




Skeletal and Dentoalveolar Changes in Growing Patients Treated with Rapid Maxillary Expansion Measured in 3D Cone-Beam Computed Tomography
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Committee and Informed Consent
2.2. Sample Size and Participants
2.3. Study Design
2.4. Procedure
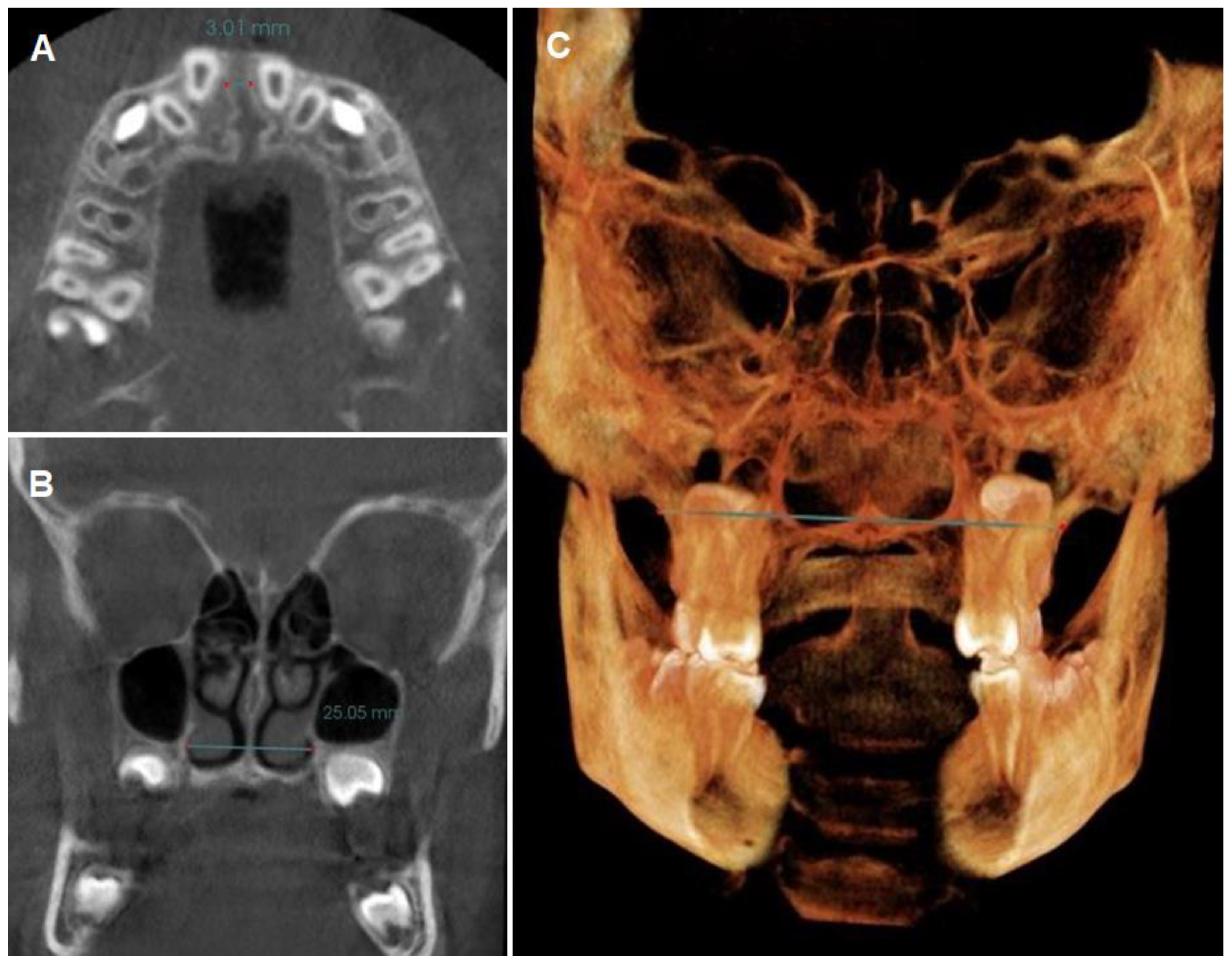
- Coronal perimeter (CP): the distance between the mesial of the right upper first molar and the mesial of the left upper first molar, passing through the vestibular side of all the teeth of the arch (Figure 2A).
- Angulation of the upper first molar (MA): the angle formed between a straight line drawn parallel to the hard palate plane (in sagittal view, utilizing the anterior nasal spine (ANS) and posterior nasal spine (PNS) as reference points) and a line passing through the center of the pulp chamber of both upper right and left first molars [12,55] (Figure 2C).
- Intermolar width (IMW): the distance between the central fossa of the upper right and left first molars was measured (Figure 2C).
2.5. Statistical Analysis
3. Results
3.1. Differences between Measurements before RME (T1) and after RME (T2)
3.2. Correlation between Variables
4. Discussion
- -
- DENTOALVEOLAR CHANGES:
- -
- SKELETAL CHANGES:
- -
- LIMITATIONS OF THIS STUDY:
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brunelle, J.A.; Bhat, M.; Lipton, J.A. Prevalence and distribution of selected occlusal characteristics in the US population, 1988–1991. J. Dent. Res. 1996, 75, 706–713. [Google Scholar] [CrossRef] [PubMed]
- Ciuffolo, F.; Manzoli, L.; D’Attilio, M.; Tecco, S.; Muratore, F.; Festa, F.; Romano, F. Prevalence and distribution by gender of occlusal characteristics in a sample of Italian secondary school students: A cross-sectional study. Eur. J. Orthod 2005, 27, 601–606. [Google Scholar] [CrossRef]
- Gabris, K.; Marton, S.; Madlena, M. Prevalence of malocclusions in Hungarian adolescents. Eur. J. Orthod. 2006, 28, 467–470. [Google Scholar] [CrossRef] [PubMed]
- Da Silva Filho, O.G.; Santamaria, M., Jr.; Capelozza Filho, L. Epidemiology of posterior crossbite in the primary dentition. J. Clin. Pediatr. Dent. 2007, 32, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Lowe, A.A. The tongue and airway. Otolaryngol. Clin. North Am. 1990, 23, 677–698. [Google Scholar] [CrossRef] [PubMed]
- Pae, E.K.; Lowe, A.A.; Sasaki, K.; Price, C.; Tsuchiya, M. A cephalometric and electromyographic study of upper airway structures in the upright and supine positions. Am. J. Orthod. Dentofac. Orthop. 1994, 106, 52–59. [Google Scholar] [CrossRef]
- Subtelny, J.D. Oral respiration: Facial maldevelopment and corrective dentofacial orthopedics. Angle Orthod. 1980, 50, 147–164. [Google Scholar]
- Adkins, M.D.; Nanda, R.S.; Currier, G.F. Arch perimeter changes on rapid palatal expansion. Am. J. Orthod. Dentofac. Orthop. 1990, 97, 194–199. [Google Scholar] [CrossRef]
- D’Souza, I.M.; Kumar, H.C.; Shetty, K.S. Dental arch changes associated with rapid maxillary expansion: A retrospective model analysis study. Contemp Clin Dent. 2015, 6, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Khosravi, M.; Ugolini, A.; Miresmaeili, A.; Mirzaei, H.; Shahidi-Zandi, V.; Soheilifar, S.; Karami, M.; Mahmoudzadeh, M. Tooth-borne versus bone-borne rapid maxillary expansion for transverse maxillary deficiency: A systematic review. Int. Orthod. 2019, 17, 425–436. [Google Scholar] [CrossRef]
- An, J.S.; Seo, B.Y.; Ahn, S.J. Comparison of dentoskeletal and soft tissue changes between tooth-borne and tooth-bone-borne hybrid nonsurgical rapid maxillary expansions in adults: A retrospective observational study. BMC Oral Health. 2021, 21, 658. [Google Scholar] [CrossRef] [PubMed]
- Bazargani, F.; Lund, H.; Magnuson, A.; Ludwig, B. Skeletal and dentoalveolar effects using tooth-borne and tooth-bone-borne RME appliances: A randomized controlled trial with 1-year follow-up. Eur. J. Orthod. 2021, 43, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Lagravère, M.O.; Ling, C.P.; Woo, J.; Harzer, W.; Major, P.W.; Carey, J.P. Transverse, vertical, and anterior-posterior changes between tooth-anchored versus Dresden bone-anchored rapid maxillary expansion 6 months post-expansion: A CBCT randomized controlled clinical trial. Int. Orthod. 2020, 18, 308–316. [Google Scholar] [CrossRef]
- Moon, H.W.; Kim, M.J.; Ahn, H.W.; Kim, S.J.; Kim, S.H.; Chung, K.R.; Nelson, G. Molar inclination and surrounding alveolar bone change relative to the design of bone-borne maxillary expanders: A CBCT study. Angle Orthod. 2020, 90, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Solano, P.; Aceytuno, P.; Solano, E.; Solano, B. Skeletal, dentoalveolar and dental changes after “mini-screw assisted rapid palatal expansion” evaluated with cone beam computed tomography. J. Clin. Med. 2022, 11, 4652. [Google Scholar]
- Sayar, G.; Kılınç, D.D. Rapid maxillary expansion outcomes according to midpalatal suture maturation levels. Prog. Orthod. 2019, 20, 27. [Google Scholar] [CrossRef] [PubMed]
- Fishman, L.S. Radiographic evaluation of skeletal maturation. A clinically oriented study based on hand-wrist films. Angle Orthod. 1982, 52, 88–112. [Google Scholar]
- Baccetti, T.; Franchi, L.; McNamara, J.A., Jr. The cervical vertebral maturation (CVM) method for the assessment of optimal treatment timing in dentofacial orthopedics. Semin. Orthod. 2005, 11, 119–129. [Google Scholar] [CrossRef]
- Korbmacher, H.; Schilling, A.; Püschel, K.; Amling, M.; Kahl-Nieke, B. Age-dependent three-dimensional microcomputed tomography analysis of the human midpalatal suture. J. Orofac. Orthop. 2007, 68, 364–376. [Google Scholar] [CrossRef] [PubMed]
- Angelieri, F.; Cevidanes, L.H.; Franchi, L.; Gonçalves, J.R.; Benavides, E.; McNamara, J.A., Jr. Midpalatal suture maturation: Classification method for individual assessment before rapid maxillary expansion. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 759–769. [Google Scholar] [CrossRef]
- Flores–Mir, C.; Nebbe, B.; Major, P.W. Use of skeletal maturation based on hand-wrist radiographic analysis as a predictor of facial growth: A systematic review. Angle Orthod. 2004, 74, 118–124. [Google Scholar] [PubMed]
- Haas, A.J. Rapid expansion of the maxillary dental arch and nasal cavity by opening the midpalatal suture. Angle Orthod. 1961, 31, 73–90. [Google Scholar]
- Wertz, R.A. Changes in nasal airflow incident to rapid maxillary expansion. Angle Orthod. 1968, 38, 1–11. [Google Scholar]
- Warren, D.W.; Turvey, T.A.; Hairfield, W.M. The nasal airway following maxillary expansion. Am. J. Orthod. Dentofac. Orthop. 1987, 91, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Cross, D.L.; McDonald, J.P. Effect of rapid maxillary expansion on skeletal, dental, and nasal structures a postero-anterior cephalometric study. Eur. J. Orthod. 2000, 22, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Melo, M.F.; Melo, S.L.; Zanet, T.G.; Fenyo-Pereira, M. Digital radiographic evaluation of the midpalatal suture in patients submitted to rapid maxillary expansion. Indian J. Dent. Res. 2013, 24, 76–80. [Google Scholar] [CrossRef]
- Haralambidis, A.; Ari-Demirkaya, A.; Acar, A.; Küçükkeleş, N.; Ateş, M.; Ozkaya, S. Morphologic changes of the nasal cavity induced by rapid maxillary expansion: A study on 3-dimensional computed tomography models. Am. J. Orthod. Dentofac. Orthop. 2009, 136, 815–821. [Google Scholar] [CrossRef]
- Christie, K.F.; Boucher, N.; Chung, C.H. Effects of bonded rapid palatal expansion on the transverse dimensions of the maxilla a cone-beam computed tomography study. Am. J. Orthod. Dentofac. Orthop. 2010, 137, S79–S85. [Google Scholar] [CrossRef]
- Caprioglio, A.; Meneghel, M.; Fastuca, R.; Zecca, P.A.; Nucera, R.; Nosetti, L. Rapid maxillary expansion in growing patients correspondence between 3-dimensional airway changes and polysomnography. Int. J. Pediatr. Otorhinolaryngol. 2014, 78, 23–27. [Google Scholar] [CrossRef]
- El, H.; Palomo, J.M. Three-dimensional evaluation of upper airway following rapid maxillary expansion a CBCT study. Angle Orthod. 2014, 84, 265–273. [Google Scholar] [CrossRef]
- Woller, J.L.; Kim, K.B.; Behrents, R.G.; Buschang, P.H. An assessment of the maxilla after rapid maxillary expansion using cone beam computed tomography in growing children. Dental Press J. Orthod. 2014, 19, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Ahn, H.W.; Kim, S.J.; Moon, S.C.; Kim, S.H.; Nelson, G. Tooth-borne vs bone-borne rapid maxillary expanders in late adolescence. Angle Orthod. 2015, 85, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Serafin, M.; Fastuca, R.; Caprioglio, A. CBCT analysis of dento-skeletal changes after rapid versus slow maxillary expansion on deciduous teeth: A randomized clinical trial. J. Clin. Med. 2022, 11, 4887. [Google Scholar] [CrossRef] [PubMed]
- Baysal, A.; Uysal, T.; Veli, I.; Ozer, T.; Karadede, I.; Hekimoglu, S. Evaluation of alveolar bone loss following rapid maxillary expansion using cone-beam computed tomography. Korean J. Orthod. 2013, 43, 83–95. [Google Scholar] [CrossRef] [PubMed]
- Bahammam, M.; El-Bialy, T. Comparison of alveolar bone thickness and height after slow expansion using quad-helix or clear aligners. Saudi Dent. J. 2023, 35, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Palaisa, J.; Ngan, P.; Martin, C.; Razmus, T. Use of conventional tomography to evaluate changes in the nasal cavity with rapid palatal expansion. Am. J. Orthod. Dentofac. Orthop. 2007, 132, 458–466. [Google Scholar] [CrossRef]
- Felippe, N.L.O.; Silveira, A.C.; Viana, G.; Kusnoto, B.; Smith, B.; Evans, C.A. Relationship between rapid maxillary expansion and nasal cavity size and airway resistance short- and long-term effects. Am. J. Orthod. Dentofacial Orthop. 2008, 134, 370–382. [Google Scholar] [CrossRef]
- Garrett, B.J.; Caruso, J.M.; Rungcharassaeng, K.; Farrage, J.R.; Kim, J.S.; Taylor, G.D. Skeletal effects to the maxilla after rapid maxillary expansion assessed with cone-beam computed tomography. Am. J. Orthod. Dentofac. Orthop. 2008, 134, 8.e1–8.e11. [Google Scholar] [CrossRef]
- Lione, R.; Ballanti, F.; Franchi, L.; Cozza, P. Treatment and posttreatment skeletal effects of rapid maxillary expansion studied with low-dose computed tomography in growing subjects. Am. J. Orthod. Dentofac. Orthop. 2008, 134, 389–392. [Google Scholar] [CrossRef]
- Zhao, Y.; Nguyen, M.; Gohl, E.; Mah, J.K.; Sameshima, G.; Enciso, R. Oropharyngeal airway changes after rapid palatal expansion evaluated with cone-beam computed tomography. Am. J. Orthod. Dentofac. Orthop. 2010, 137, S71–S78. [Google Scholar] [CrossRef] [PubMed]
- Pangrazio-Kulbersh, V.; Wine, P.; Haughey, M.; Pajtas, B.; Kaczynski, R. Cone beam computed tomography evaluation of changes in the naso-maxillary complex associated with two types of maxillary expanders. Angle Orthod. 2012, 82, 448–457. [Google Scholar] [CrossRef]
- Chang, Y.; Koenig, L.J.; Pruszynski, J.E.; Bradley, T.G.; Bosio, J.A.; Liu, D. Dimensional changes of upper airway after rapid maxillary expansion: A prospective cone-beam computed tomography study. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 462–470. [Google Scholar] [CrossRef] [PubMed]
- Bouserhal, J.; Bassil-Nassif, N.; Tauk, A.; Will, L.; Limme, M. Three-dimensional changes of the naso-maxillary complex following rapid maxillary expansion. Angle Orthod. 2014, 84, 88–95. [Google Scholar] [CrossRef]
- Caldas, L.D.; Takeshita, W.M.; Machado, A.W.; Bittencourt, M.A.V. Effect of rapid maxillary expansion on nasal cavity assessed with cone-beam computed tomography. Dental Press J. Orthod. 2020, 25, 39–45. [Google Scholar] [CrossRef]
- Buck, L.M.; Dalci, O.; Darendeliler, M.A.; Papageorgiou, S.N.; Papadopoulou, A.K. Volumetric upper airway changes after rapid maxillary expansion a systematic review and meta-analysis. Eur. J. Orthod. 2017, 39, 463–473. [Google Scholar] [CrossRef] [PubMed]
- Haas, A.J. The treatment of maxillary deficiency by opening the mid-palatal suture. Angle Orthod. 1965, 35, 200–217. [Google Scholar] [PubMed]
- Babacan, H.; Sokucu, O.; Doruk, C.; Ay, S. Rapid maxillary expansion and surgically assisted rapid maxillary expansion effects on nasal volume. Angle Orthod. 2006, 76, 66–71. [Google Scholar] [PubMed]
- Doruk, C.; Sökücü, O.; Biçakçi, A.A.; Yilmaz, U.; Taş, F. Comparison of nasal volume changes during rapid maxillary expansion using acoustic rhinometry and computed tomography. Eur. J. Orthod. 2007, 29, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Conroy-Piskai, C.; Galang-Boquiren, M.T.; Obrez, A.; Viana, M.G.; Oppermann, N.; Sanchez, F.; Edgren, B.; Kusnoto, B. Assessment of vertical changes during maxillary expansion using quad helix or bonded rapid maxillary expander. Angle Orthod. 2016, 86, 925–933. [Google Scholar] [CrossRef] [PubMed]
- Canan, S.; Şenışıkm, N.E. Comparison of the treatment effects of different rapid maxillary expansion devices on the maxilla and the mandible. Part 1: Evaluation of dentoalveolar changes. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 1125–1138. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Xu, T.; Zou, W. Effects of rapid maxillary expansion on the midpalatal suture a systematic review. Eur. J. Orthod. 2015, 37, 651–655. [Google Scholar] [CrossRef] [PubMed]
- Angelieri, F.; Franchi, L.; Cevidanes, L.H.; Bueno-Silva, B.; McNamara, J.A., Jr. Prediction of rapid maxillary expansion by assessing the maturation of the midpalatal suture on cone beam CT. Dental Press J. Orthod. 2016, 21, 115–125. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, G.L.U.; Locks, A.; Pereira, J.; Brunetto, M. Analysis of rapid maxillary expansion using cone-beam computed tomography. Dental Press J. Orthod. 2010, 15, 107–112. [Google Scholar] [CrossRef]
- Angelieri, F.; Franchi, L.; Cevidanes, L.H.; McNamara, J.A., Jr. Diagnostic performance of skeletal maturity for the assessment of midpalatal suture maturation. Am. J. Orthod. Dentofacial Orthop. 2015, 148, 1010–1016. [Google Scholar] [CrossRef] [PubMed]
- Yan-Cheng, L.; Kwok-Hing, H.; Chih-Wei, W.; Kai-Long, W.; Shun Chu, H.; Heng-Ming, C. Skeletal and dental changes after microimplant-assisted rapid palatal expansion (MARPE)—A Cephalometric and Cone-Beam Computed Tomography (CBCT) study. Clin. Investig. Orthod. 2022, 81, 84–92. [Google Scholar]
- El Nahass, H.; Naiem, S.N. Palatal bone dimensions on cone beam computed tomography. Implications for the palate as autogenous donor site: An observational study. Int. J. Oral Maxillofac. Surg. 2016, 45, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Bell, R.A. A review of maxillary expansion in relation to rate of expansion and patient’s age. Am. J. Orthod. 1982, 81, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Moreira, A.M.; de Menezes, L.M.; Roithmann, R.; Rizzatto, S.M.D.; Weissheimer, A.; Yen, S.L.; Enciso, R.; de Lima, E.M.S.; Azeredo, F. Immediate effects of rapid maxillary expansion on the nasal cavity using Haas-type and Hyrax-type expanders in CBCT. Med. Clin. Arch. 2017, 1, 1–5. [Google Scholar]
- McNamara, J.A., Jr.; Baccetti, T.; Franchi, L.; Herberger, T.A. Rapid maxillary expansion followed by fixed appliances: A long-term evaluation of changes in arch dimensions. Angle Orthod. 2003, 73, 344–353. [Google Scholar] [PubMed]
- Pereira, J.D.S.; Jacob, H.B.; Locks, A.; Brunetto, M.; Ribeiro, G.L.U. Evaluation of the rapid and slow maxillary expansion using cone-beam computed tomography: A randomized clinical trial. Dental Press J. Orthod. 2017, 22, 61–68. [Google Scholar] [CrossRef]
- Fastuca, R.; Lorusso, P.; Lagravère, M.O.; Michelotti, A.; Portelli, M.; Zecca, P.A.; Antò, V.D.; Militi, A.; Nucera, R.; Caprioglio, A. Digital evaluation of nasal changes induced by rapid maxillary expansion with different anchorage and appliance design. BMC Oral Health 2017, 17, 113. [Google Scholar] [CrossRef] [PubMed]
- Abdalla, Y.; Brown, L.; Sonnesen, L. Effects of rapid maxillary expansion on upper airway volume: A three-dimensional cone-beam computed tomography study. Angle Orthod. 2019, 89, 917–923. [Google Scholar] [CrossRef] [PubMed]
- Kinzinger, G.S.M.; Hourfar, J.; Buschhoff, C.; Heller, F.; Korbmacher-Steiner, H.M.; Lisson, J.A. Age-dependent interactions of maxillary sutures during RME and their effects on palatal morphology. J. Orofac. Orthop. 2022, 83, 412–431. [Google Scholar] [CrossRef] [PubMed]
- Berlocher, W.C.; Mueller, B.H.; Tinaoff, N. The effect of maxillary palatal expansion on the primary dental arch circumference. Pediatr. Dent. 1980, 2, 27–30. [Google Scholar] [PubMed]
- Aparecida, C.C.; Abrão, J.; Reis, S.A.; de Fantini, S.M. Correlation between transverse expansion and increase in the upper arch perimeter after rapid maxillary expansion. Braz. Oral. Res. 2006, 20, 76–81. [Google Scholar]
- Moussa, R.; O’Reilly, M.T.; Close, J.M. Long-term stability of rapid palatal expander treatment and edgewise mechanotherapy. Am. J. Orthod. Dentofac. Orthop. 1995, 108, 478–488. [Google Scholar] [CrossRef]
- Canuto, L.F.; de Freitas, M.R.; Janson, G.; de Freitas, K.M.; Martins, P.P. Influence of rapid palatal expansion on maxillary incisor alignment stability. Am. J. Orthod. Dentofac. Orthop. 2010, 137, e1–e6. [Google Scholar] [CrossRef]
- Halicioglu, K.; Kiliç, N.; Yavuz, I.; Aktan, B. Effects of rapid maxillary expansion with a memory palatal split screw on the morphology of the maxillary dental arch and nasal airway resistance. Eur. J. Orthod. 2010, 32, 716–720. [Google Scholar] [CrossRef]
- Haas, A.J. Palatal expansion: Just the beginning of dentofacial orthopedics. Am. J. Orthod. 1970, 57, 219–255. [Google Scholar] [CrossRef] [PubMed]
- Wertz, R.A. Skeletal and dental changes accompanying rapid midpalatal suture opening. Am. J. Orthod. 1970, 58, 41–66. [Google Scholar] [CrossRef]
- Podesser, B.; Williams, S.; Crismani, A.G.; Bantleon, H.P. Evaluation of the effects of rapid maxillary expansion in growing children using computer tomography scanning: A pilot study. Eur. J. Orthod. 2007, 29, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Garib, D.G.; Henriques, J.F.; Janson, G.; Freitas, M.R.; Coelho, R.A. Rapid maxillary expansion—Tooth-tissue-borne vs. tooth-borne expanders: A CT evaluation of dentoskeletal effects. Angle Orthod. 2005, 75, 548–557. [Google Scholar] [PubMed]
- Kartalian, A.; Gohl, E.; Adamian, M.; Enciso, R. Cone-beam computerized tomography evaluation of the maxillary dentoskeletal complex after rapid palatal expansion. Am. J. Orthod Dentofac. Orthop. 2010, 138, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Weissheimer, A.; Menezes, L.M.; Mezomo, M.; Dias, D.M.; Lima, E.M.; Rizzatto, S.M. Immediate effects of rapid maxillary expansion with Haas-type and hyrax-type expanders: A randomized clinical trial. Am. J. Orthod. Dentofac. Orthop. 2011, 140, 366–376. [Google Scholar] [CrossRef]
- Gunyuz Toklu, M.; Germec-Cakan, D.; Tozlu, M. Periodontal, dentoalveolar, and skeletal effects of tooth-borne and tooth-bone-borne expansion appliances. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 97–109. [Google Scholar] [CrossRef] [PubMed]
- Akkaya, S.; Lorenzon, S.; Uçem, T.T. Comparison of dental arch and arch perimeter changes between bonded rapid and slow maxillary expansion procedures. Eur. J. Orthod. 1998, 20, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Seubert, B.J.; Gaalaas, L.; Larson, B.E.; Grünheid, T. Evaluation of transverse maxillary growth on cone-beam computed tomography images. Sci. Rep. 2021, 11, 17462. [Google Scholar] [CrossRef] [PubMed]
- Björk, A.; Skieller, V. Growth in width of the maxilla studied by the implant method. Scand. J. Plast. Reconstr. Surg. 1974, 8, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Björk, A.; Skieller, V. Growth of the maxilla in three dimensions as revealed radiographically by the implant method. Br. J. Orthod. 1977, 4, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Korn, E.; Baumrind, S. Transverse development of the human jaws between the ages of 8.5 and 15.5 years, studied longitudinally with use of implants. J. Dent. Res. 1990, 69, 1298–1306. [Google Scholar] [CrossRef] [PubMed]
- Hesby, R.M.; Marshall, S.D.; Dawson, D.V.; Southard, K.A.; Casko, J.S.; Franciscus, R.G.; Southard, T.E. Transverse skeletal and dentoalveolar changes during growth. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 721–731. [Google Scholar] [CrossRef] [PubMed]
- Barone, T.R.; Cahali, M.B.; Vasconcelos, C.; Barone, J.R. A comparison of tooth-borne and bone-anchored expansion devices in SARME. Oral. Maxillofac. Surg. 2020, 24, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Altug-Atac, A.T.; Karasu, H.A.; Aytac, D. Surgically assisted rapid maxillary expansion compared with orthopedic rapid maxillary expansion. Angle Orthod. 2006, 76, 353–359. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| T1 (Mean) | T2 (Mean) | Difference T2–T1 | SD | IC95% | T | p-Value | D | |
|---|---|---|---|---|---|---|---|---|
| Dentoalveolar variables | ||||||||
| CP (mean) (mm) | 82.97 | 86.4 | 3.42 | 2.09 | [2.45–4.40] | 7.34 | <0.0001 ** | 1.64 |
| RP (mean) (mm) | 80.48 | 83.33 | 2.89 | 1.80 | [2.04–3.73] | 7.18 | <0.0001 ** | 1.61 |
| MA (mean) (degree) | 99.41/ 99.58 | 105.03/ 104.32 | 5.62/ 4.74 | 3.20/ 2.22 | [4.12–7.11]/ [3.70–5.78] | 7.84/9.56 | <0.0001/<0.0001 ** | 1.75/ 2.14 |
| IMW (mean) (mm) | 44.52 | 49.73 | 5.21 | 1.55 | [4.48–5.93] | 15.03 | <0.0001 ** | 3.36 |
| Skeletal variables | ||||||||
| SO (mean) (mm) | 0 | 2.85 | 2.85 | 0.62 | [2.57–3.14] | 20.84 | <0.0001 ** | 4.66 |
| NBW (mean) (mm) | 25.24 | 26.52 | 1.28 | 0.64 | [0.98–1.57] | 8.99 | <0.0001 ** | 2.01 |
| PH (mean) (mm) | 15.79 | 15.13 | −0.65 | 0.64 | [−0.95–−0.35] | −4.56 | <0.0001 ** | 1.02 |
| JR–JL (mean) (mm) | 59.68 | 62.47 | 2.79 | 1.48 | [2.10–3.48] | 8.43 | <0.0001 ** | 1.89 |
| Male Mean (SD) | Female Mean (SD) | p-Value | |
|---|---|---|---|
| DIF_CP | 3.51 (1.95) | 3.34 (2.28) | 0.863 |
| DIF_RP | 2.35 (1.59) | 3.32 (1.90) | 0.238 |
| DIF_NBW | 1.06 (0.71) | 1.45 (0.53) | 0.178 |
| DIF_IMW | 5.20 (1.64) | 5.21 (1.54) | 0.989 |
| DIF_PH | −0.65 (0.58) | −0.65 (0.70) | 0.999 |
| DIF_MA Right molar | 5.21 (3.62) | 5.94 (2.94) | 0.623 |
| DIF_MA Left molar | 3.28 (1.95) | 5.93 (1.68) | 0.004 ** |
| DIF_JR–JL | 2.68 (1.22) | 2.87 (1.71) | 0.789 |
| SO_T2 | 2.92 (0.53) | 2.79 (0.68) | 0.634 |
| AGE_T2 | Dif_CP | Dif_RP | Dif_ NBW | Dif_ IMW | Dif_PH | Dif_ MA | Dif_ JR–JL | SO_T2 | |
|---|---|---|---|---|---|---|---|---|---|
| AGE_T2 | 1 | ||||||||
| Dif_CP | −0.118 | 1 | |||||||
| Dif_RP | −0.189 | 0.626 ** | 1 | ||||||
| Dif_ NBW | −0.226 | 0.189 | −0.058 | 1 | |||||
| Dif_ IMW | 0.113 | 0.205 | 0.135 | 0.217 | 1 | ||||
| Dif_PH | −0.099 | −0.177 | −0.242 | −0.357 | −0.434 | 1 | |||
| Dif_MA | −0.129/ 0.067 | −0.063/ 0.066 | −0.027/ 0.200 | −0.019/ 0.319 | 0.454 */ 0.488 * | −0.234/ −0.257 | 1 | ||
| Dif_ JR–JL | −0.029 | 0.317 | 0.446 * | −0.037 | 0.346 | −0.400 | 0.091/ 0.133 | 1 | |
| SO_T2 | −0.165 | 0.558 * | 0.726 ** | 0.099 | −0.080 | −0.126 | −0.029/ −0.057 | 0.091 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colino-Gallardo, P.; Del Fresno-Aguilar, I.; Castillo-Montaño, L.; Colino-Paniagua, C.; Baptista-Sánchez, H.; Criado-Pérez, L.; Alvarado-Lorenzo, A. Skeletal and Dentoalveolar Changes in Growing Patients Treated with Rapid Maxillary Expansion Measured in 3D Cone-Beam Computed Tomography. Biomedicines 2023, 11, 3305. https://doi.org/10.3390/biomedicines11123305
Colino-Gallardo P, Del Fresno-Aguilar I, Castillo-Montaño L, Colino-Paniagua C, Baptista-Sánchez H, Criado-Pérez L, Alvarado-Lorenzo A. Skeletal and Dentoalveolar Changes in Growing Patients Treated with Rapid Maxillary Expansion Measured in 3D Cone-Beam Computed Tomography. Biomedicines. 2023; 11(12):3305. https://doi.org/10.3390/biomedicines11123305
Chicago/Turabian StyleColino-Gallardo, Peri, Irene Del Fresno-Aguilar, Laura Castillo-Montaño, Carlos Colino-Paniagua, Hugo Baptista-Sánchez, Laura Criado-Pérez, and Alfonso Alvarado-Lorenzo. 2023. "Skeletal and Dentoalveolar Changes in Growing Patients Treated with Rapid Maxillary Expansion Measured in 3D Cone-Beam Computed Tomography" Biomedicines 11, no. 12: 3305. https://doi.org/10.3390/biomedicines11123305