

Developmental Pharmacokinetics of Antibiotics Used in Neonatal ICU: Focus on Preterm Infants
Abstract
:1. Introduction
2. General Considerations on Neonate’s Pharmacokinetics
2.1. Absorption and Bioavailability
2.1.1. Absorption of Oral Penicillins
2.1.2. Absorption of Oral Cephalosporines
2.1.3. Absorption of Oral Carbapenems
2.1.4. Absorption of Oral Macrolides
2.1.5. Absorption of Oral Oxazolidinones
2.1.6. Absorption of Oral Fluoroquinolones
2.1.7. Absorption of Other Oral Antibacterial Agents
2.1.8. Effect of Food on Antibiotics Absorption
2.1.9. Absorption in Non-Oral Routes of Administration
2.2. Distribution
2.3. Metabolism
- First pattern (Class 1)—DME high in fetal life and low or absent after birth;
- Second pattern (Class 2)—DME stable throughout development;
- Third pattern (Class 3)—DME low in fetal life to increasing and high after birth.
2.4. Excretion
- ACEi—angiotensin-converting enzyme inhibitors
- ANP—atrial natriuretic peptide
- AT I, AT II—angiotensin I and II
- NO—nitric oxide
- PGI2, PGE2—prostaglandins I2 and E2.
- -
- Premature and low birth weight neonates;
- -
- Neonates with congenital heart disease and cardiac surgery;
- -
- Neonates with hypoxic ischemic encephalopathy;
- -
- Neonates with necrotizing enterocolitis;
- -
- Neonates on extracorporeal life support;
- -
- Neonates using nephrotoxic drugs.
3. Antibiotic Dosing Regimens in Neonates
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Birrie, E.; Sisay, E.; Tibebu, N.S.; Tefera, B.D.; Zeleke, M.; Tefera, Z. Neonatal Sepsis and Associated Factors among Newborns in Woldia and Dessie Comprehensive Specialized Hospitals, North-East Ethiopia, 2021. Infect. Drug Resist. 2022, 15, 4169–4179. [Google Scholar] [CrossRef]
- Roble, A.K.; Ayehubizu, L.M.; Olad, H.M. Neonatal Sepsis and Associated Factors among Neonates Admitted to Neonatal Intensive Care Unit in General Hospitals, Eastern Ethiopia 2020. Clin. Med. Insights Pediatr. 2022, 16, 11795565221098346. [Google Scholar] [CrossRef] [PubMed]
- Van Den Anker, J.; Allegaert, K. Rational Use of Antibiotics in Neonates: Still in Search of Tailored Tools. Healthcare 2019, 7, 28. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, E.M.; Hornik, C.P.; Clark, R.H.; Laughon, M.M.; Benjamin, D.K., Jr.; Smith, P.B. Best Pharmaceuticals for Children Act-Pediatric Trials Network. Medication Use in the Neonatal Intensive Care Unit. Am. J. Perinatol. 2013, 31, 811–822. [Google Scholar] [CrossRef] [Green Version]
- Prusakov, P.; Goff, D.A.; Wozniak, P.S.; Cassim, A.; Scipion, C.E.; Urzúa, S.; Ronchi, A.; Zeng, L.; Ladipo-Ajayi, O.; Aviles-Otero, N.; et al. A global point prevalence survey of antimicrobial use in neonatal intensive care units: The no-more-antibiotics and resistance (NO-MAS-R) study. EClinicalMedicine 2021, 32, 100727. [Google Scholar] [CrossRef]
- Giannoni, E.; Dimopoulou, V.; Klingenberg, C.; Navér, L.; Nordberg, V.; Berardi, A.; el Helou, S.; Fusch, G.; Bliss, J.M.; Lehnick, D.; et al. Analysis of Antibiotic Exposure and Early-Onset Neonatal Sepsis in Europe, North America, and Australia. JAMA Netw. Open 2022, 5, e2243691. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, C.; Reichert, F.; Cassini, A.; Horner, R.; Harder, T.; Markwart, R.; Tröndle, M.; Savova, Y.; Kissoon, N.; Schlattmann, P.; et al. Global incidence and mortality of neonatal sepsis: A systematic review and meta-analysis. Arch. Dis. Child. 2021, 106, 745–752. [Google Scholar] [CrossRef] [PubMed]
- Rudd, K.E.; Johnson, S.C.; Agesa, K.M.; Shackelford, K.A.; Tsoi, D.; Kievlan, D.R.; Colombara, D.V.; Ikuta, K.S.; Kissoon, N.; Finfer, S.; et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: Analysis for the Global Burden of Disease Study. Lancet 2020, 395, 200–211. [Google Scholar] [CrossRef] [Green Version]
- Yu, Y.-Q.; He, X.-R.; Wan, L.-J.; Yang, Y.-H.; Chen, P.-Y. Etiology, antimicrobial resistance, and risk factors of neonatal sepsis in China: A systematic review and meta-analysis from data of 30 years. J. Matern. Fetal Neonatal Med. 2021, 35, 7541–7550. [Google Scholar] [CrossRef]
- Zelellw, D.A.; Dessie, G.; Mengesha, E.W.; Shiferaw, M.B.; Merhaba, M.M.; Emishaw, S. A Systemic Review and Meta-analysis of the Leading Pathogens Causing Neonatal Sepsis in Developing Countries. BioMed Res. Int. 2021, 2021, 6626983. [Google Scholar] [CrossRef]
- Sands, K.; Carvalho, M.J.; Portal, E.; Thomson, K.; Dyer, C.; Akpulu, C.; Andrews, R.; Ferreira, A.; Gillespie, D.; Hender, T.; et al. Characterization of antimicrobial-resistant Gram-negative bacteria that cause neonatal sepsis in seven low- and middle-income countries. Nat. Microbiol. 2021, 6, 512–523. [Google Scholar] [CrossRef] [PubMed]
- Thomson, K.M.; Dyer, C.; Liu, F.; Sands, K.; Portal, E.; Carvalho, M.J.; Barrell, M.; Boostrom, I.; Dunachie, S.; Farzana, R.; et al. Effects of antibiotic resistance, drug target attainment, bacterial pathogenicity and virulence, and antibiotic access and affordability on outcomes in neonatal sepsis: An international microbiology and drug evaluation prospective substudy (BARNARDS). Lancet Infect. Dis. 2021, 21, 1677–1688. [Google Scholar] [CrossRef]
- Solomon, S.; Akeju, O.; Odumade, O.A.; Ambachew, R.; Gebreyohannes, Z.; Van Wickle, K.; Abayneh, M.; Metaferia, G.; Carvalho, M.J.; Thomson, K.; et al. Prevalence and risk factors for antimicrobial resistance among newborns with gram-negative sepsis. PLoS ONE 2021, 16, e0255410. [Google Scholar] [CrossRef] [PubMed]
- Ji, H.; Yu, Y.; Huang, L.; Kou, Y.; Liu, X.; Li, S.; Zhang, Y.; Li, Z.; Sun, X.; Wang, J.; et al. Pathogen Distribution and Antimicrobial Resistance of Early Onset Sepsis in Very Premature Infants: A Real-World Study. Infect. Dis. Ther. 2022, 11, 1935–1947. [Google Scholar] [CrossRef]
- Fleiss, N.; Schwabenbauer, K.; Randis, T.M.; Polin, R.A. What’s new in the management of neonatal early-onset sepsis? Arch. Dis. Child. Fetal Neonatal Ed. 2023, 108, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Paul, S.P.; Khattak, H.; Kini, P.K.; Heaton, P.A.; Goel, N. NICE guideline review: Neonatal infection: Antibiotics for prevention and treatment (NG195). Arch. Dis. Child. Educ. Pract. Ed. 2022, 107, 292–297. [Google Scholar] [CrossRef]
- Amer, Y.S.; Shaiba, L.A.; Hadid, A.; Anabrees, J.; Almehery, A.; Aassiri, M.; Alnemri, A.; Al Darwish, A.R.; Baqawi, B.; Aboshaiqah, A.; et al. Quality assessment of clinical practice guidelines for neonatal sepsis using the Appraisal of Guidelines for Research and Evaluation (AGREE) II Instrument: A systematic review of neonatal guidelines. Front. Pediatr. 2022, 10, 891572. [Google Scholar] [CrossRef] [PubMed]
- Hsia, Y.; Lee, B.R.; Versporten, A.; Yang, Y.; Bielicki, J.; Jackson, C.; Newland, J.; Goossens, H.; Magrini, N.; Sharland, M.; et al. Use of the WHO Access, Watch, and Reserve classification to define patterns of hospital antibiotic use (AWaRe): An analysis of paediatric survey data from 56 countries. Lancet Glob. Health 2019, 7, e861–e871. [Google Scholar] [CrossRef] [Green Version]
- Williams, P.; Qazi, S.; Agarwal, R.; Velaphi, S.; Bielicki, J.; Nambiar, S.; Giaquinto, C.; Bradley, J.; Noel, G.; Ellis, S.; et al. Antibiotics needed to treat multidrug-resistant infections in neonates. Bull. World Health Organ. 2022, 100, 797–807. [Google Scholar] [CrossRef]
- Darlow, C.A.; da Costa, R.M.A.; Ellis, S.; Franceschi, F.; Sharland, M.; Piddock, L.; Das, S.; Hope, W. Potential Antibiotics for the Treatment of Neonatal Sepsis Caused by Multidrug-Resistant Bacteria. Pediatr. Drugs 2021, 23, 465–484. [Google Scholar] [CrossRef]
- World Health Organization. The 2019 WHO AWaRe Classification of Antibiotics for Evaluation and Monitoring of Use. World Health Organization. 2019. Available online: https://apps.who.int/iris/handle/10665/327957 (accessed on 10 January 2023).
- Henry, C.J.; Semova, G.; Barnes, E.; Cotter, I.; Devers, T.; Rafaee, A.; Slavescu, A.; Cathain, N.O.; McCollum, D.; Roche, E.; et al. Neonatal sepsis: A systematic review of core outcomes from randomised clinical trials. Pediatr. Res. 2022, 91, 735–742. [Google Scholar] [CrossRef]
- Alghamdi, A.A.; Keers, R.N.; Sutherland, A.; Ashcroft, D.M. Prevalence and Nature of Medication Errors and Preventable Adverse Drug Events in Paediatric and Neonatal Intensive Care Settings: A Systematic Review. Drug Saf. 2019, 42, 1423–1436. [Google Scholar] [CrossRef] [Green Version]
- Basil, J.H.; Premakumar, C.M.; Ali, A.M.; Tahir, N.A.M.; Shah, N.M. Prevalence, Causes and Severity of Medication Administration Errors in the Neonatal Intensive Care Unit: A Systematic Review and Meta-Analysis. Drug Saf. 2022, 45, 1457–1476. [Google Scholar] [CrossRef] [PubMed]
- Shawahna, R.; Jaber, M.; Said, R.; Mohammad, K.; Aker, Y. Medication errors in neonatal intensive care units: A multicenter qualitative study in the Palestinian practice. BMC Pediatr. 2022, 22, 317. [Google Scholar] [CrossRef] [PubMed]
- Pawluk, S.; Jaam, M.; Hazi, F.; Al Hail, M.S.; El Kassem, W.; Khalifa, H.; Thomas, B.; Rouf, P.A. A description of medication errors reported by pharmacists in a neonatal intensive care unit. Int. J. Clin. Pharm. 2017, 39, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Van Donge, T.; Bielicki, J.A.; Anker, J.V.D.; Pfister, M. Key Components for Antibiotic Dose Optimization of Sepsis in Neonates and Infants. Front. Pediatr. 2018, 6, 325. [Google Scholar] [CrossRef] [Green Version]
- Gianvecchio, C.; Lozano, N.A.; Henderson, C.; Kalhori, P.; Bullivant, A.; Valencia, A.; Su, L.; Bello, G.; Wong, M.; Cook, E.; et al. Variation in Mutant Prevention Concentrations. Front. Microbiol. 2019, 10, 42. [Google Scholar] [CrossRef] [Green Version]
- Sumi, C.D.; Heffernan, A.J.; Lipman, J.; Roberts, J.A.; Sime, F.B. What Antibiotic Exposures Are Required to Suppress the Emergence of Resistance for Gram-Negative Bacteria? A Systematic Review. Clin. Pharmacokinet. 2019, 58, 1407–1443. [Google Scholar] [CrossRef]
- Keij, F.M.; Kornelisse, R.F.; Hartwig, N.G.; Reiss, I.K.M.; Allegaert, K.; A Tramper-Stranders, G. Oral antibiotics for neonatal infections: A systematic review and meta-analysis. J. Antimicrob. Chemother. 2019, 74, 3150–3161. [Google Scholar] [CrossRef] [Green Version]
- Neal-Kluever, A.; Fisher, J.; Grylack, L.; Kakiuchi-Kiyota, S.; Halpern, W. Physiology of the Neonatal Gastrointestinal System Relevant to the Disposition of Orally Administered Medications. Drug Metab. Dispos. 2019, 47, 296–313. [Google Scholar] [CrossRef] [Green Version]
- Indrio, F.; Neu, J.; Pettoello-Mantovani, M.; Marchese, F.; Martini, S.; Salatto, A.; Aceti, A. Development of the Gastrointestinal Tract in Newborns as a Challenge for an Appropriate Nutrition: A Narrative Review. Nutrients 2022, 14, 1405. [Google Scholar] [CrossRef] [PubMed]
- Simeoli, R.; Cairoli, S.; Decembrino, N.; Campi, F.; Vici, C.D.; Corona, A.; Goffredo, B.M. Use of Antibiotics in Preterm Newborns. Antibiotics 2022, 11, 1142. [Google Scholar] [CrossRef] [PubMed]
- Shawahna, R. Pediatric Biopharmaceutical Classification System: Using Age-Appropriate Initial Gastric Volume. AAPS J. 2016, 18, 728–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gan, J.; Bornhorst, G.M.; Henrick, B.; German, J.B. Protein Digestion of Baby Foods: Study Approaches and Implications for Infant Health. Mol. Nutr. Food Res. 2018, 62, 1700231. [Google Scholar] [CrossRef] [PubMed]
- Bonner, J.J.; Vajjah, P.; Abduljalil, K.; Jamei, M.; Rostami-Hodjegan, A.; Tucker, G.T.; Johnson, T.N. Does age affect gastric emptying time? A model-based meta-analysis of data from premature neonates through to adults. Biopharm. Drug Dispos. 2015, 36, 245–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourlieu, C.; Ménard, O.; Bouzerzour, K.; Mandalari, G.; Macierzanka, A.; Mackie, A.R.; Dupont, D. Specificity of Infant Digestive Conditions: Some Clues for Developing Relevant In Vitro Models. Crit. Rev. Food Sci. Nutr. 2014, 54, 1427–1457. [Google Scholar] [CrossRef]
- Bartelink, I.H.; Rademaker, C.M.A.; Schobben, A.F.A.M.; van den Anker, J.N. Guidelines on Paediatric Dosing on the Basis of Developmental Physiology and Pharmacokinetic Considerations. Clin. Pharmacokinet. 2006, 45, 1077–1097. [Google Scholar] [CrossRef]
- Henderickx, J.G.E.; Zwittink, R.D.; Renes, I.B.; van Lingen, R.A.; van Zoeren-Grobben, D.; Jebbink, L.J.G.; Boeren, S.; van Elburg, R.M.; Knol, J.; Belzer, C. Maturation of the preterm gastrointestinal tract can be defined by host and microbial markers for digestion and barrier defense. Sci. Rep. 2021, 11, 12808. [Google Scholar] [CrossRef]
- Palla, M.R.; Harohalli, S.; Crawford, T.N.; Desai, N. Progression of Gastric Acid Production in Preterm Neonates: Utilization of In-vitro Method. Front. Pediatr. 2018, 6, 211. [Google Scholar] [CrossRef] [Green Version]
- Kelly, E.; Newell, S.; Brownlee, K.; Primrose, J.; Dear, P. Gastric acid secretion in preterm infants. Early Hum. Dev. 1993, 35, 215–220. [Google Scholar] [CrossRef]
- Omari, T.I.; Davidson, G.F. Multipoint measurement of intragastric pH in healthy preterm infants. Arch. Dis. Child. Fetal Neonatal Ed. 2003, 88, F517–F520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Groen, B.D.; van de Steeg, E.; Mooij, M.G.; van Lipzig, M.M.; de Koning, B.A.; Verdijk, R.M.; Wortelboer, H.M.; Gaedigk, R.; Bi, C.; Leeder, J.S.; et al. Proteomics of human liver membrane transporters: A focus on fetuses and newborn infants. Eur. J. Pharm. Sci. 2018, 124, 217–227. [Google Scholar] [CrossRef] [PubMed]
- Karpen, H.; Karpen, S.J. 95-Bile Acid Metabolism During Development. In Fetal and Neonatal Physiology, 5th ed.; Polin, R.A., Abman, S.H., Rowitch, D.H., Benitz, W.E., Fox, W.W., Eds.; Elsevier: Amsterdam, The Netherlands, 2017; pp. 913–929. ISBN 9780323352147. [Google Scholar] [CrossRef]
- Konieczna, A.; Erdösová, B.; Lichnovská, R.; Jandl, M.; Čížková, K.; Ehrmann, J. Differential expression of ABC transporters (MDR1, MRP1, BCRP) in developing human embryos. J. Mol. Histol. 2011, 42, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Prasad, B.; Gaedigk, A.; Vrana, M.; Gaedigk, R.; Leeder, J.; Salphati, L.; Chu, X.; Xiao, G.; Hop, C.; Evers, R.; et al. Ontogeny of Hepatic Drug Transporters as Quantified by LC-MS/MS Proteomics. Clin. Pharmacol. Ther. 2016, 100, 362–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qian, X.; Cheng, Y.-H.; Mruk, D.D.; Cheng, C.Y. Breast cancer resistance protein (Bcrp) and the testis—An unexpected turn of events. Asian J. Androl. 2013, 15, 455–460. [Google Scholar] [CrossRef] [Green Version]
- BCRP/ABCG2 Substrates. Available online: https://go.drugbank.com/categories/DBCAT002663 (accessed on 20 January 2023).
- Klaassen, C.D.; Aleksunes, L.M. Xenobiotic, Bile Acid, and Cholesterol Transporters: Function and Regulation. Pharmacol. Rev. 2010, 62, 1–96. [Google Scholar] [CrossRef] [Green Version]
- Sugie, M.; Asakura, E.; Zhao, Y.L.; Torita, S.; Nadai, M.; Baba, K.; Kitaichi, K.; Takagi, K.; Takagi, K.; Hasegawa, T. Possible Involvement of the Drug Transporters P Glycoprotein and Multidrug Resistance-Associated Protein Mrp2 in Disposition of Azithromycin. Antimicrob. Agents Chemother. 2004, 48, 809–814. [Google Scholar] [CrossRef] [Green Version]
- Sakaeda, T.; Nakamura, T.; Okumura, K. MDR1 Genotype-Related Pharmacokinetics and Pharmacodynamics. Biol. Pharm. Bull. 2002, 25, 1391–1400. [Google Scholar] [CrossRef] [Green Version]
- Putnam, W.S.; Woo, J.M.; Huang, Y.; Benet, L.Z. Effect of theMDR1C3435T Variant and P-Glycoprotein Induction on Dicloxacillin Pharmacokinetics. J. Clin. Pharmacol. 2005, 45, 411–421. [Google Scholar] [CrossRef]
- Stage, T.B.; Graff, M.; Wong, S.; Rasmussen, L.; Nielsen, F.; Pottegård, A.; Brøsen, K.; Kroetz, D.L.; Khojasteh, S.C.; Damkier, P. Dicloxacillin induces CYP2C19, CYP2C9 and CYP3A4 in vivo and in vitro. Br. J. Clin. Pharmacol. 2018, 84, 510–519. [Google Scholar] [CrossRef] [Green Version]
- Čížková, D.; Mokrý, J.; Mičuda, S.; Österreicher, J.; Martínková, J. Expression of MRP2 and MDR1 transporters and other hepatic markers in rat and human liver and in WRL 68 cell line. Physiol. Res. 2005, 54, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Mooij, M.G.; Schwarz, U.I.; De Koning, B.A.E.; Leeder, J.S.; Gaedigk, R.; Samsom, J.N.; Spaans, E.; van Goudoever, J.; Tibboel, D.; Kim, R.B.; et al. Ontogeny of Human Hepatic and Intestinal Transporter Gene Expression during Childhood: Age Matters. Drug Metab. Dispos. 2014, 42, 1268–1274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Human Transporters MRP2. Available online: https://www.solvobiotech.com/transporters/mrp2 (accessed on 20 January 2023).
- Maeda, T.; Takahashi, K.; Ohtsu, N.; Oguma, T.; Ohnishi, T.; Atsumi, R.; Tamai, I. Identification of Influx Transporter for the Quinolone Antibacterial Agent Levofloxacin. Mol. Pharm. 2007, 4, 85–94. [Google Scholar] [CrossRef]
- Franke, R.; Baker, S.; Mathijssen, R.; Schuetz, E.; Sparreboom, A. Influence of Solute Carriers on the Pharmacokinetics of CYP3A4 Probes. Clin. Pharmacol. Ther. 2008, 84, 704–709. [Google Scholar] [CrossRef] [PubMed]
- Mahalingam, A.; Shenoy, B. Tebipenem: A Novel Oral Carbapenem. Pediatr. Infect. Dis. 2020, 2, 25–28. [Google Scholar] [CrossRef]
- Nakakariya, M.; Shimada, T.; Irokawa, M.; Maeda, T.; Tamai, I. Identification and Species Similarity of OATP Transporters Responsible for Hepatic Uptake of β-Lactam Antibiotics. Drug Metab. Pharmacokinet. 2008, 23, 347–355. [Google Scholar] [CrossRef]
- Thomson, M.M.S.; Hines, R.N.; Schuetz, E.G.; Meibohm, B. Expression Patterns of Organic Anion Transporting Polypeptides 1B1 and 1B3 Protein in Human Pediatric Liver. Drug Metab. Dispos. 2016, 44, 999–1004. [Google Scholar] [CrossRef] [Green Version]
- Tamai, I.; Nezu, J.-I.; Uchino, H.; Sai, Y.; Oku, A.; Shimane, M.; Tsuji, A. Molecular Identification and Characterization of Novel Members of the Human Organic Anion Transporter (OATP) Family. Biochem. Biophys. Res. Commun. 2000, 273, 251–260. [Google Scholar] [CrossRef]
- Kato, K.; Shirasaka, Y.; Kuraoka, E.; Kikuchi, A.; Iguchi, M.; Suzuki, H.; Shibasaki, S.; Kurosawa, T.; Tamai, I. Intestinal absorption mechanism of tebipenem pivoxil, a novel oral carbapenem: Involvement of human OATP family in apical membrane transport. Mol. Pharm. 2010, 7, 1747–1756. [Google Scholar] [CrossRef]
- Nicolas, J.-M.; Bouzom, F.; Hugues, C.; Ungell, A.-L. Oral drug absorption in pediatrics: The intestinal wall, its developmental changes and current tools for predictions. Biopharm. Drug Dispos. 2017, 38, 209–230. [Google Scholar] [CrossRef] [Green Version]
- van Elburg, R.M.; Fetter, W.P.F.; Bunkers, C.M.; Heymans, H.S.A. Intestinal permeability in relation to birth weight and gestational and postnatal age. Arch. Dis. Child. Fetal Neonatal Ed. 2003, 88, F52–F55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flanagan, S.D.; Takahashi, L.H.; Liu, X.; Benet, L.Z. Contributions of saturable active secretion, passive transcellular, and paracellular diffusion to the overall transport of furosemide across adenocarcinoma (Caco-2) cells. J. Pharm. Sci. 2002, 91, 1169–1177. [Google Scholar] [CrossRef]
- Johnson, T.N.; Tanner, M.S.; Taylor, C.J.; Tucker, G.T. Enterocytic CYP3A4 in a paediatric population: Developmental changes and the effect of coeliac disease and cystic fibrosis. Br. J. Clin. Pharmacol. 2001, 51, 451–460. [Google Scholar] [CrossRef] [Green Version]
- Huang, N.N.; High, R.H. Comparison of serum levels following the administration of oral and parenteral preparations of penicillin to infants and children of various age groups. J. Pediatr. 1953, 42, 657–668. [Google Scholar] [CrossRef] [PubMed]
- Bergdahl, S.; Eriksson, M.; Finkel, Y. Plasma concentration following oral administration of di-and flucloxacillin in infants and children. Pharmacol. Toxicol. 1987, 60, 233–234. [Google Scholar] [CrossRef]
- Bergdahl, S.; Eriksson, M.; Finkel, Y.; Lännergren, K. Oral absorption of flucloxacillin in infants and young children. Acta Pharmacol. Toxicol. 1996, 58, 255–258. [Google Scholar] [CrossRef] [PubMed]
- Herngren, L.; Ehrnebo, M.; Broberger, U. Pharmacokinetics of free and total flucloxacilin in newborn infants. Eur. J. Clin. Pharmacol. 1987, 32, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.D.; Raeburn, J.A.; Devine, J.; Kirkwood, J.; Elliott, B.; Cockburn, F.; Forfar, J.O. Pharmacology of some oral penicillins in the newborn infant. Arch. Dis. Child. 1975, 50, 230–234. [Google Scholar] [CrossRef] [Green Version]
- Keij, F.M.; Tramper-Stranders, G.A.; Koch, B.C.P.; Reiss, I.K.M.; Muller, A.E.; Kornelisse, R.F.; Allegaert, K. Pharmacokinetics of Clavulanic Acid in the Pediatric Population: A Systematic Literature Review. Clin. Pharmacokinet. 2022, 61, 637–653. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, Y.; Xie, H.; Wang, R.; Jia, Z.; Men, X.; Xu, L.; Zhang, Q. Pharmacokinetics study of amoxycillin and clavulanic acid (8:1)-A new combination in healthy Chinese adult male volunteers using the LC–MS/MS method. Cell Biochem. Biophys. 2013, 65, 363–372. [Google Scholar] [CrossRef]
- Mir, F.; Pearce, R.E.; Baig-Ansari, N.; Qazi, S.; Barrett, J.S.; Abdel-Rahman, S.; Kearns, G.; Zaidi, A.K. Serum amoxicillin levels in young infants (0–59 days) with sepsis treated with oral amoxicillin. Arch. Dis. Child. 2020, 105, 1208–1214. [Google Scholar] [CrossRef]
- Autmizguine, J.; Watt, K.M.; Théorêt, Y.; Kassir, N.; Laferrière, C.; Parent, S.; Tapiéro, B.; Ovetchkine, P. Pharmacokinetics and pharmacodynamics of oral cephalexin in children with osteoarticular infections. Pediatr. Infect. Dis. J. 2013, 32, 1340–1344. [Google Scholar] [CrossRef]
- Boothman, R.; Kerr, M.M.; Marshall, M.J.; Burland, W.L. Absorption and excretion of cephalexin by the newborn infant. Arch. Dis. Child. 1973, 48, 147–150. [Google Scholar] [CrossRef] [Green Version]
- Ginsburg, C.M.; McCracken, G.H. Pharmacokinetics of Cephradine Suspension in Infants and Children. Antimicrob. Agents Chemother. 1979, 16, 74–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ginsburg, C.M.; McCracken, G.H.; Clahsen, J.C.; Thomas, M.L. Clinical Pharmacology of Cefadroxil in Infants and Children. Antimicrob. Agents Chemother. 1978, 13, 845–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chin, K.C.; Kerr, M.M.; Cockburn, F.; McAllister, T.A. A pharmacological study of cefaclor in the newborn infant. Curr. Med. Res. Opin. 1981, 7, 168–170. [Google Scholar] [CrossRef]
- McCracken, G.H.; Ginsburg, C.M.; Clahsen, J.C.; Thomas, M.L. Pharmacokinetics of cefaclor in infants and children. J. Antimicrob. Chemother. 1978, 4, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Sáez-Llorens, X.; Shyu, W.C.; Shelton, S.; Kumiesz, H.; Nelson, J. Pharmacokinetics of cefprozil in infants and children. Antimicrob. Agents Chemother. 1990, 34, 2152–2155. [Google Scholar] [CrossRef] [Green Version]
- Powell, D.A.; James, N.C.; Ossi, M.J.; Nahata, M.C.; Donn, K.H. Pharmacokinetics of cefuroxime axetil suspension in infants and children. Antimicrob. Agents Chemother. 1991, 35, 2042–2045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, B.J. Cefixime use in children: When and why. Can. J. Infect. Dis. 1995, 6, 204–205. [Google Scholar] [CrossRef] [Green Version]
- Kearns, G.L.; Reed, M.D.; Jacobs, R.F.; Ardite, M.; Yogev, R.D.; Blumer, J.L. Single-dose pharmacokinetics of ceftibuten (SCH 39720) in infants and children. Antimicrob. Agents Chemother. 1991, 35, 2078–2084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kearns, G.L.; Abdel-Rahman, S.M.; Jacobs, R.F.; Wells, T.G.; Borin, M.T. Cefpodoxime pharmacokinetics in children: Effect of food. Pediatr. Infect. Dis. J. 1998, 17, 799–804. [Google Scholar] [CrossRef] [PubMed]
- Sato, N.; Kijima, K.; Koresawa, T.; Mitomi, N.; Morita, J.; Suzuki, H.; Hayashi, H.; Shibasaki, S.; Kurosawa, T.; Totsuka, K. Population pharmacokinetics of tebipenem pivoxil (ME1211), a novel oral carbapenem antibiotic, in pediatric patients with otolaryngological infection or pneumonia. Drug Metab. Pharmacokinet. 2008, 23, 434–446. [Google Scholar] [CrossRef] [Green Version]
- Eriksson, M.; Bolme, P.; Blennow, M. Absorption of erythromycin from pediatric suspension in infants and children. Scand. J. Infect. Dis. 1981, 13, 211–215. [Google Scholar] [CrossRef]
- Stratchunsky, L.S.; Nazarov, A.D.; Firsov, A.A.; Petrachenkova, N.A. Age dependence of erythromycin rectal bioavailability in children. Eur. J. Drug Metab. Pharmacokinet. 1991, 3, 321–323. [Google Scholar]
- Nahata, M.C.; Koranyi, K.I.; Gadgil, S.D.; Hilligoss, D.M.; Fouda, H.G.; Gardner, M.J. Pharmacokinetics of azithromycin in pediatric patients after oral administration of multiple doses of suspension. Antimicrob. Agents Chemother. 1993, 37, 314–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevens, R.C.; Reed, M.D.; Shenep, J.L.; Baker, D.K.; Foulds, G.; Luke, D.R.; Blumer, J.L.; Rodman, J.H. Pharmacokinetics of azithromycin after single- and multiple-doses in children. Pharmacotherapy 1997, 17, 574–880. [Google Scholar]
- Liu, P.; Fang, A.F.; LaBadie, R.R.; Crownover, P.H.; Arguedas, A.G. Comparison of azithromycin pharmacokinetics following single oral doses of extended-release and immediate-release formulations in children with acute otitis media. Antimicrob. Agents Chemother. 2011, 55, 5022–5026. [Google Scholar] [CrossRef] [Green Version]
- Gan, V.N.; Chu, S.Y.; Kusmiesz, H.T.; Craft, J.C. Pharmacokinetics of a clarithromycin suspension in infants and children. Antimicrob. Agents Chemother. 1992, 36, 2478–2480. [Google Scholar] [CrossRef] [Green Version]
- Guay, D.R.P.; Craft, C.J. Overview of the pharmacology of clarithromycin suspension in children and a comparison with that in adults. Pediatr. Infect. Dis. J. 1993, 12 (Suppl. S3), S106–S111. [Google Scholar] [CrossRef]
- Minotti, C.; Bonadies, L.; Liberati, C.; De Pieri, M.; Giaquinto, C.; Baraldi, E.; Donà, D. Enteral Linezolid as an Effective Option to Treat an Extremely Preterm Infant with Bacillus cereus Sepsis. Children 2022, 9, 415. [Google Scholar] [CrossRef]
- Banniettis, N.; Sharma, R.; Hand, I.; Kohlhoff, S.; Peloquin, C.A.; Hammerschlag, M.R. Steady-state pharmacokinetics of oral linezolid suspension in a premature infant with osteomyelitis. J. Antimicrob. Chemother. 2016, 71, 1738. [Google Scholar] [CrossRef] [Green Version]
- Sicard, M.; Launay, E.; Caillon, J.; Jacqueline, C.; Legrand, A.; Deslandes, G.; Navas, D.; Rozé, J.-C.; Guen, C.G.-L. Pharmacokinetics of linezolid treatment using intravenous and oral administrations in extremely premature infants. Eur. J. Clin. Pharmacol. 2015, 71, 611–615. [Google Scholar] [CrossRef] [PubMed]
- A Pharmacokinetic Study of Tedizolid Phosphate in Pediatric Participants with Gram-Positive Infections (MK-1986-014). Available online: https://clinicaltrials.gov/ct2/show/NCT03217565 (accessed on 28 January 2023).
- Arrieta, A.C.; Ang, J.Y.; Espinosa, C.; Fofanov, O.; Tøndel, C.; Chou, M.Z.; De Anda, C.S.; Kim, J.Y.; Li, D.; Sabato, P.; et al. Pharmacokinetics and Safety of Single-dose Tedizolid Phosphate in Children 2 to <12 Years of Age. Pediatr. Infect. Dis. J. 2021, 40, 317–323. [Google Scholar] [CrossRef]
- Bradley, J.S.; Flanagan, S.D.; Arrieta, A.C.; Jacobs, R.; Capparelli, E.; Prokocimer, P. Pharmacokinetics, Safety and Tolerability of Single Oral or Intravenous Administration of 200 mg Tedizolid Phosphate in Adolescents. Pediatr. Infect. Dis. J. 2016, 35, 628–633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Payen, S.; Serreau, R.; Munck, A.; Aujard, Y.; Aigrain, Y.; Bressolle, F.; Jacqz-Aigrain, E. Population pharmacokinetics of ciprofloxacin in pediatric and adolescent patients with acute infections. Antimicrob. Agents Chemother. 2003, 47, 3170–3178. [Google Scholar] [CrossRef] [Green Version]
- Zhao, W.; Hill, H.; Le Guellec, C.; Neal, T.; Mahoney, S.; Paulus, S.; Castellan, C.; Kassai, B.; Anker, J.N.V.D.; Kearns, G.L.; et al. Population pharmacokinetics of ciprofloxacin in neonates and young infants less than three months of age. Antimicrob. Agents Chemother. 2014, 58, 6572–6580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chien, S.; Wells, T.G.; Blumer, J.L.; Kearns, G.L.; Bradley, J.S.; Bocchini, J.A., Jr.; Natarajan, J.; Maldonado, S.; Noel, G.J. Levofloxacin pharmacokinetics in children. J. Clin. Pharmacol. 2005, 45, 153–160. [Google Scholar] [CrossRef]
- Thee, S.; Garcia-Prats, A.J.; Draper, H.R.; McIlleron, H.M.; Wiesner, L.; Castel, S.; Schaaf, H.S.; Hesseling, A.C. Pharmacokinetics and safety of moxifloxacin in children with multidrug-resistant tuberculosis. Clin. Infect. Dis. 2014, 60, 549–556. [Google Scholar] [CrossRef] [Green Version]
- Capparelli, E.V.; Reed, M.D.; Bradley, J.S.; Kearns, G.L.; Jacobs, R.F.; Damle, B.D.; Blumer, J.L.; Grasela, D.M. Pharmacokinetics of gatifloxacin in infants and children. Antimicrob. Agents Chemother. 2005, 49, 1106–1112. [Google Scholar] [CrossRef] [Green Version]
- Siu, Y.K.; Ng, P.C.; Fung, S.C.K.; Lee, C.H.; Wong, M.Y.; Fok, T.F.; So, K.W.; Cheung, K.L.; Wong, W.; Cheng, A.F.B. Double blind, randomised, placebo controlled study of oral vancomycin in prevention of necrotising enterocolitis in preterm, very low birthweight infants. Arch. Dis. Child. Fetal Neonatal Ed. 1998, 79, F105–F109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antoon, J.W.; Hall, M.; Metropulos, D.; Steiner, M.J.; Jhaveri, R.; Lohr, J.A. A Prospective Pilot Study on the Systemic Absorption of Oral Vancomycin in Children with Colitis. J. Pediatr. Pharmacol. Ther. 2016, 21, 426–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergeron, L.; Boucher, F.D. Possible red-man syndrome associated with systemic absorption of oral vancomycin in a child with normal renal function. Ann. Pharmacother. 1994, 28, 581–584. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, S.; Suzuki, T.; Suzuki, T.; Takatsuka, H.; Ishikawa, M.; Hattori, N.; Fujishiro, T.; Miyauchi, H.; Oami, T.; Ariyoshi, N.; et al. An extremely high bioavailability of orally administered vancomycin in a patient with severe colitis and renal insufficiency. J. Infect. Chemother. 2017, 23, 848–851. [Google Scholar] [CrossRef]
- Autmizguine, J.; Melloni, C.; Hornik, C.P.; Dallefeld, S.; Harper, B.; Yogev, R.; Sullivan, J.E.; Atz, A.M.; Al-Uzri, A.; Mendley, S.; et al. Population Pharmacokinetics of Trimethoprim-Sulfamethoxazole in Infants and Children. Antimicrob. Agents Chemother. 2017, 62, e01813-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Álvarez, L.A.; Van de Sijpe, G.; Desmet, S.; Metsemakers, W.-J.; Spriet, I.; Allegaert, K.; Rozenski, J. Ways to Improve Insights into Clindamycin Pharmacology and Pharmacokinetics Tailored to Practice. Antibiotics 2022, 11, 701. [Google Scholar] [CrossRef]
- Hashemian, S.M.; Farhadi, Z.; Farhadi, T. Fosfomycin: The characteristics, activity, and use in critical care. Ther. Clin. Risk Manag. 2019, 15, 525–530. [Google Scholar] [CrossRef] [Green Version]
- Kane, Z.; Gastine, S.; Obiero, C.; Williams, P.; Murunga, S.; Thitiri, J.; Ellis, S.; Correia, E.; Nyaoke, B.; Kipper, K.; et al. IV and oral fosfomycin pharmacokinetics in neonates with suspected clinical sepsis. J. Antimicrob. Chemother. 2021, 76, 1855–1864. [Google Scholar] [CrossRef]
- Dijkmans, A.C.; Zacarías, N.V.O.; Burggraaf, J.; Mouton, J.W.; Wilms, E.B.; van Nieuwkoop, C.; Touw, D.J.; Stevens, J.; Kamerling, I.M.C. Fosfomycin: Pharmacological, Clinical and Future Perspectives. Antibiotics 2017, 6, 24. [Google Scholar] [CrossRef] [Green Version]
- Schaaf, H.S.; Willemse, M.; Cilliers, K.; Labadarios, D.; Maritz, J.S.; Hussey, G.D.; McIlleron, H.; Smith, P.; Donald, P.R. Rifampin pharmacokinetics in children, with and without human immunodeficiency virus infection, hospitalized for the management of severe forms of tuberculosis. BMC Med. 2009, 7, 19. [Google Scholar] [CrossRef] [Green Version]
- Koup, J.R.; Williams-Warren, J.; Viswanathan, C.T.; Weber, A.; Smith, A.L. Pharmacokinetics of Rifampin in Children II. Oral Bioavailability. Ther. Drug Monit. 1986, 8, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.B.; Cotten, C.M.; Hudak, M.L.; Sullivan, J.E.; Poindexter, B.B.; Cohen-Wolkowiez, M.; Boakye-Agyeman, F.; Lewandowski, A.; Anand, R.; Benjamin, D.K.; et al. Rifampin Pharmacokinetics and Safety in Preterm and Term Infants. Antimicrob. Agents Chemother. 2019, 63, e00284-19. [Google Scholar] [CrossRef] [Green Version]
- Benedetti, M.S.; Whomsley, R.; Baltes, E.L. Differences in absorption, distribution, metabolism and excretion of xenobiotics between the paediatric and adult populations. Expert Opin. Drug Metab. Toxicol. 2005, 1, 447–471. [Google Scholar] [CrossRef] [PubMed]
- Turner, C.; Thein, N.A.M.; Turner, P.; Nosten, F.; White, N.J. Rectal pH in well and unwell infants. J. Trop. Pediatr. 2012, 58, 311–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rathi, R.; Kumar, A.; Vishvakarma, V.; Huanbutta, K.; Singh, I.; Sangnim, T. Advancements in Rectal Drug Delivery Systems: Clinical Trials, and Patents Perspective. Pharmaceutics 2022, 14, 2210. [Google Scholar] [CrossRef] [PubMed]
- Linakis, M.W.; Roberts, J.K.; Lala, A.C.; Spigarelli, M.G.; Medlicott, N.; Reith, D.M.; Ward, R.M.; Sherwin, C.M.T. Challenges Associated with Route of Administration in Neonatal Drug Delivery. Clin. Pharmacokinet. 2016, 55, 185–196. [Google Scholar] [CrossRef]
- El-Gendy, N.; Kaviratna, A.; Berkland, C.; Dhar, P. Delivery and performance of surfactant replacement therapies to treat pulmonary disorders. Ther. Deliv. 2013, 4, 951–980. [Google Scholar] [CrossRef] [Green Version]
- Hansen, T.G. Developmental paediatric anaesthetic pharmacology. Anaesth. Intensiv. Care Med. 2018, 19, 437–443. [Google Scholar] [CrossRef]
- Meesters, K.; Alemayehu, T.; Benou, S.; Buonsenso, D.; Decloedt, E.H.; Lorente, V.P.-F.; Downes, K.J.; Allegaert, K. Pharmacokinetics of Antimicrobials in Children with Emphasis on Challenges Faced by Low and Middle Income Countries, a Clinical Review. Antibiotics 2022, 12, 17. [Google Scholar] [CrossRef]
- Young, A.; Brown, L.K.; Ennis, S.; Beattie, R.M.; Johnson, M.J. Total body water in full-term and preterm newborns: Systematic review and meta-analysis. Arch. Dis. Child. Fetal Neonatal Ed. 2021, 106, 542–548. [Google Scholar] [CrossRef]
- Villar, J.; Puglia, F.A.; Fenton, T.R.; Ismail, L.C.; Staines-Urias, E.; Giuliani, F.; Ohuma, E.O.; Victora, C.G.; Sullivan, P.; Barros, F.C.; et al. Body composition at birth and its relationship with neonatal anthropometric ratios: The newborn body composition study of the INTERGROWTH-21st project. Pediatr. Res. 2017, 82, 305–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bortolotto, C.C.; Santos, I.S.; Vaz, J.D.S.; Matijasevich, A.; Barros, A.J.D.; Barros, F.C.; Santos, L.P.; Munhoz, T.N. Prematurity and body composition at 6, 18, and 30 years of age: Pelotas (Brazil) 2004, 1993, and 1982 birth cohorts. BMC Public Health 2021, 21, 321. [Google Scholar] [CrossRef] [PubMed]
- Anderson, B.J. Neonatal pharmacology. Anaesth. Intensiv. Care Med. 2016, 18, 68–74. [Google Scholar] [CrossRef]
- Ahmed, H.; Bergmann, F.; Zeitlinger, M. Protein Binding in Translational Antimicrobial Development-Focus on Interspecies Differences. Antibiotics 2022, 11, 923. [Google Scholar] [CrossRef] [PubMed]
- Torer, B.; Hanta, D.; Yapakci, E.; Gokmen, Z.; Parlakgumus, A.; Gulcan, H.; Tarcan, A. Association of Serum Albumin Level and Mortality in Premature Infants. J. Clin. Lab. Anal. 2016, 30, 867–872. [Google Scholar] [CrossRef] [Green Version]
- Bunt, J.E.H.; Rietveld, T.; Schierbeek, H.; Wattimena, J.L.D.; Zimmermann, L.J.I.; van Goudoever, J.B. Albumin synthesis in preterm infants on the first day of life studied with [1-13C]leucine. Am. J. Physiol. Gastrointest. Liver Physiol. 2007, 292, G1157–G1161. [Google Scholar] [CrossRef] [Green Version]
- Trainor, G.L. The importance of plasma protein binding in drug discovery. Expert Opin. Drug Discov. 2007, 2, 51–64. [Google Scholar] [CrossRef]
- Maharaj, A.R.; Gonzalez, D.; Cohen-Wolkowiez, M.; Hornik, C.P.; Edginton, A.N. Improving Pediatric Protein Binding Estimates: An Evaluation of α1-Acid Glycoprotein Maturation in Healthy and Infected Subjects. Clin. Pharmacokinet. 2018, 57, 577–589. [Google Scholar] [CrossRef]
- Anell-Olofsson, M.; Ahmadi, S.; Lönnqvist, P.; Eksborg, S.; von Horn, H.; Bartocci, M. Plasma concentrations of alpha-1-acid glycoprotein in preterm and term newborns: Influence of mode of delivery and implications for plasma protein binding of local anaesthetics. Br. J. Anaesth. 2018, 121, 427–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Wright, M.; Hop, C.E.C.A. Rational use of plasma protein and tissue binding data in drug design. J. Med. Chem. 2014, 57, 8238–8248. [Google Scholar] [CrossRef] [PubMed]
- Neuville, M.; El-Helali, N.; Magalhaes, E.; Radjou, A.; Smonig, R.; Soubirou, J.-F.; Voiriot, G.; Le Monnier, A.; Ruckly, S.; Bouadma, L.; et al. Systematic overdosing of oxa- and cloxacillin in severe infections treated in ICU: Risk factors and side effects. Ann. Intensiv. Care 2017, 7, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ulldemolins, M.; Roberts, J.A.; Wallis, S.C.; Rello, J.; Lipman, J. Flucloxacillin dosing in critically ill patients with hypoalbuminaemia: Special emphasis on unbound pharmacokinetics. J. Antimicrob. Chemother. 2010, 65, 1771–1778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallenburg, E.; ter Heine, R.; de Lange, D.W.; van Leeuwen, H.; Schouten, J.A.; Oever, J.T.; Kolwijck, E.; Burger, D.M.; Pickkers, P.; Gieling, E.M.; et al. High unbound flucloxacillin fraction in critically ill patients. J. Antimicrob. Chemother. 2021, 76, 3220–3228. [Google Scholar] [CrossRef] [PubMed]
- Pullen, J.; Stolk, L.M.L.; Degraeuwe, P.L.J.; Van Tiel, F.H.; Neef, C.; Zimmermann, L.J.I. Protein binding of flucloxacillin in neonates. Ther. Drug Monit. 2007, 29, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Jongmans, C.; Muller, A.E.; Broek, P.V.D.; Almeida, B.D.M.C.D.; Berg, C.V.D.; Van Oldenrijk, J.; Bos, P.K.; Koch, B.C.P. An Overview of the Protein Binding of Cephalosporins in Human Body Fluids: A Systematic Review. Front. Pharmacol. 2022, 13, 900551. [Google Scholar] [CrossRef]
- Kan, M.; Wu, Y.-E.; Li, X.; Dong, Y.-N.; Du, B.; Guo, Z.-X.; Shi, H.-Y.; Huang, X.; Su, L.-Q.; Wang, W.-Q.; et al. An adapted LC-MS/MS method for the determination of free plasma concentration of cefoperazone in children: Age-dependent protein binding. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2020, 1144, 122081. [Google Scholar] [CrossRef]
- DrugBank Online. Ceftriaxone. Available online: https://go.drugbank.com/drugs/DB01212 (accessed on 1 February 2023).
- Kan, M.; Shi, H.-Y.; Han, B.; Wu, Y.-E.; Li, Q.; Guo, Z.-X.; Li, X.; Hao, G.-X.; Zheng, Y.; Su, L.-Q.; et al. Prediction of Unbound Ceftriaxone Concentration in Children: Simple Bioanalysis Method and Basic Mathematical Equation. Antimicrob. Agents Chemother. 2020, 65, e00779-20. [Google Scholar] [CrossRef]
- Hartman, S.J.F.; Upadhyay, P.J.; Hagedoorn, N.N.; Mathôt, R.A.A.; Moll, H.A.; van der Flier, M.; Schreuder, M.F.; Brüggemann, R.J.; Knibbe, C.A.; de Wildt, S.N. Current Ceftriaxone Dose Recommendations are Adequate for Most Critically Ill Children: Results of a Population Pharmacokinetic Modeling and Simulation Study. Clin. Pharmacokinet. 2021, 60, 1361–1372. [Google Scholar] [CrossRef] [PubMed]
- Schleibinger, M.; Steinbach, C.L.; Töpper, C.; Kratzer, A.; Liebchen, U.; Kees, F.; Salzberger, B.; Kees, M.G. Protein binding characteristics and pharmacokinetics of ceftriaxone in intensive care unit patients. Br. J. Clin. Pharmacol. 2015, 80, 525–533. [Google Scholar] [CrossRef] [Green Version]
- Majumdar, A.K.; Musson, D.G.; Birk, K.L.; Kitchen, C.J.; Holland, S.; McCrea, J.; Mistry, G.; Hesney, M.; Xi, L.; Li, S.X.; et al. Pharmacokinetics of Ertapenem in Healthy Young Volunteers. Antimicrob. Agents Chemother. 2002, 46, 3506–3511. [Google Scholar] [CrossRef] [Green Version]
- Burkhardt, O.; Kumar, V.; Katterwe, D.; Majcher-Peszynska, J.; Drewelow, B.; Derendorf, H.; Welte, T. Ertapenem in critically ill patients with early-onset ventilator-associated pneumonia: Pharmacokinetics with special consideration of free-drug concentration. J. Antimicrob. Chemother. 2007, 59, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Musson, D.G.; Majumdar, A.; Holland, S.; Birk, K.; Xi, L.; Mistry, G.; Sciberras, D.; Muckow, J.; Deutsch, P.; Rogers, J.D. Pharmacokinetics of total and unbound ertapenem in healthy elderly subjects. Antimicrob. Agents Chemother. 2004, 48, 521–524. [Google Scholar] [CrossRef] [Green Version]
- DrugBank Online. Teicoplanin. Available online: https://go.drugbank.com/drugs/DB06149 (accessed on 1 February 2023).
- Sando, M.; Sato, Y.; Iwata, S.; Akita, H.; Sunakawa, K. In vitro protein binding of teicoplanin to neonatal serum. J. Infect. Chemother. 2004, 10, 280–283. [Google Scholar] [CrossRef]
- Smits, A.; Pauwels, S.; Oyaert, M.; Peersman, N.; Spriet, I.; Saegeman, V.; Allegaert, K. Factors impacting unbound vancomycin concentrations in neonates and young infants. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 1503–1510. [Google Scholar] [CrossRef] [PubMed]
- Turner, N.A.; Xu, A.; Zaharoff, S.; Holland, T.L.; Lodise, T.P. Determination of plasma protein binding of dalbavancin. J. Antimicrob. Chemother. 2022, 77, 1899–1902. [Google Scholar] [CrossRef] [PubMed]
- DrugBank Online. Telavancin. Available online: https://go.drugbank.com/drugs/DB06402 (accessed on 1 February 2023).
- DrugBank Online. Oritavancin. Available online: https://go.drugbank.com/drugs/DB04911 (accessed on 1 February 2023).
- Corona, A.; Agarossi, A.; Veronese, A.; Cattaneo, D.; D’Avolio, A. Therapeutic Drug Monitoring of Dalbavancin Treatment in Severe Necrotizing Fasciitis in 3 Critically Ill Patients: A Grand Round. Ther. Drug Monit. 2020, 42, 165–168. [Google Scholar] [CrossRef]
- DrugBank Online. Erythromycin. Available online: https://go.drugbank.com/drugs/DB00199 (accessed on 1 February 2023).
- DrugBank Online. Clarithromycin. Available online: https://go.drugbank.com/drugs/DB01211 (accessed on 1 February 2023).
- Viscardi, R.M.; Othman, A.A.; Hassan, H.E.; Eddington, N.D.; Abebe, E.; Terrin, M.L.; Kaufman, D.A.; Waites, K.B. Azithromycin to prevent bronchopulmonary dysplasia in ureaplasma-infected preterm infants: Pharmacokinetics, safety, microbial response, and clinical outcomes with a 20-milligram-per-kilogram single intravenous dose. Antimicrob. Agents Chemother. 2013, 57, 2127–2133. [Google Scholar] [CrossRef] [Green Version]
- Hassan, H.E.; Othman, A.A.; Eddington, N.D.; Duffy, L.; Xiao, L.; Waites, K.B.; Kaufman, D.A.; Fairchild, K.D.; Terrin, M.L.; Viscardi, R.M. Pharmacokinetics, safety, and biologic effects of azithromycin in extremely preterm infants at risk for ureaplasma colonization and bronchopulmonary dysplasia. J. Clin. Pharmacol. 2011, 51, 1264–1275. [Google Scholar] [CrossRef] [Green Version]
- Kratzer, A.; Kees, F.; Dorn, C. Unbound fraction of fluconazole and linezolid in human plasma as determined by ultrafiltration: Impact of membrane type. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2016, 1039, 74–78. [Google Scholar] [CrossRef]
- Ogami, C.; Tsuji, Y.; To, H.; Yamamoto, Y. Pharmacokinetics, toxicity and clinical efficacy of linezolid in Japanese pediatric patients. J. Infect. Chemother. 2019, 25, 979–986. [Google Scholar] [CrossRef]
- DrugBank Online. Tedizolid. Available online: https://go.drugbank.com/drugs/DB14569 (accessed on 1 February 2023).
- Iqbal, K.; Milioudi, A.; Wicha, S.G. Pharmacokinetics and Pharmacodynamics of Tedizolid. Clin. Pharmacokinet. 2022, 61, 489–503. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, D.; Delmore, P.; Bloom, B.T.; Cotten, C.M.; Poindexter, B.B.; McGowan, E.; Shattuck, K.; Bradford, K.K.; Smith, P.B.; Cohen-Wolkowiez, M.; et al. Clindamycin Pharmacokinetics and Safety in Preterm and Term Infants. Antimicrob. Agents Chemother. 2016, 60, 2888–2894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DrugBank Online. Lincomycin. Available online: https://go.drugbank.com/drugs/DB01627 (accessed on 1 February 2023).
- Schneider, E.K.; Huang, J.X.; Carbone, V.; Han, M.; Zhu, Y.; Nang, S.; Khoo, K.K.; Mak, J.; Cooper, M.A.; Li, J.; et al. Plasma Protein Binding Structure–Activity Relationships Related to the N-Terminus of Daptomycin. ACS Infect. Dis. 2017, 3, 249–258. [Google Scholar] [CrossRef] [PubMed]
- DrugBank Online. Daptomycin. Available online: https://go.drugbank.com/drugs/DB00080 (accessed on 1 February 2023).
- Ye, L.; You, X.; Zhou, J.; Wu, C.; Ke, M.; Wu, W.; Huang, P.; Lin, C. Physiologically based pharmacokinetic modeling of daptomycin dose optimization in pediatric patients with renal impairment. Front. Pharmacol. 2022, 13, 838599. [Google Scholar] [CrossRef]
- DrugBank Online. Levofloxacin. Available online: https://go.drugbank.com/drugs/DB01137 (accessed on 1 February 2023).
- Mitsuboshi, S.; Yamada, H.; Nagai, K.; Ueno, K. No effect of protein binding ratio of levofloxacin in hemodialysis patients. Ren. Replace. Ther. 2016, 2, 28. [Google Scholar] [CrossRef] [Green Version]
- DrugBank Online. Moxifloxacin. Available online: https://go.drugbank.com/drugs/DB00218 (accessed on 1 February 2023).
- Obiero, C.W.; Williams, P.; Murunga, S.; Thitiri, J.; Omollo, R.; Walker, A.S.; Egondi, T.; Nyaoke, B.; Correia, E.; Kane, Z.; et al. Randomised controlled trial of fosfomycin in neonatal sepsis: Pharmacokinetics and safety in relation to sodium overload. Arch. Dis. Child. 2022, 107, 802–810. [Google Scholar] [CrossRef] [PubMed]
- Verbeeck, R.K.; Singu, B.S.; Kibuule, D. Clinical Significance of the Plasma Protein Binding of Rifampicin in the Treatment of Tuberculosis Patients. Clin. Pharmacokinet. 2019, 58, 1511–1515. [Google Scholar] [CrossRef]
- Litjens, C.H.C.; Aarnoutse, R.E.; Kolmer, E.W.J.V.E.-B.; Svensson, E.M.; Colbers, A.; Burger, D.M.; Boeree, M.J.; Brake, L.H.M.T.; Heinrich, N.; Diacon, A.; et al. Protein binding of rifampicin is not saturated when using high-dose rifampicin. J. Antimicrob. Chemother. 2019, 74, 986–990. [Google Scholar] [CrossRef]
- Amin, S.B. Bilirubin Binding Capacity in the Preterm Neonate. Clin. Perinatol. 2016, 43, 241–257. [Google Scholar] [CrossRef] [Green Version]
- DrugBank Online. Sulfamethoxazole. Available online: https://go.drugbank.com/drugs/DB01015 (accessed on 1 February 2023).
- DrugBank Online. Trimethoprim. Available online: https://go.drugbank.com/drugs/DB00440 (accessed on 1 February 2023).
- Thyagarajan, B.; Deshpande, S.S. Cotrimoxazole and neonatal kernicterus: A review. Drug Chem. Toxicol. 2014, 37, 121–129. [Google Scholar] [CrossRef] [Green Version]
- Hile, G.B.; Musick, K.L.; Dugan, A.J.; Bailey, A.M.; Howington, G.T. Occurrence of Hyperbilirubinemia in Neonates Given a Short-term Course of Ceftriaxone versus Cefotaxime for Sepsis. J. Pediatr. Pharmacol. Ther. 2021, 26, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Amin, S.B. Bilirubin-Displacing Effect of Ceftriaxone in Infants with Unconjugated Hyperbilirubinemia Born at Term. J. Pediatr. 2022, 254, 91–95. [Google Scholar] [CrossRef]
- Jubeh, B.; Breijyeh, Z.; Karaman, R. Antibacterial Prodrugs to Overcome Bacterial Resistance. Molecules 2020, 25, 1543. [Google Scholar] [CrossRef] [Green Version]
- Frampton, J.E. Ceftaroline Fosamil: A Review of its Use in the Treatment of Complicated Skin and Soft Tissue Infections and Community-Acquired Pneumonia. Drugs 2013, 73, 1067–1094. [Google Scholar] [CrossRef] [PubMed]
- Eichenbaum, G.; Skibbe, J.; Parkinson, A.; Johnson, M.D.; Baumgardner, D.; Ogilvie, B.; Usuki, E.; Tonelli, F.; Holsapple, J.; Schmitt-Hoffmann, A. Use of enzyme inhibitors to evaluate the conversion pathways of ester and amide prodrugs: A case study example with the prodrug ceftobiprole medocaril. J. Pharm. Sci. 2012, 101, 1242–1252. [Google Scholar] [CrossRef] [PubMed]
- McEntee, L.; Johnson, A.; Farrington, N.; Unsworth, J.; Dane, A.; Jain, A.; Cotroneo, N.; Critchley, I.; Melnick, D.; Parr, T.; et al. Pharmacodynamics of Tebipenem: New Options for Oral Treatment of Multidrug-Resistant Gram-Negative Infections. Antimicrob. Agents Chemother. 2019, 63, e00603. [Google Scholar] [CrossRef] [Green Version]
- Dingsdag, S.A.; Hunter, N. Metronidazole: An update on metabolism, structure–cytotoxicity and resistance mechanisms. J. Antimicrob. Chemother. 2018, 73, 265–279. [Google Scholar] [CrossRef] [Green Version]
- Obach, R.S. Linezolid Metabolism Is Catalyzed by Cytochrome P450 2J2, 4F2, and 1B1. Drug Metab. Dispos. 2022, 50, 413–421. [Google Scholar] [CrossRef]
- Fanni, D.; Ambu, R.; Gerosa, C.; Nemolato, S.; Castagnola, M.; Van Eyken, P.; Faa, G.; Fanos, V. Cytochrome P450 genetic polymorphism in neonatal drug metabolism: Role and practical consequences towards a new drug culture in neonatology. Int. J. Immunopathol. Pharmacol. 2014, 27, 5–13. [Google Scholar] [CrossRef]
- Ruggiero, A.; Ariano, A.; Triarico, S.; Capozza, M.A.; Ferrara, P.; Attinà, G. Neonatal pharmacology and clinical implications. Drugs Context 2019, 8, 212608. [Google Scholar] [CrossRef] [Green Version]
- Allegaert, K.; Anker, J.D. Ontogeny of Phase I Metabolism of Drugs. J. Clin. Pharmacol. 2019, 59 (Suppl. S1), S33–S41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tateishi, T.; Nakura, H.; Asoh, M.; Watanabe, M.; Tanaka, M.; Kumai, T.; Takashima, S.; Imaoka, S.; Funae, Y.; Yabusaki, Y.; et al. A comparison of hepatic cytochrome p450 protein expression between infancy and postinfancy. Life Sci. 1997, 61, 2567–2574. [Google Scholar] [CrossRef] [PubMed]
- Zane, N.R.; Chen, Y.; Wang, M.Z.; Thakker, D.R. Cytochrome P450 and flavin-containing monooxygenase families: Age-dependent differences in expression and functional activity. Pediatr. Res. 2018, 83, 527–535. [Google Scholar] [CrossRef] [PubMed]
- Hines, R. Developmental expression of drug metabolizing enzymes: Impact on disposition in neonates and young children. Int. J. Pharm. 2013, 452, 3–7. [Google Scholar] [CrossRef]
- Ku, L.C.; Smith, P.B. Dosing in neonates: Special considerations in physiology and trial design. Pediatr. Res. 2014, 77, 2–9. [Google Scholar] [CrossRef] [Green Version]
- O’Hara, K. Pharmacokinetic changes with growth and development between birth and adulthood. J. Pharm. Pract. Res. 2017, 47, 313–318. [Google Scholar] [CrossRef]
- Song, G.; Sun, X.; Hines, R.N.; McCarver, D.G.; Lake, B.G.; Osimitz, T.G.; Creek, M.R.; Clewell, H.J.; Yoon, M. Determination of Human Hepatic CYP2C8 and CYP1A2 Age-Dependent Expression to Support Human Health Risk Assessment for Early Ages. Drug Metab. Dispos. 2017, 45, 468–475. [Google Scholar] [CrossRef] [Green Version]
- van Groen, B.D.; Nicolaï, J.; Kuik, A.C.; Van Cruchten, S.; van Peer, E.; Smits, A.; Schmidt, S.; de Wildt, S.N.; Allegaert, K.; De Schaepdrijver, L.; et al. Ontogeny of Hepatic Transporters and Drug-Metabolizing Enzymes in Humans and in Nonclinical Species. Pharmacol. Rev. 2021, 73, 597–678. [Google Scholar] [CrossRef]
- Choudhary, D.; Jansson, I.; Schenkman, J.; Sarfarazi, M.; Stoilov, I. Comparative expression profiling of 40 mouse cytochrome P450 genes in embryonic and adult tissues. Arch. Biochem. Biophys. 2003, 414, 91–100. [Google Scholar] [CrossRef]
- van den Anker, J.; Reed, M.D.; Allegaert, K.; Kearns, G.L. Developmental Changes in Pharmacokinetics and Pharmacodynamics. J. Clin. Pharmacol. 2018, 58 (Suppl. S10), S10–S25. [Google Scholar] [CrossRef] [Green Version]
- Koukouritaki, S.B.; Manro, J.R.; Marsh, S.A.; Stevens, J.C.; Rettie, A.E.; McCarver, D.G.; Hines, R. Developmental expression of human hepatic CYP2C9 and CYP2C19. Experiment 2003, 308, 965–974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevens, J.C.; Marsh, S.A.; Zaya, M.J.; Regina, K.J.; Divakaran, K.; Le, M.; Hines, R.N. Developmental changes in human liver CYP2D6 expression. Drug Metab. Dispos. 2008, 36, 1587–1593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnsrud, E.K.; Koukouritaki, S.B.; Divakaran, K.; Brunengraber, L.L.; Hines, R.N.; McCarver, D.G. Human hepatic CYP2E1 expression during development. J. Pharmacol. Exp. Ther. 2003, 307, 402–407. [Google Scholar] [CrossRef]
- Wynalda, M.A.; Hutzler, J.M.; Koets, M.D.; Podoll, T.; Wienkers, L.C. In Vitro Metabolism of Clindamycin in Human Liver and Intestinal Microsomes. Drug Metab. Dispos. 2003, 31, 878–887. [Google Scholar] [CrossRef] [PubMed]
- Lacroix, D.; Sonnier, M.; Moncion, A.; Cheron, G.; Cresteil, T. Expression of CYP3A in the human liver-Evidence that the shift between CYP3A7 and CYP3A4 occurs immediately after birth. Eur. J. Biochem. 1997, 247, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.A.; Ring, B.J.; Cantrell, V.E.; Jones, D.R.; Eckstein, J.; Ruterbories, K.; Hamman, M.A.; Hall, S.D.; Wrighton, S.A. Comparative metabolic capabilities of CYP3A4, CYP3A5, and CYP3A7. Drug Metab. Dispos. 2002, 30, 883–891. [Google Scholar] [CrossRef]
- Zhang, L.; Xu, X.; Badawy, S.; Ihsan, A.; Liu, Z.; Xie, C.; Wang, X.; Tao, Y. A Review: Effects of Macrolides on CYP450 Enzymes. Curr. Drug Metab. 2020, 21, 928–937. [Google Scholar] [CrossRef]
- Srinivas, N.R. Pharmacokinetic Interaction of Rifampicin with Oral versus Intravenous Anticancer Drugs: Challenges, Dilemmas and Paradoxical Effects Due to Multiple Mechanisms. Drugs R D 2016, 16, 141–148. [Google Scholar] [CrossRef] [Green Version]
- Derungs, A.; Donzelli, M.; Berger, B.; Noppen, C.; Krähenbühl, S.; Haschke, M. Effects of Cytochrome P450 Inhibition and Induction on the Phenotyping Metrics of the Basel Cocktail: A Randomized Crossover Study. Clin. Pharmacokinet. 2016, 55, 79–91. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Wei, M.-J.; Zhao, C.-Y.; Qi, H.-M. Determination of the inhibitory potential of 6 fluoroquinolones on CYP1A2 and CYP2C9 in human liver microsomes. Acta Pharmacol. Sin. 2008, 29, 1507–1514. [Google Scholar] [CrossRef]
- Watanabe, A.; Takakusa, H.; Kimura, T.; Inoue, S.-I.; Kusuhara, H.; Ando, O. Analysis of Mechanism-Based Inhibition of CYP 3A4 by a Series of Fluoroquinolone Antibacterial Agents. Drug Metab. Dispos. 2016, 44, 1608–1616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watanabe, A.; Takakusa, H.; Kimura, T.; Inoue, S.-I.; Kusuhara, H.; Ando, O. Difference in Mechanism-Based Inhibition of Cytochrome P450 3A4 and 3A5 by a Series of Fluoroquinolone Antibacterial Agents. Drug Metab. Dispos. 2017, 45, 336–341. [Google Scholar] [CrossRef] [Green Version]
- Niwa, T.; Morimoto, M.; Hirai, T.; Hata, T.; Hayashi, M.; Imagawa, Y. Effect of penicillin-based antibiotics, amoxicillin, ampicillin, and piperacillin, on drug-metabolizing activities of human hepatic cytochromes P450. J. Toxicol. Sci. 2016, 41, 143–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huwyler, J.; Wright, M.; Gutmann, H.; Drewe, J. Induction of Cytochrome P450 3A4 and P-Glycoprotein by the Isoxazolyl- Penicillin Antibiotic Flucloxacillin. Curr. Drug Metab. 2006, 7, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Mahmoudi, M.; Brenner, T.; Hatiboglu, G.; Burhenne, J.; Weiss, J.; Weigand, M.A.; Haefeli, W.E. Substantial Impairment of Voriconazole Clearance by High-Dose Meropenem in a Patient with Renal Failure. Clin. Infect. Dis. 2017, 65, 1033–1036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cada, D.J.; Baker, D.E. Oritavancin Diphosphate. Hosp. Pharm. 2014, 49, 1049–1060. [Google Scholar] [CrossRef] [Green Version]
- Cattaneo, D.; Gervasoni, C.; Corona, A. The Issue of Pharmacokinetic-Driven Drug-Drug Interactions of Antibiotics: A Narrative Review. Antibiotics 2022, 11, 1410. [Google Scholar] [CrossRef]
- Wen, X.; Wang, J.-S.; Backman, J.T.; Laitila, J.; Neuvonen, P.J. Trimethoprim and sulfamethoxazole are selective inhibitors of CYP2C8 and CYP2C9, respectively. Drug Metab. Dispos. 2002, 30, 631–635. [Google Scholar] [CrossRef] [Green Version]
- Türk, D.; Hanke, N.; Lehr, T. A Physiologically-Based Pharmacokinetic Model of Trimethoprim for MATE1, OCT1, OCT2, and CYP2C8 Drug–Drug–Gene Interaction Predictions. Pharmaceutics 2020, 12, 1074. [Google Scholar] [CrossRef]
- Li, H.; Lampe, J.N. Neonatal cytochrome P450 CYP3A7: A comprehensive review of its role in development, disease, and xenobiotic metabolism. Arch. Biochem. Biophys. 2019, 673, 108078. [Google Scholar] [CrossRef]
- Usui, T.; Saitoh, Y.; Komada, F. Induction of CYP3As in HepG2 cells by several drugs. Association between induction of CYP3A4 and expression of glucocorticoid receptor. Biol. Pharm. Bull. 2003, 26, 510–517. [Google Scholar] [CrossRef] [Green Version]
- Boberg, M.; Vrana, M.; Mehrotra, A.; Pearce, R.E.; Gaedigk, A.; Bhatt, D.K.; Leeder, J.S.; Prasad, B. Age-Dependent Absolute Abundance of Hepatic Carboxylesterases (CES1 and CES2) by LC-MS/MS Proteomics: Application to PBPK Modeling of Oseltamivir In Vivo Pharmacokinetics in Infants. Drug Metab. Dispos. 2017, 45, 216–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koukouritaki, S.B.; Simpson, P.; Yeung, C.K.; Rettie, A.E.; Hines, R.N. Human Hepatic Flavin-Containing Monooxygenases 1 (FMO1) and 3 (FMO3) Developmental Expression. Pediatr. Res. 2002, 51, 236–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, M.; Bhatt, D.K.; Yeung, C.K.; Claw, K.G.; Chaudhry, A.S.; Gaedigk, A.; Pearce, R.E.; Broeckel, U.; Gaedigk, R.; Nickerson, D.A.; et al. Genetic and Nongenetic Factors Associated with Protein Abundance of Flavin-Containing Monooxygenase 3 in Human Liver. J. Pharmacol. Exp. Ther. 2017, 363, 265–274. [Google Scholar] [CrossRef] [Green Version]
- Bhatt, D.K.; Gaedigk, A.; Pearce, R.E.; Leeder, J.S.; Prasad, B. Age-dependent Protein Abundance of Cytosolic Alcohol and Aldehyde Dehydrogenases in Human Liver. Drug Metab. Dispos. 2017, 45, 1044–1048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pacifici, G.M.; Franchi, M.; Giuliani, L.; Rane, A. Development of the glucuronyltransferase and sulphotransferase towards 2-naphthol in human fetus. Dev. Pharmacol. Ther. 1989, 14, 108–114. [Google Scholar] [CrossRef]
- Ladumor, M.K.; Bhatt, D.K.; Gaedigk, A.; Sharma, S.; Thakur, A.; Pearce, R.E.; Leeder, J.S.; Bolger, M.B.; Singh, S.; Prasad, B. Ontogeny of Hepatic Sulfotransferases and Prediction of Age-Dependent Fractional Contribution of Sulfation in Acetaminophen Metabolism. Drug Metab. Dispos. 2019, 47, 818–831. [Google Scholar] [CrossRef]
- Miyagi, S.J.; Collier, A.C. The development of UDP-glucuronosyltransferases 1A1 and 1A6 in the pediatric liver. Drug Metab. Dispos. 2011, 39, 912–919. [Google Scholar] [CrossRef] [Green Version]
- Strange, R.; Howie, A.; Hume, R.; Matharoo, B.; Bell, J.; Hiley, C.; Jones, P.; Beckett, G. The developmental expression of alpha-, mu- and pi-class glutathione S-transferases in human liver. Biochim. Biophys. Acta 1989, 993, 186–190. [Google Scholar] [CrossRef]
- Stojanović, V.D.; Barišić, N.A.; Radovanović, T.D.; Kovač, N.B.; Djuran, J.D.; Antić, A.P.E.; Doronjski, A.D. Serum glutathione S-transferase Pi as predictor of the outcome and acute kidney injury in premature newborns. Pediatr. Nephrol. 2018, 33, 1251–1256. [Google Scholar] [CrossRef]
- Rogers, Z.; Hiruy, H.; Pasipanodya, J.G.; Mbowane, C.; Adamson, J.; Ngotho, L.; Karim, F.; Jeena, P.; Bishai, W.; Gumbo, T. The Non-Linear Child: Ontogeny, Isoniazid Concentration, and NAT2 Genotype Modulate Enzyme Reaction Kinetics and Metabolism. EBioMedicine 2016, 11, 118–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thabit, A.K. Antibiotics in the Biliary Tract: A Review of the Pharmacokinetics and Clinical Outcomes of Antibiotics Penetrating the Bile and Gallbladder Wall. Pharmacotherapy 2020, 40, 672–691. [Google Scholar] [CrossRef] [PubMed]
- Johnson, T.N.; Jamei, M.; Rowland-Yeo, K. How Does In Vivo Biliary Elimination of Drugs Change with Age? Evidence from In Vitro and Clinical Data Using a Systems Pharmacology Approach. Drug Metab. Dispos. 2016, 44, 1090–1098. [Google Scholar] [CrossRef] [PubMed]
- Lumbers, E.R.; Kandasamy, Y.; Delforce, S.J.; Boyce, A.C.; Gibson, K.J.; Pringle, K. Programming of Renal Development and Chronic Disease in Adult Life. Front. Physiol. 2020, 11, 757. [Google Scholar] [CrossRef] [PubMed]
- Filler, G.; Bhayana, V.; Schott, C.; de Ferris, M.E.D. How should we assess renal function in neonates and infants? Acta Paediatr. 2021, 110, 773–780. [Google Scholar] [CrossRef]
- Kandasamy, Y.; Rudd, D.; Smith, R.; Lumbers, E.R.; Wright, I. Extra uterine development of preterm kidneys. Pediatr. Nephrol. 2018, 33, 1007–1012. [Google Scholar] [CrossRef] [Green Version]
- Kandasamy, Y.; Rudd, D.; Lumbers, E.R.; Smith, R. An evaluation of preterm kidney size and function over the first two years of life. Pediatr. Nephrol. 2020, 35, 1477–1482. [Google Scholar] [CrossRef]
- Smeets, N.J.; IntHout, J.; van der Burgh, M.J.; Schwartz, G.J.; Schreuder, M.F.; de Wildt, S.N. Maturation of GFR in Term-Born Neonates: An Individual Participant Data Meta-Analysis. J. Am. Soc. Nephrol. 2022, 33, 1277–1292. [Google Scholar] [CrossRef]
- Salem, F.; Johnson, T.N.; Hodgkinson, A.B.J.; Ogungbenro, K.; Rostami-Hodjegan, A. Does “Birth” as an Event Impact Maturation Trajectory of Renal Clearance via Glomerular Filtration? Reexamining Data in Preterm and Full-Term Neonates by Avoiding the Creatinine Bias. J. Clin. Pharmacol. 2021, 61, 159–171. [Google Scholar] [CrossRef]
- Correa, L.P.; Marzano, A.C.S.; Filha, R.S.; Magalhães, R.C.; Simoes-E-Silva, A.C. Biomarkers of renal function in preterm neonates at 72 h and 3 weeks of life. J. Pediatr. 2021, 97, 508–513. [Google Scholar] [CrossRef]
- Iacobelli, S.; Guignard, J.-P. Maturation of glomerular filtration rate in neonates and infants: An overview. Pediatr. Nephrol. 2021, 36, 1439–1446. [Google Scholar] [CrossRef]
- Coleman, C.; Perez, A.T.; Selewski, D.T.; Steflik, H.J. Neonatal Acute Kidney Injury. Front. Pediatr. 2022, 10, 842544. [Google Scholar] [CrossRef]
- Rhone, E.T.; Carmody, J.B.; Swanson, J.R.; Charlton, J.R. Nephrotoxic medication exposure in very low birth weight infants. J. Matern Fetal Neonatal Med. 2014, 27, 1485–1490. [Google Scholar] [CrossRef]
- Jančič, S.G.; Močnik, M.; Varda, N.M. Glomerular Filtration Rate Assessment in Children. Children 2022, 9, 1995. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Kumar, S.S.; Sherwin, C.; Ward, R.; Baer, G.; Burckart, G.J.; Wang, Y.; Yao, L.P. Renal Clearance in Newborns and Infants: Predictive Performance of Population-Based Modeling for Drug Development. Clin. Pharmacol. Ther. 2019, 105, 1462–1470. [Google Scholar] [CrossRef] [PubMed]
- Penicillin, G. DrugBank Online. Available online: https://go.drugbank.com/drugs/DB01053 (accessed on 1 February 2023).
- Padari, H.; Metsvaht, T.; Germovsek, E.; Barker, C.I.; Kipper, K.; Herodes, K.; Standing, J.F.; Oselin, K.; Tasa, T.; Soeorg, H.; et al. Pharmacokinetics of Penicillin G in Preterm and Term Neonates. Antimicrob. Agents Chemother. 2018, 62, e02238-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peechakara, B.V.; Gupta, M. Ampicillin/Sulbactam. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK526117 (accessed on 1 February 2023).
- Le, J.; Greenberg, R.G.; Yoo, Y.; Clark, R.H.; Benjamin, D.K.; Zimmerman, K.O.; Cohen-Wolkowiez, M.; Wade, K.C. Best Pharmaceuticals for Children Act–Pediatric Trials Network Steering Committee Ampicillin dosing in premature infants for early-onset sepsis: Exposure-driven efficacy, safety, and stewardship. J. Perinatol. 2022, 42, 959–964. [Google Scholar] [CrossRef]
- Stępnik, K.E.; Malinowska, I. Determination of binding properties of ampicillin in drug-human serum albumin standard solution using N-vinylpyrrolidone copolymer combined with the micellar systems. Talanta 2017, 162, 241–248. [Google Scholar] [CrossRef]
- Soto, E.; Shoji, S.; Muto, C.; Tomono, Y.; Marshall, S. Population pharmacokinetics of ampicillin and sulbactam in patients with community-acquired pneumonia: Evaluation of the impact of renal impairment. Br. J. Clin. Pharmacol. 2014, 77, 509–521. [Google Scholar] [CrossRef] [Green Version]
- DrugBank Online. Amoxicillin. Available online: https://go.drugbank.com/drugs/DB01060 (accessed on 1 February 2023).
- Pullen, J.; Stolk, L.M.; Nieman, F.H.; Degraeuwe, P.L.; van Tiel, F.H.; Zimmermann, L.J. Population pharmacokinetics and dosing of amoxicillin in (pre)term neonates. Ther. Drug Monit. 2006, 28, 226–231. [Google Scholar] [CrossRef]
- CharlesX, B.G.; Preechagoon, Y.; Lee, T.C.; Steer, P.A.; Flenady, V.J.; Debuse, N. Population pharmacokinetics of intravenous amoxicillin in very low birth weight infants. J. Pharm. Sci. 1997, 86, 1288–1292. [Google Scholar] [CrossRef]
- Landersdorfer, C.; Kirkpatrick, C.; Kinzig-Schippers, M.; Bulitta, J.B.; Holzgrabe, U.; Drusano, G.L.; Sörgel, F. Population pharmacokinetics at two dose levels and pharmacodynamic profiling of flucloxacillin. Antimicrob. Agents Chemother. 2007, 51, 3290–3297. [Google Scholar] [CrossRef] [Green Version]
- Pullen, J.; de Rozario, L.; Stolk, L.M.L.; Degraeuwe, P.L.J.; van Tiel, F.H.; Zimmermann, L.J.I. Population pharmacokinetics and dosing of flucloxacillin in preterm and term neonates. Ther. Drug Monit. 2006, 28, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Anderson, P.; Bluhm, G.; Ehrnebo, M.; Herngren, L.; Jacobson, B. Pharmacokinetics and distribution of flucloxacillin in pacemaker patients. Eur. J. Clin. Pharmacol. 1985, 27, 713–719. [Google Scholar] [CrossRef]
- Oh, K.-H.; Kim, C.; Lee, H.; Lee, H.; Jung, J.Y.; Kim, N.J.; Yu, K.-S.; Shin, K.-H.; Jang, I.-J.; Ahn, C. Pharmacokinetics of intravenous piperacillin administration in patients undergoing on-line hemodiafiltration. Antimicrob. Agents Chemother. 2009, 53, 3266–3268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen-Wolkowiez, M.; Watt, K.M.; Zhou, C.; Bloom, B.T.; Poindexter, B.; Castro, L.; Gao, J.; Capparelli, E.V.; Benjamin, D.K.; Smith, P.B. Developmental pharmacokinetics of piperacillin and tazobactam using plasma and dried blood spots from infants. Antimicrob. Agents Chemother. 2014, 58, 2856–2865. [Google Scholar] [CrossRef] [Green Version]
- Libke, R.D.; Clarke, J.T.; Ralph, E.D.; Luthy, R.P.; Kirby, W.M.M. Ticarcillin vs carbenicillin: Clinical pharmacokinetics. Clin. Pharmacol. Ther. 1975, 17, 441–446. [Google Scholar] [CrossRef]
- Watt, K.M.; Hornik, C.P.; Balevic, S.J.; Mundakel, G.; Cotten, C.M.; Harper, B.; Benjamin, D.K.; Anand, R.; Laughon, M.; Smith, P.B.; et al. Pharmacokinetics of ticarcillin–clavulanate in premature infants. Br. J. Clin. Pharmacol. 2019, 85, 1021–1027. [Google Scholar] [CrossRef]
- De Groot, R.; Hack, B.D.; Weber, A.; Chaffin, D.; Ramsey, B.; Smith, A.L. Pharmacokinetics of ticarcillin in patients with cystic fibrosis: A controlled prospective study. Clin. Pharmacol. Ther. 1990, 47, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.B.; Nicolau, D.P.; Nightingale, C.H.; Quintiliani, R. Pharmacokinetics of cefotaxime in healthy volunteers and patients. Diagn. Microbiol. Infect. Dis. 1995, 22, 49–55. [Google Scholar] [CrossRef]
- Shang, Z.-H.; Wu, Y.-E.; Lv, D.-M.; Zhang, W.; Liu, W.-Q.; Anker, J.V.D.; Xu, Y.; Zhao, W. Optimal dose of cefotaxime in neonates with early-onset sepsis: A developmental pharmacokinetic model-based evaluation. Front. Pharmacol. 2022, 13, 916253. [Google Scholar] [CrossRef]
- Aardema, H.; Bult, W.; Van Hateren, K.; Dieperink, W.; Touw, D.; Alffenaar, J.-W.C.; Zijlstra, J. Continuous versus intermittent infusion of cefotaxime in critically ill patients: A randomized controlled trial comparing plasma concentrations. J. Antimicrob. Chemother. 2020, 75, 441–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pacifici, G.; Marchini, G. Clinical Pharmacology of Cefotaxime in Neonates and Infants: Effects and Pharmacokinetics. Int. J. Pediatr. 2017, 5, 6111–6138. [Google Scholar] [CrossRef]
- Pais, G.M.; Chang, J.; Barreto, E.F.; Stitt, G.; Downes, K.J.; Alshaer, M.H.; Lesnicki, E.; Panchal, V.; Bruzzone, M.; Bumanglag, A.V.; et al. Clinical Pharmacokinetics and Pharmacodynamics of Cefepime. Clin. Pharmacokinet. 2022, 61, 929–953. [Google Scholar] [CrossRef]
- Zhao, Y.; Yao, B.-F.; Kou, C.; Xu, H.-Y.; Tang, B.-H.; Wu, Y.-E.; Hao, G.-X.; Zhang, X.-P.; Zhao, W. Developmental Population Pharmacokinetics and Dosing Optimization of Cefepime in Neonates and Young Infants. Front. Pharmacol. 2020, 11, 14. [Google Scholar] [CrossRef]
- Capparelli, E.; Hochwald, C.; Rasmussen, M.; Parham, A.; Bradley, J.; Moya, F. Population pharmacokinetics of cefepime in the neonate. Antimicrob. Agents Chemother. 2005, 49, 2760–2766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, J.; Sulaiman, Z.; Llorin, R.M.; Hee, K.-H.; Lee, L.S.-U.; Lye, D.C.; Fisher, D.A.; Tam, V.H. Pharmacokinetics of ertapenem in outpatients with complicated urinary tract infections. J. Antimicrob. Chemother. 2014, 69, 2517–2521. [Google Scholar] [CrossRef] [Green Version]
- Pacifici, G.M.; Allegaert, K. Clinical pharmacology of carbapenems in neonates. J. Chemother. 2014, 26, 67–73. [Google Scholar] [CrossRef]
- Mouton, J.W.; Mouton, J.W.; Anker, J.N.V.D. Meropenem clinical pharmacokinetics. Clin. Pharmacokinet. 1995, 28, 275–286. [Google Scholar] [CrossRef]
- Smith, P.B.; Cohen-Wolkowiez, M.; Castro, L.M.; Poindexter, B.; Bidegain, M.; Weitkamp, J.-H.; Schelonka, R.L.; Ward, R.M.; Wade, K.; Valencia, G.; et al. Population pharmacokinetics of meropenem in plasma and cerebrospinal fluid of infants with suspected or complicated intra-abdominal infections. Pediatr. Infect. Dis. J. 2011, 30, 844–849. [Google Scholar] [CrossRef]
- Dao, K.; Fuchs, A.; André, P.; Giannoni, E.; Decosterd, L.A.; Marchetti, O.; Asner, S.A.; Pfister, M.; Widmer, N.; Buclin, T.; et al. Dosing strategies of imipenem in neonates based on pharmacometric modelling and simulation. J. Antimicrob. Chemother. 2022, 77, 457–465. [Google Scholar] [CrossRef]
- DrugBank Online. Imipenem. Available online: https://go.drugbank.com/drugs/DB01598 (accessed on 1 February 2023).
- Paterson, D.L.; DePestel, D.D. Doripenem. Clin. Infect. Dis. 2009, 49, 291–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cirillo, I.; Vaccaro, N.; Castaneda-Ruiz, B.; Redman, R.; Cossey, V.; Bradley, J.S.; Allegaert, K. Open-Label Study to Evaluate the Single-Dose Pharmacokinetics, Safety, and Tolerability of Doripenem in Infants Less than 12 Weeks in Chronological Age. Antimicrob. Agents Chemother. 2015, 59, 4742–4749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DrugBank Online. Azithromycin. Available online: https://go.drugbank.com/drugs/DB00207 (accessed on 1 February 2023).
- Merchan, L.M.; Hassan, H.E.; Terrin, M.L.; Waites, K.B.; Kaufman, D.A.; Ambalavanan, N.; Donohue, P.; Dulkerian, S.J.; Schelonka, R.; Magder, L.S.; et al. Pharmacokinetics, Microbial Response, and Pulmonary Outcomes of Multidose Intravenous Azithromycin in Preterm Infants at Risk for Ureaplasma Respiratory Colonization. Antimicrob. Agents Chemother. 2015, 59, 570–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bandín-Vilar, E.; García-Quintanilla, L.; Castro-Balado, A.; Zarra-Ferro, I.; González-Barcia, M.; Campos-Toimil, M.; Mangas-Sanjuan, V.; Mondelo-García, C.; Fernández-Ferreiro, A. A Review of Population Pharmacokinetic Analyses of Linezolid. Clin. Pharmacokinet. 2022, 61, 789–817. [Google Scholar] [CrossRef]
- Thibault, C.; Kassir, N.; Goyer, I.; Théorêt, Y.; Litalien, C.; Moussa, A.; Ovetchkine, P.; Autmizguine, J. Population Pharmacokinetics of Intravenous Linezolid in Premature Infants. Pediatr. Infect. Dis. J. 2019, 38, 82–88. [Google Scholar] [CrossRef]
- Jungbluth, G.L.; Welshman, I.R.; Hopkins, N.K. Linezolid pharmacokinetics in pediatric patients: An overview. Pediatr. Infect. Dis. J. 2003, 22 (Suppl. S9), S153–S157. [Google Scholar] [CrossRef] [PubMed]
- Xie, F.; Mantzarlis, K.; Malliotakis, P.; Koulouras, V.; DeGroote, S.; Koulenti, D.; Blot, S.; Boussery, K.; Van Bocxlaer, J.; Colin, P. Pharmacokinetic evaluation of linezolid administered intravenously in obese patients with pneumonia. J. Antimicrob. Chemother. 2019, 74, 667–674. [Google Scholar] [CrossRef] [PubMed]
- Gostelow, M.; Gonzalez, D.; Smith, P.B.; Cohen-Wolkowiez, M. Pharmacokinetics and safety of recently approved drugs used to treat methicillin-resistant Staphylococcus aureus infections in infants, children and adults. Expert Rev. Clin. Pharmacol. 2014, 7, 327–340. [Google Scholar] [CrossRef] [Green Version]
- Estes, K.S.; Derendorf, H. Comparison of the pharmacokinetic properties of vancomycin, linezolid, tigecyclin, and daptomycin. Eur. J. Med. Res. 2010, 15, 533–543. [Google Scholar] [CrossRef]
- Cohen-Wolkowiez, M.; Watt, K.M.; Hornik, C.P.; Benjamin, D.K.; Smith, P.B. Pharmacokinetics and tolerability of single-dose daptomycin in young infants. Pediatr. Infect. Dis. J. 2012, 31, 935–937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stass, H.; Lettieri, J.; Vanevski, K.M.; Willmann, S.; James, L.P.; Sullivan, J.E.; Arrieta, A.C.; Bradley, J.S. Pharmacokinetics, Safety, and Tolerability of Single-Dose Intravenous Moxifloxacin in Pediatric Patients: Dose Optimization in a Phase 1 Study. J. Clin. Pharmacol. 2019, 59, 654–667. [Google Scholar] [CrossRef]
- Yeung, T.; Chung, E.; Chen, J.; Erdman, L.K.; Smiljkovic, M.; Wong, W.; Rolnitsky, A.; Morris, S.K.; El Shahed, A.; Banihani, R.; et al. Therapeutic Drug Monitoring of Moxifloxacin to Guide Treatment of Mycoplasma hominis Meningitis in an Extremely Preterm Infant. J. Pediatr. Pharmacol. Ther. 2021, 26, 857–862. [Google Scholar] [CrossRef] [PubMed]
- DrugBank Online. Amikacin. Available online: https://go.drugbank.com/drugs/DB00479 (accessed on 1 February 2023).
- An, S.H.; Kim, J.Y.; Gwak, H.S. Outcomes of a new dosage regimen of amikacin based on pharmacokinetic parameters of Korean neonates. Am. J. Health Syst. Pharm. 2014, 71, 122–127. [Google Scholar] [CrossRef]
- Gonzalez, D.; Melloni, C.; Yogev, R.; Poindexter, B.B.; Mendley, S.R.; Delmore, P.; Sullivan, J.E.; Autmizguine, J.; Lewandowski, A.; Harper, B.; et al. Use of opportunistic clinical data and a population pharmacokinetic model to support dosing of clindamycin for premature infants to adolescents. Clin. Pharmacol. Ther. 2014, 96, 429–437. [Google Scholar] [CrossRef] [Green Version]
- Rowland, M. Clinical Pharmacokinetics of Teicoplanin. Clin. Pharmacokinet. 1990, 18, 184–209. [Google Scholar] [CrossRef] [PubMed]
- Kontou, A.; Sarafidis, K.; Begou, O.; Gika, H.G.; Tsiligiannis, A.; Ogungbenro, K.; Dokoumetzidis, A.; Agakidou, E.; Roilides, E. Population Pharmacokinetics of Teicoplanin in Preterm and Term Neonates: Is It Time for a New Dosing Regimen? Antimicrob. Agents Chemother. 2020, 64, e01971-19. [Google Scholar] [CrossRef] [PubMed]
- Zaric, R.Z.; Milovanovic, J.; Rosic, N.; Milovanovic, D.; Zecevic, D.R.; Folic, M.; Jankovic, S. Pharmacokinetics of Vancomycin in Patients with Different Renal Function Levels. Open Med. 2018, 13, 512–519. [Google Scholar] [CrossRef]
- Mulubwa, M.; Griesel, H.A.; Mugabo, P.; Dippenaar, R.; Van Wyk, L. Assessment of Vancomycin Pharmacokinetics and Dose Regimen Optimisation in Preterm Neonates. Drugs R D 2020, 20, 105–113. [Google Scholar] [CrossRef] [Green Version]
- Leroux, S.; Anker, J.N.V.D.; Smits, A.; Pfister, M.; Allegaert, K. Maturational changes in vancomycin protein binding affect vancomycin dosing in neonates. Br. J. Clin. Pharmacol. 2019, 85, 865–867. [Google Scholar] [CrossRef]
- Leroux, S.; Jacqz-Aigrain, E.; Biran, V.; Lopez, E.; Madeleneau, D.; Wallon, C.; Zana-Taïeb, E.; Virlouvet, A.-L.; Rioualen, S.; Zhao, W. Clinical Utility and Safety of a Model-Based Patient-Tailored Dose of Vancomycin in Neonates. Antimicrob. Agents Chemother. 2016, 60, 2039–2042. [Google Scholar] [CrossRef] [Green Version]
- Pullen, J.; Stolk, L.M.L.; Degraeuwe, P.L.J.; van Tiel, F.H.; Neef, C.; Zimmermann, L.J.I. Pharmacokinetics of intravenous rifampicin (rifampin) in neonates. Ther. Drug Monit. 2006, 28, 654–661. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Wolkowiez, M.; Ouellet, D.; Smith, P.B.; James, L.P.; Ross, A.; Sullivan, J.E.; Walsh, M.C.; Zadell, A.; Newman, N.; White, N.R.; et al. Population Pharmacokinetics of Metronidazole Evaluated Using Scavenged Samples from Preterm Infants. Antimicrob. Agents Chemother. 2012, 56, 1828–1837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DrugBank Online. Metronidazole. Available online: https://go.drugbank.com/drugs/DB00916 (accessed on 4 March 2023).
- Li, S.; Xie, F. Foetal and neonatal exposure prediction and dosing evaluation for ampicillin using a physiologically-based pharmacokinetic modelling approach. Br. J. Clin. Pharmacol. 2022, 89, 1402–1412. [Google Scholar] [CrossRef] [PubMed]
- Padari, H.; Soeorg, H.; Tasa, T.; Metsvaht, T.; Kipper, K.; Herodes, K.; Oselin, K.; Hallik, M.; Ilmoja, M.-L.; Lutsar, I. Ampicillin Pharmacokinetics During First Week of Life in Preterm and Term Neonates. Pediatr. Infect. Dis. J. 2021, 40, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.-E.; Wang, T.; Yang, H.-L.; Tang, B.-H.; Kong, L.; Li, X.; Gao, Q.; Li, X.; Yao, B.-F.; Shi, H.-Y.; et al. Population pharmacokinetics and dosing optimization of azlocillin in neonates with early-onset sepsis: A real-world study. J. Antimicrob. Chemother. 2021, 76, 699–709. [Google Scholar] [CrossRef] [PubMed]
- Bijleveld, Y.; Mathôt, R.; van der Lee, J.; Groenendaal, F.; Dijk, P.; van Heijst, A.; Simons, S.; Dijkman, K.; van Straaten, H.; Rijken, M.; et al. Population Pharmacokinetics of Amoxicillin in Term Neonates Undergoing Moderate Hypothermia. Clin. Pharmacol. Ther. 2018, 103, 458–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quinton, M.-C.; Bodeau, S.; Kontar, L.; Zerbib, Y.; Maizel, J.; Slama, M.; Masmoudi, K.; Lemaire-Hurtel, A.-S.; Bennis, Y. Neurotoxic Concentration of Piperacillin during Continuous Infusion in Critically Ill Patients. Antimicrob. Agents Chemother. 2017, 61, e00654-17. [Google Scholar] [CrossRef] [Green Version]
- Bradley, J.S.; Stone, G.G.; Chan, P.L.S.; Raber, S.R.; Riccobene, T.; Casullo, V.M.; Yan, J.L.; Hendrick, V.M.; Hammond, J.; Leister-Tebbe, H.K. Phase 2 Study of the Safety, Pharmacokinetics and Efficacy of Ceftaroline Fosamil in Neonates and Very Young Infants with Late-onset Sepsis. Pediatr. Infect. Dis. J. 2020, 39, 411–418. [Google Scholar] [CrossRef]
- Shi, Z.-R.; Chen, X.-K.; Tian, L.-Y.; Wang, Y.-K.; Zhang, G.-Y.; Dong, L.; Jirasomprasert, T.; Jacqz-Aigrain, E.; Zhao, W. Population Pharmacokinetics and Dosing Optimization of Ceftazidime in Infants. Antimicrob. Agents Chemother. 2018, 62, e02486-17. [Google Scholar] [CrossRef] [Green Version]
- Leroux, S.; Roué, J.-M.; Gouyon, J.-B.; Biran, V.; Zheng, H.; Zhao, W.; Jacqz-Aigrain, E. A Population and Developmental Pharmacokinetic Analysis to Evaluate and Optimize Cefotaxime Dosing Regimen in Neonates and Young Infants. Antimicrob. Agents Chemother. 2016, 60, 6626–6634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Cock, R.F.W.; Smits, A.; Allegaert, K.; De Hoon, J.; Saegeman, V.; Danhof, M.; Knibbe, C.A.J. Population pharmacokinetic modelling of total and unbound cefazolin plasma concentrations as a guide for dosing in preterm and term neonates. J. Antimicrob. Chemother. 2014, 69, 1330–1338. [Google Scholar] [CrossRef] [Green Version]
- Ganguly, S.; Edginton, A.N.; Gerhart, J.G.; Cohen-Wolkowiez, M.; Greenberg, R.G.; Gonzalez, D. Best Pharmaceuticals for Children Act-Pediatric Trials Network Steering Committee. Physiologically Based Pharmacokinetic Modeling of Meropenem in Preterm and Term Infants. Clin. Pharmacokinet. 2021, 60, 1591–1604. [Google Scholar] [CrossRef] [PubMed]
- Steffens, N.A.; Zimmermann, E.S.; Nichelle, S.M.; Brucker, N. Meropenem use and therapeutic drug monitoring in clinical practice: A literature review. J. Clin. Pharm. Ther. 2021, 46, 610–621. [Google Scholar] [CrossRef] [PubMed]
- Mohzari, Y.; Aljobair, F.; Alrashed, A.; Asdaq, S.; Alshuraim, R.; Asfour, S.; Al-Mouqdad, M.; Bamogaddam, R.; Al-Anazi, D.; Zeilinger, C.; et al. Safety and Efficacy of Daptomycin in Neonates with Coagulase-Negative Staphylococci: Case Series Analysis. Antibiotics 2021, 10, 168. [Google Scholar] [CrossRef]
- Newby, B.D.; Timberlake, K.E.; Lepp, L.M.; Mihic, T.; Dersch-Mills, D.A. Levofloxacin Use in the Neonate: A Case Series. J. Pediatr. Pharmacol. Ther. 2017, 22, 304–313. [Google Scholar] [CrossRef] [Green Version]
- Smits, A.; De Cock, R.F.W.; Allegaert, K.; Vanhaesebrouck, S.; Danhof, M.; Knibbe, C.A.J. Prospective Evaluation of a Model-Based Dosing Regimen for Amikacin in Preterm and Term Neonates in Clinical Practice. Antimicrob. Agents Chemother. 2015, 59, 6344–6351. [Google Scholar] [CrossRef] [Green Version]
- Low, B.Y.S.; Tan, M.S.L.; Wan, M.A.S. Extended-Interval gentamicin dosing in achieving therapeutic concentrations in malaysian neonates. J. Pediatr. Pharmacol. Ther. 2015, 20, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Neeli, H.; Hanna, N.; Abduljalil, K.; Cusumano, J.; Taft, D.R. Application of Physiologically Based Pharmacokinetic-Pharmacodynamic Modeling in Preterm Neonates to Guide Gentamicin Dosing Decisions and Predict Antibacterial Effect. J. Clin. Pharmacol. 2021, 61, 1356–1365. [Google Scholar] [CrossRef] [PubMed]
- Valitalo, P.A.J.; Anker, J.N.V.D.; Allegaert, K.; de Cock, R.F.W.; de Hoog, M.; Simons, S.H.P.; Mouton, J.W.; Knibbe, C.A.J. Novel model-based dosing guidelines for gentamicin and tobramycin in preterm and term neonates. J. Antimicrob. Chemother. 2015, 70, 2074–2077. [Google Scholar] [CrossRef] [Green Version]
- Jacqz-Aigrain, E.; Leroux, S.; Thomson, A.H.; Allegaert, K.; Capparelli, E.V.; Biran, V.; Simon, N.; Meibohm, B.; Lo, L.; Marques, R.; et al. Population pharmacokinetic meta-analysis of individual data to design the first randomized efficacy trial of vancomycin in neonates and young infants. J. Antimicrob. Chemother. 2019, 74, 2128–2138. [Google Scholar] [CrossRef] [PubMed]
- Janssen, E.J.H.; Välitalo, P.A.J.; Allegaert, K.; de Cock, R.F.W.; Simons, S.H.P.; Sherwin, C.M.T.; Mouton, J.W.; Anker, J.N.V.D.; Knibbe, C.A.J. Towards Rational Dosing Algorithms for Vancomycin in Neonates and Infants Based on Population Pharmacokinetic Modeling. Antimicrob. Agents Chemother. 2015, 60, 1013–1021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Traunmüller, F.; Popovic, M.; Konz, K.-H.; Joukhadar, C.; Vavken, P.; Leithner, A.; Joukhadar, C. A Reappraisal of Current Dosing Strategies for Intravenous Fosfomycin in Children and Neonates. Clin. Pharmacokinet. 2011, 50, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Wolkowiez, M.; Sampson, M.; Bloom, B.T.; Arrieta, A.; Wynn, J.; Martz, K.; Harper, B.; Kearns, G.L.; Capparelli, E.V.; Siegel, D.; et al. Determining population and developmental pharmacokinetics of metronidazole using plasma and dried blood spot samples from premature infants. Pediatr. Infect. Dis. J. 2013, 32, 956–961. [Google Scholar] [CrossRef] [Green Version]
- Procianoy, R.S.; Silveira, R.D.C. The challenges of neonatal sepsis management. J. Pediatr. Rio J. 2019, 96 (Suppl. S1), 80–86. [Google Scholar] [CrossRef]
- Zyryanov, S.K.; Ushkalova, E.A.; Kondratyeva, E.I.; Butranova, O.I.; Kondakova, Y.A. Gene Polymorphism of Biotransformation Enzymes and Ciprofloxacin Pharmacokinetics in Pediatric Patients with Cystic Fibrosis. Biomedicines 2022, 10, 1050. [Google Scholar] [CrossRef]
- Yalçın, N.; Flint, R.B.; van Schaik, R.H.; Simons, S.H.; Allegaert, K. The Impact of Pharmacogenetics on Pharmacokinetics and Pharmacodynamics in Neonates and Infants: A Systematic Review. Pharm. Pers. Med. 2022, 15, 675–696. [Google Scholar] [CrossRef]



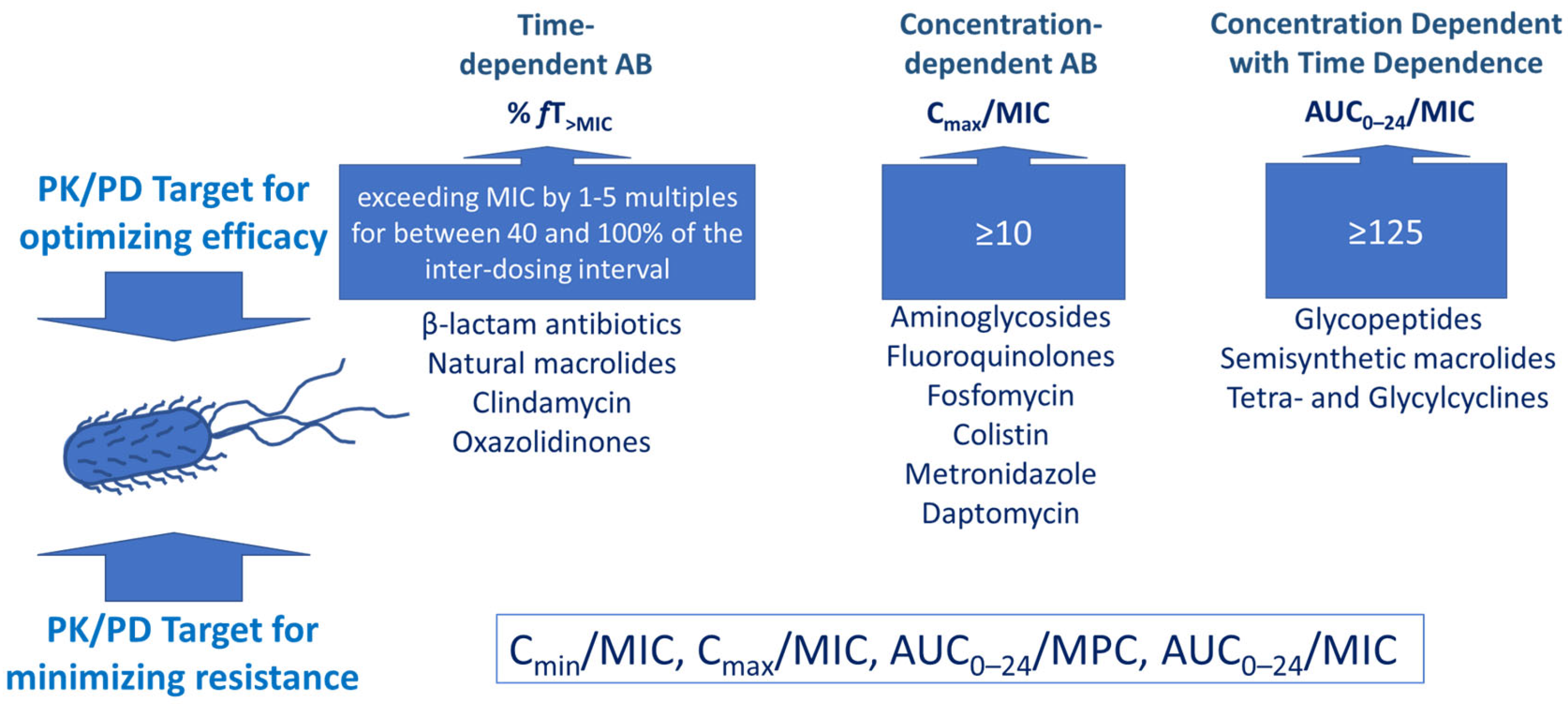{kind=link}
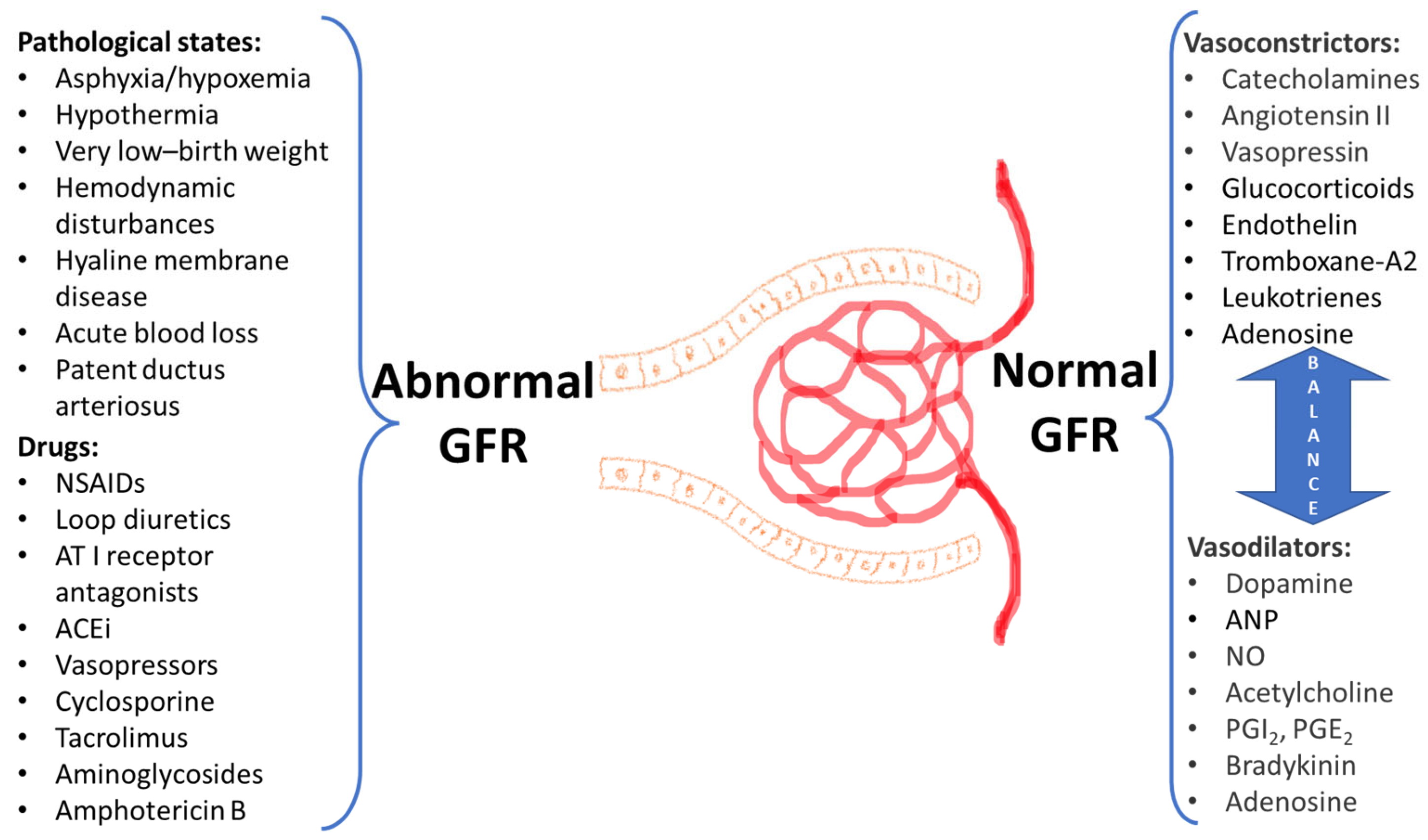{kind=link}
| Transport Protein | Time of Expression in Different Cells | Age-Dependent Change of Expression | Transported Antibiotics |
|---|---|---|---|
| BCRP | Intestinal epithelium—from 5.5 to 28 weeks of gestation. Hepatocytes—from 10 to 11 weeks [45] | Similar levels in preterm newborns, full-terms, and adults [43,46] | Delafloxacin, ciprofloxacin, enrofloxacin, nitrofurantoin, norfloxacin, ofloxacin [47,48] |
| P-gp | Enterocytes—from the 12 weeks of gestation [45] | Expression in fetus is lower than in adult samples [43] | Erythromycin, tetracycline [49] Azithromycin [50] Levofloxacin, sparfloxacin [51] Dicloxacillin [52,53] |
| MRP2 | Appears in the liver of 14-week-old fetuses, strong expression at 19 weeks [54] | Lower protein expression in fetuses and term newborns than in adults [43] MRP2 mRNA was 30-fold lower in fetal, 200-fold lower in neonatal, and 100-fold lower in infant liver compared to adults [55] | Ampicillin, azithromycin, and ceftriaxone, cefodizime, ceftriaxone [44,56] |
| OATP1A2 | - | - | Levofloxacin [49] Ciprofloxacin, enoxacin, gatifloxacin, levofloxacin, lomefloxacin, norfloxacin [57] Erythromycin [58] Tebipenem [59] |
| OATP1B1 | - | High expression in the fetus and low expression in the term newborns, with stable protein levels further on [43] OATP1B1 expression was 20-fold lower in fetal, 500-fold lower in neonatal, and 90-fold lower in infant liver compared to adults [55] | Benzylpenicillin, rifampicin, rifampin, rifampicin [49] Cefazolin, cefditoren, cefoperazone, nafcillin [60] |
| OATP1B3 | - | OATP1B3 mRNA was 30-fold lower in fetal, 600-fold lower in neonatal, and 100-fold lower in infant liver compared to adults [55] OATP1B3 exhibited high expression at birth, decline over the first months of life, and then increase in the preadolescent period [61]. | Rifampicin, rifampin [49] Cefadroxil, cefazolin, cefditoren, cefmetazole, cefoperazone, cephalexin, nafcillin [60] Erythromycin [58] |
| OATP2B1 | - | Similar levels in samples from all age groups [43] Intestinal OATP2B1 expression in neonates was significantly higher than in adults [55] | Benzylpenicillin [62] Tebipenem pivoxil [63] |
| PEPT1 | Enterocytes—from 24.7 to 40th week of gestation (comparable level with full-terms) [43] | The PEPT1 mRNA expression of the neonates/infants was only lightly lower (0.8-fold) than the older children (p < 0.05) [55] | Cefadroxil, ceftibuten, cefixime, cephradine, cephalexin [60] |
| Parameter | Age-Associated Change | Effect on Absorption and Bioavailability |
|---|---|---|
| pH | Value close to neutral at birth was described in some studies with rapid change to acidic values | High gastric pH may provide positive effect on the oral bioavailability of acid-labile drugs (e.g., ampicillin, amoxicillin, penicillin, nafcillin, erythromycin), it favors the ionization, and reduces the absorption of weak acids and may negatively affect absorption of weak bases by decreasing their solubility [64] |
| Gastric volume | Decreased | Solubility of some drugs can be decreased |
| Gastric emptying and intestinal transit | Some slowing is specific, intestinal transit in preterm newborns is 4 times longer than in adults [37] | Delay and decrease in absorption |
| Biliary function | Decreased compared with older children and adults [31] | Possible decrease in the intestinal absorption of lipid-soluble drugs |
| Pancreatic enzymes | Decrease at birth with further rise through the first year of life | Decreased intra-duodenal hydrolysis may result in incomplete absorption |
| Intestinal surface area | Reduced surface-to-volume ratio in children when compared with adults [64] | Reduced absorptive surface may influence absorption of some drugs |
| Intestinal permeability | In preterm infants (26–36 weeks gestation), intestinal permeability is higher than in healthy term infants only if measured within two days of birth [65] | Increase in absorption may by for drugs with paracellular route of absorption [66] |
| Transport proteins | Decreased p-gp, MRP1, MRP2—decreased efflux function | Possible increase in absorption of corresponding substrates |
| Light decrease in PEPT1 | Possible decrease in absorption of corresponding substrates | |
| Intestinal wall drug-metabolizing enzymes | Possible decrease in cytochrome P450 isoenzime 3A4 (CYP3A4) in neonates at birth with further rise through childhood period [67] | Possible increase in absorption and bioavailability of CYP3A4 substrates |
| Drug (Oral Administration) | Food Effect on PK Parameters in Pediatric Population | Food Effect on PK Parameters in Adults |
|---|---|---|
| Penicillin V (phenoxymethylpenicillin) | Cmax decreased | Penicillin V (phenoxymethylpenicillin) |
| Amoxicillin | Cmax decreased at lower doses, unchanged at higher doses AUC unchanged at all doses | No effect |
| Ampicillin | Cmax unchanged AUC unchanged | Some studies suggest reduction in Cmax and AUC with food |
| Cefpodoxime proxetil | Tmax prolonged Cmax unchanged | Cmax and AUC increase with any meal intake |
| Cephalexin | Cmax lightly decreased AUC lightly increased | Delay in absorption AUC unchanged |
| Cefaclor | Cmax decreased | Tmax prolonged Cmax decreased |
| Cefadroxil | Cmax decreased | No effect |
| Cephradine | Cmax decreased | No effect |
| Cefixime | No clinically significant changes in Cmax and AUC | Tmax prolonged Cmax and AUC unchanged |
| Clarithromycin | Cmax unchanged AUC unchanged | Cmax unchanged AUC unchanged |
| Routes of Administration | Main Physiological Factors Affecting PK Parameters in Neonates | Change of Absorption |
|---|---|---|
| Intramuscular | Blood flow to muscle: variable decrease over the first 2–3 weeks of life. The ratio of muscle mass to body mass: less in neonates than in adults Water content: higher proportion of water in neonates [118] | Possible variability in absorption, though for many antibiotics it nearly reaches adult values. Hydrophilic drugs may have greater intramuscular absorption in neonates than children or adults due to high water content in muscles |
| Rectal | pH: decreased in neonates compared with older infants (mean pH 6.47 vs. 6.90) [119] and with adults (pH 7.2–7.4) [120] | Nearly no change in absorption of drugs (absorbable drugs should have pKa values near or above the physiological range) |
| Percutaneous | Skin thickness and keratinization: reduced Hydration of the stratum corneum: increased Surface area to bodyweight ratio: higher than in adults [38,121] | Increased absorption of drugs including some topical antibiotics with risk of overexposure, and potential toxic effects |
| Inhalation Intranasal | Stage of lung development: late preterm neonates (28–34 weeks of gestation) may have saccular stage of lung development, more preterm infants—just the stage of development of bronchioles and alveolar epithelium, both with surfactant deficiency and high risks for respiratory distress syndrome [122] Permeability of the mucosa of the nasal cavity: Increased in neonates [121] | Reduced absorption from the lower respiratory department and increased absorption from the upper respiratory department including nasal cavity (e.g., with facemask for inhalation) |
| Antibiotic | CNS | Lungs | Gallbladder, Bile | Urinary Tract | Bones and Joints |
|---|---|---|---|---|---|
| Fosfomycin | +++ | ++ | ++ | +++ | ++ |
| Lincosamides | + High doses may result in therapeutic concentrations achievement | ++ | ++ | +/++ | ++/+++ |
| Rifamycins | +++ | +++ | + (?) | +/++ | ++/+++ |
| Fluoroquinolones | ++/+++ Minimum values for ciprofloxacin, higher value for respiratory fluoroquinolones | +++ High in alveolar cells, inflammation may decrease penetration | +/++ Higher for levofloxacin, ofloxacin, ciprofloxacin | ++/+++ | +++ |
| Macrolides | + Rapid removement by P-gp of BBB | +++ Higher values in the lung parenchyma, less in epithelial lining fluid | −/+ | −/+ | ++ |
| Aminoglycosides | + Penetration may be increased in preterm infants with increased risks of aminoglycoside-dependent ototoxicity | ++ Only in epithelial lining fluid and bronchial mucus, no cellular entry | −/+ | +++ | ++ |
| Glycopeptides | ? Variable data, not predicting clinical outcome, penetration may increase in neonates with meningitis | +++ | ++/+++ | +++ | ++/+++ |
| Lipoglycopeptides | + Poor penetration | +++ | + (?) | ++/+++ | +++ |
| Cephalosporines | ++/+++ Especially high for ceftriaxone, cefotaxime, ceftazidime, cefixime and cefepime Low—for cefuroxime. Meningeal inflammation increases penetration | +++ High concentrations in the lung parenchyma, epithelial lining fluid and bronchial mucus | ++/+++ The highest value is for cefoperazone, cefotetan, minimum—for cefotaxime | +++ | ++/+++ |
| Penicillins | + Negligible with non-inflamed BBB and increased in meningitis. Dose increase is needed in CNS infections | ++/+++ High in the epithelial lining fluid and bronchial mucus | ++/+++ The highest value is for piperacillin/tazobactam | +++ High concentrations in urine | −/+ Undetectable, exception for flucloxacillin, piperacillin tazobactam, amoxicillin clavulanat |
| Carbapenems | +++ Imipenem reaches higher CSF concentrations, but causes seizures in neonates, especially preterms, thus meropenem is preferred | ++/+++ | + Despite low bile concentrations, some studies demonstrated clinical efficacy of imipenem and meropenem) | +++ Imipenem: adding cilastatin prevents degradation with dehydropeptidase-I in kidneys | ++/+++ |
| Oxazolidinones | ++ Penetration in CNS tissues and CSF, brain concentration of linezolid is higher than for tedizolid | +++ Concentrations in epithelial lining fluid > serum > alveolar macrophages) | ++ (?) | ++ | +++ |
| Moderate to Strong Displacing Effect | Minimal Displacing Effect | No Displacing Effect |
|---|---|---|
| Sulfamethoxazole Sulfisoxazole Sulfadiazine Ceftriaxone Cefotetan Moxalactam Dicloxacillin Carbenicillin Cefazolin | Nafcillin Ampicillin Oxacillin Methicillin Cefotaxime | Aminoglycosides |
| CYP450 Isoenzyme | Antibiotic-Substrate | Comment on Ontogeny |
|---|---|---|
| CYP1A1 | Linezolid [186] | Absent-to-low expression in the neonate; activity reaches 50% of adult values by 1 year of age [193] |
| CYP1A2 | - | Becomes active at 1 to 3 months [194] The median expression was significantly greater after 15 months postnatal age (n = 55) than in fetal and younger postnatal samples [195] |
| CYP2A6 | - | Low activity during fetal age (<1% of adult values) with increase up to 50% adult activity values at neonatal age. Activity and protein expression reach adult values between 1 and 15 years of age [196] |
| CYP1B1 | Linezolid [186] | Appears in the early stages in ontogenesis [197] |
| CYP2B6 | - | 2-fold increase in expression and activity in the first month of life, it is suggested that there are no additional changes between 1 month and 18 years or a 7-fold increase between 1 year and adulthood [198] |
| CYP2C8 | Linezolid [186] | The median expression was significantly greater among samples from subjects older than 35 postnatal days (n = 122) compared with fetal samples and very young infants (fetal to 35 days postnatal, n = 100) [195] |
| CYP2C9 | - | Expression at 1 to 2% of mature values during the first trimester, with progressive increases during the second and third trimesters to levels approximately 30% of adults. From birth to 5 months values varied 35-fold and were significantly higher than those observed during the late fetal period, with 51% of samples exhibiting values commensurate with mature levels. Less variability was observed between 5 months and 18 years [199] |
| CYP2C19 | - | Expression did not change at birth, increased linearly over the first 5 postnatal months, and varied 21-fold from 5 months to 10 years [199] |
| CYP2D6 | Linezolid [186] | Hepatic expression in neonates <7 days was higher than in first and second trimesters, but close to the values of third trimester. Expression in neonates >7 days was higher than in earlier ages [200] Adult activity is achieved by 3–5 years of age [193] |
| CYP2E1 | - | Lower value in neonatal samples compared with infants 31 to 90 days of age, increased with age. Median (range) values of microsomal protein for older infants, children, and young adults were 8.8 (0–70); 23.8 (10–43); 41.4 (18–95) pmol/mg, respectively [201] |
| CYP3A4 | Erythromycin [156] Linezolid [186] Clindamycin [202] | Activity is extremely low in the fetus; it begins to increase after birth reaching 30–40% of the adult value after one month, 50% at 6–12 months, and 100% at age 1–5 years [203] Protein expression was 200-fold lower in the fetal tissues compared to either the pediatric or adult tissues [191] |
| CYP3A5 | Linezolid [186] Clindamycin [111] | Protein expression is relatively stable (0.001–0.005 nmol/mg) in fetal, pediatric, and adult samples [191] |
| CYP3A7 | Clarithromycin [204] | Highly active in fetuses with a subsequent decrease in activity after first week of life, reaching minimal levels in adults [204] Protein expression was 10-fold higher in the fetal tissues compared to either the pediatric or adult tissues [191] |
| CYP450 Isoenzyme | Antibiotics-Inhibitors | Antibiotics-Inducers |
|---|---|---|
| CYP1A2 | Ciprofloxacin [207] Caderofloxacin, antofloxacin, moxifloxacin, gatifloxacin * [208]. Oritavancin * [214] | - |
| CYP2B6 | Oritavancin * [214] | Rifampicin [215] |
| CYP2C8 | Piperacillin [211] | Rifampicin [215] Trimethoprim [216,217] |
| CYP2C9 | Oritavancin * [214]. | Rifampicin [215] Sulfamethoxazole [216] Dicloxacillin [53] Levofloxacin [208] |
| CYP2C19 | Oritavancin * [214] Meropenem [213] | Rifampicin [215] Dicloxacillin [53] |
| CYP2D6 | Oritavancin * [214] | Oritavancin [214] |
| CYP3A4 | Erythromycin, roxithromycin, clarithromycin, troleandomycin, telithromycin, josamycin [205] Oritavancin * [214] Meropenem [213] | Flucloxacillin [212] Dicloxacillin [53] Rifampin (inducer of CYP 3A4) [206,215] Oritavancin * [214] |
| CYP3A5 | Erythromycin, clarithromycin [205] | - |
| CYP3A7 | Erythromycin [218] | Rifampicin, troleandomycin, erythromycin (upregulation of expression) [218,219] |
| Drug | Vd | PPB Rate | CL | T1/2 | ||||
|---|---|---|---|---|---|---|---|---|
| Adults | Neonates | Adults | Neonates | Adults | Neonates | Adults | Neonates | |
| Penicillin Group | ||||||||
| Penicillin G | 0.53–0.67 L/kg [244] | Extremely preterm neonates comparable with full-terms, mean value 0.50 L/kg, [245] | 45–68% [244] | 60% [245] | 560mL/min [244] | Median—0.21 L/h (interquartile range, 0.16 to 0.29 L/kg) [245] | 0.4–0.9 h [244] | Median—3.6 h (interquartile range, 3.2 to 4.3 h) [245] |
| Ampicillin and Ampicillin sulbactam | 14.2 to 15.1 L [246] | GA 22–24 weeks: 0.25 L/kg; GA 25–27 weeks: 0.34 L/kg [247] | 20% [248] | Some decrease is proposed [247] | 10.7 L/h [249] | GA 22–24 weeks: 0.023 L/h/kg; GA 22–24 weeks: 0.036 L/h/kg [247] | 1 h [246] | GA 22–24 weeks: 7.6 [6.4–9.0] h; GA 25–27 weeks: 6.6 [5.6–7.9] h [247] |
| Amoxicillin | 27.7 L [250] | GA 25 to 42 weeks: 0.65 L/kg [251]; | <20% [252] | Less than in adults [252] | 21.3 L/h [250] | 0.096 ± 0.036 L/kg−1 h−1 [251] | ~1 h [250] | 5.2 ± 1.9 h [251] |
| Flucloxacillin | About 10 L [253] | GA 26 to 42 weeks: 0.54 ± 0.17 L/kg [254] | 95–96% [124] | GA 25 to 41 weeks: 86.3% [139] | 93.1 mL/min [255] | GA 26 to 42 weeks: 0.18 L/kg/h [254] | 0.88 h [255] | 2.6 ± 1.6 hours [254] |
| Piperacillin | 0.27 ± 0.13 L/kg [256] | PNA < 14 weeks: 0.42 L/kg [257] | 20–30% [256] | Median GA of 30 weeks: 30% [257] | 0.183 L/h/kg [258] | Median GA of 30 weeks: median value of 0.085 L/h/kg [257] | 1.1 ± 0.6 h [256] | 3.5 (1.7–8.9) h [257] |
| Ticarcillin | 15.7 L [258] | Preterms > 30 weeks of gestation: 0.26–0.34 L/kg Fullterms: 0.22–0.23 L/kg Total population 0.48 L/kg [259] | 45–65% [258,260] | Less than 45% [259] | 46.2 ± 10.9 mL/min/m2 [260] | PNA < 14 days: 0.078 L/kg/h; PNA ≥ 4–45 days: 0.078 L/kg/h [259] | 1.23 h [258] | PNA < 14 days: 24.3 (11.2–35.7) h; PNA = 14 days: 15.1 (5.0–44.8) h [259] |
| Cephalosporins | ||||||||
| Cefotaxime | 33.3 L/1.73 m2 [261] | GA 30 to 40.1 weeks: median value of 0.36 L/kg [262] | Median value of 29.45–29.86% in critically ill adults against 27–38% in healthy volunteers [261,263] | GA 30 to 40.1 weeks: median value of 40% [262] | 138.4 mL/min [261] | 0.04 (0.02–0.09) L/h/kg [262] | 1.1 hours [261] | GA < 32 weeks, PNA < 7 days: 3.49 ± 0.45 h, PNA ≥ 7 days: 3.72 ± 0.85 h; GA 32–63 weeks, PNA < 7 days: 3.28 ± 0.35 h, PNA ≥ 7 days: 2.0 ± 0.24 h; GA ≥ 37 weeks, PNA < 7 days: 2.77 ± 0.49 h, PNA ≥ 7 days: 2.01 ± 0.57 h [264] |
| Cefepime | 0.2 L/kg [265] | Mean GA 38.1 weeks: median value of 0.62 L/kg [266] | 20% [265] | Mean GA 38.1 weeks: ≤20% [266] | 7.2 ± 0.48 L/h [265] | 0.18 (0.13–0.24) L/h/kg [266] | 2–2.3 h [265] | 4.9 ± 2.1 h [267] |
| Carbapenems | ||||||||
| Ertapenem | 0.7 L [268] | 0.4–0.6 L/kg [269] | 92–95% [146] | Some decrease is proposed | 0.7 L/h [268] | 0.05–0.25 L/h/kg [269] | 6.1 h [268] | NA |
| Meropenem | 21 L [270] | GA 23–41 weeks: 0.4 L/kg [271] | 2% [271] | NA | 27.6–36.3 mL/min [146] | GA 23–41 weeks: 0.104 L/h/kg [271] 0.093–0.238 L/h/kg [269] | 1 h [270] | PNA 5–44 days: 1.3–5.4 h [269] |
| Imipenem | 0.22 L/kg [272] | GA 24–41 weeks: 0.73 L [272] | 20% [272] | <20% [272] | 0.2 L/h/kg [273] | 0.21 L/h [272] | 1–3 h [272] | 1.9 h in term neonates, 2.4 h in preterm neonates [272] |
| Doripenem | 16.8 L (8.09–55.5) [274] | GA <32 weeks: ~0.56 L/kg Infants: ~0.55 L/kg [275] | 8% [274] | NA | 16.0 L/h [274] | PNA < 4 weeks: 2.03 mL/min/kg; PNA > 4 weeks: 3.03 mL/min/kg [275] | 1 h [274] | 2.98 h [275] |
| Macrolides | ||||||||
| Azithromycin | 31.1 L/kg [276] | GA 24–28 weeks: 1.88 L/kg [277] | 30% [158] | NA [158] | 37.8 L/h [276] | 0.15 L/h/kg0.75 [277] | 68 h [276] | 58 h [159] |
| Oxazolidinones | ||||||||
| Linezolid | In most studies 50–60 L [278] | GA < 34 weeks: 0.92 L/kg; GA ≥ 34 weeks: 0.72 L/kg [279] Preterms < 1 week: 0.81 L/kg; Fullterms < 1 week: 0.78 L/kg; Fullterms ≥ 1 week ≤ 28 days: 0.66 L/kg [280] | 10.5–31% [278,280] | NA | 5.54 L/h for 30-year-old patients; 1.35 L/h for 85-year-old patients [281] | GA < 34 weeks: 0.17 (0.07–0.31) L/h/kg; GA ≥ 34 weeks: 0.16 (0.14–0.19) L/h/kg [279] Preterms < 1 week PNA: 2.0 mL/min/kg; Fullterms < 1 week PNA: 3.8 mL/min/kg; Fullterms ≥ 1 week ≤28 days: 5.1 mL/min/kg [280] | 4–6 h [280] | Preterms <1 week PNA: 5.6 [2.4–9.8] h; Fullterms <1 week: 3.0 [1.3–6.1] h; Fullterm ≥1 week ≤28 days: 1.5 [1.2–1.9] [280] |
| Lipoglycopeptides | ||||||||
| Telavancin | 0.1–0.15 L/kg [282] | NA | 90–93% [282] | NA | 0.012–0.014 L/h/kg [282] | NA | 6–8 h [282] | NA |
| Lipopeptides | ||||||||
| Daptomycin | 0.1 L/kg [283] | GA 23–40 weeks: 262.4 mg × h/L [284] | >90% [283] | NA | 0.01 L/h/kg [283] | GA 23–40 weeks: 0.21 L/kg [284] | 8–9 h [282] | NA |
| Fluoroquinolones | ||||||||
| Levofloxacin | 1.09–1.26 L/kg [169] | 0.5–2 years old: 1.56 L/kg (IV), 2.32 L/kg (PO) [103] | 24–38% [115] | NA | 0.5–2 years old: 0.35 L/h/kg (IV), 0.31 L/h/kg (PO) [103] | 5.76–8.52 L/h [169] | 6–8 h [169] | 0.5 to <2 years: 4.1 ± 1.3 h [103] |
| Moxifloxacin | 2.1 L/kg [285] | 2.25 L/kg [285] | 39% [285] | NA | 12 ± 2 L/h [171] | 0.35 L/h/kg [285] | 11.5–15.6 h [171] | 8.6 h [286] |
| Aminoglycosides | ||||||||
| Amikacin | 24 L [287] | 0.47–0.61 L/kg [288] | ≤10% [287] | NA | 100 mL/min—serum clearance 94mL/min—renal clearance [287] | 0.025–0.097 L/kg/hr [288] | 2–3 h [287] | PMA ≤ 29 weeks, PNA 0–7 days: 17.6 ± 4.8 h, PNA ≥ 8 days: 9.8 ± 2.1 h; PMA 30–33 weeks, PNA 0–7 days: 12.3 ± 0.5 h, PNA ≥ 8 days: 7.3 ± 3.2 h; PMA 34–36 weeks, PNA 0–7 days: 6.3 ± 1.4 h, PNA ≥ 8 days: 5.2 ± 1.6 h. [288] |
| Lincosamides | ||||||||
| Clindamycin | 0.79 L/kg [289] | PMA < 28 weeks: 1.20 L/kg; PMA > 28–32 weeks: 1.3 L/kg; PMA > 32–40 weeks: 1.03 L/kg; PMA > 40–60 weeks: 0.99 L/kg [165] | 78–94% [289] | 81% [164] | 0.3–0.4 L/h/kg [289] | PMA < 28 weeks: 0.14 L/kg/h; PMA > 28–32 weeks: 0.19 L/kg/h; PMA > 32–40 weeks: 0.24 L/kg/h; PMA > 40–60 weeks: 0.28 L/kg/h [164] | 2.4 h [202] | PMA ≤ 38 weeks: 5.89 (2.42–12.90) h; PMA > 28–32 weeks: 5.25 (2.34–8.87) h; PMA > 32–40 weeks: 3.96 (1.30–8.83) h; PMA > 40–60 weeks: 2.35 (0.94–6.44) h; PMA > 5 months < 1 year: 2.05 (1.26–3.47) h [164] |
| Glycopeptides | ||||||||
| Teicoplanin | 0.86 L/kg [290] | PMA 26 to 43 weeks: 0.283 L [291]; | 90–95% [149] | 80.5–71.9% [150] | 0.0114 L/h/kg [290] | 0.0227 L/h [291] | 70–100 h [149] | 29.75 ± 8.86 h [291] |
| Vancomycin | 0.4–1 L/kg [292] | Preterms, median age 14 (3–58) days: 0.884 L [293]; GA 23–34 weeks: 0.54 ± 0.10 L/kg [294] | 10–50% [292] | NA | 2.64 L/h [292] | Preterms, median age 14 (3–58) days: 0.1 L/h [293]; GA 23–34 weeks: 0.06 L/h/kg [294] | 4–12 h [283] | 3.5–10 h [295] |
| Other groups of antibiotics | ||||||||
| Rifampin | 1.6 L/kg [117] | 1.84 ± 0.59 [296] | 72–92% [173] | NA | 10–19.3 L/h [117] | 3.6 L/h, 70 kg [117] | 2.5 h [117] | PNA < 14 days: 7.1 (3–23.9) h; PNA ≥ 14 days: 3.5 (1.9–6.5) h [117] |
| Fosfomycin | 0.42 L/kg [113] | GA 38–40 weeks: 0.38 L/kg [172] | Negligible [172] | NA | 8.7 ± 1.7 L/h [113] | 0.14 L/h [172] | 2.4–2.8 h [113] | 2.4 ± 0.4 h [113] |
| Metronidazole | 0.25–0.85 L/kg [297] | 0.71 L/kg [297] | 20% [297] | NA | GA < 26 weeks: 0.024 (0.010–0.086) L/h; GA 26–29 weeks: 0.026 (0.012–0.076) L/h; GA 30–32 weeks: 0.029 (0.015–0.074) L/h [297] | 6–10 h [298] | 8 h [297] | GA < 26 weeks: 20.5 (5.7–49.9) h; GA 26–29 weeks: 18.6 (6.5–38.7) h; GA 30–32 weeks: 16.7 (6.5–38.7) h [297] |
| Antibiotic | Regimen and Indications for Critically Ill Neonates | Comments | PK/PD Target | Safety |
|---|---|---|---|---|
| Penicillin Group | ||||
| Penicillin G [245] | EOS: 25,000 IU/kg every 12 h for all MIC values tested (up to 2 mg/L). | GA of ≥32 weeks PNA of <72 h | 40% fT > MIC MIC < 2 mg/L 100% fT > MIC MIC ≤ 0.5 mg/L | 100 μg/mL At high doses—risk of neurotoxicity and encephalopathy [245] |
| Ampicillin [299] | 50 mg/kg every 8 h | PNA 1—10 days | 75% T > MIC MIC ≤ 8 mg/L | 140 μg/mL At high doses—risk of neurotoxicity [247] |
| Ampicillin [300] | 50 mg/kg every 8 or 12 h | GA ≥ 32 weeks | 40% fT > MIC; 100% fT > MIC | |
| Ampicillin [247] | EOS: A short-course ampicillin regimen: 2 doses, 50 mg/kg every 12 h | GA 22–27 weeks PNA < 7 days, BW < 1500 g | 100% fT > MIC MIC ≤ 8 mg/L | |
| Azlocillin [301] | 100 mg/kg every 8 h | GA 30.1–41.1 weeks PNA 1.0–2.0 days | 70% fT > MIC MIC = 2–16 mg/L | Risk of hepatotoxicity |
| Amoxicillin [302] | 50 mg/kg every 24 h 75 mg/kg every 24 h | GA 36–37 weeks GA 38–42 weeks | 100% T > MIC MIC = 0.25–1 mg/L | Doses > 140–150 mg/L: risk of nephrotoxicity |
| Flucloxacillin [254] | 25 mg/kg every 4 h 10 mg/kg every 6 h | For all neonates, irrespective of their GA and PNA. | 40% T > MIC MIC = 0.25–2 mg/L | 200 mg/L |
| Piperacillin/Tazobactam [257] | 100 mg/kg every 8 h | PMA ≤ 30 weeks | 50–75% fT > MIC MIC = 0.5–32 mg/L | 157.2 mg/L Risk of neurotoxicity [303] |
| 80 mg/kg every 6 h | PMA 30–35 weeks | |||
| 80 mg/kg every 4 h | PMA 35–49 weeks | |||
| Ticarcillin/Clavulanic acid [259] | 75 mg/kg every 12 h | PNA < 14 weeks | 75% fT > MIC MIC = 0.5–16 mg/L | |
| 75 mg/kg every 8 h | PNA ≥ 14–45 weeks | |||
| Cephalosporins | ||||
| Ceftoraline Fosamil [304] | 6 mg/kg every 8 h | <2 months | 35–44% fT > MIC MIC = 0.5–2 mg/L | High risk of diarrhea |
| Ceftazidime [305] | 25 mg/kg every 8 h for MIC 4 mg/L | 0.1–2 years | 70% fT > MIC MIC = 4–8 mg/L | |
| 50 mg/kg every 8 h for MIC 8 mg/L | ||||
| Cefotaxime [262] | 50 mg/kg every 12 h | GA 30.0–41.1 weeks PNA 1.0–3.0 days | 70% fT > MIC MIC = 2 mg/L | Feeding intolerance Diarrhea [262] |
| Cefotaxime [306] | 50 mg/kg every 12 h | PNA < 7 days | 75% fT > MIC MIC = 2–4 mg/L | |
| 50 mg/kg every 8 h | GA < 32 weeks PNA ≥ 7 days | |||
| 50 mg/kg every 6 h | GA ≥ 32 weeks PNA ≥ 7 days | |||
| Cefepime [266] | 50 mg/kg every 12 h for MIC 4 mg/L | PMA < 38 weeks | 70% fT > MIC MIC = 4–8 mg/L | |
| 40 mg/kg every 8 h for MIC 8 mg/L | PMA ≥ 38 weeks | |||
| Cefazoline [307] | 25 mg/kg every 12 h | PNA ≤ 7 days BW ≤ 2000 g | 60% fT > MIC MIC > 8 mg/L | |
| 50 mg/kg every 12 h | PNA ≤ 7 days BW > 2000 g | |||
| 25 mg/kg every 8 h | PNA 8–28 days BW ≤ 2000 g | |||
| 50 mg/kg every 8 h | PNA 8–28 days BW > 2000 g | |||
| Carbapenems | ||||
| Meropenem [308] | 20 mg/kg every 12 h | GA < 32 weeks PNA < 14 weeks | 50% T > MIC MIC = 4 mg/L 75% T > MIC MIC = 2 mg/L | 64.2 mg/L—risk of neurotoxicity 44.45 mg/L for Cmin—risk of nephrotoxicity [309] |
| 20 mg/kg every 8 h | GA < 32 weeks PNA ≥ 14 weeks GA ≥ 32 weeks PNA < 14 weeks | |||
| 30 mg/kg every 8 h | GA ≥ 32 weeks PNA ≥ 14 weeks | |||
| Doripenem [275] | 5 mg/kg every 24 h | <8 weeks PNA < 12 weeks | 70–100% T > MIC MIC = 1 mg/L | Well tolerated |
| 8 mg/kg every 24 h | >8 weeks PNA < 12 weeks | |||
| Imipenem [272] | 20–25 mg/kg every 6–12 h | GA 24–41 weeks PNA 2–153 days | 100% T > MIC MIC = 2 mg/L | |
| Lipopeptides | ||||
| Daptomycin [310] | 6 mg/kg every 12 h | Median GA 27 weeks; PNA 5 days | NO PK/PD STUDY | Risk of elevation of liver enzymes |
| Fluoroquinolones | ||||
| Levofloxacin [311] | 10 mg/kg every 12 h | PMA 27–42 weeks | NO PK/PD STUDY | Risk of diarrhea, hepatotoxicity, Dysglycemia |
| Moxifloxacin [285] | 6 mg/kg every 12 h | >3 months to <2 years | AUC(0–24) at steady state 20–60 mg·h/L Cmax at steady state 2–6 mg/L | Risk of individual intolerance risk of QT prolongation |
| Moxifloxacin [286] | 5 mg/kg every 24 h | GA 25 weeks | Cmax/MIC: >10 AUC0–24/MIC: ≥100 | |
| Macrolides | ||||
| Azithromycin [277] | 20 mg/kg every 24 h × 3 days | GA 24–28 weeks PMA < 72 h | AUC24/MIC90 of >4 h | Risk of necrotizing enterocolitis, intraventricular hemorrhage |
| Lincosamides | ||||
| Clindamycin [164] | 5 mg/kg every 8 h | PMA ≤ 32 weeks | AUCss,0–8 = 33.8 μg·h/mL Css,max = 7.9 μg/mL fCss,50 = 0.12 μg/mL | No adverse events related to clindamycin use in this study |
| 7 mg/kg every 8 h | PMA 32–40 weeks | |||
| 9 mg/kg every 8 h | PMA > 40–60 weeks | |||
| Aminoglycosides | ||||
| Amikacin [312] | 15 mg/kg 30–36 h | PNA ≤ 14 days BW 2000 g; ≥2800 g | Ctrough < 3 μg/mL Cmax 24 g/mL | Toxicity risk at Cmin > 5 μg/mL [312] |
| Amikacin [288] | 13 mg/kg every 48 h | PNA 0–7 days PCA ≤ 29 weeks | Serum peak concentration 20–30 mg/L | |
| 13 mg/kg every 36 h | PNA ≥ 8 days PCA ≤ 29 weeks PNA 0–7 days PCA 30–33 weeks | |||
| 13 mg/kg every 24 h | PNA ≥ 8 days PCA 30–33 weeks PNA 0–7 days PCA 34–36 weeks | |||
| 13 mg/kg every 18 h | PNA ≥ 8 days PCA 34–36 weeks | |||
| 13 mg/kg every 24 h | PNA 0–7 days PCA ≥ 37 weeks | |||
| 13 mg/kg every 24 h | PNA ≥ 8 days PCA ≥37 weeks | |||
| Gentamicin [313] | 5 mg/kg every 48 h | Premature BW <1200 g | Cmax/MIC ratio at least 8–10 | Toxicity risk at Cmin > 2 μg/mL and Cmax > 35 μg/mL Risk of nephrotoxicity, neurotoxicity, ototoxicity |
| 5 mg/kg every 36 h | Premature BW 1200–2500 g | |||
| 5 mg/kg every 24 h | BW > 2500 g; Term neonates 1–28 days | |||
| Gentamicin [314] | 5 mg/kg every 36 h | PMA 30–34 weeks PNA 8–28 days PMA ≥ 35 weeks PNA 0–7 days | Ctrough < 1 μg/mL | |
| Gentamicin/Tobramicin [315] | 4.5 mg/kg of gentamicin and 5.5 mg/kg of tobramycin every 72 h | PNA ≤ 5 days | Cmax 5–12 μg/mL Ctrough < 0.5 μg/mL | |
| Glycopeptides | ||||
| Vancomycin [293] | 12 mg/kg every 8 h | GA 23–34 weeks | AUC0–24 h of ≥400 mg·h/L | >20 μg/mL—risk of nephrotoxicity [293] |
| Vancomycin [316] | 25 mg/kg (LD) 15 mg/kg (MD) every 12 h | PMA < 35 weeks | AUC0–24 of 400 mg·h/L at steady-state | |
| 25 mg/kg (LD) 15 mg/kg (MD) every 8 h | PMA ≥ 35 weeks | |||
| Vancomycin [317] | 32–60 mg/kg/day (4 doses) | <1 year | AUC0–24/MIC > 400 | |
| 60 mg/kg/day (4 doses) | >1 year | |||
| Vancomycin [294] | 10 mg/kg every 12 h | PMA < 30 weeks | AUC0–24/MIC ≥ 267 at steady state | |
| 10 mg/kg every 8 h | PMA ≥ 35 weeks | |||
| Teicoplanin [291] | 16 mg/kg 10–11 mg/kg every 24 h | BW: <1000 g BW: 1000 <2000 g | AUC/MIC ratio of ≥400 | |
| Other groups of antibiotics | ||||
| Rifampin [117] | 8 mg/kg every 24 h | PNA < 14 days | AUC∞ = 55.2 μg·h/mL Cmax,ss = 8.3 ± 1.8 μg/mL | Well tolerated |
| 15 mg/kg every 24 h | PNA 14–61 days | AUC∞ = 55.2 μg·h/mL Cmax,ss = 13.2 ± 3.3 μg/mL | ||
| Rifampin [296] | 10 mg/kg every 24 h | GA 29.9 (4.1) weeks PNA 24.8 (13.4) days | Plasma concentrations >MIC | |
| Fosfomycin [318] | 50–100 mg/kg every 8 h 50–70 mg/kg every 6 h | Healthy Pre-Term and Full-Term Neonates | MIC = 64 mg/L | Well tolerated |
| 100 mg/kg every 24 h 2 partial doses | Pre-Term Neonates aged 1–3 days | MIC = 32 mg/L | ||
| 150–200 mg/kg every 24 h 3–4 partial doses | Pre-Term neonates aged 3–5 weeks | MIC = 32 mg/L | ||
| Fosfomycin [172] | 100 mg/kg every 12 h | Neonates aged < 7 days or weighing < 1500 g | MIC = 32 mg/L | |
| Metronidazole [319] | 7.5 mg/kg every 12 h 15 mg/kg (LD) | PMA < 34 weeks | Cminss > 2 mg/L | |
| 7.5 mg/kg every 8 h 15 mg/kg (LD) | PMA 34–40 weeks | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Butranova, O.I.; Ushkalova, E.A.; Zyryanov, S.K.; Chenkurov, M.S. Developmental Pharmacokinetics of Antibiotics Used in Neonatal ICU: Focus on Preterm Infants. Biomedicines 2023, 11, 940. https://doi.org/10.3390/biomedicines11030940
Butranova OI, Ushkalova EA, Zyryanov SK, Chenkurov MS. Developmental Pharmacokinetics of Antibiotics Used in Neonatal ICU: Focus on Preterm Infants. Biomedicines. 2023; 11(3):940. https://doi.org/10.3390/biomedicines11030940
Chicago/Turabian StyleButranova, Olga I., Elena A. Ushkalova, Sergey K. Zyryanov, and Mikhail S. Chenkurov. 2023. "Developmental Pharmacokinetics of Antibiotics Used in Neonatal ICU: Focus on Preterm Infants" Biomedicines 11, no. 3: 940. https://doi.org/10.3390/biomedicines11030940