
Intranasal Lidocaine Administration via Mucosal Atomization Device: A Simple and Successful Treatment for Postdural Puncture Headache in Obstetric Patients
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval of the Study Protocol
2.2. Data Collection
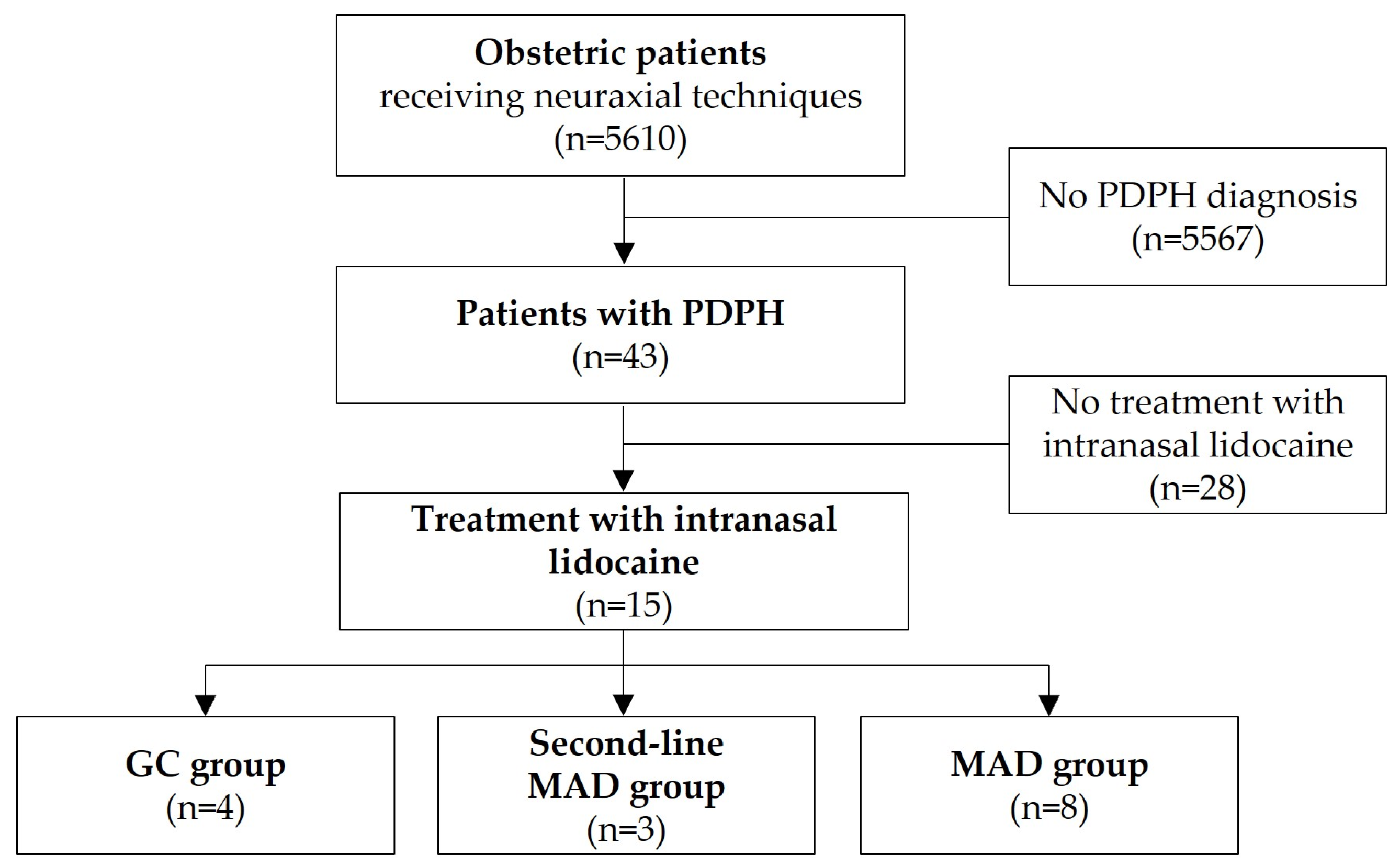
2.3. Study Population, In- and Exclusion Criteria
2.4. Intranasal Application of Lidocaine
2.5. Study-Related Data and Outcome Measures
2.6. Statistical Analysis
3. Results
3.1. Patients’ Characteristics and Clinical Management of PDPH
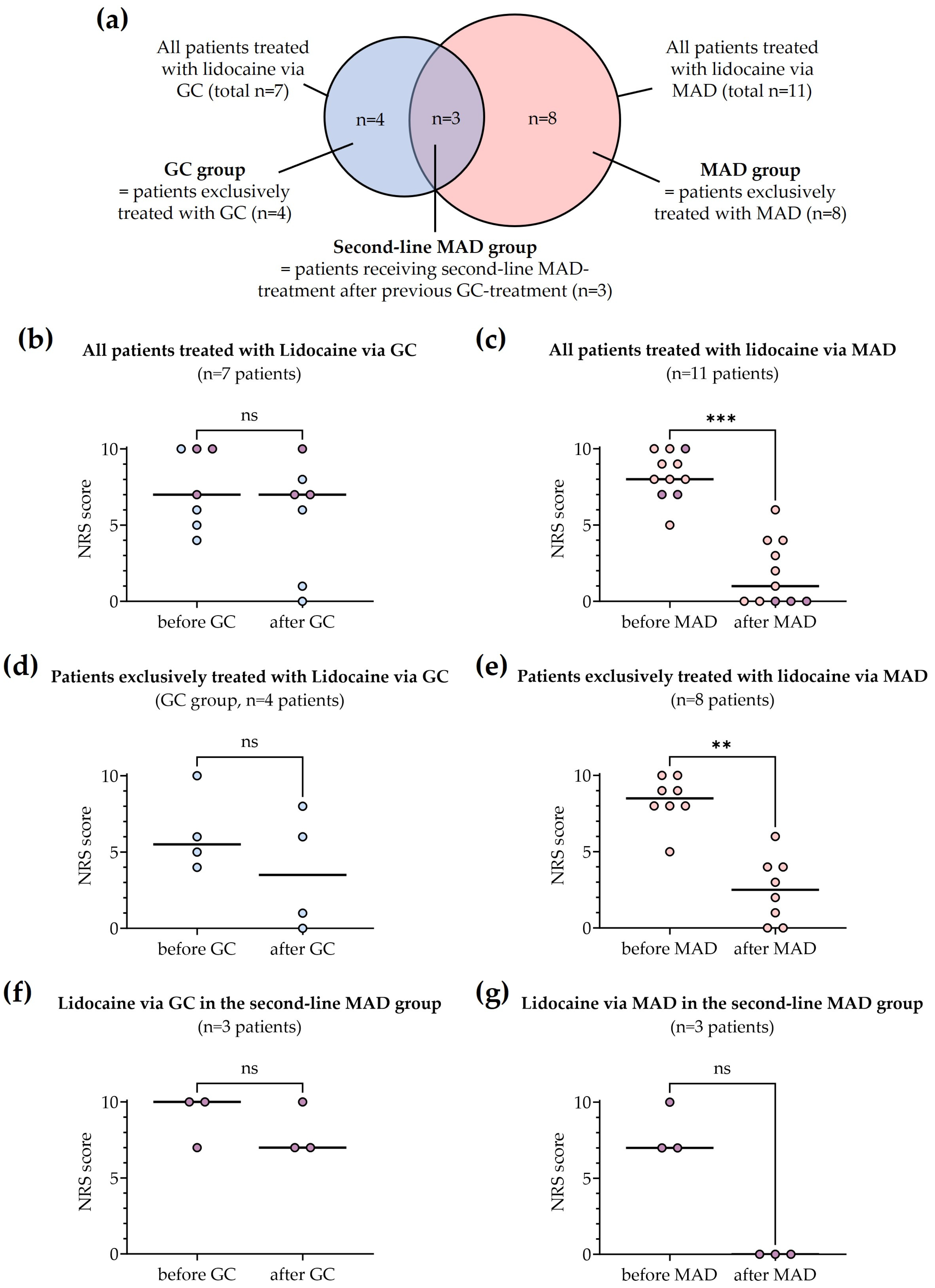
3.2. Intranasal Lidocaine Administration
3.3. Reduction of Pain Intensity
3.4. Adverse Events, Recurring Symptoms and Need for an EBP
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Seijmonsbergen-Schermers, A.E.; van den Akker, T.; Rydahl, E. Variations in use of childbirth interventions in 13 high-income countries: A multinational cross-sectional study. PLoS Med. 2020, 17, e1003103. [Google Scholar] [CrossRef]
- Delgado, C.; Bollag, L.; Van Cleve, W. Neuraxial Labor Analgesia Utilization, Incidence of Postdural Puncture Headache, and Epidural Blood Patch Placement for Privately Insured Parturients in the United States (2008–2015). Anesth. Analg. 2020, 131, 850–856. [Google Scholar] [CrossRef]
- Butwick, A.J.; Bentley, J.; Wong, C.A.; Snowden, J.M.; Sun, E.; Guo, N. United States State-Level Variation in the Use of Neuraxial Analgesia During Labor for Pregnant Women. JAMA Netw. Open 2018, 1, e186567. [Google Scholar] [CrossRef]
- Brebion, M.; Bonnet, M.P.; Sauvegrain, P.; Saurel-Cubizolles, M.J.; Blondel, B.; Deneux-Tharaux, C.; Azria, E. Use of labour neuraxial analgesia according to maternal immigration status: A national cross-sectional retrospective population-based study in France. Br. J. Anaesth. 2021, 127, 942–952. [Google Scholar] [CrossRef]
- D’Angelo, R.; Smiley, R.M.; Riley, E.T.; Segal, S. Serious complications related to obstetric anesthesia: The serious complication repository project of the Society for Obstetric Anesthesia and Perinatology. Anesthesiology 2014, 120, 1505–1512. [Google Scholar] [CrossRef]
- Guglielminotti, J.; Landau, R.; Li, G. Major Neurologic Complications Associated With Postdural Puncture Headache in Obstetrics: A Retrospective Cohort Study. Anesth. Analg. 2019, 129, 1328–1336. [Google Scholar] [CrossRef]
- Sprigge, J.S.; Harper, S.J. Accidental dural puncture and post dural puncture headache in obstetric anaesthesia: Presentation and management: A 23-year survey in a district general hospital. Anaesthesia 2008, 63, 36–43. [Google Scholar] [CrossRef]
- Poma, S.; Bonomo, M.C.; Gazzaniga, G.; Pizzulli, M.; De Silvestri, A.; Baldi, C.; Broglia, F.; Ciceri, M.; Fuardo, M.; Morgante, F.; et al. Complications of unintentional dural puncture during labour epidural analgesia: A 10-year retrospective observational study. J. Anesth. Analg. Crit. Care 2023, 3, 42. [Google Scholar] [CrossRef]
- Bezov, D.; Ashina, S.; Lipton, R. Post-dural puncture headache: Part II—Prevention, management, and prognosis. Headache 2010, 50, 1482–1498. [Google Scholar] [CrossRef]
- Turnbull, D.K.; Shepherd, D.B. Post-dural puncture headache: Pathogenesis, prevention and treatment. Br. J. Anaesth. 2003, 91, 718–729. [Google Scholar] [CrossRef]
- Reamy, B.V. Post-epidural headache: How late can it occur? J. Am. Board Fam. Med. JABFM 2009, 22, 202–205. [Google Scholar] [CrossRef] [PubMed]
- Stella, C.L.; Jodicke, C.D.; How, H.Y.; Harkness, U.F.; Sibai, B.M. Postpartum headache: Is your work-up complete? Am. J. Obstet. Gynecol. 2007, 196, 318.e1–318.e7. [Google Scholar] [CrossRef] [PubMed]
- Costigan, S.N.; Sprigge, J.S. Dural puncture: The patients’ perspective. A patient survey of cases at a DGH maternity unit 1983–1993. Acta Anaesthesiol. Scand. 1996, 40, 710–714. [Google Scholar] [CrossRef] [PubMed]
- Mims, S.C.; Tan, H.S.; Sun, K.; Pham, T.; Rubright, S.; Kaplan, S.J.; Habib, A.S. Long-term morbidities following unintentional dural puncture in obstetric patients: A systematic review and meta-analysis. J. Clin. Anesth. 2022, 79, 110787. [Google Scholar] [CrossRef] [PubMed]
- Siegler, B.H.; Oehler, B.; Kranke, P.; Weigand, M.A. Postdural puncture headache in obstetrics: Pathogenesis, diagnostics and treatment. Die Anaesthesiol. 2022, 71, 646–660. [Google Scholar] [CrossRef] [PubMed]
- Bremerich, D.; Annecke, T.; Chapell, D.; Hanß, R.; Kaufner, L.; Kehl, F.; Kranke, P.; Girard, T.; Gogarten, W.; Greve, S.; et al. AWMF-Guideline “Die Geburtshilfliche Analgesie und Anästhesie. S1-Leitlinie der Deutschen Gesellschaft für Anästhesiologie und Intensivmedizin in Zusammenarbeit mit der Deutschen Gesellschaft für Gynäkologie und Geburtshilfe” Registry Number 001-038. 2020. Available online: https://www.awmf.org/leitlinien/detail/ll/001-038.html (accessed on 11 December 2023).
- Uppal, V.; Russell, R.; Sondekoppam, R.V.; Ansari, J.; Baber, Z.; Chen, Y.; DelPizzo, K.; Dirzu, D.S.; Kalagara, H.; Kissoon, N.R.; et al. Evidence-based clinical practice guidelines on postdural puncture headache: A consensus report from a multisociety international working group. Reg. Anesth. Pain Med. 2023, 1–31. [Google Scholar] [CrossRef] [PubMed]
- Radke, K.; Radke, O.C. Post-dural puncture headache. Der Anaesthesist 2013, 62, 149–161. [Google Scholar] [CrossRef] [PubMed]
- Woodward, W.M.; Levy, D.M.; Dixon, A.M. Exacerbation of post-dural puncture headache after epidural blood patch. Can. J. Anaesth. J. Can. D’anesthesie 1994, 41, 628–631. [Google Scholar] [CrossRef]
- Gupta, A.; von Heymann, C.; Magnuson, A.; Alahuhta, S.; Fernando, R.; Van de Velde, M.; Mercier, F.J.; Schyns-van den Berg, A. Management practices for postdural puncture headache in obstetrics: A prospective, international, cohort study. Br. J. Anaesth. 2020, 125, 1045–1055. [Google Scholar] [CrossRef]
- Abdelaal Ahmed Mahmoud, A.; Mansour, A.Z.; Yassin, H.M.; Hussein, H.A.; Kamal, A.M.; Elayashy, M.; Elemady, M.F.; Elkady, H.W.; Mahmoud, H.E.; Cusack, B.; et al. Addition of Neostigmine and Atropine to Conventional Management of Postdural Puncture Headache: A Randomized Controlled Trial. Anesth. Analg. 2018, 127, 1434–1439. [Google Scholar] [CrossRef]
- Thangathurai, D.; Bowles, H.F.; Allen, H.W.; Mikhail, M.S. Epidural morphine and headache secondary to dural puncture. Anaesthesia 1988, 43, 519. [Google Scholar] [CrossRef] [PubMed]
- Dietzel, J.; Witstruck, T.; Adler, S.; Usichenko, T.I. Acupuncture for treatment of therapy-resistant post-dural puncture headache: A retrospective case series. Br. J. Anaesth. 2013, 111, 847–849. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Cheam, E. Acupuncture in the management of post-partum headache following neuraxial analgesia. Int. J. Obstet. Anesth. 2009, 18, 417–419. [Google Scholar] [CrossRef] [PubMed]
- Kent, S.; Mehaffey, G. Transnasal sphenopalatine ganglion block for the treatment of postdural puncture headache in obstetric patients. J. Clin. Anesth. 2016, 34, 194–196. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, L.M.; Godinho, P.M.; Durán, F.J.; Valente, E.C. Sphenopalatine ganglion block by transnasal approach in post-dural puncture headache. J. Clin. Anesth. 2018, 48, 50. [Google Scholar] [CrossRef] [PubMed]
- Urits, I.; Viswanath, O.; Orhurhu, V.; Petro, J.; Cai, V. Sphenopalatine ganglion block in combination with greater and lesser occipital nerve blocks for the management of post dural puncture headache. J. Clin. Anesth. 2019, 52, 69–70. [Google Scholar] [CrossRef] [PubMed]
- Youssef, H.A.; Abdel-Ghaffar, H.S.; Mostafa, M.F.; Abbas, Y.H.; Mahmoud, A.O.; Herdan, R.A. Sphenopalatine Ganglion versus Greater Occipital Nerve Blocks in Treating Post-Dural Puncture Headache after Spinal Anesthesia for Cesarean Section: A Randomized Clinical Trial. Pain Physician 2021, 24, E443–E451. [Google Scholar]
- Cohen, S.; Levin, D.; Mellender, S.; Zhao, R.; Patel, P.; Grubb, W.; Kiss, G. Topical Sphenopalatine Ganglion Block Compared With Epidural Blood Patch for Postdural Puncture Headache Management in Postpartum Patients: A Retrospective Review. Reg. Anesth. Pain Med. 2018, 43, 880–884. [Google Scholar] [CrossRef]
- Jespersen, M.S.; Jaeger, P.; Ægidius, K.L.; Fabritius, M.L.; Duch, P.; Rye, I.; Afshari, A.; Meyhoff, C.S. Sphenopalatine ganglion block for the treatment of postdural puncture headache: A randomised, blinded, clinical trial. Br. J. Anaesth. 2020, 124, 739–747. [Google Scholar] [CrossRef]
- Siegler, B.H.; Gruß, M.; Oehler, B.; Keßler, J.; Fluhr, H.; Weis, C.; Schulz, F.; Weigand, M.A. Intranasal lidocaine atomization as novel and noninvasive treatment option for postdural puncture headache: Two case reports from obstetric anesthesiology. Der Anaesthesist 2021, 70, 392–397. [Google Scholar] [CrossRef]
- Dieterich, M. Diagnostik und Therapie des Postpunktionellen und Spontanen Liquorunterdruck-Syndroms, S1-Guideline, in: Deutsche Gesellschaft für Neurologie (Hrsg.), Leitlinien für Diagnostik und Therapie in der Neurologie. 2018. Available online: www.dgn.org/leitlinien (accessed on 10 October 2023).
- Ranganathan, P.; Golfeiz, C.; Phelps, A.L.; Singh, S.; Shnol, H.; Paul, N.; Attaallah, A.F.; Vallejo, M.C. Chronic headache and backache are long-term sequelae of unintentional dural puncture in the obstetric population. J. Clin. Anesth. 2015, 27, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Khonsary, S.A.; Ma, Q.; Villablanca, P.; Emerson, J.; Malkasian, D. Clinical functional anatomy of the pterygopalatine ganglion, cephalgia and related dysautonomias: A review. Surg. Neurol. Int. 2013, 4, S422–S428. [Google Scholar] [CrossRef] [PubMed]
- Piagkou, M.; Demesticha, T.; Troupis, T.; Vlasis, K.; Skandalakis, P.; Makri, A.; Mazarakis, A.; Lappas, D.; Piagkos, G.; Johnson, E.O. The pterygopalatine ganglion and its role in various pain syndromes: From anatomy to clinical practice. Pain Pract. 2012, 12, 399–412. [Google Scholar] [CrossRef] [PubMed]
- Dwivedi, P.; Singh, P.; Patel, T.K.; Bajpai, V.; Kabi, A.; Singh, Y.; Sharma, S.; Kishore, S. Trans-nasal sphenopalatine ganglion block for post-dural puncture headache management: A meta-analysis of randomized trials. Braz. J. Anesth. 2023, 73, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Santos, N.S.; Nunes, J.M.; Font, M.L.; Carmona, C.; Castro, M.M. Early versus late sphenopalatine ganglion block with ropivacaine in postdural puncture headache: An observational study. Braz. J. Anesth. 2023, 73, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Levin, D.; Cohen, S. Images in anesthesiology: Three safe, simple, and inexpensive methods to administer the sphenopalatine ganglion block. Reg. Anesth. Pain Med. 2020, 45, 880–882. [Google Scholar] [CrossRef] [PubMed]
- Binfalah, M.; Alghawi, E.; Shosha, E.; Alhilly, A.; Bakhiet, M. Sphenopalatine Ganglion Block for the Treatment of Acute Migraine Headache. Pain Res. Treat. 2018, 2018, 2516953. [Google Scholar] [CrossRef]
- Cady, R.; Saper, J.; Dexter, K.; Manley, H.R. A double-blind, placebo-controlled study of repetitive transnasal sphenopalatine ganglion blockade with tx360(®) as acute treatment for chronic migraine. Headache 2015, 55, 101–116. [Google Scholar] [CrossRef]
- Scavone, J.M.; Greenblatt, D.J.; Fraser, D.G. The bioavailability of intranasal lignocaine. Br. J. Clin. Pharmacol. 1989, 28, 722–724. [Google Scholar] [CrossRef]
- Johnson, N.J.; Hanson, L.R.; Frey, W.H. Trigeminal pathways deliver a low molecular weight drug from the nose to the brain and orofacial structures. Mol. Pharm. 2010, 7, 884–893. [Google Scholar] [CrossRef]
- Burkett, J.G.; Robbins, M.S.; Robertson, C.E.; Mete, M.; Saikali, N.P.; Halker Singh, R.B.; Ailani, J. Sphenopalatine ganglion block in primary headaches: An American Headache Society member survey. Neurol. Clin. Pract. 2020, 10, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Narouze, S. Topical intranasal lidocaine is not a sphenopalatine ganglion block. Reg. Anesth. Pain Med. 2021, 46, 276–279. [Google Scholar] [CrossRef] [PubMed]
- Berger, J.J.; Pyles, S.T.; Saga-Rumley, S.A. Does topical anesthesia of the sphenopalatine ganglion with cocaine or lidocaine relieve low back pain? Anesth. Analg. 1986, 65, 700–702. [Google Scholar] [CrossRef] [PubMed]
- Chua, H.; Loh, L.; Mok, M. Transnasal sphenopalatine ganglion block for post-dural puncture headache and associated tinnitus. Anaesth. Rep. 2021, 9, 37–40. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, F.M.; Kaufman, A.G.; Dunbar, S.A.; Cain, C.F.; Cherukuri, S. Sphenopalatine ganglion block for the treatment of myofascial pain of the head, neck, and shoulders. Reg. Anesth. Pain Med. 1998, 23, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Kanai, A.; Suzuki, A.; Kobayashi, M.; Hoka, S. Intranasal lidocaine 8% spray for second-division trigeminal neuralgia. Br. J. Anaesth. 2006, 97, 559–563. [Google Scholar] [CrossRef] [PubMed]
- Levin, D.; Acquadro, M.; Cerasuolo, J.; Gerges, F. Sphenopalatine ganglion block for ipsilateral shoulder pain following open pancreaticoduodenectomy. BMJ Case Rep. 2022, 15, e243746. [Google Scholar] [CrossRef]
- Moore, D.; Chong, M.S.; Shetty, A.; Zakrzewska, J.M. A systematic review of rescue analgesic strategies in acute exacerbations of primary trigeminal neuralgia. Br. J. Anaesth. 2019, 123, e385–e396. [Google Scholar] [CrossRef]
- Quevedo, J.P.; Purgavie, K.; Platt, H.; Strax, T.E. Complex regional pain syndrome involving the lower extremity: A report of 2 cases of sphenopalatine block as a treatment option. Arch. Phys. Med. Rehabil. 2005, 86, 335–337. [Google Scholar] [CrossRef]
- Hermanns, H.; Hollmann, M.W.; Stevens, M.F.; Lirk, P.; Brandenburger, T.; Piegeler, T.; Werdehausen, R. Molecular mechanisms of action of systemic lidocaine in acute and chronic pain: A narrative review. Br. J. Anaesth. 2019, 123, 335–349. [Google Scholar] [CrossRef]
- van der Wal, S.E.; van den Heuvel, S.A.; Radema, S.A.; van Berkum, B.F.; Vaneker, M.; Steegers, M.A.; Scheffer, G.J.; Vissers, K.C. The in vitro mechanisms and in vivo efficacy of intravenous lidocaine on the neuroinflammatory response in acute and chronic pain. Eur. J. Pain (Lond. Engl.) 2016, 20, 655–674. [Google Scholar] [CrossRef] [PubMed]
- Fassoulaki, A.; Sarantopoulos, C.; Melemeni, A.; Hogan, Q. EMLA reduces acute and chronic pain after breast surgery for cancer. Reg. Anesth. Pain Med. 2000, 25, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Chaplan, S.R.; Bach, F.W.; Shafer, S.L.; Yaksh, T.L. Prolonged alleviation of tactile allodynia by intravenous lidocaine in neuropathic rats. Anesthesiology 1995, 83, 775–785. [Google Scholar] [CrossRef] [PubMed]
- Hu, K.L.; Mei, N.; Feng, L.; Jiang, X.G. Hydrophilic nasal gel of lidocaine hydrochloride. 2nd communication: Improved bioavailability and brain delivery in rats with low ciliotoxicity. Arzneim. Forsch. 2009, 59, 635–640. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Total (n = 15 Patients) | GC Group (n = 4 Patients) | Second-Line MAD Group (n = 3 Patients) | MAD Group (n = 8 Patients) |
|---|---|---|---|---|
| Age (years) | 32 (24 to 40) | 30 (26 to 40) | 34 (24 to 36) | 33 (29 to 40) |
| Body weight (kg) | 71 (57 to 179) | 80 (58 to 179) | 80 (60 to 140) | 71 (57 to 95) |
| Height (cm) | 163 (158 to 182) | 161 (158 to 170) | 160 (160 to 160) | 170 (150 to 182) |
| Body mass index (kg/m2) | 27 (21 to 70) | 29 (22 to 70) | 31 (23 to 55) | 25 (21 to 32) |
| Risk factors for PDPH | ||||
| Age 20–30 years | 6 (40%) | 3 (75%) | 1 (33%) | 2 (25%) |
| Body mass index < 20 kg/m2 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| History of headache/migraine | 3 (20%) | 1 (25%) | 1 (33%) | 1 (13%) |
| History of PDPH | 3 (20%) | 1 (25%) | 1 (33%) | 1 (13%) |
| Neuraxial technique | ||||
| Spinal anesthesia | 8 (53%) | 2 (50%) | 2 (67%) | 4 (50%) |
| Epidural anesthesia | 5 (33%) | 0 (0.0%) | 1 (33%) | 4 (50%) |
| Both a | 2 (13%) | 2 (50%) | 0 (0.0%) | 0 (0.0%) |
| Time from puncture to PDPH onset (days) | 1.0 (0.0 to 3.0) | 1.5 (1.0 to 3.0) | 1.0 (1.0 to 1.0) | 1.5 (0.0 to 3.0) |
| Pain intensity at time of PDPH diagnosis (NRS score) | 7 (2 to 10) | 7 (5 to 10) | 6 (3 to 10) | 8.5 (2 to 10) |
| PDPH-associated symptoms | ||||
| Neck stiffness/pain | 12 (80%) | 4 (100%) | 2 (67%) | 6 (75%) |
| Tinnitus/hearing loss | 3 (20%) | 0 (0.0%) | 0 (0.0%) | 3 (38%) |
| Photophobia | 1 (6.7%) | 0 (0.0%) | 0 (0.0%) | 1 (13%) |
| Nausea/vomiting | 4 (27%) | 2 (50%) | 0 (0.0%) | 2 (25%) |
| Conservative treatment | ||||
| Oral/IV fluid intake | 9 (60%) | 3 (75%) | 1 (33%) | 5 (63%) |
| Caffeine | 12 (80%) | 3 (75%) | 3 (100%) | 6 (75%) |
| Ibuprofen | 12 (80%) | 3 (75%) | 3 (100%) | 6 (75%) |
| Paracetamol | 8 (53%) | 2 (50%) | 1 (33%) | 5 (63%) |
| Patient | Technique (Needle Size) | Attempts/ Risks | Day of PDPH Diagnosis a | Imaging/Neurol. Review | EBP | Day of Intranasal Lidocaine Started b | Treatment Group | Number of Treatments | NRS ≤ 3 within 1 h | NRS ≤ 3 within 24 h |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | EDA (18G) SpA (25G) | Multiple c | 2 | No | refused | 4 | GC | 1 | No | Yes |
| 2 | EDA (18G) SpA (25G) | Multiple d | 1 | No | refused | 4 | GC | 3 per day, 3 days | No | No |
| 3 | SpA (25G) | 4 attempts 2 levels | 1 | No | refused | 2 | GC | 1 | No | No |
| 4 | SpA (25G) | 1 attempt, BMI 69.9 | 3 | No | refused | 3 | GC | 1 | No | Yes |
| 5 | SpA (25G) | 1 attempt | 1 | No | refused | 1 | Second-line MAD | 1xGC, 1xMAD (next day) | No | Yes (after MAD) |
| 6 | EDA (18G) | 4 attempts, 2 levels | 1 | No | refused | 2 | Second-line MAD | 1xGC, 1xMAD (next day) | Yes (after MAD) | Yes (after MAD) |
| 7 | SpA (22G) | 2 attempts, 2 levels, BMI 54.7 | 1 | No | refused, too difficult | 1 | Second-line MAD | 1xGC 1xMAD (same day) | Yes (after MAD) | Yes (after MAD) |
| 8 | SpA (25G) | 2 attempts, 1 level | 3 | No | refused | 3 | MAD | 1 | Yes | Yes |
| 9 | SpA (25G) | 1 attempt | 1 | No | refused | 1 | MAD | 1 | Yes | Yes |
| 10 | SpA (25G) | 2 attempts, 1 level | 1 | No | refused | 4 | MAD | 1 | No | Yes |
| 11 | EDA (18G) | 3 attempts, 1 level | 2 | No | refused | 3 | MAD | 1 | No | No |
| 12 | EDA (18G) | 2 attempts, 1 level | 3 | No | refused | 4 | MAD | 1 | No | Yes |
| 13 | EDA (18G) | 2 attempts, 2 levels, ADP | 0 | No | refused | 1 | MAD | 3 per day, 3 days | No | No |
| 14 | SpA (25G) | 2 attempts, 1 level | 1 | No | refused | 1 | MAD | 1 | Yes | Yes |
| 15 | EDA (18G) | 2 attempts 2 levels, ADP | 2 | No | refused | 2 | MAD | 2 within 3 h | No | No |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siegler, B.H.; dos Santos Pereira, R.P.; Keßler, J.; Wallwiener, S.; Wallwiener, M.; Larmann, J.; Picardi, S.; Carr, R.; Weigand, M.A.; Oehler, B. Intranasal Lidocaine Administration via Mucosal Atomization Device: A Simple and Successful Treatment for Postdural Puncture Headache in Obstetric Patients. Biomedicines 2023, 11, 3296. https://doi.org/10.3390/biomedicines11123296
Siegler BH, dos Santos Pereira RP, Keßler J, Wallwiener S, Wallwiener M, Larmann J, Picardi S, Carr R, Weigand MA, Oehler B. Intranasal Lidocaine Administration via Mucosal Atomization Device: A Simple and Successful Treatment for Postdural Puncture Headache in Obstetric Patients. Biomedicines. 2023; 11(12):3296. https://doi.org/10.3390/biomedicines11123296
Chicago/Turabian StyleSiegler, Benedikt Hermann, Rui Pedro dos Santos Pereira, Jens Keßler, Stephanie Wallwiener, Markus Wallwiener, Jan Larmann, Susanne Picardi, Richard Carr, Markus Alexander Weigand, and Beatrice Oehler. 2023. "Intranasal Lidocaine Administration via Mucosal Atomization Device: A Simple and Successful Treatment for Postdural Puncture Headache in Obstetric Patients" Biomedicines 11, no. 12: 3296. https://doi.org/10.3390/biomedicines11123296