
Inflammatory Blood Signature Related to Common Psychological Comorbidity in Chronic Pain
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
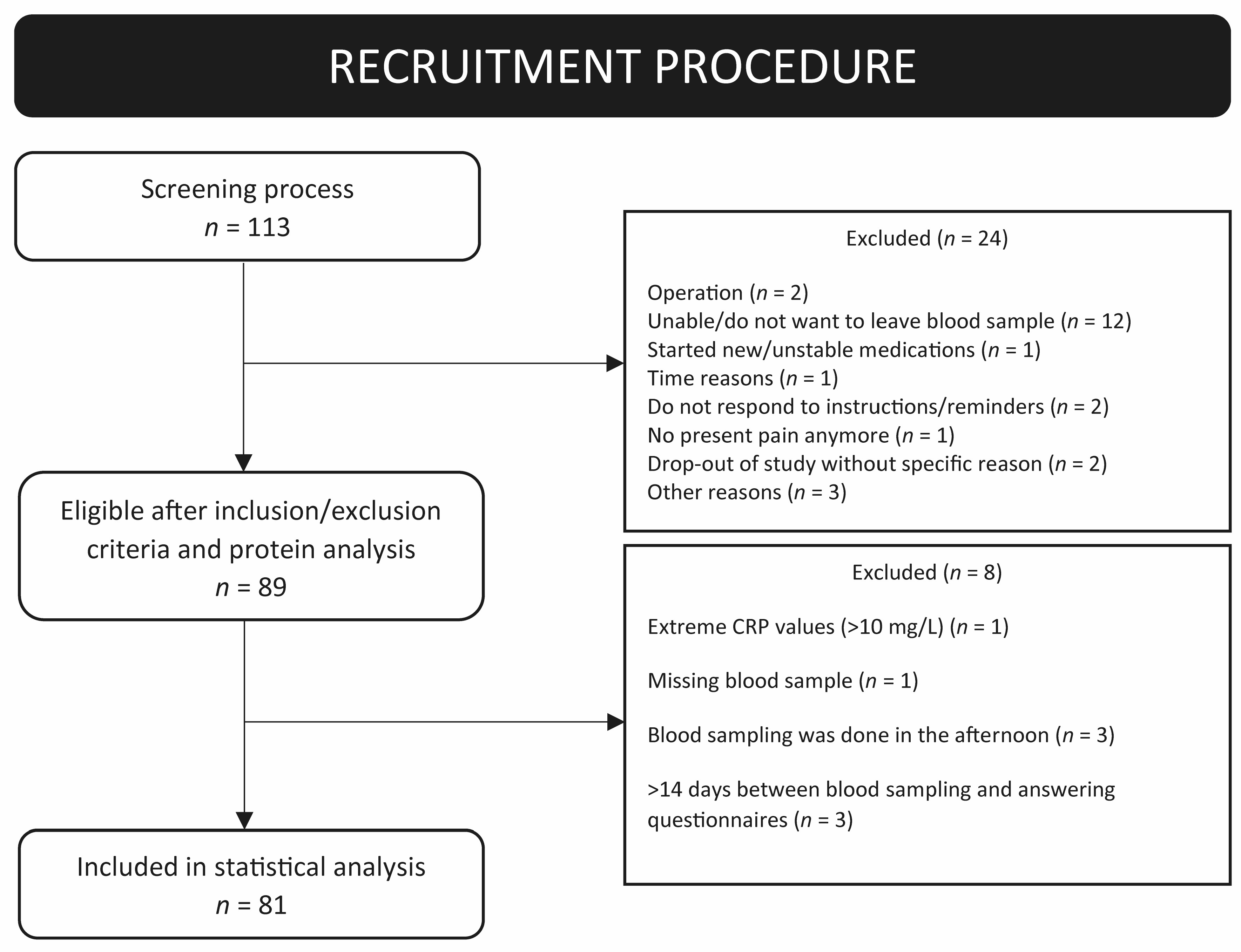
2.1. Study Participants and Procedure
2.2. Patient-Reported Outcomes (PROMs)
2.2.1. Anthropometric Parameters
2.2.2. Pain Parameters
2.2.3. Psychological Parameters
2.2.4. Other Clinical Parameters
2.3. Blood Sampling
2.4. Inflammatory Cytokine Panel Analysis
2.5. Statistical Analysis
2.5.1. Principal Component Analysis (PCA)
2.5.2. Orthogonal Partial Least Square Analysis (OPLS)
2.5.3. Orthogonal Partial Least Squares Discriminant Analysis (OPLS-DA)
3. Results
3.1. Cohort Characteristics
3.2. PCA Investigating Patient Subgroups Based on Inflammatory Protein Profile
3.3. Correlation of Inflammatory Proteins with Pain Intensity, Psychological Comorbidity, and Age
3.4. Inflammation and Age in Chronic Pain
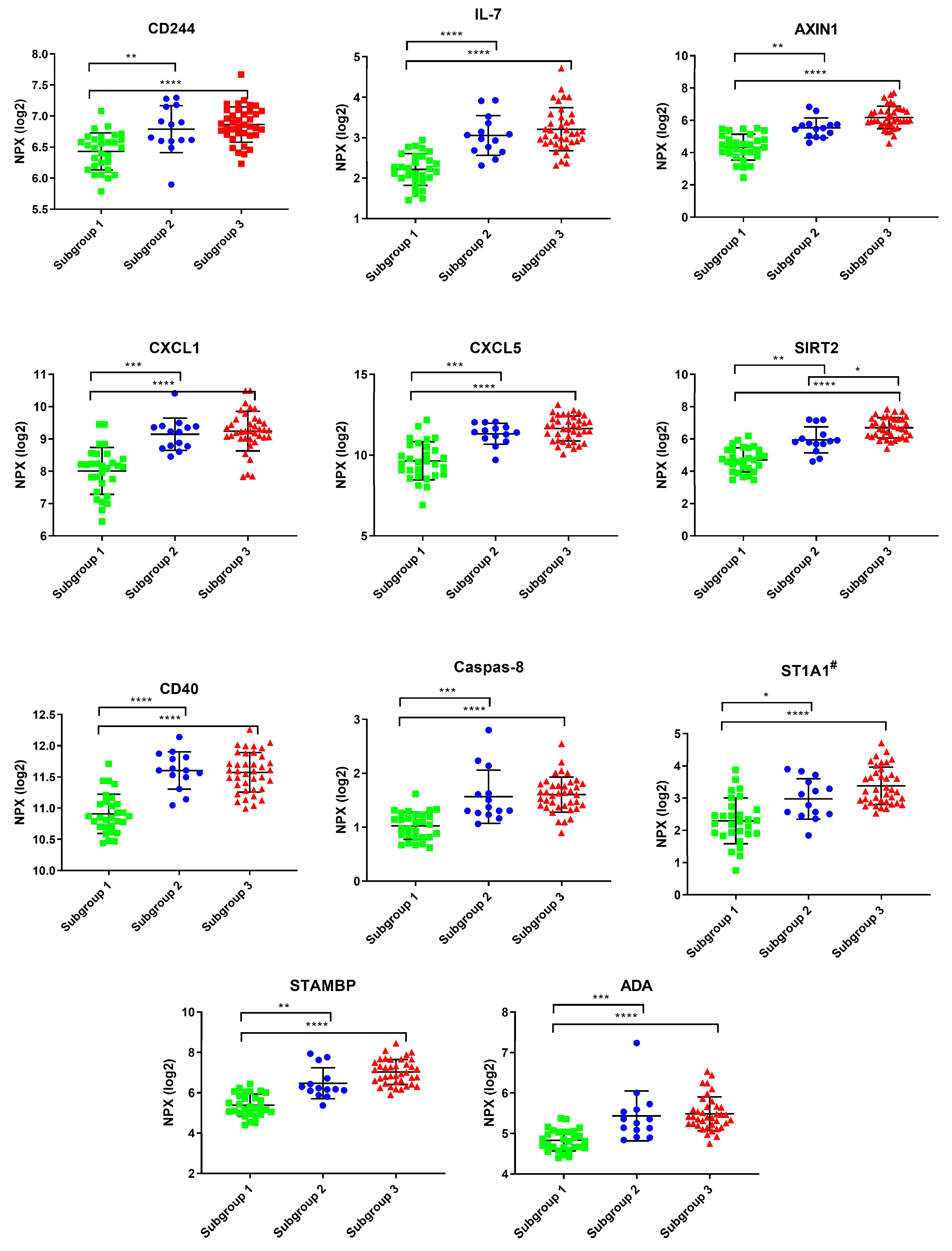
3.5. OPLS-DA Modeling of Chronic Pain Patients with a Higher Psychiatric Profile (Anxiety or Depression) Versus Chronic Pain Patients with no Psychiatric Comorbidity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Karshikoff, B.; Tadros, M.A.; Mackey, S.; Zouikr, I. Neuroimmune modulation of pain across the developmental spectrum. Curr. Opin. Behav. Sci. 2019, 28, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Grace, P.M.; Hutchinson, M.R.; Maier, S.F.; Watkins, L.R. Pathological pain and the neuroimmune interface. Nat. Rev. Immunol. 2014, 14, 217–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burke, N.N.; Finn, D.P.; Roche, M. Neuroinflammatory Mechanisms Linking Pain and Depression. Mod. Trends. Pharm. 2015, 30, 36–50. [Google Scholar] [CrossRef] [Green Version]
- Walker, A.K.; Kavelaars, A.; Heijnen, C.J.; Dantzer, R. Neuroinflammation and comorbidity of pain and depression. Pharmacol. Rev. 2014, 66, 80–101. [Google Scholar] [CrossRef] [Green Version]
- Cohen, S.P.; Vase, L.; Hooten, W.M. Chronic pain: An update on burden, best practices, and new advances. Lancet 2021, 397, 2082–2097. [Google Scholar] [CrossRef]
- Raja, S.N.; Carr, D.B.; Cohen, M.; Finnerup, N.B.; Flor, H.; Gibson, S.; Keefe, F.J.; Mogil, J.S.; Ringkamp, M.; Sluka, K.A.; et al. The revised International Association for the Study of Pain definition of pain: Concepts, challenges, and compromises. Pain 2020, 161, 1976–1982. [Google Scholar] [CrossRef]
- Mills, S.E.E.; Nicolson, K.P.; Smith, B.H. Chronic pain: A review of its epidemiology and associated factors in population-based studies. Br. J. Anaesth. 2019, 123, e273–e283. [Google Scholar] [CrossRef]
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef]
- Chavan, S.S.; Pavlov, V.A.; Tracey, K.J. Mechanisms and Therapeutic Relevance of Neuro-immune Communication. Immunity 2017, 46, 927–942. [Google Scholar] [CrossRef] [Green Version]
- Baral, P.; Udit, S.; Chiu, I.M. Pain and immunity: Implications for host defence. Nat. Rev. Immunol. 2019, 19, 433–447. [Google Scholar] [CrossRef]
- Haroon, E.; Raison, C.L.; Miller, A.H. Psychoneuroimmunology meets neuropsychopharmacology: Translational implications of the impact of inflammation on behavior. Neuropsychopharmacol. Off. Publ. Am. Coll. Neuropsychopharmacol. 2012, 37, 137–162. [Google Scholar] [CrossRef]
- Sorge, R.E.; Totsch, S.K. Sex Differences in Pain. J. Neurosci. Res. 2017, 95, 1271–1281. [Google Scholar] [CrossRef]
- Rosen, S.; Ham, B.; Mogil, J.S. Sex differences in neuroimmunity and pain. J. Neurosci. Res. 2017, 95, 500–508. [Google Scholar] [CrossRef]
- Harth, M.; Nielson, W.R. Pain and affective distress in arthritis: Relationship to immunity and inflammation. Expert. Rev. Clin. Immunol. 2019, 15, 541–552. [Google Scholar] [CrossRef]
- Khan, A.N.; Jacobsen, H.E.; Khan, J.; Filippi, C.G.; Levine, M.; Lehman, R.A., Jr.; Riew, K.D.; Lenke, L.G.; Chahine, N.O. Inflammatory biomarkers of low back pain and disc degeneration: A review. Ann. N. Y. Acad. Sci. 2017, 1410, 68–84. [Google Scholar] [CrossRef]
- Talwar, S.; Munson, P.J.; Barb, J.; Fiuza, C.; Cintron, A.P.; Logun, C.; Tropea, M.; Khan, S.; Reda, D.; Shelhamer, J.H.; et al. Gene expression profiles of peripheral blood leukocytes after endotoxin challenge in humans. Physiol. Genom. 2006, 25, 203–215. [Google Scholar] [CrossRef]
- Li, W.; Gong, Y.; Liu, J.; Guo, Y.; Tang, H.; Qin, S.; Zhao, Y.; Wang, S.; Xu, Z.; Chen, B. Peripheral and Central Pathological Mechanisms of Chronic Low Back Pain: A Narrative Review. J. Pain Res. 2021, 14, 1483–1494. [Google Scholar] [CrossRef]
- Ng, Q.X.; Soh, A.Y.S.; Loke, W.; Lim, D.Y.; Yeo, W.S. The role of inflammation in irritable bowel syndrome (IBS). J. Inflamm. Res. 2018, 11, 345–349. [Google Scholar] [CrossRef] [Green Version]
- Felger, J.C.; Haroon, E.; Patel, T.A.; Goldsmith, D.R.; Wommack, E.C.; Woolwine, B.J.; Le, N.A.; Feinberg, R.; Tansey, M.G.; Miller, A.H. What does plasma CRP tell us about peripheral and central inflammation in depression? Mol. Psychiatry 2018, 25, 1301–1311. [Google Scholar] [CrossRef]
- Harsanyi, S.; Kupcova, I.; Danisovic, L.; Klein, M. Selected Biomarkers of Depression: What Are the Effects of Cytokines and Inflammation? Int. J. Mol. Sci. 2022, 24, 578. [Google Scholar] [CrossRef]
- Osimo, E.F.; Pillinger, T.; Rodriguez, I.M.; Khandaker, G.M.; Pariante, C.M.; Howes, O.D. Inflammatory markers in depression: A meta-analysis of mean differences and variability in 5,166 patients and 5,083 controls. Brain Behav. Immun. 2020, 87, 901–909. [Google Scholar] [CrossRef] [PubMed]
- Slavich, G.M.; Sacher, J. Stress, sex hormones, inflammation, and major depressive disorder: Extending Social Signal Transduction Theory of Depression to account for sex differences in mood disorders. Psychopharmacology 2019, 236, 3063–3079. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Varela, D.; Barry, A.M.; Schmidt, M. Proteome-based systems biology in chronic pain. J. Proteom. 2019, 190, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Backryd, E.; Themistocleous, A.; Larsson, A.; Gordh, T.; Rice, A.S.C.; Tesfaye, S.; Bennett, D.L.; Gerdle, B. Hepatocyte growth factor, colony-stimulating factor 1, CD40, and 11 other inflammation-related proteins are associated with pain in diabetic neuropathy: Exploration and replication serum data from the Pain in Neuropathy Study. Pain 2022, 163, 897–909. [Google Scholar] [CrossRef] [PubMed]
- Ernberg, M.; Jasim, H.; Wåhlén, K.; Ghafouri, B. Altered Plasma Proteins in Myogenous Temporomandibular Disorders. J. Clin. Med. 2022, 11, 2777. [Google Scholar] [CrossRef]
- Han, C.L.; Sheng, Y.C.; Wang, S.Y.; Chen, Y.H.; Kang, J.H. Serum proteome profiles revealed dysregulated proteins and mechanisms associated with fibromyalgia syndrome in women. Sci. Rep. 2020, 10, 12347. [Google Scholar] [CrossRef]
- Hsu, W.H.; Han, D.S.; Ku, W.C.; Chao, Y.M.; Chen, C.C.; Lin, Y.L. Metabolomic and proteomic characterization of sng and pain phenotypes in fibromyalgia. Eur. J. Pain 2022, 26, 445–462. [Google Scholar] [CrossRef]
- Jonsson, M.; Gerdle, B.; Ghafouri, B.; Backryd, E. The inflammatory profile of cerebrospinal fluid, plasma, and saliva from patients with severe neuropathic pain and healthy controls-a pilot study. BMC Neurosci. 2021, 22, 6. [Google Scholar] [CrossRef]
- Khoonsari, P.E.; Musunri, S.; Herman, S.; Svensson, C.I.; Tanum, L.; Gordh, T.; Kultima, K. Systematic analysis of the cerebrospinal fluid proteome of fibromyalgia patients. J. Proteom. 2018, 190, 35–43. [Google Scholar] [CrossRef]
- Olausson, P.; Ghafouri, B.; Backryd, E.; Gerdle, B. Clear differences in cerebrospinal fluid proteome between women with chronic widespread pain and healthy women—A multivariate explorative cross-sectional study. J. Pain Res. 2017, 10, 575–590. [Google Scholar] [CrossRef] [Green Version]
- Ramirez-Tejero, J.A.; Martinez-Lara, E.; Rus, A.; Camacho, M.V.; Del Moral, M.L.; Siles, E. Insight into the biological pathways underlying fibromyalgia by a proteomic approach. J. Proteom. 2018, 186, 47–55. [Google Scholar] [CrossRef]
- Wåhlén, K.; Ernberg, M.; Kosek, E.; Mannerkorpi, K.; Gerdle, B.; Ghafouri, B. Significant correlation between plasma proteome profile and pain intensity, sensitivity, and psychological distress in women with fibromyalgia. Sci. Rep. 2020, 10, 12508. [Google Scholar] [CrossRef]
- Wåhlén, K.; Olausson, P.; Carlsson, A.; Ghafouri, N.; Gerdle, B.; Ghafouri, B. Systemic alterations in plasma proteins from women with chronic widespread pain compared to healthy controls: A proteomic study. J. Pain Res. 2017, 10, 797–809. [Google Scholar] [CrossRef] [Green Version]
- Backryd, E.; Edstrom, S.; Gerdle, B.; Ghafouri, B. Do fragments and glycosylated isoforms of alpha-1-antitrypsin in CSF mirror spinal pathophysiological mechanisms in chronic peripheral neuropathic pain? An exploratory, discovery phase study. BMC Neurol. 2018, 18, 116. [Google Scholar] [CrossRef] [Green Version]
- Ciregia, F.; Giacomelli, C.; Giusti, L.; Boldrini, C.; Piga, I.; Pepe, P.; Consensi, A.; Gori, S.; Lucacchini, A.; Mazzoni, M.R.; et al. Putative salivary biomarkers useful to differentiate patients with fibromyalgia. J. Proteom. 2019, 190, 44–54. [Google Scholar] [CrossRef]
- Lim, T.K.Y.; Anderson, K.M.; Hari, P.; Di Falco, M.; Reihsen, T.E.; Wilcox, G.L.; Belani, K.G.; LaBoissiere, S.; Pinto, M.R.; Beebe, D.S.; et al. Evidence for a Role of Nerve Injury in Painful Intervertebral Disc Degeneration: A Cross-Sectional Proteomic Analysis of Human Cerebrospinal Fluid. J. Pain 2017, 18, 1253–1269. [Google Scholar] [CrossRef]
- Olausson, P.; Ghafouri, B.; Ghafouri, N.; Gerdle, B. Specific proteins of the trapezius muscle correlate with pain intensity and sensitivity—An explorative multivariate proteomic study of the trapezius muscle in women with chronic widespread pain. J. Pain Res. 2016, 9, 345–356. [Google Scholar] [CrossRef] [Green Version]
- Wåhlén, K.; Ghafouri, B.; Ghafouri, N.; Gerdle, B. Plasma Protein Pattern Correlates With Pain Intensity and Psychological Distress in Women With Chronic Widespread Pain. Front. Psychol. 2018, 9, 2400. [Google Scholar] [CrossRef] [Green Version]
- Gerdle, B.; Wåhlén, K.; Ghafouri, B. Plasma protein patterns are strongly correlated with pressure pain thresholds in women with chronic widespread pain and in healthy controls-an exploratory case-control study. Medicine 2020, 99, e20497. [Google Scholar] [CrossRef]
- Lasselin, J.; Elsenbruch, S.; Lekander, M.; Axelsson, J.; Karshikoff, B.; Grigoleit, J.S.; Engler, H.; Schedlowski, M.; Benson, S. Mood disturbance during experimental endotoxemia: Predictors of state anxiety as a psychological component of sickness behavior. Brain Behav. Immun. 2016, 57, 30–37. [Google Scholar] [CrossRef]
- Lasselin, J.; Lekander, M.; Axelsson, J.; Karshikoff, B. Sex differences in how inflammation affects behavior: What we can learn from experimental inflammatory models in humans. Front. Neuroendocrinol. 2018, 50, 91–106. [Google Scholar] [CrossRef] [PubMed]
- Lasselin, J.; Lekander, M.; Benson, S.; Schedlowski, M.; Engler, H. Sick for science: Experimental endotoxemia as a translational tool to develop and test new therapies for inflammation-associated depression. Mol. Psychiatry 2020, 26, 3672–3683. [Google Scholar] [CrossRef] [PubMed]
- Lasselin, J.; Schedlowski, M.; Karshikoff, B.; Engler, H.; Lekander, M.; Konsman, J.P. Comparison of bacterial lipopolysaccharide-induced sickness behavior in rodents and humans: Relevance for symptoms of anxiety and depression. Neurosci. Biobehav. Rev. 2020, 115, 15–24. [Google Scholar] [CrossRef]
- Arnone, D.; Saraykar, S.; Salem, H.; Teixeira, A.L.; Dantzer, R.; Selvaraj, S. Role of Kynurenine pathway and its metabolites in mood disorders: A systematic review and meta-analysis of clinical studies. Neurosci. Biobehav. Rev. 2018, 92, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Haroon, E.; Daguanno, A.W.; Woolwine, B.J.; Goldsmith, D.R.; Baer, W.M.; Wommack, E.C.; Felger, J.C.; Miller, A.H. Antidepressant treatment resistance is associated with increased inflammatory markers in patients with major depressive disorder. Psychoneuroendocrinology 2018, 95, 43–49. [Google Scholar] [CrossRef]
- Jeng, J.S.; Li, C.T.; Chen, M.H.; Lin, W.C.; Bai, Y.M.; Tsai, S.J.; Su, T.P.; Chang, W.H.; Sung, Y.J. Repeated Low-Grade Infections Predict Antidepressant-Resistant Depression: A Nationwide Population-Based Cohort Study. J. Clin. Psychiatry 2018, 79, 17m11540. [Google Scholar] [CrossRef]
- Pariante, C.M. Why are depressed patients inflamed? A reflection on 20 years of research on depression, glucocorticoid resistance and inflammation. Eur. Neuropsychopharmacol. 2017, 27, 554–559. [Google Scholar] [CrossRef] [Green Version]
- Furtado, M.; Katzman, M.A. Neuroinflammatory pathways in anxiety, posttraumatic stress, and obsessive compulsive disorders. Psychiatry Res. 2015, 229, 37–48. [Google Scholar] [CrossRef]
- Renna, M.E.; O’Toole, M.S.; Spaeth, P.E.; Lekander, M.; Mennin, D.S. The association between anxiety, traumatic stress, and obsessive-compulsive disorders and chronic inflammation: A systematic review and meta-analysis. Depress. Anxiety 2018, 35, 1081–1094. [Google Scholar] [CrossRef] [Green Version]
- Passos, I.C.; Vasconcelos-Moreno, M.P.; Costa, L.G.; Kunz, M.; Brietzke, E.; Quevedo, J.; Salum, G.; Magalhães, P.V.; Kapczinski, F.; Kauer-Sant’Anna, M. Inflammatory markers in post-traumatic stress disorder: A systematic review, meta-analysis, and meta-regression. Lancet Psychiatry 2015, 2, 1002–1012. [Google Scholar] [CrossRef]
- Khoonsari, P.E.; Ossipova, E.; Lengqvist, J.; Svensson, C.I.; Kosek, E.; Kadetoff, D.; Jakobsson, P.J.; Kultima, K.; Lampa, J. The human CSF pain proteome. J. Proteom. 2018, 190, 67–76. [Google Scholar] [CrossRef]
- Karshikoff, B.; Åström, J.; Holmström, L.; Lekander, M.; Kemani, M.K.; Wicksell, R.K. Baseline Pro-Inflammatory Cytokine Levels Moderate Psychological Inflexibility in Behavioral Treatment for Chronic Pain. J. Clin. Med. 2022, 11, 2285. [Google Scholar] [CrossRef]
- Tait, R.C.; Chibnall, J.T.; Krause, S. The Pain Disability Index: Psychometric properties. Pain 1990, 40, 171–182. [Google Scholar] [CrossRef]
- Kemani, M.K.; Zetterqvist, V.; Kanstrup, M.; Holmström, L.; Wicksell, R.K. A validation of the pain interference index in adults with long-standing pain. Acta Anaesthesiol. Scand. 2016, 60, 250–258. [Google Scholar] [CrossRef]
- Sullivan, M.J.L.; Bishop, S.R.; Pivik, J. The Pain Catastrophizing Scale: Development and validation. Psychol. Assess. 1995, 7, 524–532. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L. The PHQ-9: A new depression diagnostic and severity measure. Psychiatr. Ann. 2002, 32, 509–515. [Google Scholar] [CrossRef] [Green Version]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Lowe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Eriksson, I.; Unden, A.L.; Elofsson, S. Self-rated health. Comparisons between three different measures. Results from a population study. Int. J. Epidemiol. 2001, 30, 326–333. [Google Scholar] [CrossRef] [Green Version]
- Bastien, C.H.; Vallieres, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Nordin, M.; Nordin, S. Psychometric evaluation and normative data of the Swedish version of the 10-item perceived stress scale. Scand. J. Psychol. 2013, 54, 502–507. [Google Scholar] [CrossRef]
- Ware, J., Jr.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lundberg, M.; Eriksson, A.; Tran, B.; Assarsson, E.; Fredriksson, S. Homogeneous antibody-based proximity extension assays provide sensitive and specific detection of low-abundant proteins in human blood. Nucleic. Acids Res. 2011, 39, e102. [Google Scholar] [CrossRef] [PubMed]
- Assarsson, E.; Lundberg, M.; Holmquist, G.; Bjorkesten, J.; Thorsen, S.B.; Ekman, D.; Eriksson, A.; Rennel Dickens, E.; Ohlsson, S.; Edfeldt, G.; et al. Homogenous 96-plex PEA immunoassay exhibiting high sensitivity, specificity, and excellent scalability. PLoS ONE 2014, 9, e95192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wheelock, A.M.; Wheelock, C.E. Trials and tribulations of ‘omics data analysis: Assessing quality of SIMCA-based multivariate models using examples from pulmonary medicine. Mol. Biosyst. 2013, 9, 2589–2596. [Google Scholar] [CrossRef] [Green Version]
- Eriksson, L.; Byrne, T.; Johansson, E.; Trygg, J.; Vikström, C. Multi and Megavariate Data Analysis: Basic Principles and Applications; MKS Umetrics AB: Malmö, Sweden; Umetrics Academy: Malmö, Sweden, 2013. [Google Scholar]
- Bazzichi, L.; Ciregia, F.; Giusti, L.; Baldini, C.; Giannaccini, G.; Giacomelli, C.; Sernissi, F.; Bombardieri, S.; Lucacchini, A. Detection of potential markers of primary fibromyalgia syndrome in human saliva. Proteom. Clin. Appl. 2009, 3, 1296–1304. [Google Scholar] [CrossRef]
- Conti, A.; Ricchiuto, P.; Iannaccone, S.; Sferrazza, B.; Cattaneo, A.; Bachi, A.; Reggiani, A.; Beltramo, M.; Alessio, M. Pigment epithelium-derived factor is differentially expressed in peripheral neuropathies. Proteomics 2005, 5, 4558–4567. [Google Scholar] [CrossRef]
- Sundquist, K.; Memon, A.A.; Palmer, K.; Sundquist, J.; Wang, X. Inflammatory proteins and miRNA-144-5p in patients with depression, anxiety, or stress- and adjustment disorders after psychological treatment. Cytokine 2021, 146, 155646. [Google Scholar] [CrossRef]
- Jonsjo, M.A.; Olsson, G.L.; Wicksell, R.K.; Alving, K.; Holmstrom, L.; Andreasson, A. The role of low-grade inflammation in ME/CFS (Myalgic Encephalomyelitis/Chronic Fatigue Syndrome)—Associations with symptoms. Psychoneuroendocrinology 2020, 113, 104578. [Google Scholar] [CrossRef]
- Panezai, J.; Ali, A.; Ghaffar, A.; Benchimol, D.; Altamash, M.; Klinge, B.; Engstrom, P.E.; Larsson, A. Upregulation of circulating inflammatory biomarkers under the influence of periodontal disease in rheumatoid arthritis patients. Cytokine 2020, 131, 155117. [Google Scholar] [CrossRef]
- Ek, M.; Roth, B.; Engstrom, G.; Ohlsson, B. AXIN1 in Plasma or Serum Is a Potential New Biomarker for Endometriosis. Int. J. Mol. Sci. 2019, 20, 189. [Google Scholar] [CrossRef] [Green Version]
- Majster, M.; Lira-Junior, R.; Hoog, C.M.; Almer, S.; Bostrom, E.A. Salivary and Serum Inflammatory Profiles Reflect Different Aspects of Inflammatory Bowel Disease Activity. Inflamm. Bowel. Dis. 2020, 26, 1588–1596. [Google Scholar] [CrossRef]
- Moraes, L.; Magnusson, M.K.; Mavroudis, G.; Polster, A.; Jonefjall, B.; Tornblom, H.; Sundin, J.; Simren, M.; Strid, H.; Ohman, L. Systemic Inflammatory Protein Profiles Distinguish Irritable Bowel Syndrome (IBS) and Ulcerative Colitis, Irrespective of Inflammation or IBS-Like Symptoms. Inflamm. Bowel. Dis. 2020, 26, 874–884. [Google Scholar] [CrossRef]
- Fineschi, S.; Klar, J.; Gustafsson, K.A.; Jonsson, K.; Karlsson, B.; Dahl, N. Inflammation and Interferon Signatures in Peripheral B-Lymphocytes and Sera of Individuals With Fibromyalgia. Front. Immunol. 2022, 13, 874490. [Google Scholar] [CrossRef]
- Shi, J.; Chi, S.; Xue, J.; Yang, J.; Li, F.; Liu, X. Emerging Role and Therapeutic Implication of Wnt Signaling Pathways in Autoimmune Diseases. J. Immunol. Res. 2016, 2016, 9392132. [Google Scholar] [CrossRef] [Green Version]
- Dihm, K.; Ek, M.; Roth, B.; Ohlsson, B. Plasma AXIN1 expression exhibit negative correlations with inflammatory biomarkers and is associated with gastrointestinal symptoms in endometriosis. Biomed. Rep. 2020, 12, 211–221. [Google Scholar] [CrossRef] [Green Version]
- Fan, Z.; Bin, L. Will Sirtuin 2 Be a Promising Target for Neuroinflammatory Disorders? Front. Cell. Neurosci. 2022, 16, 915587. [Google Scholar] [CrossRef]
- Zhu, C.; Dong, X.; Wang, X.; Zheng, Y.; Qiu, J.; Peng, Y.; Xu, J.; Chai, Z.; Liu, C. Multiple Roles of SIRT2 in Regulating Physiological and Pathological Signal Transduction. Genet. Res. 2022, 2022, 9282484. [Google Scholar] [CrossRef]
- Backryd, E.; Tanum, L.; Lind, A.L.; Larsson, A.; Gordh, T. Evidence of both systemic inflammation and neuroinflammation in fibromyalgia patients, as assessed by a multiplex protein panel applied to the cerebrospinal fluid and to plasma. J. Pain Res. 2017, 10, 515–525. [Google Scholar] [CrossRef] [Green Version]
- Akerblom, S.; Cervin, M.; Perrin, S.; Rivano Fischer, M.; Gerdle, B.; McCracken, L.M. A Network Analysis of Clinical Variables in Chronic Pain: A Study from the Swedish Quality Registry for Pain Rehabilitation (SQRP). Pain Med. 2021, 22, 1591–1602. [Google Scholar] [CrossRef]
- Palada, V.; Ahmed, A.S.; Freyhult, E.; Hugo, A.; Kultima, K.; Svensson, C.I.; Kosek, E. Elevated inflammatory proteins in cerebrospinal fluid from patients with painful knee osteoarthritis are associated with reduced symptom severity. J. Neuroimmunol. 2020, 349, 577391. [Google Scholar] [CrossRef]
- Palada, V.; Ahmed, A.S.; Finn, A.; Berg, S.; Svensson, C.I.; Kosek, E. Characterization of neuroinflammation and periphery-to-CNS inflammatory cross-talk in patients with disc herniation and degenerative disc disease. Brain Behav. Immun. 2018, 75, 60–71. [Google Scholar] [CrossRef] [PubMed]
- Dantzer, R. Neuroimmune Interactions: From the Brain to the Immune System and Vice Versa. Physiol. Rev. 2018, 98, 477–504. [Google Scholar] [CrossRef] [PubMed]
- Karshikoff, B.; Martucci, K.T.; Mackey, S. Relationship Between Blood Cytokine Levels, Psychological Comorbidity, and Widespreadness of Pain in Chronic Pelvic Pain. Front. Psychiatry 2021, 12, 651083. [Google Scholar] [CrossRef] [PubMed]
- Kruse, J.L.; Olmstead, R.; Hellemann, G.; Breen, E.C.; Tye, S.J.; Brooks, J.O., 3rd; Wade, B.; Congdon, E.; Espinoza, R.; Narr, K.L.; et al. Interleukin-8 and lower severity of depression in females, but not males, with treatment-resistant depression. J. Psychiatr. Res. 2021, 140, 350–356. [Google Scholar] [CrossRef]
- Schrepf, A.; O’Donnell, M.; Luo, Y.; Bradley, C.S.; Kreder, K.; Lutgendorf, S.; Multidisciplinary Approach to the Study of Chronic Pelvic Pain Research Network. Inflammation and inflammatory control in interstitial cystitis/bladder pain syndrome: Associations with painful symptoms. Pain 2014, 155, 1755–1761. [Google Scholar] [CrossRef] [Green Version]
- Schrepf, A.; O’Donnell, M.A.; Luo, Y.; Bradley, C.S.; Kreder, K.J.; Lutgendorf, S.K. Inflammation and Symptom Change in Interstitial Cystitis or Bladder Pain Syndrome: A Multidisciplinary Approach to the Study of Chronic Pelvic Pain Research Network Study. Urology 2016, 90, 56–61. [Google Scholar] [CrossRef] [Green Version]
- Arnberg, F.K.; Lekander, M.; Morey, J.N.; Segerstrom, S.C. Self-rated health and interleukin-6: Longitudinal relationships in older adults. Brain Behav. Immun. 2016, 54, 226–232. [Google Scholar] [CrossRef] [Green Version]
- Leshem-Rubinow, E.; Shenhar-Tsarfaty, S.; Milwidsky, A.; Toker, S.; Shapira, I.; Berliner, S.; Benyamini, Y.; Melamed, S.; Rogowski, O. Self-Rated Health is Associated with Elevated C-Reactive Protein Even among Apparently Healthy Individuals. Isr. Med. Assoc. J. 2015, 17, 213–218. [Google Scholar]
- Schistad, E.I.; Stubhaug, A.; Furberg, A.S.; Engdahl, B.L.; Nielsen, C.S. C-reactive protein and cold-pressor tolerance in the general population: The Tromso Study. Pain 2017, 158, 1280–1288. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables |
Full Cohort (n = 81) |
|---|---|
| Background data | Mean (SD) |
| Age (years) | 51.0 (14.6) |
| BMI (kg/m 2 ) | 25.3 (4.5) |
| Sex females/males % (n) | 71.6% (58)/28.4% (23) |
| Days difference blood sample and filling in questionnaires | 2.6 (2.8) |
| Pain characteristics | |
| Pain area number (sum) | 4.7 (2.9) |
| Local pain ( 1–2 sites) | 32.1% |
| Widespread pain (>3 sites) | 67.9% |
| Type of pain (reported pain in following areas) | |
| Back | 70.4% |
| Neck | 58.0% |
| Leg | 51.9% |
| Headache | 48.1% |
| Foot | 45.7% |
| Arm | 40.7% |
| Hand | 35.8% |
| Abdominal | 34.6% |
| Entire body | 32.1% |
| Teeth and jaw | 23.5% |
| Chest | 11.1% |
| Facial | 9.9% |
| Genital | 6.2% |
| Pain intensity (NRS) | 6.2 (1.9) |
| Pain duration (years) | 11.3 (8.9) |
| Psychological comorbidity | |
| Depression (PHQ-9) | 9.3 (5.4) |
| Anxiety (GAD-7) | 6.3 (4.5) |
| Other clinical parameters | |
| Insomnia (ISI) | 13.3 (6.6) |
| Stress (PSS) | 20.0 (9.1) |
| General health (SRH-5) | 2.9 (1.0) |
| Physical wellbeing (PCS-12) | 33.0 (8.6) |
| Mental wellbeing (MCS-12) | 39.8 (13.2) |
| Protein Name | Uniprot Protein Accession Number | VIP | p(corr) | Moderate/High Psychological Comorbidity Mean (SD) (n = 33) | Mild/No Psychological Comorbidity Mean (SD) (n = 39) |
|---|---|---|---|---|---|
| SIRT2 | Q8IXJ6 | 2.42 | −0.90 | 6.28 (0.98) | 5.58 (1.05) |
| STAMBP | O95630 | 2.42 | −0.90 | 6.71 (0.88) | 6.12 (0.92) |
| AXIN1 | O15169 | 2.32 | −0.86 | 5.84 (1.01) | 5.23 (1.02) |
| IL-7 | P13232 | 2.09 | −0.78 | 3.09 (0.63) | 2.70 (0.58) |
| CASP-8 | Q14790 | 2.02 | −0.75 | 1.51 (0.47) | 1.32 (0.40) |
| CXCL1 | P09341 | 1.94 | −0.72 | 8.99 (0.73) | 8.71 (0.92) |
| CD40 | P25942 | 1.94 | −0.72 | 11.48 (0.41) | 11.30 (0.46) |
| CXCL5 | P42830 | 1.88 | −0.70 | 11.30 (1.02) | 10.74 (1.25) |
| ST1A1 | P50225 | 1.79 | −0.67 | 3.17 (0.82) | 2.84 (0.76) |
| CD244 | Q9BZW8 | 1.79 | −0.66 | 6.81 (0.34) | 6.66 (0.36) |
| TNFSF14 | O43557 | 1.64 | −0.61 | 3.98 (0.55) | 3.65 (0.48) |
| 4E-BP1 | Q13541 | 1.57 | −0.58 | 9.45 (0.82) | 9.18 (0.93) |
| CXCL6 | P80162 | 1.56 | −0.58 | 8.78 (0.64) | 8.41 (0.98) |
| LAP TGF-beta-1 | P01137 | 1.52 | −0.57 | 7.30 (0.37) | 7.07 (0.40) |
| IFN-gamma | P01579 | 1.19 | 0.44 | 5.74 (0.62) | 6.50 (1.19) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karshikoff, B.; Wåhlén, K.; Åström, J.; Lekander, M.; Holmström, L.; Wicksell, R.K. Inflammatory Blood Signature Related to Common Psychological Comorbidity in Chronic Pain. Biomedicines 2023, 11, 713. https://doi.org/10.3390/biomedicines11030713
Karshikoff B, Wåhlén K, Åström J, Lekander M, Holmström L, Wicksell RK. Inflammatory Blood Signature Related to Common Psychological Comorbidity in Chronic Pain. Biomedicines. 2023; 11(3):713. https://doi.org/10.3390/biomedicines11030713
Chicago/Turabian StyleKarshikoff, Bianka, Karin Wåhlén, Jenny Åström, Mats Lekander, Linda Holmström, and Rikard K. Wicksell. 2023. "Inflammatory Blood Signature Related to Common Psychological Comorbidity in Chronic Pain" Biomedicines 11, no. 3: 713. https://doi.org/10.3390/biomedicines11030713