
Researcher’s Perspective on Musculoskeletal Conditions in Primary Care Physiotherapy Units through the International Classification of Functioning, Disability, and Health (ICF): A Scoping Review
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Literature Search
2.3. Study Selection
2.4. Extraction of Relevant Concepts
2.5. Linkage of the Concepts to the ICF
2.6. Frequency Analysis
2.7. Comparison with the ICF Core Set for Post-Acute Musculoskeletal Conditions
3. Results
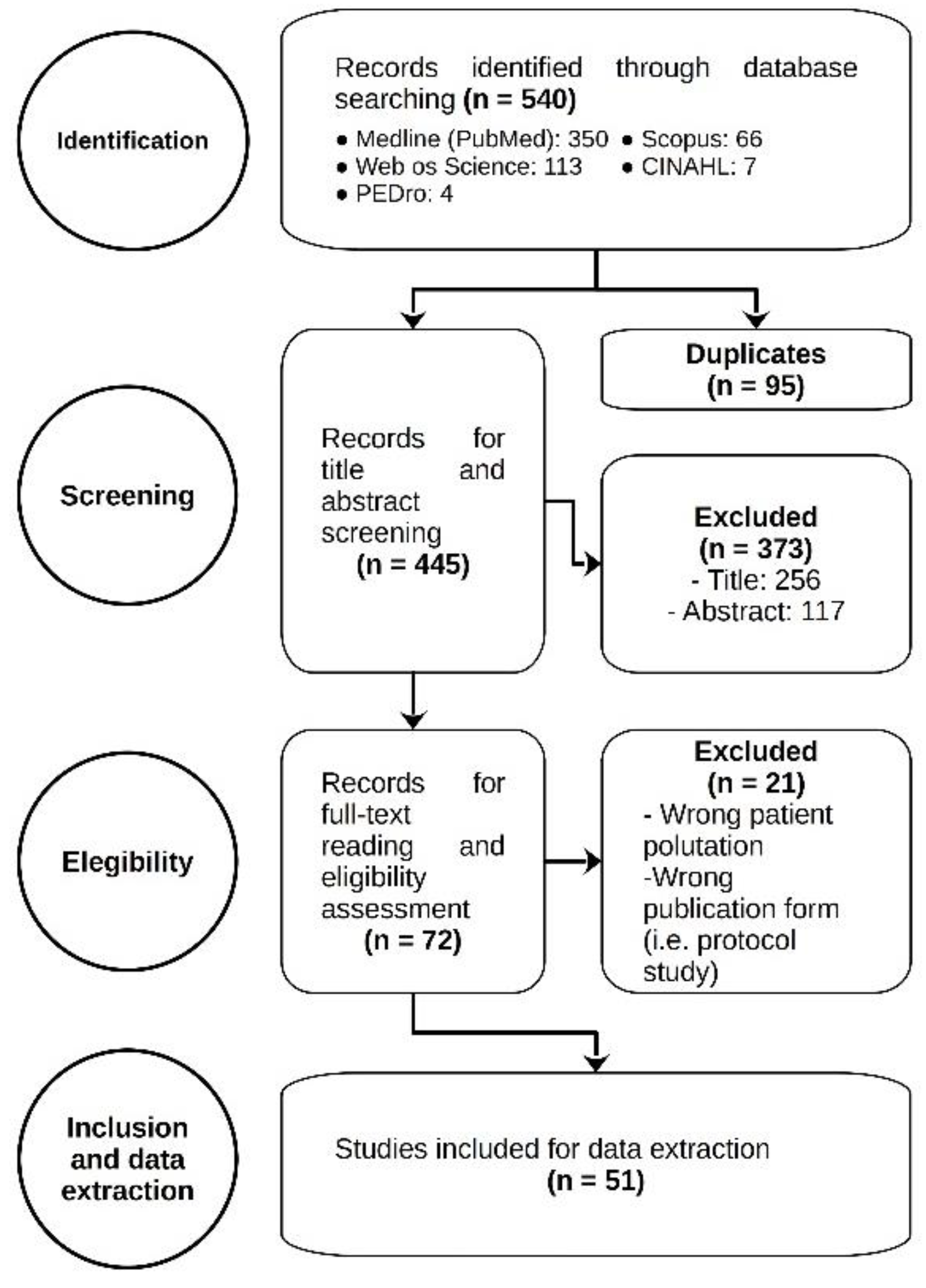
3.1. Study Selection
3.2. Study Characteristics
3.3. Outcome Measures
3.4. Linking Results
3.5. Comparison with Comprehensive ICF Core Set for Post-Acute Musculoskeletal Conditions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A. Search Strategy
- ((("Musculoskeletal Diseases"[Mesh] AND "Primary Health Care"[Mesh])) AND "Physical Therapy Modalities"[Mesh]) AND ("Outcome Assessment, Health Care"[Mesh] OR "Patient Reported Outcome Measures"[Mesh] OR "International Classification of Functioning, Disability and Health"[Mesh])
- (((musculoskeletal AND (disease* OR condition* OR disorder*)) AND (primary health care OR Community-Based Primary Care)) AND (physical therapy modalities OR physical therapy OR physiotherapy)) AND (body function* OR body structure* OR activit* OR participation* OR ICF OR international classification of functioning disability and health OR outcomes measures)
- musculoskeletal condition AND physiotherapy AND primary health care AND outcomes measures (title-abs-key)
- musculoskeletal disorder AND physiotherapy AND primary health care AND outcomes measures (title-abs-key)
- musculoskeletal condition AND physical therapy AND primary health care AND outcomes measures (title-abs-key)
- musculoskeletal disorder AND physical therapy AND primary health care AND outcomes measures (title-abs-key)
- musculoskeletal condition AND physiotherapy AND primary health care AND outcomes measures
- musculoskeletal disorder AND physiotherapy AND primary health care AND outcomes measures
- musculoskeletal condition AND physical therapy AND primary health care AND outcomes measures
- musculoskeletal disorder AND physical therapy AND primary health care AND outcomes measures
- musculoskeletal condition AND physiotherapy AND primary health care AND outcomes measures
- musculoskeletal disorder AND physiotherapy AND primary health care AND outcomes measures
- musculoskeletal condition AND physical therapy AND primary health care AND outcomes measures
- musculoskeletal disorder AND physical therapy AND primary health care AND outcomes measures
- musculoskeletal disorder physical therapy primary health care outcomes measures
- musculoskeletal disorder physiotherapy primary health care outcomes measures
- musculoskeletal condition physical therapy primary health care outcomes measures
- musculoskeletal condition physiotherapy primary health care outcomes measures
Appendix B

{kind=link}
| Study | Country | Design | Sample Size | Participants | Outcome Measures * | ||
|---|---|---|---|---|---|---|---|
| Age (Years) | Female/Male | Pathology | |||||
| Abbot et al. (2019) | New Zealand | Experimental (RCT) | 206 | 37-92 | 114/92 | Hip or knee osteoarthritis | Primary: WOMAC Secondary: NPRS, WT, STS, TUG, AdEv |
| Allen et al. (2017) | United States of America | Experimental (RCT) | 537 | NR | 397/140 | Hip or knee osteoarthritis | Primary: WOMAC Secondary: PHQ, SPPB, ATU, PAL |
| Amorim et al. (2019) | Australia | Experimental (RCT) | 68 | >18 | 34/34 | Chronic low back pain | Primary: CS, NPRS, RMDQ Secondary: PAL, DASS, FABQ, IPAQ, PSQI |
| Arden et al. (2017) | United Kingdom | Observational (RCS) | 62 | >18 | 39/23 | Low back pain | Primary: BQ, WT, ST, STS |
| Battista et al. (2021) | Italy | Observational (DQS) | 11 | NR | 6/5 | Hip and knee osteoarthritis | Primary: DQ (3) |
| Benell et al. (2017) | Australia | Experimental (RCT) | 148 | >50 | 83/65 | Chronic Knee Pain | Primary: NPRS, WOMAC Secondary: GROC, PCS, AQLI, ASES, CSQ, AdEv |
| Benell et al. (2014) | Australia | Experimental (RCT) | 78 | NR | 42/36 | Knee osteoarthritis | Primary: VAS, WOMAC Secondary: Adh |
| Bornhöft et al. (2019) | Sweden | Experimental (RCT) | 55 | 16-67 | 34/21 | Musculoskeletal disorders | Primary: NPRS, DRI, EQL5, OMPQ Secondary: ARM |
| Burns et al. (2018) | United States of America | Experimental (RCT) | 90 | ≥18 | 37/53 | Low back pain | Primary: NPRS, ODI, GROC |
| Chesterton et al. (2013) | United Kingdom | Experimental (RCT) | 241 | NR | 109/132 | Tennis elbow | Primary: NPRS Secondary: GROC, PRTEE, EQL5, IPQ, SF-12 |
| Christiansen et al. (2018) | Denmark | Observational (PCS) | 160 | >18 | 90/70 | Neck, shoulder, and low-back pain | Primary: DASH, NPRS, NDI, OMPQ, RMDQ, WHO5 |
| Costa et al. (2022) | Portugal | Experimental (NCIS) | 343 | >18 | 205/138 | Musculoskeletal pain | Primary: NPRS Secondary: ATU (2), GAD, PHQ, FABQ, WPAI, Adh |
| Crossley et al. (2015) | Australia | Experimental (RCT) | 92 | >40 | 53/39 | Patelofemoral osteoarthritis | Primary: GROC, KOOS, VAS Secondary: Adh, AdEv |
| Cuesta-Vargas et al. (2015) | Spain | Experimental (RCT) | 114 | NR | NR | Chronic musculoskeletal disorders | Primary: SF-12, EQL5, VAS, RMDQ, NDI, WOMAC |
| Darlow et al. (2019) | New Zealand | Experimental (RCT) | 221 | NR | 105/116 | Low back pain | Primary: RMDQ Secondary: NPRS, DRS, PS, EQL5, OCCQ, PSEQ, PyScFQ (4) |
| Emilson et al. (2017) | Sweden | Experimental (RCT) | 43 | 18-65 | 30/10/22 | Musculoskeletal pain | Primary: NPRS, PDI, TSK, PR |
| Ferrer-Peña et al. (2019) | Spain | Observational (CSS) | 49 | NR | 41/8 | Greater trochanteric pain syndrome | Primary: PPSA, GCPS, PPT, TS, CPMI, VAS |
| Gohir et al (2021) | United Kingdom | Experimental (RCT) | 105 | >45 | 71/34 | Knee osteoarthritis | Primary: NPRS Secondary: WOMAC, STS, TUG, MHQ, MVC, PPT, TS, CPM, SQM, PSQI, MUA |
| Goldberg et al. (2018) | United States of America | Observational (CSS) | 853 | >18 | 458/395 | Musculoskeletal pain | Primary: TSK, SF-8 |
| Hill et al. (2020) | United Kingdom | Experimental (RCT) | 524 | NR | 318/206 | Musculoskeletal pain (back, neck, knee or multi-site pain) | Primary: RMDQ, NDI, SPADI, KOOS, SF-12 Secondary: STMT, MHQ, TSK, ECRQ, EQL5, PS, GROC, WA, WP, PQ |
| Hopewell et al. (2021) | United Kingdom | Experimental (RCT) | 708 | >18 | 349/359 | A rotator cuff disorder | Primary: SPADI Secondary: EQL5 |
| Laslett et al. (2014) | New Zealand | Observational (PCS) | 161 | >18–81 | 82/79 | Shoulder pain | Primary: SPADI, VAS, FABQ, SF-8, DRS |
| Leaver et al. (2013) | Australia | Observational (PCS) | 181 | 18-70 | 117/64 | Cervical pain | Primary: PR Secondary: NPRS, NDI |
| Leemans et al. (2021) | Belgium | Experimental (RCT) | 50 | 25-80 | 27/23 | Low back pain | Primary: NPRS, BPS Secondary: PPT, TS, CPM, FABQ, SF-36, CSI, ATU |
| Legha et al. (2020) | United Kingdom | Experimental (RCT) | 1083 | NR | 619/464 | Knee osteoarthritis | Primary: WOMAC |
| Lentz et al. (2018) | United States of America | Observational (PCS) | 440 | NR | 275/164 | Neck, low back, knee or shoulder | Primary: PQ (2), NPRS, NDI, ODI, DASH, IKDF, OSPRO-ROS, OSPRO-YF |
| Lewis et al. (2017) | United Kingdom | Experimental (RCT) | 227 | >18 | 109/118 | Subacromial pain syndrome | Primary: OSS Secondary: SPADI, VAS, DVAS, PQ, ROM, OT-NS, OT-HT |
| Lingner et al. (2018) | Germany | Experimental (RCT) | 87 | 18-50 | 44/43 | Low back pain | Primary: NPRS, VAS Secondary: ATU (3), HFAQ, GROC, WA, PS |
| López-López et al. (2015) | Spain | Experimental (RCT) | 48 | 18-65 | 42/6 | Chronic neck pain | Primary: VAS Secondary: ROM, PPT, STAI, BDI, TSK, PCS |
| Marra et al. (2012) | Canada | Experimental (RCT) | 139 | ≥ 50 | 79/60 | Knee osteoarthritis | Primary: OA-QI Secondary: HUI3, LEFS, PAT5, WOMAC |
| Matarán-Peñarrocha et al. (2020) | Spain | Experimental (RCT) | 64 | 18-65 | 32/32 | Chronic non specific low back pain | Primary: MQ-OT, FTFd, ODI, RMDQ, TSK, VAS |
| Miedema et al. (2016) | Netherlands | Observational (PCS) | 682 | 18-64 | 286/396 | Musculoskeletal pain of arm, neck and shoulder | Primary: DASH, PR |
| Minns Lowe et al. (2020) | United Kingdom | Experimental (RCT) | 41 | >18 | 20/21 | Musculoskeletal disorders | Primary: WT Secondary: PAL (2), NPRS, PANAS, GSES, SF-36 (1), PR, DAQ |
| Molgaard Nielsen et al. (2017) | Denmark | Observational (PCS) | 928 | 18-65 | 418/510 | Low back pain | Primary: NPRS, RMDQ Secondary: PQ (3) |
| Moseng et al. (2020) | Norway | Experimental (RCT) | 393 | ≥45 | 280/113 | Hip and/or knee osteoarthritis | Primary: NPRS, DQ (2), ROM, HOOS, KOOS |
| Murphy et al. (2013) | Ireland | Observational (PCS) | 1532 | NR | 958/574 | Low back pain | Primary: VAS, RMDQ, DRAM, BBQ, ROM, MSPQ, SFAT |
| Noblet et al. (2020) | England | Experimental (RCT) | 29 | >18 | 17/12/22 | Low back pain | Primary: NPRS, RMDQ Secondary: EQL5, TSK, PAL, WA, ATU (2) |
| Østerås et al. (2014) | Norway | Experimental (RCT) | 130 | 40-79 | 117/13 | Hand osteoarthritis | Primary: FIHOA, NPRS, PSFS, DQ Secondary: ROM, GROC, DQ, MVC, MPU-OT, Adh, AdEv |
| Østerås et al. (2019) | Norway | Experimental (RCT) | 393 | ≥45 | 279/114 | Hip and/or knee osteoarthritis | Primary: OA-QI Secondary: PS, PAL, PR |
| Paanalahti et al. (2016) | Sweden | Experimental (RCT) | 1057 | 18–65 | 740/317 | Neck pain and/or back pain | Primary: CPQ, NPRS, DQ (3) Secondary: PR, ATU |
| Palacín-Marín et al. (2013) | Spain | Experimental (RCT) | 15 | >18 | 06/09 | Lumbar pain | Primary: ROM, ST-OT, SLR-OT, ODI, VAS, SF-12, TSK |
| Sandal et al. (2021) | Denmark | Experimental (RCT) | 461 | >18 | 255/206 | Low back pain | Primary: RMDQ Secondary: NPRS, PSEQ, FABQ, IPQ, EQL5, GROC, SGPAL |
| Schroder et al. (2021) | Sweden | Experimental (RCT) | 467 | 18-65 | 204/263 | Low back pain | Primary: NPRS, ODI Secondary: IPQ, EQL5, PEI, GROC, PS |
| Schuetze et al. (2014) | Australia | Experimental (NCIS) | 16 | 18-65 | 12/04/22 | Low back pain | Primary: OMPQ, ODI, DASS, MAAS, PCS, CPAQ, SF-36, ClSQ |
| Trulsson Schouenborg et al. (2021) | Sweden | Observational (PCS) | 274 | >18 | 194/80 | Chronic musculoskeletal pain | Primary: NPRS Secondary: DRI, EQL5 |
| Uhl et al. (2017) | United States of America | Observational (RCS) | 128 | NR | 74/53 | Shoulder pain | Primary: PQ, NPRS, Adh, ATU, DASH |
| Van der Maas et al. (2015) | Netherlands | Experimental (RCT) | 94 | NR | 77/17 | Chronic musculoskeletal pain | Primary: NPRS, BDI, SF-36, PDI, SBC, PSEQ, PCS |
| Vibe Fersum et al. (2019) | Norway | Experimental (RCT) | 121 | 18-65 | 33/88 | Non-specific low back pain | Primary: OMPQ Secondary: ODI, HSC, FABQ |
| Vibe Fersum et al. (2013) | Norway | Experimental (RCT) | 121 | 18-65 | 63/58 | Non-specific low back pain | Primary: NPRS, ODI Secondary: HSC, FABQ, ROM, PS, WA, CS |
| Williams et al (2019) | United Kingdom | Experimental (RCT) | 440 | >18 | 288/152 | Musculoskeletal disorders | Primary: PSFS Secondary: EQL5, PAM, MRI |
| Xia et al. (2016) | United States of America | Experimental (RCT) | 192 | 21-54 | 88/104 | Low back pain | Primary: RMDQ Secondary: VAS, FABQ, SF-36 |
Appendix C
| Assessment Instrument | No of Studies | Type | Main Theme |
|---|---|---|---|
| Illness Perception Questionnaire | 3 | Multi-item | Other |
| Knee injury and Osteoarthritis Outcome Score (KOOS) | 3 | Multi-item | Disability |
| Pain self-efficacy questionnaire (PSEQ) | 3 | Multi-item | Disability |
| Sit-to-stand test | 3 | Single-item | Physical performance |
| Temporal summation | 3 | Single-item | Pain description |
| Walking test | 3 | Single-item | Physical performance |
| Beck Depression Inventory | 2 | Multi-item | Psychosocial factors |
| Care seeking | 2 | Single-item | Other (indirect recovery) |
| Conditional pain modulation | 2 | Single-item | Pain description |
| Depression Anxiety Stress Scales (DASS) | 2 | Multi-item | Psychosocial factors |
| Disability Rating Index (DRI) | 2 | Multi-item | Disability |
| Disability Rating Scale | 2 | Single-item | Disability |
| Hopkins Symptoms Checklist | 2 | Multi-item | Psychosocial factors |
| Musculoskeletal Health Questionnaire | 2 | Multi-item | Disability |
| OsteoArthritis Quality Indicator questionnaire | 2 | Multi-item | Other (environmental factor) |
| Pain Disability Index | 2 | Multi-item | Disability |
| Patient Health Questionnaire (PHQ) | 2 | Multi-item | Psychosocial factors |
| Patient-Specific Function Scale (PSFS) | 2 | Multi-item | Disability |
| Peak muscle strength | 2 | Single-item | Physical measure |
| Pittsburgh Sleep Quality Index | 2 | Multi-item | Other (sleep) |
| Short Form Health Survey 8 questionnaire (SF-8) | 2 | Multi-item | Quality of life related to health |
| Timed up and go (TUG) | 2 | Single-item | Physical performance |
| Arthritis Self-Efficacy Scale | 1 | Multi-item | Disability |
| Assessment Quality of Life Instrument (AQLI) | 1 | Multi-item | Quality of life related to health |
| Attitudes regarding Responsibility for Musculoskeletal disorders scale (ARM) | 1 | Multi-item | Other (environmental factor) |
| Back Beliefs Questionnaire (BBQ) | 1 | Multi-item | Psychosocial factors |
| Back Performance Scale (BPS) | 1 | Multi-item | Disability |
| Bournemouth Questionnaire | 1 | Multi-item | Pain description |
| Central Sensitization Inventory (CSI) | 1 | Multi-item | Pain description |
| Chronic Pain Acceptance Questionnaire (CPAQ) | 1 | Multi-item | Psychosocial factors |
| Chronic Pain Assessment Questionnaire (CPQ) | 1 | Multi-item | Pain description |
| Client Satisfaction Questionnaire (CSQ) | 1 | Multi-item | Other |
| Conditioned Pain Modulation Index (CPMI) | 1 | Multi-item | Pain description |
| Coping Strategies Questionnaire | 1 | Multi-item | Psychosocial factors |
| Daily Activities Questionnaire | 1 | Multi-item | Disability |
| Disability Visual Analog Scale | 1 | Single-item | Disability |
| Distress and Risk Assessment Method (DRAM) | 1 | Multi-item | Psychosocial factors |
| Effective Consultation and Reassurance Questionnaire (ECRQ) | 1 | Multi-item | Other (environmental factor) |
| Finger-to-floor distance | 1 | Single-item | Physical measure |
| Functional Index for Hand OsteoArthritis | 1 | Multi-item | Disability |
| General Self-Efficacy Scale | 1 | Multi-item | Disability |
| Generalized Anxiety Disorder (GAD) | 1 | Multi-item | Psychosocial factors |
| Graded Chronic Pain Scale (GCPS) | 1 | Multi-item | Pain description |
| Hannover functional ability questionnaire (FfbH-R) | 1 | Multi-item | Disability |
| Hawkin’s test | 1 | Single-item | Physical measure (orthopaedic) |
| Health Utilities Index Mark 3 (HUI3) | 1 | Multi-item | Quality of life related to health |
| Hip disability and Osteoarthritis Outcome Score (HOOS) | 1 | Multi-item | Disability |
| International Knee Documentation Committee Subjective Knee Form (IKDC) | 1 | Multi-item | Disability |
| International Physical Activity Questionnaire | 1 | Multi-item | Physical performance |
| Lower Extremities Function Scale (LEFS) | 1 | Multi-item | Disability |
| McQuade test | 1 | Single-item | Physical measure (orthopaedic) |
| MedRisk instrument | 1 | Multi-item | Other (environmental factor) |
| Mindful Attention Awareness Scale (MAAS) | 1 | Multi-item | Other (self-perception) |
| Moberg Pick-up Test | 1 | Single-item | Physical measure (orthopaedic) |
| Modified somatic perception questionnaire | 1 | Multi-item | Other (self-perception) |
| Musculoskeletal ultrasonographic assessment | 1 | Single-item | Other |
| Neer sign | 1 | Single-item | Physical measure (orthopaedic) |
| OSPRO Review of Systems tool (OSPRO-ROS) | 1 | Multi-item | Psychosocial factors |
| OSPRO Yellow Flag tool (OSPRO-YF) | 1 | Multi-item | Psychosocial factors |
| Otago Costs and Consequences Questionnaire for Low Back Pain | 1 | Multi-item | Other (environmental factor) |
| Oxford Shoulder Score | 1 | Multi-item | Disability |
| Pain Enablement Instrument | 1 | Multi-item | Other (self-management) |
| Paper Adaptive Test-5D (PAT- 5D) | 1 | Multi-item | Quality of life related to health |
| Patient Activation Measure | 1 | Multi-item | Other (self-management ) |
| Patient-rated Tennis Elbow Evaluation (PRTEE) | 1 | Multi-item | Disability |
| Percentage Pain Surface Area (PPSA) | 1 | Single-item | Pain description |
| Positive and negative affect schedule (PANAS scale) | 1 | Multi-item | Psychosocial factors |
| Question about work productivity | 1 | Single-item | Other (environmental factor) |
| Saltin-Grimby Physical Activity Level Scale | 1 | Multi-item | Physical performance |
| Scale of Body Connection (SBC) | 1 | Multi-item | Other (self-perception) |
| Short Physical Performance Battery (SPPB) | 1 | Multi-item | Physical performance |
| Simmond’s functional assessment tool | 1 | Multi-item | Physical performance |
| Sleep quality measure | 1 | Single-item | Other (sleep) |
| Sorensen test | 1 | Single-item | Physical measure (orthopaedic) |
| StarT MSK tool | 1 | Multi-item | Disability |
| State Trait Anxiety Inventory (STAI) | 1 | Multi-item | Psychosocial factors |
| Step test | 1 | Single-item | Physical performance |
| Straight leg raise | 1 | Single-item | Physical measure (orthopaedic) |
| WHO 5 Well-being Index | 1 | Multi-item | Quality of life related to health |
| Work Productivity and Activity Impairment (WPAI) | 1 | Multi-item | Other (environmental factor) |
Appendix D
| ICF Category | ICF Chapter (Theme) * | Count |
|---|---|---|
| b130 Energy and drive functions | b1 Mental functions (global mental functions) | 73 |
| b134 Sleep functions (B) | b1 a, b | 58 |
| b152 Emotional functions | b1 Mental functions (specific mental functions) | 104 |
| b260 Proprioceptive function (B) | b2 Sensory functions and pain (additional sensory functions) | 4 |
| b270 Sensory functions related to temperature and other stimuli | b2 Sensory functions and pain b | 3 |
| b280 Sensation of pain (B) | b2 Sensory functions and pain (pain) | 207 |
| b415 Blood vessel functions | b4 Functions of the cardiovascular, haematological, immunological and respiratory systems (functions of the cardiovascular system) | 1 |
| b435 Immunological system functions (B) | b4a (functions of the haematological and immunological systems) | 0 |
| b440 Respiration functions | b4 a (functions of the respiratory system) | 11 |
| b455 Exercise tolerance functions | b4 a (additional functions and sensations of the cardiovascular and respiratory systems) | 45 |
| b525 Defecation functions | b5 Functions of the digestive, metabolic and endocrine systems (functions related to the digestive system) | 2 |
| b530 Weight maintenance functions (B) | b5 a,b | 11 |
| b620 Urination functions (B) | b6 Genitourinary and reproductive functions (urinary functions) | 4 |
| b710 Mobility of joint functions | b7 Neuromusculoskeletal and movement-related functions (functions of the joints and bones) | 104 |
| b715 Stability of joint functions | b7 a,b | 92 |
| b730 Muscle power functions (B) | b7a (muscle functions) | 104 |
| b735 Muscle tone functions | b7 a,b | 99 |
| b740 Muscle endurance functions (B) | b7 a.b | 99 |
| b755 Involuntary movement reaction functions (B) | b7 a (movement functions) | 93 |
| b760 Control of voluntary movement functions | b7 a,b | 94 |
| b770 Gait pattern functions | b7 a,b | 66 |
| b780 Sensations related to muscles and movement functions (B) | b7 a,b | 29 |
| b810 Protective functions of the skin | b8 Functions of the skin and related structures (functions of the skin) | 1 |
| d155 Acquiring skills (B) | d1 a (basic learning) | 0 |
| d177 Making decisions (B) | d1 a (applying knowledge) | 5 |
| d230 Carrying out daily routine (B) | d2 General tasks and demands | 23 |
| d240 Handling stress and other psychological demands (B) | d2 a | 41 |
| d310 Communicating with - receiving - spoken messages | d3 Communication (communicating with – receiving – spoken messages) | 0 |
| d410 Changing basic body position (B) | d4 Mobility (changing and maintaining body position) | 46 |
| d415 Maintaining a body position (B) | d4 a,b | 64 |
| d420 Transferring oneself | d4 a,b | 13 |
| d430 Lifting and carrying objects (B) | d4 Mobility (carrying, moving and handling objects) | 43 |
| d440 Fine hand use | d4 a,b | 32 |
| d445 Hand and arm use (B) | d4 a,b | 16 |
| d450 Walking (B) | d4 Mobility (walking and moving) | 90 |
| d460 Moving around in different locations | d4 a,b | 44 |
| d465 Moving around using equipment (B) | d4 a,b | 29 |
| d510 Washing oneself (B) | d5 Self-care (theme not available) | 70 |
| d520 Caring for body parts (B) | d5 a,b | 12 |
| d530 Toileting (B) | d5 a,b | 19 |
| d540 Dressing (B) | d5 a,b | 83 |
| d550 Eating (B) | d5 a,b | 18 |
| d560 Drinking | d5 a,b | 18 |
| d570 Looking after one’s health | d5 a,b | 49 |
| d760 Family relationships | d7 Interpersonal interactions and relationships (particular interpersonal interactions) | 48 |
| e110 Products or substances for personal consumption (B) | e1 Products and technology (theme not available) | 36 |
| e115 Products and technology for personal use in daily living (B) | e1 a,b | 24 |
| e120 Products and technology for personal indoor and outdoor mobility and transportation (B) | e1 a,b | 37 |
| e125 Products and technology for communication | e1 a,b | 0 |
| e150 Design, construction and building products and technology of buildings for public use | e1 a,b | 1 |
| e225 Climate (B) | e2 Natural environment and human-made changes to environment (theme not available) | 0 |
| e310 Immediate family | e3 Support and relationships (theme not available) | 13 |
| e320 Friends | e3 a,b | 14 |
| e340 Personal care providers and personal assistants | e3 a,b | 14 |
| e355 Health professionals (B) | e3 a,b | 73 |
| e410 Individual attitudes of immediate family members | e4 Attitudes (theme not available) | 0 |
| e420 Individual attitudes of friends | e4 a,b | 0 |
| e430 Individual attitudes of people in positions of authority | e4 a,b | 6 |
| e440 Individual attitudes of personal care providers and personal assistants | e4 a,b | 0 |
| e450 Individual attitudes of health professionals (B) | e4 a,b | 63 |
| e555 Associations and organizational services, systems and policies | e5 Services, systems and policies (theme not available) | 0 |
| e575 General social support services, systems and policies | e5 a,b | 0 |
| e580 Health services, systems and policies | e5 a,b | 73 |
| s710 Structure of head and neck region | s7 Structures related to movement | 8 |
| s720 Structure of shoulder region | s7 a | 19 |
| s730 Structure of upper extremity | s7 a | 12 |
| s740 Structure of pelvic region | s7 a | 1 |
| s750 Structure of lower extremity | s7 a | 15 |
| s760 Structure of trunk | s7 a | 33 |
| s810 Structure of areas of skin | s8 Skin and related structures | 0 |
Appendix E
| ICF code | Description | Count | Included in studies (%) |
|---|---|---|---|
| d859 | Work and employment, other specified and unspecified | 89 | 86.3 |
| b720 | Mobility of bone functions | 93 | 82.4 |
| b180 | Experience of self and time functions | 82 | 74.5 |
| d640 | Doing housework | 54 | 72.5 |
| b160 | Thought functions | 70 | 68.6 |
| d920 | Recreation and leisure | 65 | 68.6 |
| d455 | Moving around | 44 | 52.9 |
| d649 | Household tasks, other specified and unspecified | 40 | 51.0 |
| b126 | Temperament and personality functions | 42 | 49.0 |
| d299 | General tasks and demands, unspecified | 32 | 45.1 |
| d910 | Community life | 37 | 41.2 |
| d620 | Acquisition of goods and services | 28 | 37.3 |
| d999 | Community, social and civic life, unspecified | 38 | 35.3 |
| d160 | Focusing attention | 14 | 33.3 |
| b289 | Sensation of pain, unspecified Sensation of pain, other specified (conditional pain modulation) Sensation of pain, other specified (temporal summation) | 23 3 3 | 29.4 5.9 5.9 |
| d899 | Major life areas, unspecified | 33 | 25.5 |
| d770 | Intimate relationships | 17 | 25.5 |
| e399 | Support and relationships, unspecified | 14 | 25.5 |
| e570 | Social security services, systems and policies | 23 | 23.5 |
| d429 | Changing and maintaining body position, other specified and unspecified | 19 | 23.5 |
| b140 | Attention functions | 16 | 23.5 |
| d159 | Basic learning, other specified and unspecified | 5 | 23.5 |
| d699 | Domestic life, unspecified | 25 | 21.6 |
| d850 | Remunerative employment | 18 | 21.6 |
| d750 | Informal social relationships | 14 | 21.6 |
| d650 | Caring for household objects | 12 | 21.6 |
| d163 | Thinking | 18 | 19.6 |
| d740 | Formal relationships | 11 | 19.6 |
| d599 | Self-care, unspecified | 10 | 19.6 |
| e325 | Acquaintances, peers, colleagues, neighbours and community members | 11 | 17.6 |
| d630 | Preparing meals | 11 | 15.7 |
| b122 | Global psychosocial functions | 10 | 15.7 |
| d730 | Relating with strangers | 9 | 13.7 |
| d449 | Carrying, moving and handling objects, other specified and unspecified | 7 | 13.7 |
| e499 | Attitudes, unspecified | 7 | 13.7 |
| d820 | School education | 7 | 11.8 |
| b265 | Touch function | 6 | 11.8 |
| d845 | Acquiring, keeping and terminating a job | 6 | 11.8 |
| d110 | Watching | 5 | 11.8 |
| d799 | Interpersonal interactions and relationships, unspecified | 5 | 11.8 |
| d855 | Non-remunerative employment | 19 | 9.8 |
| d166 | Reading | 13 | 9.8 |
| b164 | Higher-level cognitive functions | 7 | 9.8 |
| b765 | Involuntary movement functions | 6 | 9.8 |
| d879 | Economic life, other specified and unspecified (economic charge for the family) | 9 | 7.8 |
| e330 | People in positions of authority | 6 | 7.8 |
| b144 | Memory functions | 5 | 7.8 |
| b210 | Seeing functions | 5 | 7.8 |
| d170 | Writing | 5 | 7.8 |
| d330 | Speaking | 5 | 7.8 |
| e425 | Individual attitudes of acquaintances, peers, colleagues, neighbours and community members | 5 | 7.8 |
| b110 | Consciousness functions | 4 | 7.8 |
| b240 | Sensations associated with hearing and vestibular function | 4 | 7.8 |
| d475 | Driving | 4 | 7.8 |
| d489 | Moving around using transportation, other specified and unspecified | 4 | 7.8 |
| e315 | Extended family | 4 | 7.8 |
| s770 | Additional musculoskeletal structures related to movement | 9 | 5.9 |
| d138 | Acquiring information | 6 | 5.9 |
| d175 | Solving problems | 6 | 5.9 |
| d930 | Religion and spirituality | 6 | 5.9 |
| d470 | Using transportation | 5 | 5.9 |
| d720 | Complex interpersonal interactions | 5 | 5.9 |
| b114 | Orientation functions | 3 | 5.9 |
| b410 | Heart functions | 3 | 5.9 |
| b449 | Functions of the respiratory system, other specified and unspecified | 3 | 5.9 |
| b510 | Ingestion functions | 3 | 5.9 |
| d660 | Assisting others | 3 | 5.9 |
| b450 | Additional functions of the respiratory system | 2 | 5.9 |
| b156 | Perceptual functions | 3 | 3.9 |
| b230 | Hearing functions | 3 | 3.9 |
| d710 | Basic interpersonal interactions | 3 | 3.9 |
| b235 | Vestibular functions | 2 | 3.9 |
| d729 | General interpersonal interactions, other specified and unspecified | 2 | 3.9 |
| d779 | Particular interpersonal relationships, other specified and unspecified | 2 | 3.9 |
| b749 | Muscle functions, other specified and unspecified (flexibility) | 1 | 3.9 |
| e398 | Support and relationships, other specified | 1 | 3.9 |
| b139 | Global mental functions, other specified and unspecified | 3 | 2.0 |
| d179 | Applying knowledge, other specified and unspecified (disease prevention) | 2 | 2.0 |
| b117 | Intellectual functions | 1 | 2.0 |
| b460 | Sensations associated with cardiovascular and respiratory functions | 1 | 2.0 |
| b599 | Functions of the digestive, metabolic and endocrine systems, unspecified | 1 | 2.0 |
| b830 | Other functions of the skin | 1 | 2.0 |
| b840 | Sensation related to the skin | 1 | 2.0 |
| e455 | Individual attitudes of other professionals | 1 | 2.0 |
| e498 | Attitudes, other specified (criticism) | 1 | 2.0 |
| e590 | Labour and employment services, systems and policies | 1 | 2.0 |
| s120 | Spinal cord and related structures | 1 | 2.0 |
References
- Cieza, A.; Causey, K.; Kamenov, K.; Hanson, S.W.; Chatterji, S.; Vos, T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2021, 396, 2006–2017. [Google Scholar] [CrossRef] [PubMed]
- Arendt-Nielsen, L.; Fernández-De-Las-Peñas, C.; Graven-Nielsen, T. Basic aspects of musculoskeletal pain: From acute to chronic pain. J. Man. Manip. Ther. 2011, 19, 186–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cimmino, M.A.; Ferrone, C.; Cutolo, M. Epidemiology of chronic musculoskeletal pain. Best Pract. Res. Clin. Rheumatol. 2011, 25, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Demont, A.; Bourmaud, A.; Kechichian, A.; Desmeules, F. The impact of direct access physiotherapy compared to primary care physician led usual care for patients with musculoskeletal disorders: A systematic review of the literature. Disabil. Rehabil. 2021, 43, 1637–1648. [Google Scholar] [CrossRef]
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. Lancet Low Back Pain Series Working Group, What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. International Classification of Functioning, Disability and Health; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Leonardi, M.; Lee, H.; Kostanjsek, N.; Fornari, A.; Raggi, A.; Martinuzzi, A.; Yáñez, M.; Almborg, A.-H.; Fresk, M.; Besstrashnova, Y.; et al. 20 Years of ICF—International Classification of Functioning, Disability and Health: Uses and Applications around the World. Int. J. Environ. Res. Public Health 2022, 19, 11321. [Google Scholar] [CrossRef]
- Bickenbach, J.; Cieza, A.; Selb, M. ICF Core Sets. Manual for Clinical Practice, 2nd ed.; Hogrefe: Göttingen, Germany, 2021. [Google Scholar]
- Stoll, T.; Brach, M.; Huber, E.O.; Scheuringer, M.; Schwarzkopf, S.R.; Konstanjsek, N.; Stucki, G. ICF Core Set for patients with musculoskeletal conditions in the acute hospital. Disabil. Rehabil. 2005, 27, 381–387. [Google Scholar] [CrossRef]
- Scheuringer, M.; Stucki, G.; Huber, E.O.; Brach, M.; Schwarzkopf, S.R.; Kostanjsek, N.; Stoll, T. ICF Core Set for patients with musculoskeletal conditions in early post-acute rehabilitation facilities. Disabil. Rehabil. 2005, 27, 405–410. [Google Scholar] [CrossRef]
- Grill, E.; Ewert, T.; Chatterji, S.; Kostanjsek, N.; Stucki, G. ICF Core Sets development for the acute hospital and early post-acute rehabilitation facilities. Disabil. Rehabil. 2005, 27, 361–366. [Google Scholar] [CrossRef]
- Hernández-Lázaro, H.; Mingo-Gómez, M.T.; Ceballos-Laita, L.; Medrano-de-la-Fuente, R.; Jiménez-Del Barrio, S. Validation of the international classification of functioning, disability, and health (ICF) core sets for musculoskeletal conditions in a primary health care setting from physiotherapists’ perspective using the Delphi method. Disabil. Rehabil. 2022, 13, 1–11. [Google Scholar] [CrossRef]
- Selb, M.; Escorpizo, R.; Kostanjsek, N.; Stucki, G.; Üstün, B.; Cieza, A. A guide on how to develop an International Classification of Functioning, Disability and Health Core Set. Eur. J. Phys. Rehabil. Med. 2015, 51, 105–117. [Google Scholar] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Cieza, A.; Fayed, N.; Bickenbach, J.; Prodinger, B. Refinements of the ICF Linking Rules to strengthen their potential for establishing comparability of health information. Disabil. Rehabil. 2019, 41, 574–583. [Google Scholar] [CrossRef]
- Abbott, J.; Wilson, R.; Pinto, D.; Chapple, C.M.; Wright, A.A. Incremental clinical effectiveness and cost effectiveness of providing supervised physiotherapy in addition to usual medical care in patients with osteoarthritis of the hip or knee: 2-year results of the MOA randomised controlled trial. Osteoarthr. Cartil. 2019, 27, 424–434. [Google Scholar] [CrossRef] [Green Version]
- Allen, K.D.; Oddone, E.Z.; Coffman, C.J.; Jeffreys, A.S.; Bosworth, H.B.; Chatterjee, R.; McDuffie, J.; Strauss, J.L.; Yancy, W.S., Jr.; Datta, S.K.; et al. Patient, Provider, and Combined Interventions for Managing Osteoarthritis in Primary Care: A Cluster Randomized Trial. Ann. Intern. Med. 2017, 166, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Amorim, A.B.; Pappas, E.; Simic, M.; Ferreira, M.L.; Jennings, M.; Tiedemann, A.; Carvalho-E-Silva, A.P.; Caputo, E.; Kongsted, A.; Ferreira, P.H. Integrating Mobile-health, health coaching, and physical activity to reduce the burden of chronic low back pain trial (IMPACT): A pilot randomised controlled trial. BMC Musculoskelet. Disord. 2019, 20, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arden, K.; Fatoye, F.; Yeowell, G. Evaluation of a rolling rehabilitation programme for patients with non-specific low back pain in primary care: An observational cohort study. J. Evaluation Clin. Pract. 2017, 23, 272–278. [Google Scholar] [CrossRef]
- Battista, S.; Dell’Isola, A.; Manoni, M.; Englund, M.; Palese, A.; Testa, M. Experience of the COVID-19 pandemic as lived by patients with hip and knee osteoarthritis: An Italian qualitative study. BMJ Open 2021, 11, e053194. [Google Scholar] [CrossRef] [PubMed]
- Bennell, K.L.; Kyriakides, M.; Hodges, P.W.; Hinman, R.S. Effects of Two Physiotherapy Booster Sessions on Outcomes With Home Exercise in People With Knee Osteoarthritis: A Randomized Controlled Trial. Arthritis Care Res. 2014, 66, 1680–1687. [Google Scholar] [CrossRef] [Green Version]
- Bennell, K.L.; Nelligan, R.; Dobson, F.; Rini, C.; Keefe, F.; Kasza, J.; French, S.; Bryant, C.; Dalwood, A.; Abbott, J.H.; et al. Effectiveness of an Internet-Delivered Exercise and Pain-Coping Skills Training Intervention for Persons With Chronic Knee Pain: A Randomized Trial. Ann. Intern. Med. 2017, 166, 453–462. [Google Scholar] [CrossRef]
- Bornhöft, L.; Larsson, M.E.; Nordeman, L.; Eggertsen, R.; Thorn, J. Health effects of direct triaging to physiotherapists in primary care for patients with musculoskeletal disorders: A pragmatic randomized controlled trial. Ther. Adv. Musculoskelet. Dis. 2019, 11, 1759720X19827504. [Google Scholar] [CrossRef] [PubMed]
- Burns, S.A.; Cleland, J.A.; Cook, C.E.; Bade, M.; Rivett, D.A.; Snodgrass, S. Variables Describing Individuals With Improved Pain and Function With a Primary Complaint of Low Back Pain: A Secondary Analysis. J. Manip. Physiol. Ther. 2018, 41, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Chesterton, L.S.; Lewis, A.M.; Sim, J.; Mallen, C.D.; Mason, E.E.; Hay, E.M.; van der Windt, D.A. Transcutaneous electrical nerve stimulation as adjunct to primary care management for tennis elbow: Pragmatic randomised controlled trial (TATE trial). BMJ 2013, 347, f5160. [Google Scholar] [CrossRef] [Green Version]
- Christiansen, D.H.; de Vos Andersen, N.-B.; Poulsen, P.H.; Ostelo, R.W. The smallest worthwhile effect of primary care physiotherapy did not differ across musculoskeletal pain sites. J. Clin. Epidemiol. 2018, 101, 44–52. [Google Scholar] [CrossRef]
- Costa, F.; Janela, D.; Molinos, M.; Lains, J.; Francisco, G.E.; Bento, V.; Correia, F.D. Telerehabilitation of acute musculoskeletal multi-disorders: Prospective, single-arm, interventional study. BMC Musculoskelet. Disord. 2022, 23, 29. [Google Scholar] [CrossRef]
- Crossley, K.; Vicenzino, B.; Lentzos, J.; Schache, A.; Pandy, M.; Ozturk, H.; Hinman, R. Exercise, education, manual-therapy and taping compared to education for patellofemoral osteoarthritis: A blinded, randomised clinical trial. Osteoarthr. Cartil. 2015, 23, 1457–1464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuesta-Vargas, A.I.; White, M.; González-Sánchez, M.; Kuisma, R. The optimal frequency of aquatic physiotherapy for individuals with chronic musculoskeletal pain: A randomised controlled trial. Disabil. Rehabil. 2015, 37, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Darlow, B.; Stanley, J.; Dean, S.; Abbott, J.H.; Garrett, S.; Wilson, R.; Mathieson, F.; Dowell, A. The Fear Reduction Exercised Early (FREE) approach to management of low back pain in general practice: A pragmatic cluster-randomised controlled trial. PLOS Med. 2019, 16, e1002897. [Google Scholar] [CrossRef] [Green Version]
- Emilson, C.; Demmelmaier, I.; Bergman, S.; Lindberg, P.; Denison, E.; Åsenlöf, P. A 10-year follow-up of tailored behavioural treatment and exercise-based physiotherapy for persistent musculoskeletal pain. Clin. Rehabil. 2017, 31, 186–196. [Google Scholar] [CrossRef] [Green Version]
- Ferrer-Peña, R.; Muñoz-García, D.; Lobo, C.C.; Fernandez-Carnero, J. Pain Expansion and Severity Reflect Central Sensitization in Primary Care Patients with Greater Trochanteric Pain Syndrome. Pain Med. 2019, 20, 961–970. [Google Scholar] [CrossRef]
- Gohir, S.A.; Eek, F.; Kelly, A.; Abhishek, A.; Valdes, A.M. Effectiveness of Internet-Based Exercises Aimed at Treating Knee Osteoarthritis: The iBEAT-OA Randomized Clinical Trial. JAMA Netw. Open 2021, 4, e210012. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, P.; Zeppieri, G.; Bialosky, J.; Bocchino, C.; Boogaard, J.V.D.; Tillman, S.; Chmielewski, T.L. Kinesiophobia and Its Association With Health-Related Quality of Life Across Injury Locations. Arch. Phys. Med. Rehabil. 2018, 99, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.C.; Garvin, S.; Chen, Y.; Cooper, V.; Wathall, S.; Saunders, B.; Lewis, M.; Protheroe, J.; Chudyk, A.; Dunn, K.M.; et al. Stratified primary care versus non-stratified care for musculoskeletal pain: Findings from the STarT MSK feasibility and pilot cluster randomized controlled trial. BMC Fam. Pract. 2020, 21, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hopewell, S.; Keene, D.J.; Heine, P.; Marian, I.R.; Dritsaki, M.; Cureton, L.; Dutton, S.J.; Dakin, H.; Carr, A.; Hamilton, W.; et al. Progressive exercise compared with best-practice advice, with or without corticosteroid injection, for rotator cuff disorders: The GRASP factorial RCT. Health Technol. Assess. 2021, 25, 1–158. [Google Scholar] [CrossRef] [PubMed]
- Laslett, M.; Steele, M.; Hing, W.; McNair, P.; Cadogan, A. Shoulder pain patients in primary care-part 1: Clinical outcomes over 12 months following standardized diagnostic workup, corticosteroid injections, and community-based care. J. Rehabil. Med. 2014, 46, 898–907. [Google Scholar] [CrossRef] [Green Version]
- Leaver, A.M.; Maher, C.G.; McAuley, J.H.; Jull, G.; Latimer, J.; Refshauge, K.M. People seeking treatment for a new episode of neck pain typically have rapid improvement in symptoms: An observational study. J. Physiother. 2013, 59, 31–37. [Google Scholar] [CrossRef] [Green Version]
- Leemans, L.; Elma, Ö.; Nijs, J.; Wideman, T.H.; Siffain, C.; Bandt, H.D.; Van Laere, S.; Beckwée, D. Transcutaneous electrical nerve stimulation and heat to reduce pain in a chronic low back pain population: A randomized controlled clinical trial. Braz. J. Phys. Ther. 2021, 25, 86–96. [Google Scholar] [CrossRef]
- Legha, A.; Burke, D.L.; Foster, N.E.; Windt, D.A.; Quicke, J.G.; Healey, E.L.; Runhaar, J.; Holden, M.A. Do comorbidities predict pain and function in knee osteoarthritis following an exercise intervention, and do they moderate the effect of exercise? Analyses of data from three randomized controlled trials. Musculoskelet. Care 2020, 18, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Lentz, T.A.; Beneciuk, J.M.; George, S.Z. Prediction of healthcare utilization following an episode of physical therapy for musculoskeletal pain. BMC Health Serv. Res. 2018, 18, 648. [Google Scholar] [CrossRef]
- Lewis, J.; Sim, J.; Barlas, P. Acupuncture and electro-acupuncture for people diagnosed with subacromial pain syndrome: A multicentre randomized trial. Eur. J. Pain 2017, 21, 1007–1019. [Google Scholar] [CrossRef]
- Lingner, H.; Blase, L.; Großhennig, A.; Schmiemann, G. Manual therapy applied by general practitioners for nonspecific low back pain: Results of the ManRück pilot-study. Chiropr. Man. Ther. 2018, 26, 39. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Lopez, A.; Perez, J.L.A.; Gutierez, J.L.G.; La Touche, R.; Lara, S.L.; Izquierdo, H.; Fernandez-Carnero, J. Mobilization versus manipulations versus sustain apophyseal natural glide techniques and interaction with psychological factors for patients with chronic neck pain: Randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2015, 51, 121–132. [Google Scholar] [PubMed]
- Marra, C.A.; Cibere, J.; Grubisic, M.; Grindrod, K.A.; Gastonguay, L.; Thomas, J.M.; Embley, P.; Colley, L.; Tsuyuki, R.T.; Khan, K.M.; et al. Pharmacist-initiated intervention trial in osteoarthritis: A multidisciplinary intervention for knee osteoarthritis. Arthritis Care Res. 2012, 64, 1837–1845. [Google Scholar] [CrossRef] [PubMed]
- Matarán-Peñarrocha, G.A.; Palomo, I.C.L.; Soler, E.A.; Gil-Martínez, E.; Fernández-Sánchez, M.; Aguilar-Ferrándiz, M.E.; Castro-Sánchez, A.M. Comparison of efficacy of a supervised versus non-supervised physical therapy exercise program on the pain, functionality and quality of life of patients with non-specific chronic low-back pain: A randomized controlled trial. Clin. Rehabil. 2020, 34, 948–959. [Google Scholar] [CrossRef] [PubMed]
- Miedema, H.S.; Feleus, A.; Bierma-Zeinstra, S.M.; Hoekstra, T.; Burdorf, A.; Koes, B.W. Disability Trajectories in Patients With Complaints of Arm, Neck, and Shoulder (CANS) in Primary Care: Prospective Cohort Study. Phys. Ther. 2016, 96, 972–984. [Google Scholar] [CrossRef] [Green Version]
- Minns Lowe, C.J.; Kelly, P.; Milton, K.; Foster, C.; Barker, K. “WALK30X5”: A feasibility study of a physiotherapy walking programme for people with mild to moderate musculoskeletal conditions. Physiotherapy 2020, 107, 275–285. [Google Scholar] [CrossRef]
- Molgaard Nielsen, A.; Hestbaek, L.; Vach, W.; Kent, P.; Kongsted, A. Latent class analysis derived subgroups of low back pain patients-do they have prognostic capacity? BMC Musculoskelet. Disord. 2017, 18, 345. [Google Scholar] [CrossRef] [Green Version]
- Moseng, T.; Dagfinrud, H.; van Bodegom-Vos, L.; Dziedzic, K.; Hagen, K.B.; Natvig, B.; Røtterud, J.H.; Vlieland, T.V.; Østerås, N. Low adherence to exercise may have influenced the proportion of OMERACT-OARSI responders in an integrated osteoarthritis care model: Secondary analyses from a cluster-randomised stepped-wedge trial. BMC Musculoskelet. Disord. 2020, 21, 236. [Google Scholar] [CrossRef] [Green Version]
- Murphy, S.; Blake, C.; Power, C.K.; Fullen, B.M. The role of clinical specialist Physiotherapists in the management of low back pain in a Spinal Triage Clinic. Ir. J. Med. Sci. 2013, 182, 643–650. [Google Scholar] [CrossRef] [PubMed]
- Noblet, T.; Marriott, J.; Hensman-Crook, A.; O’Shea, S.; Friel, S.; Rushton, A. Independent prescribing by advanced physiotherapists for patients with low back pain in primary care: A feasibility trial with an embedded qualitative component. PLoS ONE 2020, 15, e0229792. [Google Scholar] [CrossRef]
- Østerås, N.; Hagen, K.B.; Grotle, M.; Sand-Svartrud, A.L.; Mowinckel, P.; Kjeken, I. Limited effects of exercises in people with hand osteoarthritis: Results from a randomized controlled trial. Osteoarthr. Cartilage. 2014, 22, 1224–1233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Østerås, N.; Moseng, T.; van Bodegom-Vos, L.; Dziedzic, K.; Mdala, I.; Natvig, B.; Røtterud, J.H.; Schjervheim, U.B.; Vlieland, T.V.; Andreassen, Ø.; et al. Implementing a structured model for osteoarthritis care in primary healthcare: A stepped-wedge cluster-randomised trial. PLoS Med. 2019, 16, e1002949. [Google Scholar]
- Paanalahti, K.; Holm, L.W.; Nordin, M.; Höijer, J.; Lyander, J.; Asker, M.; Skillgate, E. Three combinations of manual therapy techniques within naprapathy in the treatment of neck and/or back pain: A randomized controlled trial. BMC Musculoskelet. Disord. 2016, 17, 176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palacín-Marín, F.; Esteban-Moreno, B.; Olea, N.; Herrera-Viedma, E.; Arroyo-Morales, M. Agreement between telerehabilitation and face-to-face clinical outcome assessments for low back pain in primary care. Spine 2013, 38, 947–952. [Google Scholar] [CrossRef]
- Sandal, L.F.; Bach, K.; Øverås, C.K.; Svendsen, M.J.; Dalager, T.; Stejnicher Drongstrup Jensen, J.; Kongsvold, A.; Nordstoga, A.L.; Bardal, E.M.; Ashikhmin, I.; et al. Effectiveness of App-Delivered, Tailored Self-management Support for Adults With Lower Back Pain-Related Disability: A selfBACK Randomized Clinical Trial. JAMA Intern. Med. 2021, 181, 1288–1296. [Google Scholar] [CrossRef]
- Schröder, K.; Öberg, B.; Enthoven, P.; Hedevik, H.; Fors, M.; Abbott, A. Effectiveness and Quality of Implementing a Best Practice Model of Care for Low Back Pain (BetterBack) Compared with Routine Care in Physiotherapy: A Hybrid Type 2 Trial. J. Clin. Med. 2021, 10, 1230. [Google Scholar] [CrossRef]
- Schütze, R.; Slater, H.; O’Sullivan, P.; Thornton, J.; Finlay-Jones, A.; Rees, C.S. Mindfulness-Based Functional Therapy: A preliminary open trial of an integrated model of care for people with persistent low back pain. Front. Psychol. 2014, 5, 839. [Google Scholar]
- Trulsson Schouenborg, A.; Rivano Fischer, M.; Bondesson, E.; Jöud, A. Physiotherapist-led rehabilitation for patients with chronic musculoskeletal pain: Interventions and promising long-term outcomes. BMC Musculoskelet. Disord. 2021, 22, 910. [Google Scholar] [CrossRef]
- Uhl, T.L.; Smith-Forbes, E.; Nitz, A.J. Factors influencing final outcomes in patients with shoulder pain: A retrospective review. J. Hand Ther. 2017, 30, 200–207. [Google Scholar] [CrossRef] [Green Version]
- Van der Maas, L.C.; Köke, A.; Pont, M.; Bosscher, R.J.; Twisk, J.W.; Janssen, T.W.; Peters, M.L. Improving the Multidisciplinary Treatment of Chronic Pain by Stimulating Body Awareness: A Cluster-randomized Trial. Clin. J. Pain 2015, 31, 660–669. [Google Scholar] [CrossRef] [Green Version]
- Vibe Fersum, K.; O’Sullivan, P.; Skouen, J.S.; Smith, A.; Kvåle, A. Efficacy of classification-based cognitive functional therapy in patients with non-specific chronic low back pain: A randomized controlled trial. Eur. J. Pain 2013, 17, 916–928. [Google Scholar] [CrossRef] [PubMed]
- Vibe Fersum, K.; Smith, A.; Kvåle, A.; Skouen, J.S.; O’Sullivan, P. Cognitive functional therapy in patients with non-specific chronic low back pain-a randomized controlled trial 3-year follow-up. Eur. J. Pain 2019, 23, 1416–1424. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.; Rushton, A.; Lewis, J.; Phillips, C. Evaluation of the clinical effectiveness of a work-based mentoring programme to develop clinical reasoning on patient outcome: A stepped wedge cluster randomised controlled trial. PLoS ONE 2019, 14, e0220110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xia, T.; Long, C.R.; Gudavalli, M.R.; Wilder, D.G.; Vining, R.D.; Rowell, R.M.; Reed, W.R.; DeVocht, J.W.; Goertz, C.M.; Owens, E.F., Jr.; et al. Similar Effects of Thrust and Nonthrust Spinal Manipulation Found in Adults With Subacute and Chronic Low Back Pain: A Controlled Trial With Adaptive Allocation. Spine 2016, 41, E702–E709. [Google Scholar] [CrossRef] [Green Version]
- Nijs, J.; Lahousse, A.; Kapreli, E.; Bilika, P.; Saraçoğlu, İ.; Malfliet, A.; Coppieters, I.; De Baets, L.; Leysen, L.; Roose, E.; et al. Nociplastic Pain Criteria or Recognition of Central Sensitization? Pain Phenotyping in the Past, Present and Future. J. Clin. Med. 2021, 10, 3203. [Google Scholar] [CrossRef]
- International Association for the Study of Pain (IASP) [Internet]. IASP Announces Revised Definition of Pain; IASP: Washington, DC, USA, 2020; Available online: https://www.iasp-pain.org/publications/iasp-news/iasp-announces-revised-definition-of-pain (accessed on 3 December 2022).
- Dworkin, R.H.; Turk, D.C.; Farrar, J.T.; Haythornthwaite, J.A.; Jensen, M.P.; Katz, N.P.; Kerns, R.D.; Stucki, G.; Allen, R.R.; Bellamy, N.; et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain 2005, 113, 9–19. [Google Scholar] [CrossRef]
- Cohen, S.P.; Vase, L.; Hooten, W.M. Chronic pain: An update on burden, best practices, and new advances. Lancet 2021, 397, 2082–2097. [Google Scholar] [CrossRef]
- Mills, S.E.; Nicolson, K.P.; Smith, B.H. Chronic pain: A review of its epidemiology and associated factors in population-based studies. Br. J. Anaesth. 2019, 123, e273–e283. [Google Scholar] [CrossRef]
- van Dijk, M.J.; Smorenburg, N.T.; Visser, B.; Nijhuis-van der Sanden, M.W.; Heerkens, Y.F. Description of movement quality in patients with low back pain: A qualitative study as a first step to a practical definition. Physiother. Theory Pract. 2017, 33, 227–237. [Google Scholar] [CrossRef]
- Ludewig, P.M.; Lawrence, R.L.; Braman, J.P. What’s in a name? Using movement system diagnoses versus pathoanatomic diagnoses. J. Orthop. Sports Phys. Ther. 2013, 43, 280–283. [Google Scholar] [CrossRef] [Green Version]
- Jull, G.; Moore, A. Physiotherapy’s identity. Man. Ther. 2013, 18, 447–448. [Google Scholar] [CrossRef] [PubMed]
- E Finger, M.; Cieza, A.; Stoll, J.; Stucki, G.; O Huber, E. Identification of Intervention Categories for Physical Therapy, Based on the International Classification of Functioning, Disability and Health: A Delphi Exercise. Phys. Ther. 2006, 86, 1203–1220. [Google Scholar] [CrossRef] [PubMed]
- Vlaeyen, J.W.S.; Linton, S.J. Fear-avoidance and its consequences in chronic musculoskeletal pain: A state of the art. Pain 2000, 85, 317–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lundberg, M.; Larsson, M.; Östlund, H.; Styf, J. Kinesiophobia among patients with musculoskeletal pain in primary healthcare. J. Rehabil. Med. 2006, 38, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Calderon, J.; Jensen, M.P.; Morales-Asencio, J.M.; Luque-Suarez, A. Pain Catastrophizing and Function In Individuals With Chronic Musculoskeletal Pain: A Systematic Review and Meta-Analysis. Clin. J. Pain 2019, 35, 279–293. [Google Scholar] [CrossRef]
- Macías-Toronjo, I.; Rojas-Ocaña, M.J.; Sánchez-Ramos, J.L.; García-Navarro, E.B. Pain catastrophizing, kinesiophobia and fear-avoidance in non-specific work-related low-back pain as predictors of sickness absence. PLoS ONE 2020, 15, e0242994. [Google Scholar] [CrossRef]
- Chiarotto, A.; Ostelo, R.W.; Boers, M.; Terwee, C.B. A systematic review highlights the need to investigate the content validity of patient-reported outcome measures for physical functioning in patients with low back pain. J. Clin. Epidemiol. 2018, 95, 73–93. [Google Scholar] [CrossRef]
- Perera, S.; Patel, K.V.; Rosano, C.; Rubin, S.M.; Satterfield, S.; Harris, T.; Ensrud, K.; Orwoll, E.; Lee, C.G.; Chandler, J.M.; et al. Gait Speed Predicts Incident Disability: A Pooled Analysis. J. Gerontol. Ser. A 2016, 71, 63–71. [Google Scholar] [CrossRef]
- Dumurgier, J.; Artaud, F.; Touraine, C.; Rouaud, O.; Tavernier, B.; Dufouil, C.; Singh-Manoux, A.; Tzourio, C.; Elbaz, A. Gait Speed and Decline in Gait Speed as Predictors of Incident Dementia. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2017, 72, 655–661. [Google Scholar] [CrossRef] [Green Version]
- Day, A.M.B.; Theurer, J.A.; Dykstra, A.D.; Doyle, P.C. Nature and the natural environment as health facilitators: The need to reconceptualize the ICF environmental factors. Disabil. Rehabil. 2012, 34, 2281–2290. [Google Scholar] [CrossRef]
- Geyh, S.; Schwegler, U.; Peter, C.; Müller, R. Representing and organizing information to describe the lived experience of health from a personal factors perspective in the light of the International Classification of Functioning, Disability and Health (ICF): A discussion paper. Disabil. Rehabil. 2019, 41, 1727–1738. [Google Scholar] [CrossRef] [PubMed]
- Chiarotto, A.; Terwee, C.B.; Kamper, S.J.; Boers, M.; Ostelo, R.W. Evidence on the measurement properties of health-related quality of life instruments is largely missing in patients with low back pain: A systematic review. J. Clin. Epidemiol. 2018, 102, 23–37. [Google Scholar] [CrossRef] [PubMed]
- Terwee, C.B.; Prinsen, C.A.C.; Chiarotto, A.; Westerman, M.J.; Patrick, D.L.; Alonso, J.; Bouter, L.M.; de Vet, H.C.W.; Mokkink, L.B. COSMIN methodology for evaluating the content validity of patient-reported outcome measures: A Delphi study. Qual. Life Res. 2018, 27, 1159–1170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleinlugtenbelt, Y.V.; Krol, R.G.; Bhandari, M.; Goslings, J.C.; Poolman, R.W.; Scholtes, V.A.B. Are the patient-rated wrist evaluation (PRWE) and the disabilities of the arm, shoulder and hand (DASH) questionnaire used in distal radial fractures truly valid and reliable? Bone Joint Res. 2018, 7, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Schwarzkopf, S.R.; Ewert, T.; Dreinhöfer, K.E.; Cieza, A.; Stucki, G. Towards an ICF Core Set for chronic musculoskeletal conditions: Commonalities across ICF Core Sets for osteoarthritis, rheumatoid arthritis, osteoporosis, low back pain and chronic widespread pain. Clin. Rheumatol. 2008, 27, 1355–1361. [Google Scholar] [CrossRef] [PubMed]
- Tomandl, J.; Heinmüller, S.; Selb, M.; Graessel, E.; Freiberger, E.; Kühlein, T.; Hueber, S.; Book, S.; Gotthardt, S. Laying the foundation for a Core Set of the International Classification of Functioning, Disability and Health for community-dwelling older adults in primary care: Relevant categories of their functioning from the research perspective, a scoping review. BMJ Open 2021, 11, e037333. [Google Scholar] [CrossRef]
- De Araújo Filho, J.C.; Cavalcanti, F.C.B.; Morais, G.S.; Bezerra, S.D.; Costa, M.J.C.; Marinho, P.É.M. Development of an International Classification of Functioning, Disability and Health core set for adults with chronic kidney disease undergoing hemodialysis: A scoping review protocol. JBI Evid. Synth. 2020, 18, 1116–1123. [Google Scholar]

| Assessment Instrument | Main Theme | Type | No of Studies |
|---|---|---|---|
| 11-points numeric pain rating scale (NPRS) | Pain description | Single-item | 27 |
| 0–100 mm. Visual analog scale (VAS) | Pain description | Single-item | 11 |
| Question about pain | Pain description | Single-item | 7 |
| Örebro Musculoskeletal Pain Screening questionnaire (OMPQ) | Pain description | Multi-item | 4 |
| Pressure pain detection threshold (PPT) | Pain description | Single-item | 4 |
| Roland Morris Disability questionnaire (RMDQ) | Disability | Multi-item | 11 |
| Question about disability | Disability | Single-item | 10 |
| Oswestry Disability Index (ODI) | Disability | Multi-item | 8 |
| Western Ontario and McMaster Universities Arthritis Index (WOMAC) | Disability | Multi-item | 8 |
| Neck disability index (NDI) | Disability | Multi-item | 5 |
| Disabilities of the arm, shoulder, and hand (DASH) | Disability | Multi-item | 4 |
| Shoulder pain and disability index (SPADI) | Disability | Multi-item | 4 |
| Work absence reported | Disability | Single-item | 4 |
| Fear avoidance beliefs questionnaire (FABQ). | Psychosocial factors | Multi-item | 8 |
| Tampa Scale for Kinesiophobia (TSK) | Psychosocial factors | Multi-item | 7 |
| Pain catastrophizing scale (PCS) | Psychosocial factors | Multi-item | 4 |
| Question about psychosocial factors | Psychosocial factors | Single-item | 4 |
| EuroQoL 5 dimensions (EQ5D) | Quality of life related to health | Multi-item | 11 |
| Short form health survey 36 questionnaire (SF-36) | Quality of life related to health | Multi-item | 5 |
| Short form health survey 12 questionnaire (SF-12) | Quality of life related to health | Multi-item | 4 |
| Global rating of change (GROC) | Global perception of change | Single-item | 9 |
| Perceived recovery | Global perception of change | Single-item | 7 |
| Range of movement measure (ROM) | Physical measure | Single-item | 7 |
| Physical activity level measure | Physical performance | Single-item | 7 |
| Variation in the use of analgesics or other therapies | Other (indirect measure of recovery) | Single-item | 10 |
| Patient Satisfaction questionnaire | Other (patient satisfaction) | Multi-item | 6 |
| Adherence to treatment | Other (personal factor) | Single-item | 5 |
| Adverse events reported | Other (adverse events) | Single-item | 4 |
| ICF Category * | Count | Outcome Measures |
|---|---|---|
| b134 Sleep functions | 58 | PSQI, SQM (actigraphy) |
| b260 Proprioceptive function | 4 | Physical performance measures (e.g., SPPB) |
| b280 Sensation of pain | 207 | NPRS, VAS, OMPQ, PPDT, TS, CPM, BC, CSI, CPAQ, FABQ, GCPS, PCS, TSK |
| b435 Immunological system functions | 0 | - |
| b530 Weight maintenance functions | 11 | IPQ, DRAM, PHQ |
| b620 Urination functions | 4 | DRAM, CSI |
| b730 Muscle power functions | 104 | Physical measure (e.g., dynamometer) |
| b740 Muscle endurance functions | 99 | Physical measure (e.g., McQuade test) |
| b755 Involuntary movement reaction functions | 93 | Region-specific functional scales (e.g., BPS) or physical performance measures (e.g., TUG) |
| b780 Sensations related to muscles and movement functions | 29 | HSC, MHQ, OSPRO-YF, IPQ, CSI, region-specific functional scales (e.g., DASH) |
| d155 Acquiring skills | 0 | - |
| d177 Making decisions | 5 | DRAM, BDI |
| d230 Carrying out daily routine | 23 | Quality of life scale (e.g., SF-36), pain-related questionnaires (e.g., CPAQ or PEI), CSQ, DRAM, MHQ |
| d240 Handling stress and other psychological demands | 41 | AQLI, BDI, CSQ, DASS, GAD, OSPRO-YF, PCS, PAM, PHQ, SF-36, STAI |
| d410 Changing basic body position | 46 | LEFS, region-specific functional scale (e.g., HOOS) |
| d415 Maintaining a body position | 64 | DRI, region-specific functional scales |
| d430 Lifting and carrying objects | 43 | DAQ, DRI, PAT5, region-specific functional scales (e.g., ODI or SPADI), |
| d445 Hand and arm use | 16 | DASH, FIHOA, OSS, PRTEE, SPADI |
| d450 Walking | 90 | TUG, LEFS, ASES, DRI, DAQ, quality of life scales (e.g., EQL5), region-specific functional scale (e.g., KOOS) |
| d465 Moving around using equipment | 29 | DAQ, IPAQ, SGPAL |
| d510 Washing oneself | 70 | SF-36, AQLI, DRI, EQL5, MHQ, PDI, region-specific functional scale (e.g., DASH) |
| d520 Caring for body parts | 12 | AQLI, region-specific functional scale (e.g., DASH) |
| d530 Toileting | 19 | AQLI, PAT5, region-specific functional scale (e.g., WOMAC) |
| d540 Dressing | 83 | ASES, AQLI, DRI, EQL5, MHQ, PDI, PAT5, region-specific functional scale (e.g., PRTEE) |
| d550 Eating | 18 | AQLI, DRAM, PDI, PAT5, region-specific functional scale (e.g., DASH) |
| e110 Products or substances for personal consumption | 36 | BBQ, OSPRO-ROS, OCCQ, PAM |
| e115 Products and technology for personal use in daily living | 24 | ASES, HUI3 |
| e120 Products and technology for personal indoor and outdoor mobility and transportation | 37 | BBQ, HUI3, OA-QI |
| e225 Climate | 0 | - |
| e355 Health professionals | 73 | AdEv, ARM, BBQ, CSQ, ECRQ, MRI, OA-QI |
| e450 Individual attitudes of health professionals | 63 | CSQ, ECRQ, MRI, OA-QI, PSEQ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández-Lázaro, H.; Mingo-Gómez, M.T.; Jiménez-del-Barrio, S.; Lahuerta-Martín, S.; Hernando-Garijo, I.; Medrano-de-la-Fuente, R.; Ceballos-Laita, L. Researcher’s Perspective on Musculoskeletal Conditions in Primary Care Physiotherapy Units through the International Classification of Functioning, Disability, and Health (ICF): A Scoping Review. Biomedicines 2023, 11, 290. https://doi.org/10.3390/biomedicines11020290
Hernández-Lázaro H, Mingo-Gómez MT, Jiménez-del-Barrio S, Lahuerta-Martín S, Hernando-Garijo I, Medrano-de-la-Fuente R, Ceballos-Laita L. Researcher’s Perspective on Musculoskeletal Conditions in Primary Care Physiotherapy Units through the International Classification of Functioning, Disability, and Health (ICF): A Scoping Review. Biomedicines. 2023; 11(2):290. https://doi.org/10.3390/biomedicines11020290
Chicago/Turabian StyleHernández-Lázaro, Héctor, María Teresa Mingo-Gómez, Sandra Jiménez-del-Barrio, Silvia Lahuerta-Martín, Ignacio Hernando-Garijo, Ricardo Medrano-de-la-Fuente, and Luis Ceballos-Laita. 2023. "Researcher’s Perspective on Musculoskeletal Conditions in Primary Care Physiotherapy Units through the International Classification of Functioning, Disability, and Health (ICF): A Scoping Review" Biomedicines 11, no. 2: 290. https://doi.org/10.3390/biomedicines11020290