
Screening Cases of Suspected Early Stage Chronic Kidney Disease from Clinical Laboratory Data: The Comparison between Urine Conductivity and Urine Protein

Abstract
:1. Introduction
2. Materials and Methods
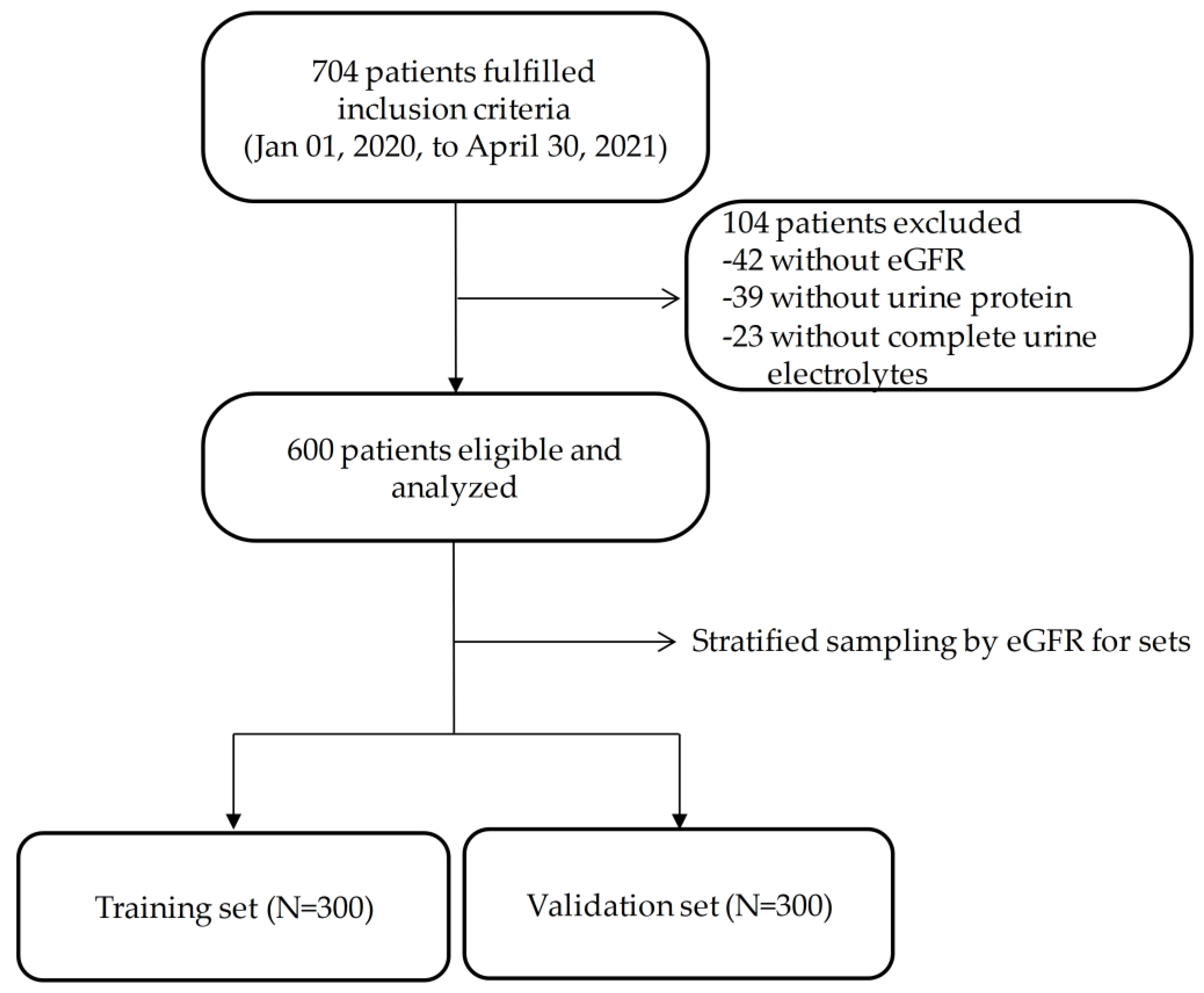
2.1. Study Design, Setting, and Population
2.2. Estimated Glomerular Filtration Rate
2.3. Laboratory Data with a Urine Sample
2.3.1. Urine Quantitative Analysis
2.3.2. Urine Electrolytes
2.3.3. Urine Conductivity and Osmolality
2.3.4. Urine Specific Gravity
2.4. Statistical Analyses
2.4.1. Sets Grouping
2.4.2. Predictive Models Development
2.4.3. The Better Fitness Population for the Predicted Model
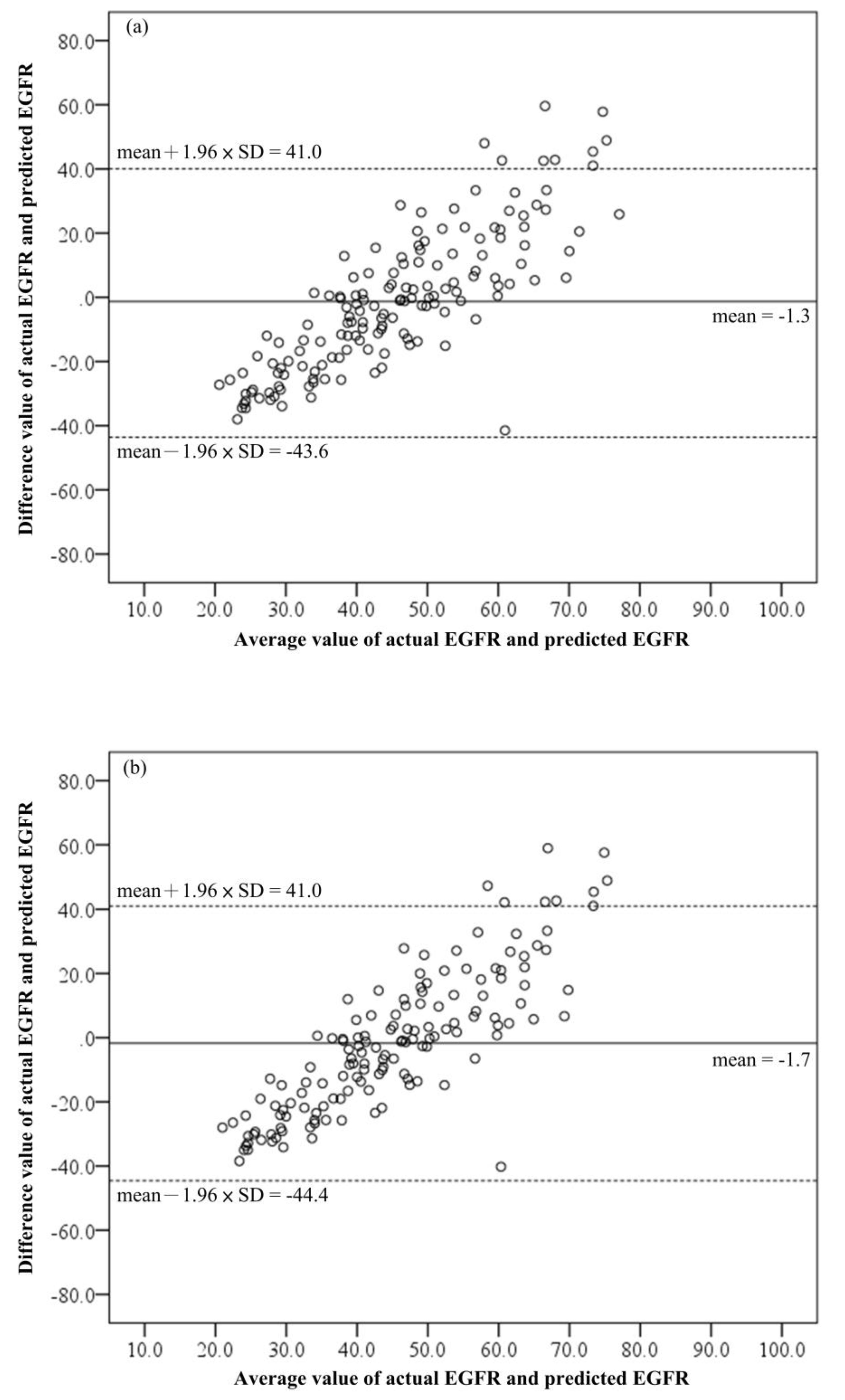
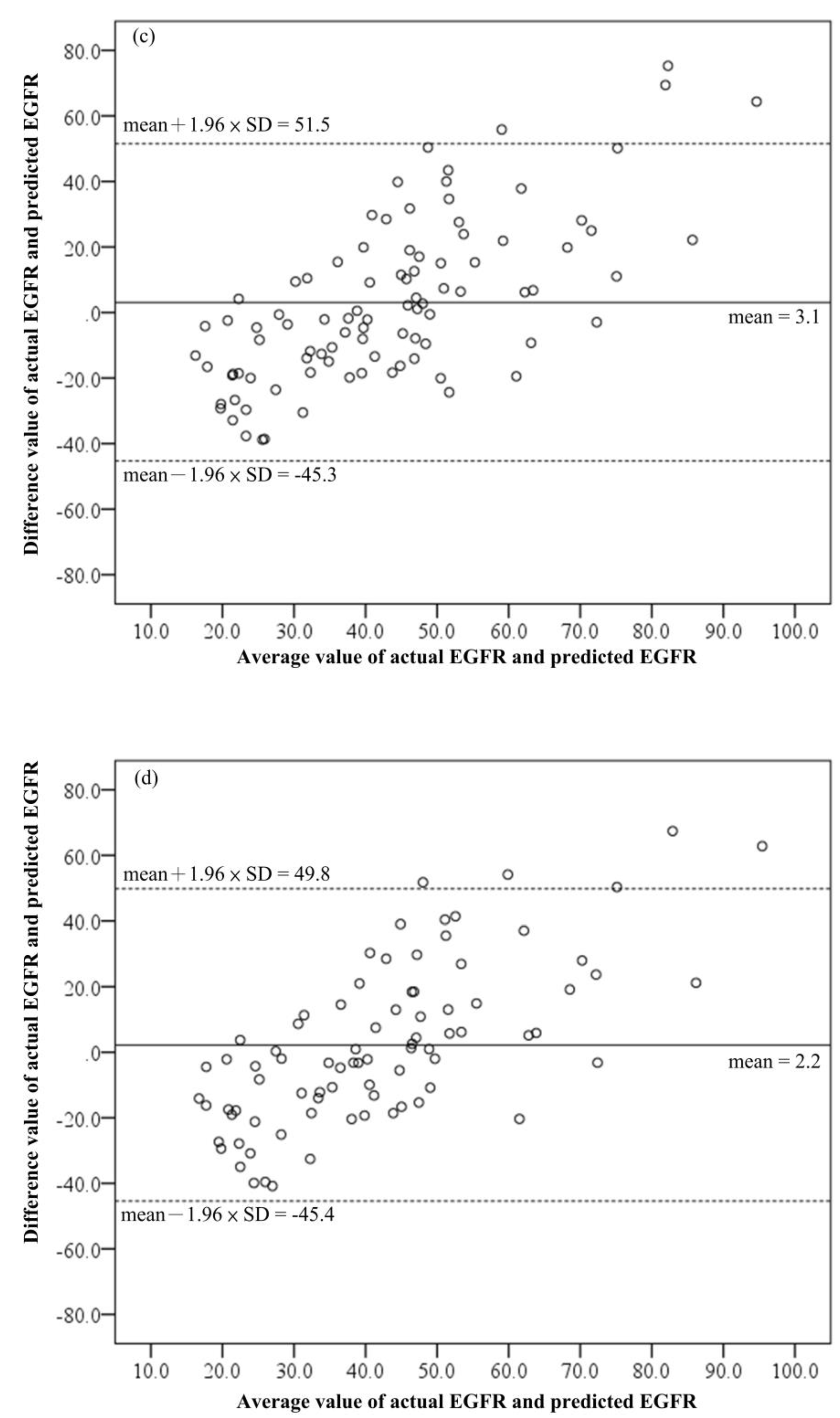
2.4.4. The Validation and the Comparison
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tojo, A.; Kinugasa, S. Mechanisms of glomerular albumin filtration and tubular reabsorption. Int. J. Nephrol. 2012, 2012, 481520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gburek, J.; Konopska, B.; Gołąb, K. Renal Handling of Albumin-From Early Findings to Current Concepts. Int. J. Mol. Sci. 2021, 22, 5809. [Google Scholar] [CrossRef] [PubMed]
- Weiner, I.D.; Verlander, J.W. Ammonia Transporters and Their Role in Acid-Base Balance. Physiol. Rev. 2017, 97, 465–494. [Google Scholar] [CrossRef]
- Mather, A.; Pollock, C. Glucose handling by the kidney. Kidney Int. 2011, 79, S1–S6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cunha, R.S.D.; Azevedo, C.A.B.; Falconi, C.A.; Ruiz, F.F.; Liabeuf, S.; Carneiro-Ramos, M.S.; Stinghen, A.E.M. The Interplay between Uremic Toxins and Albumin, Membrane Transporters and Drug Interaction. Toxins 2022, 14, 177. [Google Scholar] [CrossRef]
- Sahay, M.; Kalra, S.; Bandgar, T. Renal endocrinology: The new frontier. Indian J. Endocrinol. Metab. 2012, 16, 154–155. [Google Scholar]
- Lee, W.C.; Lee, Y.T.; Li, L.C.; Ng, H.Y.; Kuo, W.H.; Lin, P.T.; Liao, Y.C.; Chiou, T.T.; Lee, C.T. The Number of Comorbidities Predicts Renal Outcomes in Patients with Stage 3–5 Chronic Kidney Disease. J. Clin. Med. 2018, 7, 493. [Google Scholar] [CrossRef] [Green Version]
- Kidney Disease: Improving Global Outcomes (KDIGO) Blood Pressure Work Group. KDIGO 2021 Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease. Kidney Int. 2021, 99, S1–S87. [Google Scholar] [CrossRef]
- Kovesdy, C.P. Epidemiology of chronic kidney disease: An update 2022. Kidney Int. 2022, 12, 7–11. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Chronic Kidney Disease in the United States, 2021; US Department of Health and Human Services, Centers for Disease Control and Prevention: Atlanta, GA, USA, 2021.
- Djukanović, L. Benefits of screening for Chronic Kidney Disease. Prilozi 2010, 31, 249–259. [Google Scholar]
- Damtie, S.; Biadgo, B.; Baynes, H.W.; Ambachew, S.; Melak, T.; Asmelash, D.; Abebe, M. Chronic Kidney Disease and Associated Risk Factors Assessment among Diabetes Mellitus Patients at A Tertiary Hospital, Northwest Ethiopia. Ethiop. J. Health Sci. 2018, 28, 691–700. [Google Scholar] [CrossRef]
- Mathew, T.; Corso, O. Review article: Early detection of chronic kidney disease in Australia: Which way to go? Nephrology 2009, 14, 367–373. [Google Scholar] [CrossRef]
- Tonelli, M.; Dickinson, J.A. Early Detection of CKD: Implications for Low-Income, Middle-Income, and High-Income Countries. J. Am. Soc. Nephrol. 2020, 31, 1931–1940. [Google Scholar] [CrossRef]
- George, C.; Echouffo-Tcheugui, J.B.; Jaar, B.G.; Okpechi, I.G.; Kengne, A.P. The need for screening, early diagnosis, and prediction of chronic kidney disease in people with diabetes in low- and middle-income countries-a review of the current literature. BMC Med. 2022, 20, 247. [Google Scholar] [CrossRef]
- Cravedi, P.; Remuzzi, G. Pathophysiology of proteinuria and its value as an outcome measure in chronic kidney disease. Br. J. Clin. Pharmacol. 2013, 76, 516–523. [Google Scholar]
- Jaar, B.G.; Khatib, R.; Plantinga, L.; Boulware, L.E.; Powe, N.R. Principles of Screening for Chronic Kidney Disease. Clin. J. Am. Soc. Nephrol. 2008, 3, 601–609. [Google Scholar] [CrossRef] [Green Version]
- Clark, W.F.; Macnab, J.J.; Sontrop, J.M.; Jain, A.K.; Moist, L.; Salvadori, M.; Suri, R.; Garg, A.X. Dipstick proteinuria as a screening strategy to identify rapid renal decline. J. Am. Soc. Nephrol. 2011, 22, 1729–1736. [Google Scholar] [CrossRef] [Green Version]
- White, S.L.; Yu, R.; Craig, J.C.; Polkinghorne, K.R.; Atkins, R.C.; Chadban, S.J. Diagnostic accuracy of urine dipsticks for detection of albuminuria in the general community. Am. J. Kidney Dis. 2011, 58, 19–28. [Google Scholar] [CrossRef]
- Park, J.I.; Baek, H.; Kim, B.R.; Jung, H.H. Comparison of urine dipstick and albumin:creatinine ratio for chronic kidney disease screening: A population-based study. PLoS ONE 2017, 12, e0171106. [Google Scholar] [CrossRef] [Green Version]
- Mejia, J.R.; Fernandez-Chinguel, J.E.; Dolores-Maldonado, G.; Becerra-Chauca, N.; Goicochea-Lugo, S.; Herrera-Añazco, P.; Zafra-Tanaka, J.H.; Taype-Rondan, A. Diagnostic accuracy of urine dipstick testing for albumin-to-creatinine ratio and albuminuria: A systematic review and meta-analysis. Heliyon 2021, 7, e08253. [Google Scholar] [CrossRef]
- Zhang, W.; Chen, X.; Wang, Y.; Wu, L.; Hu, Y. Experimental and Modeling of Conductivity for Electrolyte Solution Systems. ACS Omega 2020, 5, 22465–22474. [Google Scholar] [CrossRef] [PubMed]
- Broeren, M.A.; Bahçeci, S.; Vader, H.; Arents, N.L. Screening for urinary tract infection with the Sysmex UF-1000i urine flow cytometer. J. Clin. Microbiol. 2011, 49, 1025–1029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.M.; Wen, C.Y.; Lin, C.Y.; Li, J.Y.; Lee, C.H.; Wu, M.F. Evaluating the performance of urine conductivity as screening for early stage chronic kidney disease. Clin. Lab. 2014, 60, 635–643. [Google Scholar] [CrossRef] [PubMed]
- Han, H. The Utility of Receiver Operating Characteristic Curve in Educational Assessment: Performance Prediction. Mathematics 2022, 10, 1493. [Google Scholar] [CrossRef]
- van Stralen, K.J.; Stel, V.S.; Reitsma, J.B.; Dekker, F.W.; Zoccali, C.; Jager, K.J. Diagnostic methods I: Sensitivity, specificity, and other measures of accuracy. Kidney Int. 2009, 75, 1257–1263. [Google Scholar] [CrossRef] [Green Version]
- Kavukcu, S.; Turkmen, M.; Soylu, A.; Kuralay, F. Could conductivity be used as a parameter in urinalysis? J. Pak. Med. Assoc. 1998, 48, 238–240. [Google Scholar]
- Palmer, B.F.; Clegg, D.J. The Use of Selected Urine Chemistries in the Diagnosis of Kidney Disorders. Clin. J. Am. Soc. Nephrol. 2019, 14, 306–316. [Google Scholar] [CrossRef] [Green Version]
- Umbrello, M.; Formenti, P.; Chiumello, D. Urine Electrolytes in the Intensive Care Unit: From Pathophysiology to Clinical Practice. Anesth. Analg. 2020, 131, 1456–1470. [Google Scholar] [CrossRef]
- Dhondup, T.; Qian, Q. Electrolyte and Acid-Base Disorders in Chronic Kidney Disease and End-Stage Kidney Failure. Blood Purif. 2017, 43, 179–188. [Google Scholar] [CrossRef]
- He, J.; Mills, K.T.; Appel, L.J.; Yang, W.; Chen, J.; Lee, B.T.; Rosas, S.E.; Porter, A.; Makos, G.; Weir, M.R.; et al. Urinary Sodium and Potassium Excretion and CKD Progression. J. Am. Soc. Nephrol. 2016, 27, 1202–1212. [Google Scholar] [CrossRef] [Green Version]
- Palmer, B.F. Regulation of Potassium Homeostasis. Clin. J. Am. Soc. Nephrol. 2015, 10, 1050–1060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeon, U.S. Kidney and calcium homeostasis. Electrolyte Blood Press 2008, 6, 68–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.W.; Park, J.T.; Yoo, T.H.; Lee, J.; Chung, W.; Lee, K.B.; Chae, D.W.; Ahn, C.; Kang, S.W.; Choi, K.H.; et al. Urinary Potassium Excretion and Progression of CKD. Clin. J. Am. Soc. Nephrol. 2019, 14, 330–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McQuarrie, E.P.; Traynor, J.P.; Taylor, A.H.; Freel, E.M.; Fox, J.G.; Jardine, A.G.; Mark, P.B. Association between urinary sodium, creatinine, albumin, and long-term survival in chronic kidney disease. Hypertension 2014, 64, 111–117. [Google Scholar] [CrossRef]
- Manoni, F.; Fornasiero, L.; Ercolin, M.; Tinello, A.; Ferrian, M.; Valverde, S.; Gessoni, G. Laboratory diagnosis of renal failure: Urine conductivity and tubular function. Ital. J. Urol. Nephrol. 2009, 61, 17–20. [Google Scholar]
- Yoo, D.-W.; Lee, S.M.; Moon, S.Y.; Kim, I.-S.; Chang, C.L. Evaluation of conductivity-based osmolality measurement in urine using the Sysmex UF5000. J. Clin. Lab. Anal. 2021, 35, e23586. [Google Scholar] [CrossRef]
- Chan, G.C.W.; Lam, B.; Yap, D.Y.H.; Ip, M.S.M.; Lai, K.N.; Tang, S.C.W. Proteinuria is associated with sleep apnea in chronic kidney disease. Nephrol. Dial. Transplant. 2015, 31, 772–779. [Google Scholar] [CrossRef]
- Ahmed Aziz, K.M. Association of High Levels of Spot Urine Protein with High Blood Pressure, Mean Arterial Pressure and Pulse Pressure with the Development of Diabetic Chronic Kidney Dysfunction or Failure among Diabetic Patients. Statistical Regression Modeling to Predict Diabetic Proteinuria. Curr. Diabetes Rev. 2019, 15, 486–496. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| All (n = 600) | Training Set (n = 300) | Validation Set (n = 300) | p-Value | |
|---|---|---|---|---|
| Age (years old) | 61.9 ± 15.0 | 61.5 ± 14.6 | 62.3 ± 15.5 | 0.522 |
| Sex | 0.286 | |||
| male/female (n, %) | 332 (55.3)/268 (44.7) | 159 (53.0)/141 (47.0) | 173 (57.7)/127 (42.3) | |
| eGFR (mL/min/1.73 m2) | 47.7 ± 26.6 | 46.6 ± 26.5 | 47.9 ± 26.7 | 0.917 |
| ≥90 (n, %) | 39 (6.5) | 19 (6.3) | 20 (6.7) | |
| 60–89 (n, %) | 136 (22.7) | 68 (22.7) | 68 (22.7) | |
| 30–59 (n, %) | 268 (44.7) | 134 (44.7) | 134 (44.7) | |
| 15–29 (n, %) | 84 (14.0) | 42 (14.0) | 42 (14.0) | |
| <15 (n, %) | 73 (12.2) | 37 (12.3) | 36 (12.0) | |
| Serum creatinine (mg/dL) | 2.13 ± 1.93 | 2.14 ± 2.04 | 2.12 ± 1.82 | 0.908 |
| Urine S.G. | 1.014 ± 0.006 | 1.014 ± 0.006 | 1.014 ± 0.006 | 0.645 |
| UO (mOsm/kg) | 192.4 ± 85.4 | 193.9 ± 88.9 | 190.9 ± 81.8 | 0.670 |
| Urine protein (mg/dL) | 82.3 ± 195.3 | 81.3 ± 192.3 | 83.3 ± 198.0 | 0.900 |
| <15 (mg/dL) (n, %) | 305 (50.8) | 150 (50.0) | 155 (51.7) | |
| ≥15 (mg/dL) (n, %) | 295 (49.2) | 150 (50.0) | 145 (48.3) | |
| Urine protein <15 (mg/dL) | 7.5 ± 3.2 | 7.5 ± 3.2 | 7.5 ± 3.2 | 0.934 |
| Urine protein ≥ 15 ( mg/dL) | 159.6 ± 256.7 | 155.1 ± 252.4 | 164.3 ± 261.9 | 0.759 |
| Urine glucose (mg/dL) κ | 1282 ± 1519.6 | 1180.9 ± 1531.6 | 1366.2 ± 1520.4 | 0.572 |
| Urine creatinine (mg/dL) λ | 86.1 ± 56.8 | 87.2 ± 59.6 | 84.8 ± 53.9 | 0.694 |
| Urine Na+ (mEq/L) | 70.2 ± 32.3 | 70.0 ± 32.6 | 70.8 ± 32.0 | 0.641 |
| Urine K+ (mEq/L) | 30.5 ± 18.6 | 31.3 ± 20.0 | 29.7 ± 17.2 | 0.289 |
| Urine Cl− (mEq/L) | 65.7 ± 37.2 | 65.4 ± 37.8 | 66.0 ± 36.6 | 0.854 |
| Urine Ca++ (mEq/L) | 4.9 ± 5.5 | 5.1 ± 6.1 | 4.8 ± 4.9 | 0.516 |
| UCond (mEq/L) | 10.8 ± 4.6 | 10.9 ± 4.8 | 10.8 ± 4.4 | 0.698 |
| Male (n = 332) | Female (n = 268) | p-Value | |
|---|---|---|---|
| Age (years old) | 62.3 ± 14.5 | 61.4 ± 15.7 | 0.485 |
| eGFR (mL/min/1.73 m2) | 47.0 ± 23.5 | 48.7 ± 30.0 | 0.442 |
| Serum creatinine (mg/dL) | 2.24 ± 1.78 | 2.01 ± 2.11 | 0.144 |
| Urine S.G. | 1.014 ± 0.067 | 1.013 ± 0.006 | 0.013 * |
| UO (mOsm/kg) | 194.2 ± 84.4 | 190.2 ± 86.7 | 0.563 |
| Urine protein (mg/dL) | 74.4 ± 152.3 | 92.1 ± 238.1 | 0.293 |
| Urine glucose (mg/dL) κ | 1649.3 ± 1714.3 | 751.3 ± 983.5 | 0.003 * |
| Urine creatinine (mg/dL) λ | 95.3 ± 58.5 | 72.6 ± 51.6 | 0.000 * |
| UCond (mEq/L) | 10.9 ± 4.6 | 10.7 ± 4.7 | 0.547 |
| eGFR | Urine Conductivity | |||||
|---|---|---|---|---|---|---|
| All | Male | Female | All | Male | Female | |
| Age | −0.288 * | −0.170 * | −0.385 * | 0.043 | 0.096 | −0.011 |
| Urine S.G. | 0.344 * | 0.311 * | 0.400 * | 0.628 * | 0.627 * | 0.642 * |
| Urine osmolality | 0.369 * | 0.355 * | 0.387 * | 1.000 * | 1.000 * | 1.000 * |
| Urine protein | −0.244 * | −0.419 * | −0.155 | −0.137 * | −0.186 * | −0.112 |
| Urine glucose | 0.278 | 0.416 | 0.225 | 0.038 | 0.040 | −0.058 |
| Urine creatinine | 0.143 | 0.243 * | 0.066 | 0.482 * | 0.446 * | −0.113 |
| Urine Na+ | 0.158 * | 0.113 | 0.208 * | 0.828 * | 0.832 * | 0.826 * |
| Urine K+ | 0.356 * | 0.381 * | 0.336 * | 0.699 * | 0.717 * | 0.684 * |
| Urine Cl− | 0.264 * | 0.229 * | 0.302 * | 0.893 * | 0.872 * | 0.920 * |
| Urine Ca++ | 0.478 * | 0.429 * | 0.538 * | 0.517 * | 0.495 * | 0.547 * |
| Urine conductivity | 0.366 * | 0.350 * | 0.385 * | - | - | - |
| eGFR = 90 | |||||||
|---|---|---|---|---|---|---|---|
| Age | ≥45 | ≥50 | ≥55 | ≥60 | ≥65 | ≥70 | All Ages |
| male | 0.541 | 0.542 | 0.530 | 0.301 | 0.563 | 0.466 | 0.685 |
| female | 0.588 | 0.617 | 0.553 | 0.410 | 0.443 | 0.289 | 0.620 |
| All | 0.573 | 0.591 | 0.540 | 0.361 | 0.489 | 0.374 | 0.637 |
| eGFR = 60 | |||||||
| Age | ≥45 | ≥50 | ≥55 | ≥60 | ≥65 | ≥70 | All ages |
| male | 0.710 | 0.712 | 0.645 | 0.636 | 0.552 | 0.588 | 0.675 |
| female | 0.694 | 0.703 | 0.723 | 0.697 | 0.660 | 0.670 | 0.691 |
| All | 0.702 | 0.708 | 0.683 | 0.664 | 0.613 | 0.634 | 0.683 |
| Nonstandardized Coefficients | t | p | R2 | ||
|---|---|---|---|---|---|
| β | Standard Error | ||||
| Formula 2 | 0.152 | ||||
| Constant | 25.541 | 4.465 | 5.721 | 0.000 | |
| UCond | 1.847 | 0.374 | 4.946 | 0.000 | |
| Formula 3 | 0.137 | ||||
| Constant | 26.686 | 4.676 | 5.707 | 0.000 | |
| UCond | 1.768 | 0.394 | 4.488 | 0.000 | |
| Formula 4 | 0.245 | ||||
| Constant | 69.563 | 16.419 | 4.237 | 0.000 | |
| UCond | 2.303 | 0.494 | 4.660 | 0.000 | |
| Age | −0.752 | 0.222 | −3.385 | 0.001 | |
| Formula 5 | 0.238 | ||||
| Constant | 78.160 | 19.077 | 4.097 | 0.000 | |
| UCond | 2.217 | 0.512 | 4.328 | 0.000 | |
| Age | −0.854 | 0.259 | −3.301 | 0.001 | |
| Subjects | Screening | Sn (%) | Sp (%) | Accuracy (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|---|---|
| Male ≥ 45 (n = 152) | UCond (F2) | 97.3 | 17.5 | 76.3 | 76.7 | 70.0 |
| Urine protein | 67.5 | 62.5 | 63.8 | 39.1 | 84.3 | |
| Male ≥ 50 (n = 145) | UCond (F3) | 99.1 | 7.90 | 75.2 | 75.2 | 75 |
| Urine protein | 65.8 | 62.6 | 63.4 | 38.5 | 83.8 | |
| Female ≥ 50 (n = 93) | UCond (F4) | 94.2 | 20.8 | 75.3 | 77.4 | 55.6 |
| Urine protein | 79.2 | 53.6 | 60.2 | 37.3 | 88.1 | |
| Female ≥ 55 (n = 83) | UCond (F5) | 98.4 | 30.0 | 81.9 | 81.6 | 85.7 |
| Urine protein | 75.0 | 57.1 | 61.4 | 35.7 | 87.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, M.-F.; Lee, C.-H.; Pai, P.-H.; Wang, J.-M. Screening Cases of Suspected Early Stage Chronic Kidney Disease from Clinical Laboratory Data: The Comparison between Urine Conductivity and Urine Protein. Biomedicines 2023, 11, 379. https://doi.org/10.3390/biomedicines11020379
Wu M-F, Lee C-H, Pai P-H, Wang J-M. Screening Cases of Suspected Early Stage Chronic Kidney Disease from Clinical Laboratory Data: The Comparison between Urine Conductivity and Urine Protein. Biomedicines. 2023; 11(2):379. https://doi.org/10.3390/biomedicines11020379
Chicago/Turabian StyleWu, Ming-Feng, Ching-Hsiao Lee, Po-Hsin Pai, and Jiunn-Min Wang. 2023. "Screening Cases of Suspected Early Stage Chronic Kidney Disease from Clinical Laboratory Data: The Comparison between Urine Conductivity and Urine Protein" Biomedicines 11, no. 2: 379. https://doi.org/10.3390/biomedicines11020379