

ACTH Stimulation Test for the Diagnosis of Secondary Adrenal Insufficiency: Light and Shadow
 ,
,
Abstract
:1. Introduction
2. Methodology
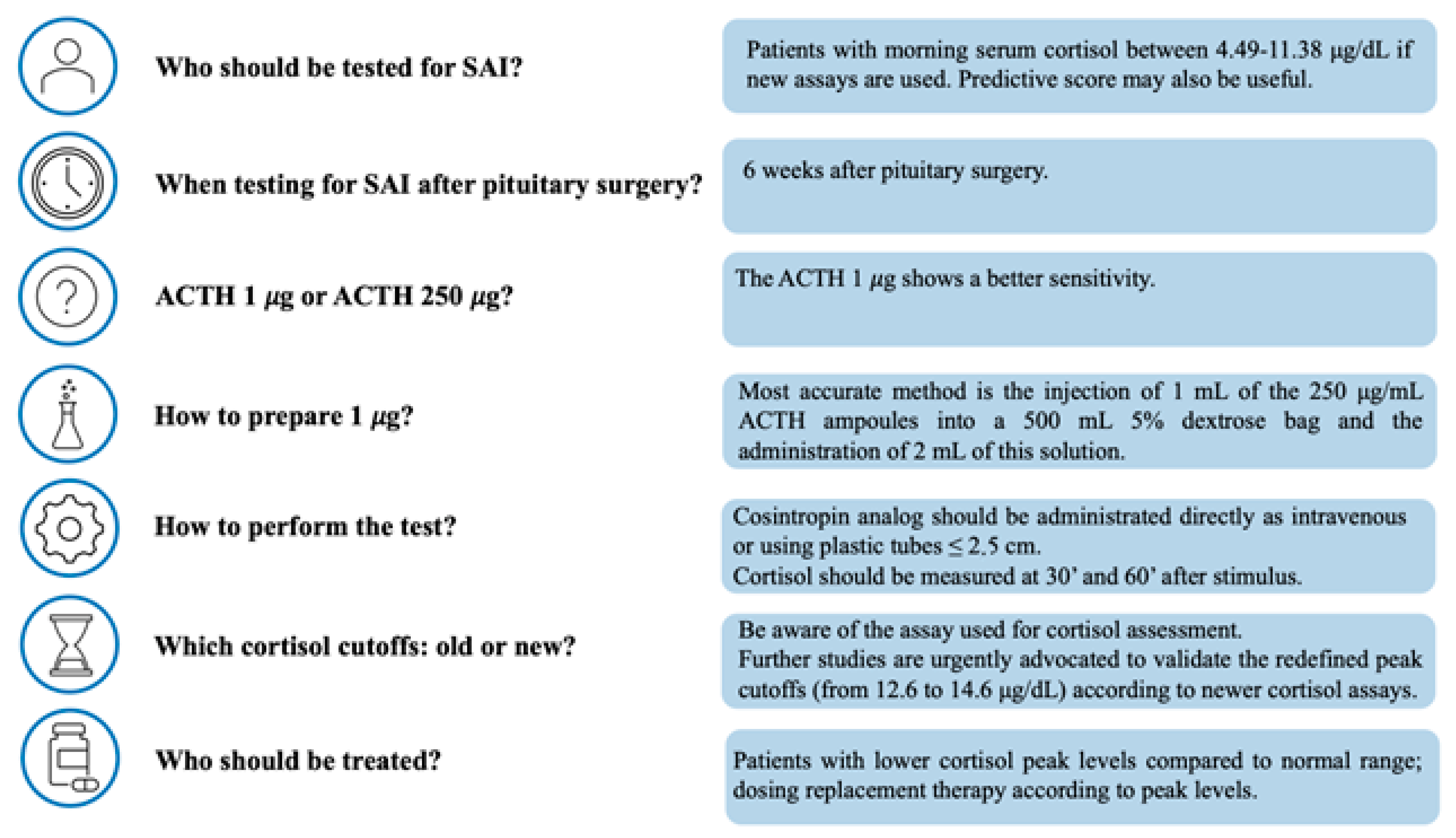
3. Patients to Be Tested and Timing for Testing
4. How to Perform the Test
5. Alternative Tests for the Assessment of HPA Axis
6. How to Interpret the Results: Old and New Cortisol Cutoffs
7. When to Repeat the Test?
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Arlt, W.; Allolio, B. Adrenal insufficiency. Lancet 2003, 361, 1881–1893. [Google Scholar] [CrossRef] [PubMed]
- Rushworth, R.L.; Torpy, D.J. The Changing Epidemiology of Adrenal Insufficiency: Iatrogenic Factors Predominate. J. Endocr. Soc. 2023, 7, bvad017. [Google Scholar] [CrossRef]
- Husebye, E.S.; Pearce, S.H.; Krone, N.P.; Kampe, O. Adrenal insufficiency. Lancet 2021, 397, 613–629. [Google Scholar] [CrossRef]
- Falhammar, H. Skeletal fragility induced by overtreatment of adrenal insufficiency. Endocrine 2018, 59, 239–241. [Google Scholar] [CrossRef] [Green Version]
- Bornstein, S.R.; Allolio, B.; Arlt, W.; Barthel, A.; Don-Wauchope, A.; Hammer, G.D.; Husebye, E.S.; Merke, D.P.; Murad, M.H.; Stratakis, C.A.; et al. Diagnosis and Treatment of Primary Adrenal Insufficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2016, 101, 364–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paluzzi, A.; Fernandez-Miranda, J.C.; Tonya Stefko, S.; Challinor, S.; Snyderman, C.H.; Gardner, P.A. Endoscopic endonasal approach for pituitary adenomas: A series of 555 patients. Pituitary 2014, 17, 307–319. [Google Scholar] [CrossRef] [PubMed]
- Oshino, S.; Saitoh, Y.; Kinoshita, M.; Mukai, K.; Otsuki, M.; Kishima, H. Characteristics of Nonfunctioning Pituitary Adenomas That Cause Secondary Adrenal Insufficiency. World Neurosurg. 2021, 153, e275–e281. [Google Scholar] [CrossRef]
- Jacques, J.P.; Valadares, L.P.; Moura, A.C.; Oliveira, M.R.F.; Naves, L.A. Frequency and clinical characteristics of hypophysitis and hypopituitarism in patients undergoing immunotherapy—A systematic review. Front. Endocrinol. 2023, 14, 1091185. [Google Scholar] [CrossRef]
- Burgos, N.; Ghayee, H.K.; Singh-Ospina, N. Pitfalls in the interpretation of the cosyntropin stimulation test for the diagnosis of adrenal insufficiency. Curr. Opin. Endocrinol. Diabetes Obes. 2019, 26, 139–145. [Google Scholar] [CrossRef]
- Garrahy, A.; Agha, A. How should we interrogate the hypothalamic-pituitary-adrenal axis in patients with suspected hypopituitarism? BMC Endocr. Disord. 2016, 16, 36. [Google Scholar] [CrossRef] [Green Version]
- Fleseriu, M.; Hashim, I.A.; Karavitaki, N.; Melmed, S.; Murad, M.H.; Salvatori, R.; Samuels, M.H. Hormonal Replacement in Hypopituitarism in Adults: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2016, 101, 3888–3921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inder, W.J.; Hunt, P.J. Glucocorticoid replacement in pituitary surgery: Guidelines for perioperative assessment and management. J. Clin. Endocrinol. Metab. 2002, 87, 2745–2750. [Google Scholar] [CrossRef] [PubMed]
- Ravindran, R.; Carter, J.L.; Kumar, A.; Capatana, F.; Khan, I.N.; Adlan, M.A.; Premawardhana, L.D. Pre-test Cortisol Levels in Predicting Short Synacthen Test Outcome: A Retrospective Analysis. Clin. Med. Insights Endocrinol. Diabetes 2022, 15, 11795514221093316. [Google Scholar] [CrossRef] [PubMed]
- Gasco, V.; Bima, C.; Geranzani, A.; Giannelli, J.; Marinelli, L.; Bona, C.; Cambria, V.; Berton, A.M.; Prencipe, N.; Ghigo, E.; et al. Morning Serum Cortisol Level Predicts Central Adrenal Insufficiency Diagnosed by Insulin Tolerance Test. Neuroendocrinology 2021, 111, 1238–1248. [Google Scholar] [CrossRef]
- Michaelidou, M.; Yadegarfar, G.; Morris, L.; Dolan, S.; Robinson, A.; Naseem, A.; Livingston, M.; Duff, C.J.; Trainer, P.; Fryer, A.A.; et al. Recalibration of thinking about adrenocortical function assessment: How the “random” cortisol relates to the short synacthen test results. Cardiovasc. Endocrinol. Metab. 2021, 10, 137–145. [Google Scholar] [CrossRef]
- Bioletto, F.; Berton, A.M.; Varaldo, E.; Cuboni, D.; Bona, C.; Parasiliti-Caprino, M.; Prencipe, N.; Ghigo, E.; Grottoli, S.; Maccario, M.; et al. Development and internal validation of a predictive score for the diagnosis of central adrenal insufficiency when morning cortisol is in the grey zone. J. Endocrinol. Investig. 2023, 46, 535–543. [Google Scholar] [CrossRef]
- Dorin, R.I.; Qualls, C.R.; Crapo, L.M. Diagnosis of adrenal insufficiency. Ann. Intern. Med. 2003, 139, 194–204. [Google Scholar] [CrossRef]
- Ospina, N.S.; Al Nofal, A.; Bancos, I.; Javed, A.; Benkhadra, K.; Kapoor, E.; Lteif, A.N.; Natt, N.; Murad, M.H. ACTH Stimulation Tests for the Diagnosis of Adrenal Insufficiency: Systematic Review and Meta-Analysis. J. Clin. Endocrinol. Metab. 2016, 101, 427–434. [Google Scholar] [CrossRef] [Green Version]
- Kazlauskaite, R.; Evans, A.T.; Villabona, C.V.; Abdu, T.A.; Ambrosi, B.; Atkinson, A.B.; Choi, C.H.; Clayton, R.N.; Courtney, C.H.; Gonc, E.N.; et al. Corticotropin tests for hypothalamic-pituitary- adrenal insufficiency: A metaanalysis. J. Clin. Endocrinol. Metab. 2008, 93, 4245–4253. [Google Scholar] [CrossRef] [Green Version]
- Daidoh, H.; Morita, H.; Mune, T.; Murayama, M.; Hanafusa, J.; Ni, H.; Shibata, H.; Yasuda, K. Responses of plasma adrenocortical steroids to low dose ACTH in normal subjects. Clin. Endocrinol. 1995, 43, 311–315. [Google Scholar] [CrossRef]
- Grinspoon, S.K.; Biller, B.M. Clinical review 62: Laboratory assessment of adrenal insufficiency. J. Clin. Endocrinol. Metab. 1994, 79, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Elder, C.J.; Sachdev, P.; Wright, N.P. The short Synacthen test: A questionnaire survey of current usage. Arch. Dis. Child 2012, 97, 870–873. [Google Scholar] [CrossRef]
- Cross, A.S.; Helen Kemp, E.; White, A.; Walker, L.; Meredith, S.; Sachdev, P.; Krone, N.P.; Ross, R.J.; Wright, N.P.; Elder, C.J. International survey on high and low-dose synacthen test and assessment of accuracy in preparing low-dose synacthen. Clin. Endocrinol. 2018, 88, 744–751. [Google Scholar] [CrossRef] [Green Version]
- Wade, M.; Baid, S.; Calis, K.; Raff, H.; Sinaii, N.; Nieman, L. Technical details influence the diagnostic accuracy of the 1 microg ACTH stimulation test. Eur. J. Endocrinol. 2010, 162, 109–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saiegh, L.; Abu-Ahmad, A.; Sheikh-Ahmad, M.; Reut, M.; Chen-Konak, L.; Jiries, N.; Shechner, C. Performance of low-dose cosyntropin stimulation test handled via plastic tube. Endocrine 2017, 57, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.; Madathil, S.; Maheshwari, V.; Roy, K.; Kumar, B.; Jain, V. Long-acting intramuscular ACTH stimulation test for the diagnosis of secondary adrenal insufficiency in children. J. Pediatr. Endocrinol. Metab. 2019, 32, 57–63. [Google Scholar] [CrossRef]
- Ozsu, E.; Siklar, Z.; Bilici, E.; Ceran, A.; Uyanik, R.; Cetin, T.; Aycan, Z.; Berberoglu, M. Intramuscular Short-term ACTH Test for the Determination of Adrenal Function in Children: Safe, Effective and Reliable. J. Clin. Res. Pediatr. Endocrinol. 2020, 12, 241–247. [Google Scholar] [CrossRef]
- Chatha, K.K.; Middle, J.G.; Kilpatrick, E.S. National UK audit of the short synacthen test. Ann. Clin. Biochem. 2010, 47, 158–164. [Google Scholar] [CrossRef]
- Park, Y.J.; Park, K.S.; Kim, J.H.; Shin, C.S.; Kim, S.Y.; Lee, H.K. Reproducibility of the cortisol response to stimulation with the low dose (1 microg) of ACTH. Clin. Endocrinol. 1999, 51, 153–158. [Google Scholar] [CrossRef]
- Munro, V.; Elnenaei, M.; Doucette, S.; Clarke, D.B.; Imran, S.A. The effect of time of day testing and utility of 30 and 60 minute cortisol values in the 250 mcg ACTH stimulation test. Clin. Biochem. 2018, 54, 37–41. [Google Scholar] [CrossRef]
- Cartaya, J.; Misra, M. The low-dose ACTH stimulation test: Is 30 minutes long enough? Endocr. Pr. 2015, 21, 508–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gill, H.; Barrowman, N.; Webster, R.; Ahmet, A. Evaluating the Low-Dose ACTH Stimulation Test in Children: Ideal Times for Cortisol Measurement. J. Clin. Endocrinol. Metab. 2019, 104, 4587–4593. [Google Scholar] [CrossRef] [PubMed]
- Yudina, A.E.; Pavlova, M.G.; Sotnikov, V.M.; Tselovalnikova, T.Y.; Mazerkina, N.A.; Zheludkova, O.G.; Gerasimov, A.N.; Teryaeva, N.B.; Martynova, E.; Kim, E.I. The glucagon test in diagnosis of secondary adrenal insufficiency after craniospinal irradiation: The feasibility of application, the features of performing the test, and its diagnostic informativity. Probl. Endokrinol. 2019, 65, 227–235. [Google Scholar] [CrossRef]
- Ach, T.; Abdelkrim, A.B.; Hasni, Y.; Saad, G.; Kacem, M.; Chaieb, M.; Zaouali, M.; Maaroufi, A.; Ach, K. Safety Assessment and Potential Risks of the Glucagon Stimulation Test in the Diagnosis of Secondary Adrenal Insufficiency. Curr. Drug Saf. 2022, 17, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Yalovitsky, G.; Shaki, D.; Hershkovitz, E.; Friger, M.; Haim, A. Comparison of glucagon stimulation test and low dose ACTH test in assessing hypothalamic-pituitary-adrenal (HPA) axis in children. Clin. Endocrinol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Fiad, T.M.; Kirby, J.M.; Cunningham, S.K.; McKenna, T.J. The overnight single-dose metyrapone test is a simple and reliable index of the hypothalamic-pituitary-adrenal axis. Clin. Endocrinol. 1994, 40, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Hartzband, P.I.; Van Herle, A.J.; Sorger, L.; Cope, D. Assessment of hypothalamic-pituitary-adrenal (HPA) axis dysfunction: Comparison of ACTH stimulation, insulin-hypoglycemia and metyrapone. J. Endocrinol. Investig. 1988, 11, 769–776. [Google Scholar] [CrossRef] [PubMed]
- Papierska, L.; Rabijewski, M.; Migda, B.; Leszczynska, D.; Nowak, K.; Lebek-Szatanska, A.; Glinicki, P.; Zgliczynski, W. Evaluation of plasma ACTH in the metyrapone test is insufficient for the diagnosis of secondary adrenal insufficiency. Front. Endocrinol. 2022, 13, 1004129. [Google Scholar] [CrossRef]
- Raverot, V.; Richet, C.; Morel, Y.; Raverot, G.; Borson-Chazot, F. Establishment of revised diagnostic cut-offs for adrenal laboratory investigation using the new Roche Diagnostics Elecsys((R)) Cortisol II assay. Ann. Endocrinol. 2016, 77, 620–622. [Google Scholar] [CrossRef]
- Vogeser, M.; Kratzsch, J.; Ju Bae, Y.; Bruegel, M.; Ceglarek, U.; Fiers, T.; Gaudl, A.; Kurka, H.; Milczynski, C.; Prat Knoll, C.; et al. Multicenter performance evaluation of a second generation cortisol assay. Clin. Chem. Lab. Med. 2017, 55, 826–835. [Google Scholar] [CrossRef] [Green Version]
- Hawley, J.M.; Owen, L.J.; Lockhart, S.J.; Monaghan, P.J.; Armston, A.; Chadwick, C.A.; Wilshaw, H.; Freire, M.; Perry, L.; Keevil, B.G. Serum Cortisol: An Up-To-Date Assessment of Routine Assay Performance. Clin. Chem. 2016, 62, 1220–1229. [Google Scholar] [CrossRef] [Green Version]
- Monaghan, P.J.; Keevil, B.G.; Stewart, P.M.; Trainer, P.J. Case for the wider adoption of mass spectrometry-based adrenal steroid testing, and beyond. J. Clin. Endocrinol. Metab. 2014, 99, 4434–4437. [Google Scholar] [CrossRef] [Green Version]
- Monaghan, P.J.; Keevil, B.G.; Trainer, P.J. The use of mass spectrometry to improve the diagnosis and the management of the HPA axis. Rev. Endocr. Metab. Disord. 2013, 14, 143–157. [Google Scholar] [CrossRef] [PubMed]
- Javorsky, B.R.; Raff, H.; Carroll, T.B.; Algeciras-Schimnich, A.; Singh, R.J.; Colon-Franco, J.M.; Findling, J.W. New Cutoffs for the Biochemical Diagnosis of Adrenal Insufficiency after ACTH Stimulation using Specific Cortisol Assays. J. Endocr. Soc. 2021, 5, bvab022. [Google Scholar] [CrossRef] [PubMed]
- Ueland, G.A.; Methlie, P.; Oksnes, M.; Thordarson, H.B.; Sagen, J.; Kellmann, R.; Mellgren, G.; Raeder, M.; Dahlqvist, P.; Dahl, S.R.; et al. The Short Cosyntropin Test Revisited: New Normal Reference Range Using LC-MS/MS. J. Clin. Endocrinol. Metab. 2018, 103, 1696–1703. [Google Scholar] [CrossRef] [Green Version]
- El-Farhan, N.; Pickett, A.; Ducroq, D.; Bailey, C.; Mitchem, K.; Morgan, N.; Armston, A.; Jones, L.; Evans, C.; Rees, D.A. Method-specific serum cortisol responses to the adrenocorticotrophin test: Comparison of gas chromatography-mass spectrometry and five automated immunoassays. Clin. Endocrinol. 2013, 78, 673–680. [Google Scholar] [CrossRef]
- Grassi, G.; Morelli, V.; Ceriotti, F.; Polledri, E.; Fustinoni, S.; D’Agostino, S.; Mantovani, G.; Chiodini, I.; Arosio, M. Minding the gap between cortisol levels measured with second-generation assays and current diagnostic thresholds for the diagnosis of adrenal insufficiency: A single-center experience. Hormones 2020, 19, 425–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kline, G.A.; Buse, J.; Krause, R.D. Clinical implications for biochemical diagnostic thresholds of adrenal sufficiency using a highly specific cortisol immunoassay. Clin. Biochem. 2017, 50, 475–480. [Google Scholar] [CrossRef]
- Zha, L.; Li, J.; Krishnan, S.M.; Brennan, M.R.; Zhang, Y.V.; Povse, P.; Kerlin, R.; Shively, K.; Oleksik, F.; Williams, J.; et al. New Diagnostic Cutoffs for Adrenal Insufficiency After Cosyntropin Stimulation Using Abbott Architect Cortisol Immunoassay. Endocr. Pr. 2022, 28, 684–689. [Google Scholar] [CrossRef]
- Husni, H.; Abusamaan, M.S.; Dinparastisaleh, R.; Sokoll, L.; Salvatori, R.; Hamrahian, A.H. Cortisol values during the standard-dose cosyntropin stimulation test: Personal experience with Elecsys cortisol II assay. Front. Endocrinol. 2022, 13, 978238. [Google Scholar] [CrossRef]


{kind=link}
| Author, Year | ACTH Dose | Cohort | N. of Patients | 30-Min Cortisol Post-ACTH Stimulus | |||
|---|---|---|---|---|---|---|---|
| Elecsys I | Elecsys II | Access | LC-MS/MS | ||||
| Raverot et al., 2016 [39] | NA | PAI/SAI | 109 | 18.1 μg/dL (500 nmol/L | 13.6 μg/dL (374 nmol/L) | NA | NA |
| Kline et al., 2017 [48] | 250 μg/1 μg | NA | 56 * | 18.1 μg/dL (500 nmol/L) | 12.6 μg/dL (350 nmol/L) | NA | NA |
| Ueland et al., 2018 [45] | 250 μg | PAI/SAI | 94 | 18.1 μg/dL (500 nmol/L) | NA | NA | 14.9 μg/dL (412 nmol/L) |
| Grassi et al., 2020 [47] | 250 μg/1 μg | PAI/SAI | 30 | 18.1 μg/dL (500 nmol/L) | 12.7 μg/dL (351 nmol/L) | NA | 13.3 μg/dL (368 nmol/L) |
| Javorsky et al., 2021 [44] | 250 μg | PAI/SAI/TAI | 110 | 18.1 μg/dL (500 nmol/L) | 14.6 μg/dL (402 nmol/L) | 14.8 μg/dL (408 nmol/L) | 14.5 μg/dL (400 nmol/L) |
| Zha et al., 2022 [49] | 250 μg | NA | 50 | 18.1 μg/dL (500 nmol/L) | NA | 13.2 μg/dL (364 nmol/L) | NA |
| Husni et al., 2022 [50] | 250 μg | healthy volunteers | 63 | 18.1 μg/dL (500 nmol/L) | 15.7 μg/dL (433 nmol/) | NA | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Birtolo, M.F.; Antonini, S.; Saladino, A.; Zampetti, B.; Lavezzi, E.; Chiodini, I.; Mazziotti, G.; Lania, A.G.A.; Cozzi, R. ACTH Stimulation Test for the Diagnosis of Secondary Adrenal Insufficiency: Light and Shadow. Biomedicines 2023, 11, 904. https://doi.org/10.3390/biomedicines11030904
Birtolo MF, Antonini S, Saladino A, Zampetti B, Lavezzi E, Chiodini I, Mazziotti G, Lania AGA, Cozzi R. ACTH Stimulation Test for the Diagnosis of Secondary Adrenal Insufficiency: Light and Shadow. Biomedicines. 2023; 11(3):904. https://doi.org/10.3390/biomedicines11030904
Chicago/Turabian StyleBirtolo, Maria Francesca, Simone Antonini, Andrea Saladino, Benedetta Zampetti, Elisabetta Lavezzi, Iacopo Chiodini, Gherardo Mazziotti, Andrea G. A. Lania, and Renato Cozzi. 2023. "ACTH Stimulation Test for the Diagnosis of Secondary Adrenal Insufficiency: Light and Shadow" Biomedicines 11, no. 3: 904. https://doi.org/10.3390/biomedicines11030904