

Cerebrospinal Fluid Biomarkers in Differential Diagnosis of Multiple Sclerosis and Systemic Inflammatory Diseases with Central Nervous System Involvement
 , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Patient Selection
2.2. IFN-γ, CXCL13, GFAP, CHI3L1, OPN, IL6 and NF-Light Assessment in CSF
2.3. Statistic
3. Results
3.1. Study Population and Standard OCBs Analysis
- (1)
- 134 patients with MS (PwMS) according to McDonald criteria 2017;
- (2)
- 28 patients with systemic inflammatory diseases with CNS involvement (SID);
- (3)
- 10 patients with cerebrovascular diseases (CVD) (e.g., small vessel disease);
- (4)
- 70 patients with other non-inflammatory diseases (NID) (e.g., migraine, depression, patients with MRI non-specific white matter lesions).
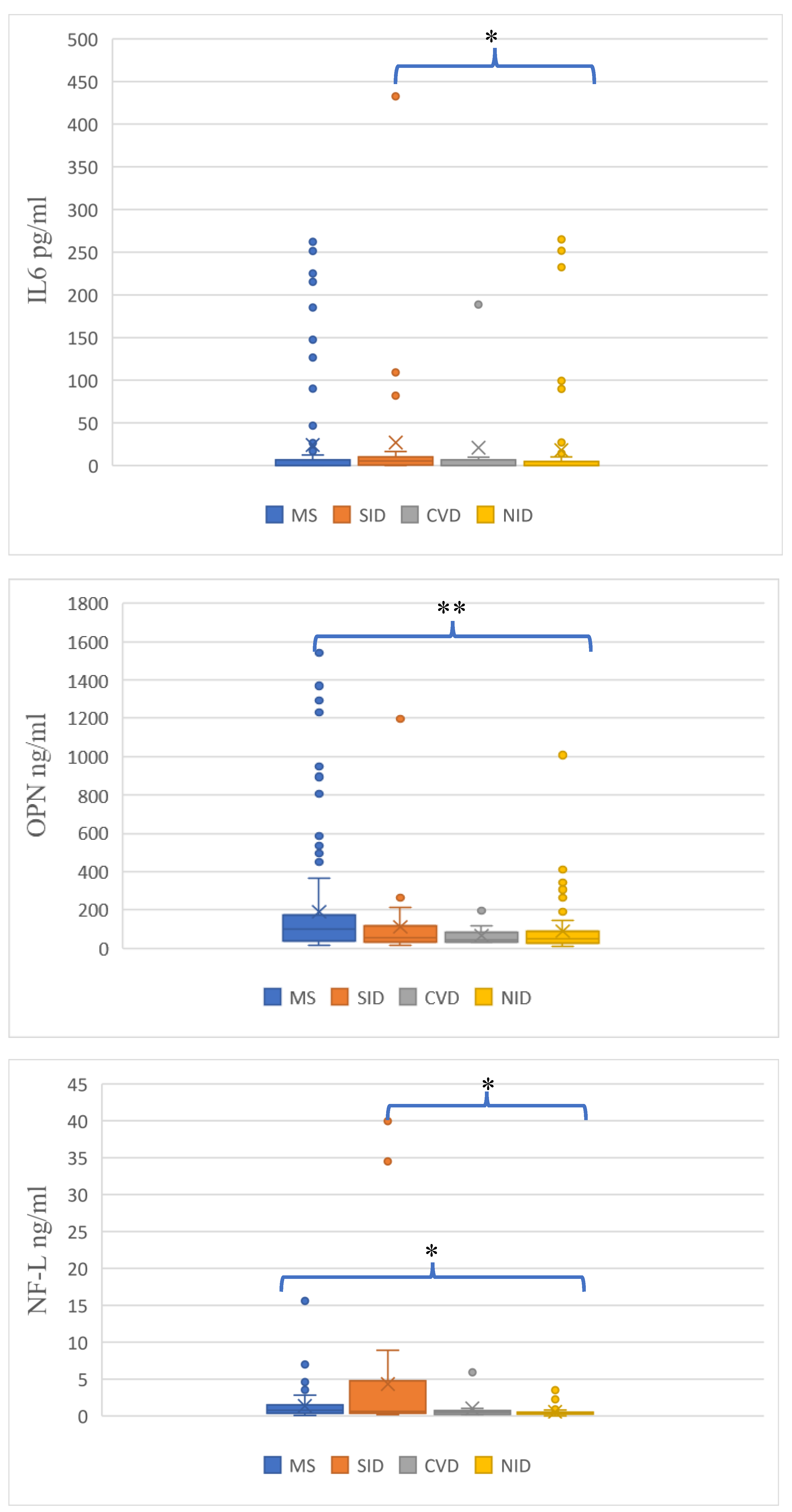
3.2. Assessment of Non-Standard CSF Biomarkers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Oh, J.; Vidal-Jordana, A.; Montalban, X. Multiple sclerosis: Clinical aspects. Curr. Opin. Neurol. 2018, 31, 752–759. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 62–173. [Google Scholar] [CrossRef] [PubMed]
- Wattjes, M.P.; Ciccarelli, O.; Reich, D.S.; Banwell, B.; de Stefano, N.; Enzinger, C.; Fazekas, F.; Filippi, M.; Frederiksen, J.; Gasperini, C.; et al. Magnetic Resonance Imaging in Multiple Sclerosis Study Group; Consortium of Multiple Sclerosis Centres; North American Imaging in Multiple Sclerosis Cooperative MRI guidelines working group. 2021 MAGNIMS-CMSC-NAIMS consensus recommendations on the use of MRI in patients with multiple sclerosis. Lancet Neurol. 2021, 20, 653–670. [Google Scholar] [PubMed]
- Solomon, A.J.; Naismith, R.T.; Cross, A.H. Misdiagnosis of multiple sclerosis: Impact of the 2017 McDonald criteria on clinical practice. Neurology 2019, 92, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Solomon, A.J.; Bourdette, D.N.; Cross, A.H.; Applebee, A.; Skidd, P.M.; Howard, D.B.; Spain, R.I.; Cameron, M.H.; Kim, E.; Mass, M.K.; et al. The contemporary spectrum of multiple sclerosis misdiagnosis: A multicenter study. Neurology 2016, 87, 1393–1399. [Google Scholar] [CrossRef]
- Midaglia, L.; Sastre-Garriga, J.; Pappolla, A.; Quibus, L.; Carvajal, R.; Vidal-Jordana, A.; Arrambide, G.; Río, J.; Comabella, M.; Nos, C.; et al. The frequency and characteristics of MS misdiagnosis in patients referred to the multiple sclerosis centre of Catalonia. Mult. Scler. 2021, 27, 913–921. [Google Scholar] [CrossRef]
- Wildner, P.; Stasiołek, M.; Matysiak, M. Differential diagnosis of multiple sclerosis and other inflammatory CNS diseases. Mult. Scler. Relat. Disord. 2020, 37, 101452. [Google Scholar] [CrossRef]
- Gaitán, M.I.; Sanchez, M.; Farez, M.F.; Fiol, M.P.; Ysrraelit, M.C.; Solomon, A.J.; Correale, J. The frequency and characteristics of multiple sclerosis misdiagnosis in Latin America: A referral center study in Buenos Aires, Argentina. Mult. Scler. 2022, 28, 1373–1381. [Google Scholar] [CrossRef]
- Kaisey, M.; Solomon, A.J.; Luu, M.; Giesser, B.S.; Sicotte, N.L. Incidence of multiple sclerosis misdiagnosis in referrals to two academic centers. Mult. Scler. Relat. Disord. 2019, 30, 51–56. [Google Scholar] [CrossRef]
- Arrambide, G.; Tintore, M.; Espejo, C.; Auger, C.; Castillo, M.; Vidal-Jordana, A.; Galán, I.; Nos, C.; Mitjana, R.; Mulero, P.; et al. The value of oligoclonal bands in the multiple sclerosis diagnostic criteria. Brain 2018, 141, 1075–1084. [Google Scholar] [CrossRef] [Green Version]
- Freedman, M.S.; Thompson, E.J.; Deisenhammer, F.; Giovannoni, G.; Grimsley, G.; Keir, G.; Ohman, S.; Racke, M.K.; Sharief, M.; Sindic, C.J.; et al. Recommended standard of cerebrospinal fluid analysis in the diagnosis of multiple sclerosis: A consensus statement. Arch. Neurol. 2005, 62, 865–870. [Google Scholar] [CrossRef] [PubMed]
- Mayringer, I.; Timeltaler, B.; Deisenhammer, F. Correlation between the IgG index, oligoclonal bands in CSF, and the diagnosis of demyelinating diseases. Eur. J. Neurol. 2005, 12, 527–530. [Google Scholar] [CrossRef]
- Konen, F.F.; Schwenkenbecher, P.; Jendretzky, K.F.; Gingele, S.; Sühs, K.-F.; Tumani, H.; Süße, M.; Skripuletz, T. The Increasing Role of Kappa Free Light Chains in the Diagnosis of Multiple Sclerosis. Cells 2021, 10, 3056. [Google Scholar] [CrossRef] [PubMed]
- Leurs, C.E.; Twaalfhoven, H.; Lissenberg-Witte, B.I.; van Pesch, V.; Dujmovic, I.; Drulovic, J.; Castellazzi, M.; Bellini, T.; Pugliatti, M.; Kuhle, J.; et al. Kappa free light chains is a valid tool in the diagnostics of MS: A large multicenter study. Mult. Scler. 2020, 26, 912–923. [Google Scholar] [CrossRef]
- Felgenhauer, K.; Reiber, H. The diagnostic significance of antibody specificity indices in multiple sclerosis and herpes virus induced diseases of the nervous system. Clin. Investig. 1992, 70, 28–37. [Google Scholar] [CrossRef]
- Jarius, S.; Eichhorn, P.; Franciotta, D.; Petereit, H.F.; Akman-Demir, G.; Wick, M.; Wildemann, B. The MRZ reaction as a highly specific marker of multiple sclerosis: Re-evaluation and structured review of the literature. J. Neurol. 2017, 264, 453–466. [Google Scholar] [CrossRef] [PubMed]
- Norgren, N.; Sundström, P.; Svenningsson, A.; Rosengren, L.; Stigbrand, T.; Gunnarsson, M. Neurofilament and glial fibrillary acidic protein in multiple sclerosis. Neurology 2004, 63, 1586–1590. [Google Scholar] [CrossRef] [PubMed]
- Bridel, C.; van Wieringen, W.N.; Zetterberg, H.; Tijms, B.M.; Teunissen, C.E.; The NFL Group; Alvarez-Cermeño, C.J.; Andreasson, U.; Axelsson, M.; Bäckström, D.C.; et al. Diagnostic value of cerebrospinal fluid neurofilament light protein in neurology: A systematic review and meta-analysis. JAMA Neurol. 2019, 76, 1035–1048. [Google Scholar] [CrossRef] [PubMed]
- Martínez, M.A.; Olsson, B.; Bau, L.; Matas, E.; Cobo Calvo, Á.; Andreasson, U.; Blennow, U.; Romero-Pinel, L.; Martínez-Yélamos, S.; Zetterberg, H. Glial and neuronal markers in cerebrospinal fluid predict progression in multiple sclerosis. Mult. Scler. 2015, 21, 550–561. [Google Scholar] [CrossRef]
- Correale, J.; Fiol, M. Chitinase effects on immune cell response in neuromyelitis optica and multiple sclerosis. Mult. Scler. 2011, 17, 521–531. [Google Scholar] [CrossRef]
- Braitch, M.; Nunan, R.; Niepel, G.; Edwards, L.J.; Constantinescu, C.S. Increased osteopontin levels in the cerebrospinal fluid of patients with multiple sclerosis. Arch. Neurol. 2008, 65, 633–635. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, S.A.; Lin, J.; Sadiq, S.A. Specificity and correlation with disease activity of cerebrospinal fluid osteopontin levels in patients with multiple sclerosis. Arch. Neurol. 2008, 65, 232–235. [Google Scholar] [CrossRef] [PubMed]
- Agah, E.; Zardoui, A.; Saghazadeh, A.; Ahmadi, M.; Tafakhori, A.; Rezaei, M. Osteopontin (OPN) as a CSF and blood biomarker for multiple sclerosis: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0190252. [Google Scholar] [CrossRef]
- Bai, Z.; Chen, D.; Wang, L.; Zhao, Y.; Liu, T.; Yu, Y.; Yan, T.; Cheng, Y. Cerebrospinal fluid and blood cytokines as biomarkers for multiple sclerosis: A systematic review and meta-analysis of 226 studies with 13,526 multiple sclerosis patients. Front. Neurosci. 2019, 13, 1026. [Google Scholar] [CrossRef] [PubMed]
- Sellebjerg, F.; Börnsen, L.; Khademi, M.; Krakauer, M.; Olsson, T.; Frederiksen, J.L.; Sørensen, P.S. Increased cerebrospinal fluid concentrations of the chemokine CXCL13 in active MS. Neurology 2009, 73, 2003–2010. [Google Scholar] [CrossRef]
- Brownlee, W.; Solomon, A.J. Misdiagnosis of multiple sclerosis: Time for action. Mult. Scler. 2021, 27, 805–806. [Google Scholar] [CrossRef] [PubMed]
- Brownlee, W.J. Use (and misuse) of the McDonald criteria to diagnose multiple sclerosis. Eur. J. Neurol. 2018, 25, 209–210. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, M.; Gasperini, C.; Tortorella, C.; Schiavi, G.; Frisullo, G.; Ragonese, P.; Fantozzi, R.; Prosperini, L.; Annovazzi, P.; Cordioli, C.; et al. “Better explanations” in multiple sclerosis diagnostic workup: A 3-year longitudinal study. Neurology 2019, 92, e2527–e2537. [Google Scholar] [CrossRef]
- Dobson, R.; Ramagopalan, S.; Davis, A.; Giovannoni, G. Cerebrospinal fluid oligoclonal bands in multiple sclerosis and clinically isolated syndromes: A meta-analysis of prevalence, prognosis and effect of latitude. J. Neurol. Neurosurg. Psychiatry 2013, 84, 909–914. [Google Scholar] [CrossRef]
- Karathanasis, D.; Rapti, A.; Nezos, A.; Skarlis, C.; Kilidireas, C.; Mavragani, C.P.; Evangelopoulos, M.E. Differentiating central nervous system demyelinating disorders: The role of clinical, laboratory, imaging characteristics and peripheral blood type I interferon activity. Front. Pharmacol. 2022, 13, 898049. [Google Scholar] [CrossRef]
- Nikolopoulos, D.; Kitsos, D.; Papathanasiou, M.; Chondrogianni, M.; Theodorou, A.; Garantziotis, P.; Pieta, A.; Doskas, T.; Bertsias, G.; Voumvourakis, K.; et al. Demyelination with autoimmune features: A distinct clinical entity? Results from a longitudinal cohort. Rheumatology 2021, 60, 4166–4174. [Google Scholar] [CrossRef] [PubMed]
- Nikolopoulos, D.; Kitsos, D.; Papathanasiou, M.; Kapsala, N.; Garantziotis, P.; Pieta, A.; Gioti, O.; Grivas, A.; Voumvourakis, K.; Boumpas, D.; et al. Demyelinating Syndromes in Systemic Lupus Erythematosus: Data From the “Attikon” Lupus Cohort. Front. Neurol. 2022, 13, 889613. [Google Scholar] [CrossRef] [PubMed]
- Saadeh, R.S.; Bryant, S.C.; McKeon, A.; Weinshenker, B.; Murray, D.L.; Pittock, S.J.; Willrich, M.A.V. CSF Kappa Free Light Chains: Cutoff Validation for Diagnosing Multiple Sclerosis. Mayo. Clin. Proc. 2022, 97, 738–751. [Google Scholar] [CrossRef] [PubMed]
- Harris, V.K.; Tuddenham, J.F.; Sadiq, S.A. Biomarkers of multiple sclerosis: Current findings. Degener. Neurol. Neuromuscul. Dis. 2017, 7, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Ziemssen, T.; Akgün, K.; Brück, W. Molecular biomarkers in multiple sclerosis. J. Neuroinflamm. 2019, 16, 272. [Google Scholar] [CrossRef]
- Kaisey, M.; Lashgari, G.; Fert-Bober, J.; Ontaneda, D.; Solomon, A.J.; Sicotte, N.L. An Update on Diagnostic Laboratory Biomarkers for Multiple Sclerosis. Curr. Neurol. Neurosci. Rep. 2022, 22, 675–688. [Google Scholar] [CrossRef]
- Saadeh, R.S.; Ramos, P.A.; Algeciras-Schimnich, A.; Flanagan, E.P.; Pittock, S.J.; Willrich, M.A. An Update on Laboratory-Based Diagnostic Biomarkers for Multiple Sclerosis and Beyond. Clin. Chem. 2022, 68, 1134–1150. [Google Scholar] [CrossRef]
- Picón, C.; Tejeda-Velarde, A.; Fernández-Velasco, J.I.; Comabella, M.; Álvarez-Lafuente, R.; Quintana, E.; Sainz de la Maza, S.; Monreal, E.; Villarrubia, N.; Álvarez-Cermeño, J.C.; et al. Identification of the Immunological Changes Appearing in the CSF During the Early Immunosenescence Process Occurring in Multiple Sclerosis. Front. Immunol. 2021, 12, 685139. [Google Scholar] [CrossRef]
- Lycke, J.N.; Karlsson, J.E.; Andersen, O.; Rosengren, L.E. Neurofilament protein in cerebrospinal fluid: A potential marker of activity in multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 1998, 64, 402–404. [Google Scholar] [CrossRef]
- Malmeström, C.; Haghighi, S.; Rosengren, L.; Andersen, O.; Lycke, J. Neurofilament light protein and glial fibrillary acidic protein as biological markers in MS. Neurology 2003, 61, 1720–1725. [Google Scholar] [CrossRef]
- Olesen, M.N.; Soelberg, K.; Debrabant, B.; Nilsson, A.C.; Lillevang, S.T.; Grauslund, J.; Brandslund, I.; Madsen, J.S.; Paul, F.; Smith, T.J.; et al. Cerebrospinal fluid biomarkers for predicting development of multiple sclerosis in acute optic neuritis: A population-based prospective cohort study. J. Neuroinflamm. 2019, 16, 59. [Google Scholar] [CrossRef]
- Lauvsnes, M.B.; Zetterberg, H.; Blennow, K.; Kvaløy, J.T.; Tjensvoll, A.B.; Maroni, S.; Beyer, M.K.; Greve, O.J.; Kvivik, I.; Alves, G.; et al. Neurofilament light in plasma is a potential biomarker of central nervous system involvement in systemic lupus erythematosus. J. Neurol. 2022, 269, 3064–3074. [Google Scholar] [CrossRef] [PubMed]
- Tjensvoll, A.B.; Lauvsnes, M.B.; Zetterberg, H.; Kvaløy, J.T.; Kvivik, I.; Maroni, S.S.; Greve, O.J.; Beyer, M.K.; Hirohata, S.; Putterman, C.; et al. Neurofilament light is a biomarker of brain involvement in lupus and primary Sjögren’s syndrome. J. Neurol. 2021, 268, 1385–1394. [Google Scholar] [CrossRef] [PubMed]
- Byg, K.E.; Nielsen, H.H.; Sejbaek, T.; Madsen, J.S.; Olsen, D.A.; Nguyen, N.; Kindt, A.; Grauslund, J.; Illes, Z.; Ellingsen, T. Elevated Neurofilament Light Chain in Cerebrospinal Fluid and Plasma Reflect Inflammatory MRI Activity in Neurosarcoidosis. Brain Sci. 2021, 11, 238. [Google Scholar] [CrossRef] [PubMed]
- Zervides, K.A.; Janelidze, S.; Nystedt, J.; Gullstrand, B.; Nilsson, P.; Sundgren, P.C.; Bengtsson, A.A.; Hansson, O.; Jönsen, A. Plasma and cerebrospinal fluid neurofilament light concentrations reflect neuronal damage in systemic lupus Erythematosus. BMC Neurol. 2022, 22, 467. [Google Scholar] [CrossRef] [PubMed]
- Strehlow, F.; Bauer, S.; Martus, P.; Weller, M.; Roth, P.; Schlegel, U.; Seidel, S.; Scheibenbogen, C.; Korfel, A.; Kreher, S. Osteopontin in cerebrospinal fluid as diagnostic biomarker for central nervous system lymphoma. J. Neurooncol. 2016, 129, 165–171. [Google Scholar] [CrossRef]
- Hirohata, S.; Miyamoto, T. Elevated levels of interleukin-6 in cerebrospinal fluid from patients with systemic lupus erythematosus and central nervous system involvement. Arthritis Rheum. 1990, 33, 644–649. [Google Scholar] [CrossRef]
- Chazal, T.; Costopoulos, M.; Maillart, E.; Fleury, C.; Psimaras, D.; Legendre, P.; Pineton de Chambrun, M.; Haroche, J.; Lubetzki, C.; Amoura, Z.; et al. The cerebrospinal fluid CD4/CD8 ratio and interleukin-6 and -10 levels in neurosarcoidosis: A multicenter, pragmatic, comparative study. Eur. J. Neurol. 2019, 26, 1274–1280. [Google Scholar] [CrossRef]
- Levraut, M.; Landes, C.; Mondot, L.; Cohen, M.; Bresch, S.; Brglez, V.; Seitz-Polski, B.; Lebrun-Frenay, C. Kappa Free Light Chains, Soluble Interleukin-2 Receptor, and Interleukin-6 Help Explore Patients Presenting With Brain White Matter Hyperintensities. Front. Immunol. 2022, 13, 864133. [Google Scholar] [CrossRef]
- Ichinose, K.; Arima, K.; Ushigusa, T.; Nishino, A.; Nakashima, Y.; Suzuki, T.; Horai, Y.; Nakajima, H.; Kawashiri, S.Y.; Iwamoto, N.; et al. Distinguishing the cerebrospinal fluid cytokine profile in neuropsychiatric systemic lupus erythematosus from other autoimmune neurological diseases. Clin. Immunol. 2015, 157, 114–120. [Google Scholar] [CrossRef] [Green Version]
- Martynova, E.; Goyal, M.; Johri, S.; Kumar, V.; Khaibullin, T.; Rizvanov, A.A.; Verma, S.; Khaiboullina, S.F.; Baranwal, M. Serum and Cerebrospinal Fluid Cytokine Biomarkers for Diagnosis of Multiple Sclerosis. Mediat. Inflamm. 2020, 2020, 2727042. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, E.; Piccio, L.; Mikesell, R.J.; Klawiter, E.C.; Parks, B.J.; Naismith, R.T. Cross AH. CXCL13 is a biomarker of inflammation in multiple sclerosis, neuromyelitis optica, and other neurological conditions. Mult. Scler. 2013, 19, 1204–1208. [Google Scholar] [CrossRef]
- Leth, T.A.; Dessau, R.B.; Møller, J.K. Discriminating between Lyme neuroborreliosis and other central nervous system infections by use of biomarkers CXCL13 and IL-6. Ticks Tick Borne Dis. 2022, 13, 101984. [Google Scholar] [CrossRef] [PubMed]
- Hinsinger, G.; Galéotti, N.; Nabholz, N.; Urbach, S.; Rigau, V.; Demattei, C.; Lehmann, S.; Camu, W.; Labauge, P.; Castelnovo, G.; et al. Chitinase 3-like proteins as diagnostic and prognostic biomarkers of multiple sclerosis. Mult. Scler. 2015, 21, 1251–1261. [Google Scholar] [CrossRef] [PubMed]
- Kušnierová, P.; Zeman, D.; Hradílek, P.; Zapletalová, O.; Stejskal, D. Determination of chitinase 3-like 1 in cerebrospinal fluid in multiple sclerosis and other neurological diseases. PLoS ONE 2020, 15, e0233519. [Google Scholar] [CrossRef] [PubMed]
- Lucchini, M.; De Arcangelis, V.; Piro, G.; Nociti, V.; Bianco, A.; De Fino, C.; Di Sante, G.; Ria, F.; Calabresi, P.; Mirabella, M. CSF CXCL13 and Chitinase 3-like-1 Levels Predict Disease Course in Relapsing Multiple Sclerosis. Mol. Neurobiol. 2023, 60, 36–50. [Google Scholar] [CrossRef] [PubMed]
- Aslam, N.; Khan, I.U.; Bashamkh, A.; Alghool, F.A.; Aboulnour, M.; Alsuwayan, N.M.; Alturaif, R.K.; Brahimi, S.; Aljaamel, S.S.; Al Khamdi, K. Multiple Sclerosis Diagnosis Using Machine Learning and Deep Learning: Challenges and Opportunities. Sensors 2022, 22, 7856. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patients n = 242 | MS n = 134 | SID n = 28 | CVD n = 10 | NID n = 70 |
|---|---|---|---|---|
| Female sex, n (%) | 97 (72.4) | 17 (60.7) | 7 (70.0) | 58 (82.8) |
| Age, years | 35.8 (10.4) * | 39.3 (10.3) | 44.3 (7.9) * | 42.4 (12.9) * |
| OCBs, n (%) | 125 (93.3) * | 8 (28.6) * | 0 (0) * | 4 (5.7) * |
| Patients with T2 Lesions in MRI Suspected of MS | PwMS and SID Population | |
|---|---|---|
| OCBs sensitivity | 91.2% | 93.9% |
| OCBs specificity | 89.2% | 70.4% |
| Biomarkers | Spearman R | p |
|---|---|---|
| INF-γ and CXCL13 | 0.132640 | 0.037 |
| INF-γ and CHI3L1 | −0.205150 | 0.001 * |
| IL6 and CHI3L1 | 0.297844 | 0.000 * |
| OPN and CXCL13 | −0.179078 | 0.005 * |
| OPN and NF-L | 0.256492 | 0.000 * |
| OPN and IL6 | −0.126423 | 0.047 |
| Patients n = 242 | MS n = 134 | SID n = 28 | CVD n = 10 | NID n = 70 |
|---|---|---|---|---|
| INF-γ (pg/mL) | 9.9 (43.6) 0.0 [0.0–5.2] | 29.3 (87.4) 0.9 [0.0–9.9] | 12.9 (23.7) 1.2 [0.0–16.1] | 4.7 (10.8) 0.0 [0.0–4.6] |
| IL6 (pg/mL) | 23.9 (64.7) 0.0 [0.0–6.4] | 26.9 (83.1) 5.5 [1.2–10.0] | 20.9 (59.1) 0.0 [0.0–5.7] | 18.2 (57.4) 0.0 [0.0–4.6] |
| OPN (ng/mL) | 189.1 (274.9) 95.3 [37.9–170.7] | 112.2 (221.2) 53.4 [30.9–108.4 | 66.1 (52.9) 43.2 [32.8–67.6] | 89.5 (134.8) 51.5 [28.8–86.6] |
| CXCL13 (pg/mL) | 260.7 (250.3) 207.8 [71.2–397.6] | 411.2 (802.3) 129.4 [0.0–452.4] | 295.6 (359.9) 157.7 [62.5–301.9] | 260.0 (251.9) 220.9 [33.4–418.5] |
| NF-L (ng/mL) | 1.4 (2.1) 0.8 [0.4–1.5] | 4.3 (9.6) 0.6 [0.4–3.9] | 1.0 (1.7) 0.5 [0.3–0.6] | 0.6 (0.6) 0.3 [0.3–0.5] |
| CHI3L1 (ng/mL) | 32.9 (63.3) 10.9 [5.7–29.8] | 33.4 (48.9) 27.5 [6.7–38.1] | 39.2 (69.9) 21.5 [7.5–28.8] | 38.9 (59.5) 27.1 [6.8–33.8] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Świderek-Matysiak, M.; Oset, M.; Domowicz, M.; Galazka, G.; Namiecińska, M.; Stasiołek, M. Cerebrospinal Fluid Biomarkers in Differential Diagnosis of Multiple Sclerosis and Systemic Inflammatory Diseases with Central Nervous System Involvement. Biomedicines 2023, 11, 425. https://doi.org/10.3390/biomedicines11020425
Świderek-Matysiak M, Oset M, Domowicz M, Galazka G, Namiecińska M, Stasiołek M. Cerebrospinal Fluid Biomarkers in Differential Diagnosis of Multiple Sclerosis and Systemic Inflammatory Diseases with Central Nervous System Involvement. Biomedicines. 2023; 11(2):425. https://doi.org/10.3390/biomedicines11020425
Chicago/Turabian StyleŚwiderek-Matysiak, Mariola, Magdalena Oset, Małgorzata Domowicz, Grażyna Galazka, Magdalena Namiecińska, and Mariusz Stasiołek. 2023. "Cerebrospinal Fluid Biomarkers in Differential Diagnosis of Multiple Sclerosis and Systemic Inflammatory Diseases with Central Nervous System Involvement" Biomedicines 11, no. 2: 425. https://doi.org/10.3390/biomedicines11020425