
Biomarkers of Neutrophil Activation in Patients with Symptomatic Chronic Peripheral Artery Disease Predict Worse Cardiovascular Outcome
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Clinical Data Collection and Biochemical Analysis at Baseline
2.3. Quantification of Circulating Markers of Neutrophil Activation and NETs Target by ELISA
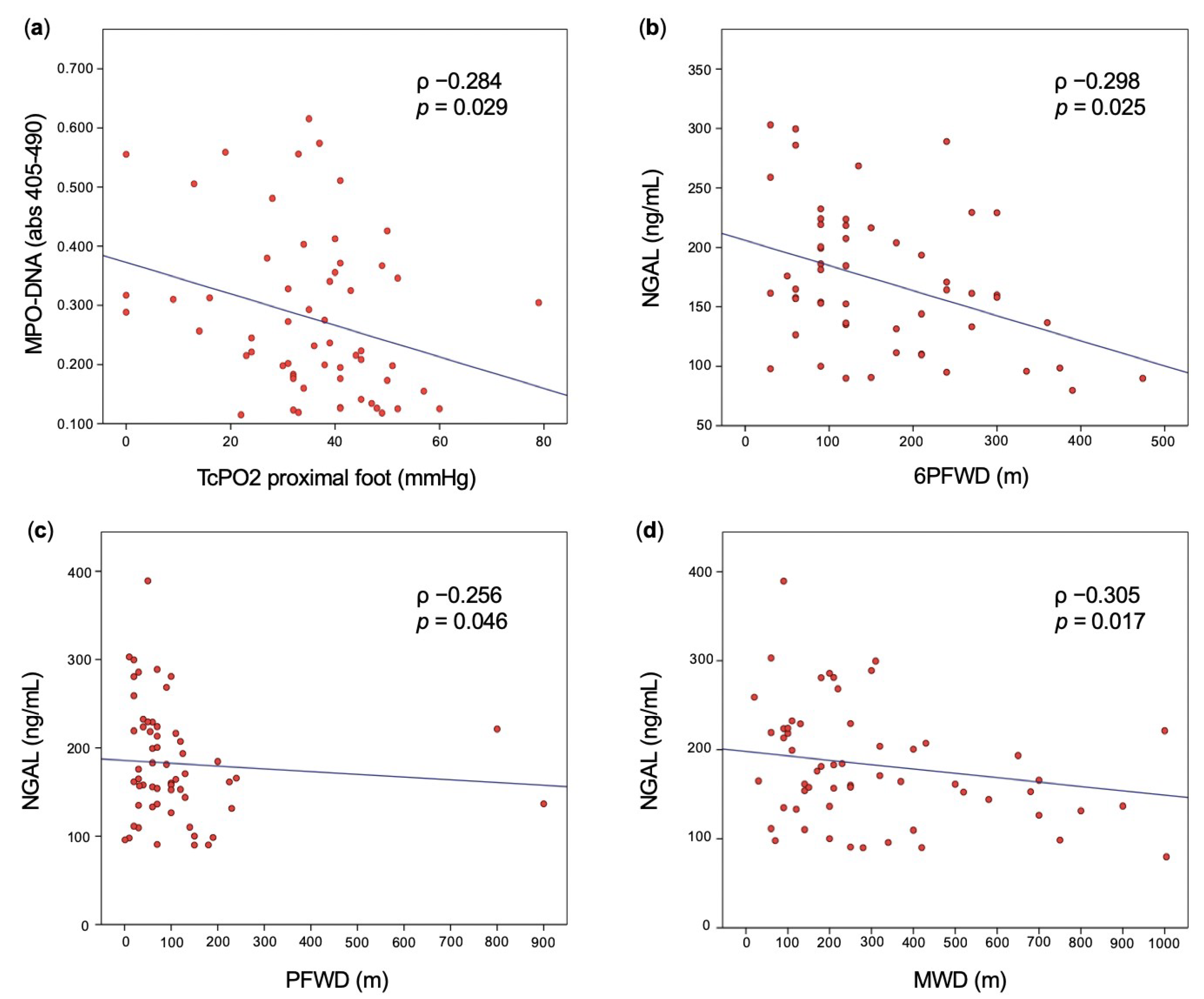
2.4. Vascular Assessment in Patients with PAD
2.5. Clinical Outcomes
2.6. Statistical Analysis
3. Results
3.1. General Study Population Characteristics
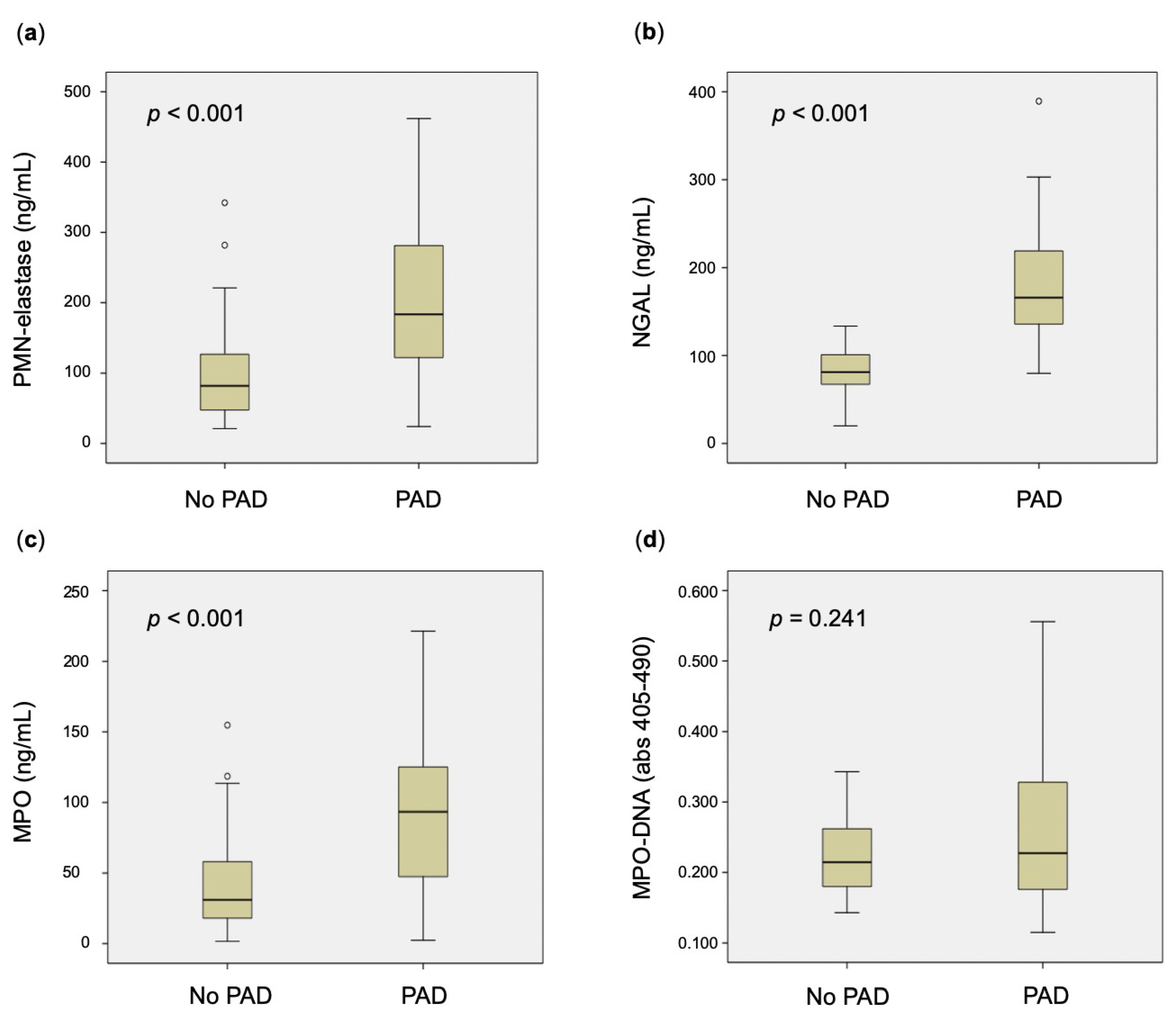
3.2. Circulating Markers of Neutrophil Degranulation in Patients with PAD and Controls
3.3. Circulating NETs in Patients with PAD and Controls
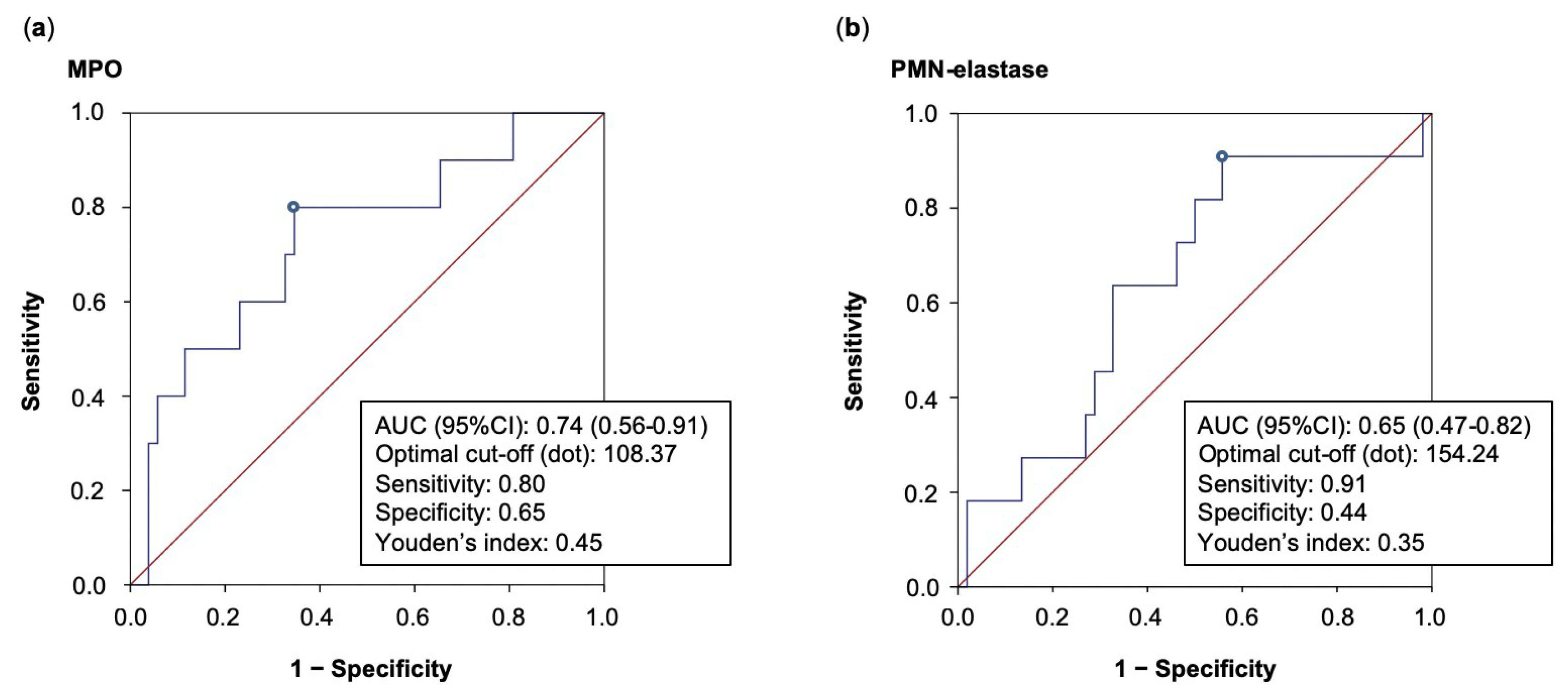
3.4. Clinical Outcomes in Patients with PAD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fowkes, F.G.; Rudan, D.; Rudan, I.; Aboyans, V.; Denenberg, J.O.; McDermott, M.M.; Norman, P.E.; Sampson, U.K.; Williams, L.J.; Mensah, G.A.; et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: A systematic review and analysis. Lancet 2013, 382, 1329–1340. [Google Scholar] [CrossRef] [PubMed]
- Libby, P.; Ridker, P.M.; Hansson, G.K. Progress and challenges in translating the biology of atherosclerosis. Nature 2011, 473, 317–325. [Google Scholar] [CrossRef]
- Wyss, C.A.; Neidhart, M.; Altwegg, L.; Spanaus, K.S.; Yonekawa, K.; Wischnewsky, M.B.; Corti, R.; Kucher, N.; Roffi, M.; Eberli, F.R.; et al. Cellular actors, Toll-like receptors, and local cytokine profile in acute coronary syndromes. Eur. Heart J. 2010, 31, 1457–1469. [Google Scholar] [CrossRef] [PubMed]
- Rosales, C. Neutrophil: A Cell with Many Roles in Inflammation or Several Cell Types? Front. Physiol. 2018, 9, 113. [Google Scholar] [CrossRef] [PubMed]
- Madjid, M.; Awan, I.; Willerson, J.T.; Casscells, S.W. Leukocyte count and coronary heart disease: Implications for risk assessment. J. Am. Coll. Cardiol. 2004, 44, 1945–1956. [Google Scholar] [CrossRef] [PubMed]
- Brill, A.; Fuchs, T.A.; Savchenko, A.S.; Thomas, G.M.; Martinod, K.; De Meyer, S.F.; Bhandari, A.A.; Wagner, D.D. Neutrophil extracellular traps promote deep vein thrombosis in mice. J. Thromb. Haemost. 2012, 10, 136–144. [Google Scholar] [CrossRef]
- Fuchs, T.A.; Brill, A.; Duerschmied, D.; Schatzberg, D.; Monestier, M.; Myers, D.D., Jr.; Wrobleski, S.K.; Wakefield, T.W.; Hartwig, J.H.; Wagner, D.D. Extracellular DNA traps promote thrombosis. Proc. Natl. Acad. Sci. USA 2010, 107, 15880–15885. [Google Scholar] [CrossRef]
- Sharma, S.; Hofbauer, T.M.; Ondracek, A.S.; Chausheva, S.; Alimohammadi, A.; Artner, T.; Panzenboeck, A.; Rinderer, J.; Shafran, I.; Mangold, A.; et al. Neutrophil extracellular traps promote fibrous vascular occlusions in chronic thrombosis. Blood 2021, 137, 1104–1116. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.K.; Joshi, M.B.; Philippova, M.; Erne, P.; Hasler, P.; Hahn, S.; Resink, T.J. Activated endothelial cells induce neutrophil extracellular traps and are susceptible to NETosis-mediated cell death. FEBS Lett. 2010, 584, 3193–3197. [Google Scholar] [CrossRef]
- Knight, J.S.; Luo, W.; O’Dell, A.A.; Yalavarthi, S.; Zhao, W.; Subramanian, V.; Guo, C.; Grenn, R.C.; Thompson, P.R.; Eitzman, D.T.; et al. Peptidylarginine deiminase inhibition reduces vascular damage and modulates innate immune responses in murine models of atherosclerosis. Circ. Res. 2014, 114, 947–956. [Google Scholar] [CrossRef]
- Borissoff, J.I.; Joosen, I.A.; Versteylen, M.O.; Brill, A.; Fuchs, T.A.; Savchenko, A.S.; Gallant, M.; Martinod, K.; Ten Cate, H.; Hofstra, L.; et al. Elevated levels of circulating DNA and chromatin are independently associated with severe coronary atherosclerosis and a prothrombotic state. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 2032–2040. [Google Scholar] [CrossRef]
- van Montfoort, M.L.; Stephan, F.; Lauw, M.N.; Hutten, B.A.; Van Mierlo, G.J.; Solati, S.; Middeldorp, S.; Meijers, J.C.; Zeerleder, S. Circulating nucleosomes and neutrophil activation as risk factors for deep vein thrombosis. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 147–151. [Google Scholar] [CrossRef]
- Kremers, B.M.M.; Birocchi, S.; van Oerle, R.; Zeerleder, S.; Spronk, H.M.H.; Mees, B.M.E.; Luken, B.M.; Ten Cate, H.; Ten Cate-Hoek, A.J. Searching for a Common Thrombo-Inflammatory Basis in Patients With Deep Vein Thrombosis or Peripheral Artery Disease. Front. Cardiovasc. Med. 2019, 6, 33. [Google Scholar] [CrossRef]
- Li, T.; Peng, R.; Wang, F.; Hua, L.; Liu, S.; Han, Z.; Pei, J.; Pei, S.; Zhao, Z.; Jiang, X.; et al. Lysophosphatidic acid promotes thrombus stability by inducing rapid formation of neutrophil extracellular traps: A new mechanism of thrombosis. J. Thromb. Haemost. 2020, 18, 1952–1964. [Google Scholar] [CrossRef] [PubMed]
- Buso, G.; Faggin, E.; Rosenblatt-Velin, N.; Pellegrin, M.; Galliazzo, S.; Calanca, L.; Rattazzi, M.; Mazzolai, L. The Role of Neutrophils in Lower Limb Peripheral Artery Disease: State of the Art and Future Perspectives. Int. J. Mol. Sci. 2023, 24, 1169. [Google Scholar] [CrossRef] [PubMed]
- Aboyans, V.; Ricco, J.B.; Bartelink, M.E.L.; Bjorck, M.; Brodmann, M.; Cohnert, T.; Collet, J.P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteriesEndorsed by: The European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur. Heart J. 2018, 39, 763–816. [Google Scholar] [CrossRef] [PubMed]
- Daugherty, A.; Dunn, J.L.; Rateri, D.L.; Heinecke, J.W. Myeloperoxidase, a catalyst for lipoprotein oxidation, is expressed in human atherosclerotic lesions. J. Clin. Investig. 1994, 94, 437–444. [Google Scholar] [CrossRef]
- Sugiyama, S.; Okada, Y.; Sukhova, G.K.; Virmani, R.; Heinecke, J.W.; Libby, P. Macrophage myeloperoxidase regulation by granulocyte macrophage colony-stimulating factor in human atherosclerosis and implications in acute coronary syndromes. Am. J. Pathol. 2001, 158, 879–891. [Google Scholar] [CrossRef] [PubMed]
- Kutter, D.; Devaquet, P.; Vanderstocken, G.; Paulus, J.M.; Marchal, V.; Gothot, A. Consequences of total and subtotal myeloperoxidase deficiency: Risk or benefit ? Acta Haematol. 2000, 104, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Asselbergs, F.W.; Reynolds, W.F.; Cohen-Tervaert, J.W.; Jessurun, G.A.; Tio, R.A. Myeloperoxidase polymorphism related to cardiovascular events in coronary artery disease. Am. J. Med. 2004, 116, 429–430. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Brennan, M.L.; Fu, X.; Aviles, R.J.; Pearce, G.L.; Penn, M.S.; Topol, E.J.; Sprecher, D.L.; Hazen, S.L. Association between myeloperoxidase levels and risk of coronary artery disease. JAMA 2001, 286, 2136–2142. [Google Scholar] [CrossRef] [PubMed]
- Buffon, A.; Biasucci, L.M.; Liuzzo, G.; D’Onofrio, G.; Crea, F.; Maseri, A. Widespread coronary inflammation in unstable angina. N. Engl. J. Med. 2002, 347, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Cheng, M.; Cheng, M.; Wei, Q. Association of myeloperoxidase, homocysteine and high-sensitivity C-reactive protein with the severity of coronary artery disease and their diagnostic and prognostic value. Exp. Ther. Med. 2020, 20, 1532–1540. [Google Scholar] [CrossRef]
- Brennan, M.L.; Penn, M.S.; Van Lente, F.; Nambi, V.; Shishehbor, M.H.; Aviles, R.J.; Goormastic, M.; Pepoy, M.L.; McErlean, E.S.; Topol, E.J.; et al. Prognostic value of myeloperoxidase in patients with chest pain. N. Engl. J. Med. 2003, 349, 1595–1604. [Google Scholar] [CrossRef] [PubMed]
- Weihrauch, D.; Martin, D.P.; Jones, D.; Krolikowski, J.; Struve, J.; Naylor, S.; Pritchard, K.A., Jr. Inhibition of myeloperoxidase increases revascularization and improves blood flow in a diabetic mouse model of hindlimb ischaemia. Diab. Vasc. Dis. Res. 2020, 17, 1479164120907971. [Google Scholar] [CrossRef]
- Schiano, V.; Laurenzano, E.; Brevetti, G.; De Maio, J.I.; Lanero, S.; Scopacasa, F.; Chiariello, M. Omega-3 polyunsaturated fatty acid in peripheral arterial disease: Effect on lipid pattern, disease severity, inflammation profile, and endothelial function. Clin. Nutr. 2008, 27, 241–247. [Google Scholar] [CrossRef]
- Schahab, N.; Mansuroglu, S.; Schaefer, C.; Fimmers, R.; Nickenig, G.; Tiyerili, V. Prognostic value of myeloperoxidase in patients with peripheral artery disease. Vascular 2021, 29, 363–371. [Google Scholar] [CrossRef]
- Faurschou, M.; Borregaard, N. Neutrophil granules and secretory vesicles in inflammation. Microbes Infect. 2003, 5, 1317–1327. [Google Scholar] [CrossRef]
- Polverino, E.; Rosales-Mayor, E.; Dale, G.E.; Dembowsky, K.; Torres, A. The Role of Neutrophil Elastase Inhibitors in Lung Diseases. Chest 2017, 152, 249–262. [Google Scholar] [CrossRef]
- Bell, D.; Jackson, M.; Nicoll, J.J.; Millar, A.; Dawes, J.; Muir, A.L. Inflammatory response, neutrophil activation, and free radical production after acute myocardial infarction: Effect of thrombolytic treatment. Br. Heart J. 1990, 63, 82–87. [Google Scholar] [CrossRef]
- Ogura, Y.; Tajiri, K.; Murakoshi, N.; Xu, D.; Yonebayashi, S.; Li, S.; Okabe, Y.; Feng, D.; Shimoda, Y.; Song, Z.; et al. Neutrophil Elastase Deficiency Ameliorates Myocardial Injury Post Myocardial Infarction in Mice. Int. J. Mol. Sci. 2021, 22, 722. [Google Scholar] [CrossRef]
- Jorch, S.K.; Kubes, P. An emerging role for neutrophil extracellular traps in noninfectious disease. Nat. Med. 2017, 23, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Franck, G.; Mawson, T.L.; Folco, E.J.; Molinaro, R.; Ruvkun, V.; Engelbertsen, D.; Liu, X.; Tesmenitsky, Y.; Shvartz, E.; Sukhova, G.K.; et al. Roles of PAD4 and NETosis in Experimental Atherosclerosis and Arterial Injury: Implications for Superficial Erosion. Circ. Res. 2018, 123, 33–42. [Google Scholar] [CrossRef]
- Ge, L.; Zhou, X.; Ji, W.J.; Lu, R.Y.; Zhang, Y.; Zhang, Y.D.; Ma, Y.Q.; Zhao, J.H.; Li, Y.M. Neutrophil extracellular traps in ischemia-reperfusion injury-induced myocardial no-reflow: Therapeutic potential of DNase-based reperfusion strategy. Am. J. Physiol. Heart Circ. Physiol. 2015, 308, H500–H509. [Google Scholar] [CrossRef] [PubMed]
- Savchenko, A.S.; Borissoff, J.I.; Martinod, K.; De Meyer, S.F.; Gallant, M.; Erpenbeck, L.; Brill, A.; Wang, Y.; Wagner, D.D. VWF-mediated leukocyte recruitment with chromatin decondensation by PAD4 increases myocardial ischemia/reperfusion injury in mice. Blood 2014, 123, 141–148. [Google Scholar] [CrossRef]
- Mangold, A.; Alias, S.; Scherz, T.; Hofbauer, M.; Jakowitsch, J.; Panzenbock, A.; Simon, D.; Laimer, D.; Bangert, C.; Kammerlander, A.; et al. Coronary neutrophil extracellular trap burden and deoxyribonuclease activity in ST-elevation acute coronary syndrome are predictors of ST-segment resolution and infarct size. Circ. Res. 2015, 116, 1182–1192. [Google Scholar] [CrossRef]
- Fadini, G.P.; Menegazzo, L.; Rigato, M.; Scattolini, V.; Poncina, N.; Bruttocao, A.; Ciciliot, S.; Mammano, F.; Ciubotaru, C.D.; Brocco, E.; et al. NETosis Delays Diabetic Wound Healing in Mice and Humans. Diabetes 2016, 65, 1061–1071. [Google Scholar] [CrossRef] [PubMed]
- Demyanets, S.; Stojkovic, S.; Mauracher, L.M.; Kopp, C.W.; Wojta, J.; Thaler, J.; Panzer, S.; Gremmel, T. Surrogate Markers of Neutrophil Extracellular Trap Formation are Associated with Ischemic Outcomes and Platelet Activation after Peripheral Angioplasty and Stenting. J. Clin. Med. 2020, 9, 304. [Google Scholar] [CrossRef]
- Brinkmann, V.; Reichard, U.; Goosmann, C.; Fauler, B.; Uhlemann, Y.; Weiss, D.S.; Weinrauch, Y.; Zychlinsky, A. Neutrophil extracellular traps kill bacteria. Science 2004, 303, 1532–1535. [Google Scholar] [CrossRef] [PubMed]
- Sollberger, G.; Tilley, D.O.; Zychlinsky, A. Neutrophil Extracellular Traps: The Biology of Chromatin Externalization. Dev. Cell 2018, 44, 542–553. [Google Scholar] [CrossRef] [PubMed]
- Silvain, J.; Collet, J.P.; Nagaswami, C.; Beygui, F.; Edmondson, K.E.; Bellemain-Appaix, A.; Cayla, G.; Pena, A.; Brugier, D.; Barthelemy, O.; et al. Composition of coronary thrombus in acute myocardial infarction. J. Am. Coll. Cardiol. 2011, 57, 1359–1367. [Google Scholar] [CrossRef]
- Jimenez-Alcazar, M.; Kim, N.; Fuchs, T.A. Circulating Extracellular DNA: Cause or Consequence of Thrombosis? Semin. Thromb. Hemost. 2017, 43, 553–561. [Google Scholar] [CrossRef] [PubMed]
- Helseth, R.; Shetelig, C.; Andersen, G.O.; Langseth, M.S.; Limalanathan, S.; Opstad, T.B.; Arnesen, H.; Hoffmann, P.; Eritsland, J.; Seljeflot, I. Neutrophil Extracellular Trap Components Associate with Infarct Size, Ventricular Function, and Clinical Outcome in STEMI. Mediat. Inflamm. 2019, 2019, 7816491. [Google Scholar] [CrossRef] [PubMed]
- Davignon, J. Beneficial cardiovascular pleiotropic effects of statins. Circulation 2004, 109, III39–III43. [Google Scholar] [CrossRef] [PubMed]
- Radbakhsh, S.; Kovanen, P.T.; Sahebkar, A. Regulating NETosis: An emerging facet of statin pleiotropy. Drug Discov. Today 2022, 27, 675–677. [Google Scholar] [CrossRef] [PubMed]
- Sapey, E.; Patel, J.M.; Greenwood, H.; Walton, G.M.; Grudzinska, F.; Parekh, D.; Mahida, R.Y.; Dancer, R.C.A.; Lugg, S.T.; Howells, P.A.; et al. Simvastatin Improves Neutrophil Function and Clinical Outcomes in Pneumonia. A Pilot Randomized Controlled Clinical Trial. Am. J. Respir. Crit. Care Med. 2019, 200, 1282–1293. [Google Scholar] [CrossRef]
- Eilenberg, W.; Stojkovic, S.; Kaider, A.; Kozakowski, N.; Domenig, C.M.; Burghuber, C.; Nanobachvili, J.; Huber, K.; Klinger, M.; Neumayer, C.; et al. NGAL and MMP-9/NGAL as biomarkers of plaque vulnerability and targets of statins in patients with carotid atherosclerosis. Clin. Chem. Lab. Med. 2017, 56, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Lenglet, S.; Quercioli, A.; Fabre, M.; Galan, K.; Pelli, G.; Nencioni, A.; Bauer, I.; Pende, A.; Python, M.; Bertolotto, M.; et al. Statin treatment is associated with reduction in serum levels of receptor activator of NF-kappaB ligand and neutrophil activation in patients with severe carotid stenosis. Mediat. Inflamm. 2014, 2014, 720987. [Google Scholar] [CrossRef] [PubMed]
- Ali, Z.; Sarcia, P.; Mosley, T.H., Jr.; Kondragunta, V.; Kullo, I.J. Association of serum myeloperoxidase with the ankle-brachial index and peripheral arterial disease. Vasc. Med. 2009, 14, 215–220. [Google Scholar] [CrossRef]
- Leng, G.C.; Lee, A.J.; Fowkes, F.G.; Whiteman, M.; Dunbar, J.; Housley, E.; Ruckley, C.V. Incidence, natural history and cardiovascular events in symptomatic and asymptomatic peripheral arterial disease in the general population. Int. J. Epidemiol. 1996, 25, 1172–1181. [Google Scholar] [CrossRef] [PubMed]
- Frank, U.; Nikol, S.; Belch, J.; Boc, V.; Brodmann, M.; Carpentier, P.H.; Chraim, A.; Canning, C.; Dimakakos, E.; Gottsäter, A.; et al. ESVM Guideline on peripheral arterial disease. Vasa 2019, 48, 1–79. [Google Scholar] [CrossRef] [PubMed]
- Treat-Jacobson, D.; McDermott, M.M.; Bronas, U.G.; Campia, U.; Collins, T.C.; Criqui, M.H.; Gardner, A.W.; Hiatt, W.R.; Regensteiner, J.G.; Rich, K.; et al. Optimal Exercise Programs for Patients With Peripheral Artery Disease: A Scientific Statement From the American Heart Association. Circulation 2019, 139, e10–e33. [Google Scholar] [CrossRef]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. American Thoracic Society. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Van Bortel, L.M.; Laurent, S.; Boutouyrie, P.; Chowienczyk, P.; Cruickshank, J.; De Backer, T.; Filipovsky, J.; Huybrechts, S.; Mattace-Raso, F.U.; Protogerou, A.; et al. Expert consensus document on the measurement of aortic stiffness in daily practice using carotid-femoral pulse wave velocity. J. Hypertens. 2012, 30, 445–448. [Google Scholar] [CrossRef] [PubMed]
- Thijssen, D.H.J.; Bruno, R.M.; Van Mil, A.C.C.M.; Holder, S.M.; Faita, F.; Greyling, A.; Zock, P.L.; Taddei, S.; Deanfield, J.E.; Luscher, T.; et al. Expert consensus and evidence-based recommendations for the assessment of flow-mediated dilation in humans. Eur. Hear. J. 2019, 40, 2534–2547. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| All Subjects (=110) | PAD (=66) | No PAD (=44) | p | |
|---|---|---|---|---|
| Clinical characteristics | ||||
| Sex (male) (%) | 77 (70.0) | 45 (68.2) | 32 (72.7) | 0.766 |
| Age (years) (±SD) | 59.1 (11.0) | 64.2 (8.9) | 51.3 (8.9) | <0.001 |
| BMI (kg/m2) (±SD) | 27.3 (5.0) | 27.0 (5.2) | 27.7 (4.7) | 0.287 |
| Waist (cm) (±SD) | 99.1 (14.7) | 100.0 (15.9) | 97.9 (12.8) | 0.918 |
| Comorbidities | ||||
| Obesity (%) | 24 (21.8) | 14 (21.2) | 10 (22.7) | 1.000 |
| Diabetes (%) | 26 (23.9) | 24 (36.4) | 2 (4.7) | <0.001 |
| Active smoking (%) | 47 (42.7) | 34 (51.5) | 13 (29.5) | 0.037 |
| Hypertension (%) | 64 (58.2) | 46 (69.7) | 18 (40.9) | 0.003 |
| Family history of CV events (%) | 45 (42.5) | 25 (40.3) | 20 (45.5) | 0.691 |
| Baseline treatment | ||||
| Antihypertensive (%) | 64 (58.2) | 52 (78.8) | 12 (27.3) | <0.001 |
| Antiplatelet (%) | 58 (52.7) | 58 (87.9) | - | - |
| Statin (%) | 60 (54.5) | 57 (86.4) | 3 (6.8) | <0.001 |
| Laboratory parameters | ||||
| Creatinine (mg/dl) (±SD) | 0.95 (0.32) | 1.02 (0.38) | 0.86 (0.17) | 0.106 |
| GFR (ml/min/1.73 m2) (±SD) | 79.63 (22.21) | 77.72 (23.15) | 82.28 (20.83) | 0.843 |
| Total cholesterol (mg/dl) (±SD) | 182.13 (40.39) | 167.25 (31.76) | 203 (42.11) | <0.001 |
| LDL cholesterol (mg/dl) (±SD) | 104.78 (37.68) | 87.11 (28.73) | 128.89 (35.19) | <0.001 |
| HDL cholesterol (mg/dl) (±SD) | 51.74 (28.28) | 50.95 (18.37) | 52.91 (38.86) | 0.215 |
| Triglycerides (mg/dl) (±SD) | 156.20 (86.65) | 152.91 (90.02) | 160.91 (82.37) | 0.229 |
| Markers of neutrophil activation | ||||
| PMN-elastase (ng/mL) (±SD) | 187.57 (163.91) | 235.64 (182.03) | 113.78 (92.75) | <0.001 |
| NGAL (ng/mL) (±SD) | 162.47 (150.19) | 210.16 (175.46) | 89.30 (36.08) | <0.001 |
| MPO (ng/mL) (±SD) | 83.16 (70.88) | 105.15 (75.27) | 49.12 (46.81) | <0.001 |
| MPO–DNA (abs 405–490) (±SD) | 0.257 (0.110) | 0.275 (0.131) | 0.231 (0.063) | 0.241 |
| All Subjects (=63) | No Outcome (=52) | MACE and/or MALE (=11) | p | All Subjects (=49) | No Outcome (=35) | ABI Reduction ≥ 0.15 a (=14) | p | All Subjects (=40) | No Outcome (=30) | 6MWD Reduction ≥ 20 m (=10) | p | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PMN-elastase (ng/mL) (±SD) | 240.39 (184.79) | 227.27 (182.83) | 302.37 (190.04) | 0.128 | 204.88 (106.44) | 206.67 (112.93) | 201.19 (91.76) | 0.765 | 207.21 (104.35) | 215.20 (114.12) | 183.25 (66.11) | 0.508 |
| NGAL (ng/mL) (±SD) | 207.94 (178.06) | 188.69 (97.55) | 298.93 (370.14) | 0.269 | 182.56 (99.35) | 173.18 (81.74) | 201.91 (136.76) | 0.609 | 176.47 (83.71) | 181.71 (89.55) | 160.74 (64.46) | 0.634 |
| MPO (ng/mL) (±SD) | 106.85 (76.14) | 98.52 (74.83) | 150.17 (71.26) | 0.020 | 98.25 (74.69) | 90.54 (61.48) | 114.14 (97.18) | 0.406 | 95.28 (62.70) | 94.85 (58.66) | 96.58 (77.10) | 0.794 |
| MPO–DNA (abs 405–490) (±SD) | 0.275 (0.133) | 0.256 (0.126) | 0.362 (0.132) | 0.014 | 0.250 (0.114) | 0.262 (0.105) | 0.227 (0.129) | 0.209 | 0.246 (0.126) | 0.252 (0.124) | 0.230 (0.135) | 0.528 |
| MACE and/or MALE | ABI reduction ≥ 0.15 or TBI reduction ≥ 0.1 | 6MWD reduction ≥ 20 m | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariable Analyses | Multivariable Analyses a | Univariable Analyses | Univariable Analyses | |||||||||
| HR | 95%CI | p | HR | 95%CI | p | HR | 95%CI | p | HR | 95%CI | p | |
| PMN-elastase (ng/mL) (±SD) | 1.003 | 1.000–1.007 | 0.077 | 1.010 | 1.000–1.020 | 0.040 | 1.000 | 0.994–1.005 | 0.864 | 0.997 | 0.989–1.004 | 0.400 |
| NGAL (ng/mL) (±SD) | 1.001 | 0.999–1.003 | 0.358 | - | 1.003 | 0.997–1.009 | 0.354 | 0.996 | 0.987–1.007 | 0.996 | ||
| MPO (ng/mL) (±SD) | 1.027 | 1.004–1.051 | 0.019 | 1.027 | 1.004–1.051 | 0.019 | 1.004 | 0.996–1.012 | 0.311 | 1.000 | 0.989–1.012 | 0.939 |
| MPO–DNA (abs 405–490) (±SD) | 0.960 * | 0.904–1.019 | 0.178 | - | 0.971 * | 0.915–1.030 | 0.324 | 0.985 * | 0.926–1.048 | 0.640 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buso, G.; Faggin, E.; Bressan, A.; Galliazzo, S.; Cinetto, F.; Felice, C.; Fusaro, M.; Erdmann, A.; Pauletto, P.; Rattazzi, M.; et al. Biomarkers of Neutrophil Activation in Patients with Symptomatic Chronic Peripheral Artery Disease Predict Worse Cardiovascular Outcome. Biomedicines 2023, 11, 866. https://doi.org/10.3390/biomedicines11030866
Buso G, Faggin E, Bressan A, Galliazzo S, Cinetto F, Felice C, Fusaro M, Erdmann A, Pauletto P, Rattazzi M, et al. Biomarkers of Neutrophil Activation in Patients with Symptomatic Chronic Peripheral Artery Disease Predict Worse Cardiovascular Outcome. Biomedicines. 2023; 11(3):866. https://doi.org/10.3390/biomedicines11030866
Chicago/Turabian StyleBuso, Giacomo, Elisabetta Faggin, Alessandro Bressan, Silvia Galliazzo, Francesco Cinetto, Carla Felice, Michele Fusaro, Andreas Erdmann, Paolo Pauletto, Marcello Rattazzi, and et al. 2023. "Biomarkers of Neutrophil Activation in Patients with Symptomatic Chronic Peripheral Artery Disease Predict Worse Cardiovascular Outcome" Biomedicines 11, no. 3: 866. https://doi.org/10.3390/biomedicines11030866