.0–42.0) | 45.5 (39.0–61.0) | 1.153 | 0.249 |
| Left PI | 0.9 (0.8–1.0) | 1.0 (0.7–1.2) | 1.363 | 0.173 |
| Left RI | 0.6 (0.6–0.6) | 0.6 (0.5–0.7) | 1.153 | 0.249 |
| Right PSV, cm/s | 58.5 (52.0–68.0) | 71.0 (60.0–85.0) | 0.674 | 0.500 |
| Right EDV, cm/s | 26.0 (20.0–31.0) | 28.5 (24.0–42.0) | 0.943 | 0.345 |
| Right MV, cm/s | 38.0 (32.0–44.0) | 42.0 (36.0–61.0) | 0.629 | 0.529 |
| Right PI | 0.9 (0.8–1.0) | 0.9 (0.7–1.0) | 1.214 | 0.225 |
| Right RI | 0.6 (0.5–0.6) | 0.6 (0.5–0.6) | 0.135 | 0.893 |
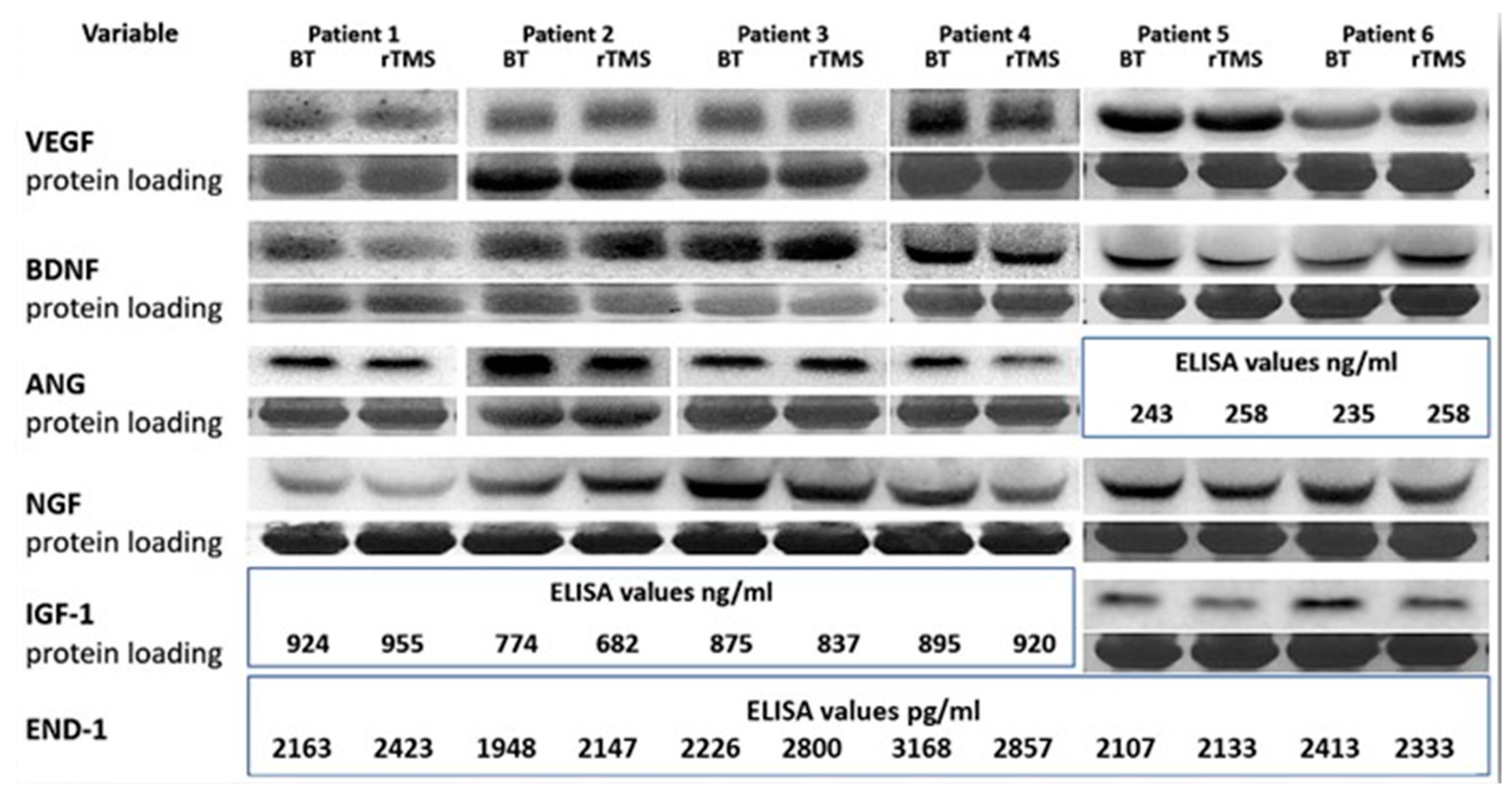
| Variable | Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 |
|---|---|---|---|---|---|---|
| VEGF | −13% | 8% | −17% | −8% | −6% | 42% |
| BDNF | −30% | 2% | 35% | −12% | −17% | 31% |
| ANG | −10% | −20% | 20% | −10% | 5% | 8% |
| NGF | −12% | −10% | −23% | −30% | −12% | −17% |
| IGF-1 | 4% | −12% | −5% | 3% | −24% | −16% |
| END-1 | 12% | 10% | 25% | −20% | 0% | 0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nicoletti, V.G.; Fisicaro, F.; Aguglia, E.; Bella, R.; Calcagno, D.; Cantone, M.; Concerto, C.; Ferri, R.; Mineo, L.; Pennisi, G.; et al. Challenging the Pleiotropic Effects of Repetitive Transcranial Magnetic Stimulation in Geriatric Depression: A Multimodal Case Series Study. Biomedicines 2023, 11, 958. https://doi.org/10.3390/biomedicines11030958
Nicoletti VG, Fisicaro F, Aguglia E, Bella R, Calcagno D, Cantone M, Concerto C, Ferri R, Mineo L, Pennisi G, et al. Challenging the Pleiotropic Effects of Repetitive Transcranial Magnetic Stimulation in Geriatric Depression: A Multimodal Case Series Study. Biomedicines. 2023; 11(3):958. https://doi.org/10.3390/biomedicines11030958
Chicago/Turabian StyleNicoletti, Vincenzo G., Francesco Fisicaro, Eugenio Aguglia, Rita Bella, Damiano Calcagno, Mariagiovanna Cantone, Carmen Concerto, Raffaele Ferri, Ludovico Mineo, Giovanni Pennisi, and et al. 2023. "Challenging the Pleiotropic Effects of Repetitive Transcranial Magnetic Stimulation in Geriatric Depression: A Multimodal Case Series Study" Biomedicines 11, no. 3: 958. https://doi.org/10.3390/biomedicines11030958