
Textural Analysis of Magnetic Resonance Images as an Additional Evaluation Tool of Parotid Glands in Sjögren—Primarily Findings

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Group
- For participants above 16 years, informed consent was obtained from all for study participation.
- For participants below 16 years, informed consent was obtained from all of the parents or legal guardians for study participation.
2.2. MRI Examination
- Diffusion-weighted imaging (DWI) is sensitive to the movement of water molecules within tissues. It offers a valuable understanding of the tissue microstructure and helps identify areas of restricted diffusion, which can specify various pathological conditions.
- T2-weighted imaging offers exceptional contrast for visualizing different types of tissues, making this type of sequence helpful in identifying anatomical structures and pathological changes. This image can highlight areas of edema and inflammation, which can be highly important in the context of diseases like Sjögren’s Syndrome.
2.3. Image Analysis
- Grade 0 (normal)—no evidence;
- Grade 1 (punctate)—areas ≤ 1 mm in diameter;
- Grade 2 (globular)—1–2 mm in diameter;
- Grade 3 (cavitary)—up to 1 cm in diameter;
- Grade 4 (destructive)— complete destruction of the gland parenchyma.
- First-order statistic (FSO), including Energy, Total Energy, Entropy, Minimum, 10th percentile, 90th percentile, Maximum, Mean, Median, Interquartile Range, Range, Mean Absolute Deviation (MAD), Robust Mean Absolute Deviation (rMAD), Root Mean Square (RMS), Standard Deviation, Skewness, Kurtosis, Variance, Uniformity;
- Gray Level Co-occurrence Matrix (GLCM) features, including Joint Average, Cluster Prominence, Cluster Shade, Cluster Tendency, Contrast, Correlation, Difference Average, Difference Entropy, Difference Variance, Joint Energy, Joint Entropy, Informational Measure of Correlation 1 and 2 (IMC), Inverse Difference Moment (IDM), Maximal Correlation Coefficient (MCC), Inverse Difference Moment Normalized (IDMN), Inverse Difference (ID), Inverse Difference Normalized (IDN), Inverse Variance, Maximum Probability, Sum Average, Sum Entropy, Sum of Squares;
- Gray Level Size Zone Matrix (GLSZM) features, including Small Area Emphasis (SAE), Large Area Emphasis (LAE), Gray Level Non-Uniformity (GLN), Gray Level Non-Uniformity Normalized (GLNN), Size-Zone Non-Uniformity (SZN), Size-Zone Non-Uniformity Normalized (SZNN), Zone Percentage (ZP), Gray Level Variance (GLV), Zone Variance (ZV), Zone Entropy (ZE), Low Gray Level Zone Emphasis (LGLZE), High Gray Level Zone Emphasis (HGLZE), Small Area Low Gray Level Emphasis (SALGLE), Small Area High Gray Level Emphasis (SAHGLE), Large Area Low Gray Level Emphasis (LALGLE), Large Area High Gray Level Emphasis (LAHGLE);
- Gray Level Run Length Matrix (GLRLM) features, including Short Run Emphasis (SRE), Long Run Emphasis (LRE), Gray Level Non-Uniformity (GLN), Gray Level Non-Uniformity Normalized (GLNN), Run Length Non-Uniformity (RLN), Run Length Non-Uniformity Normalized (RLNN), Run Percentage (RP), Gray Level Variance (GLV), Run Variance (RV), Run Entropy (RE), Low Gray Level Run Emphasis (LGLRE), High Gray Level Run Emphasis (HGLRE), Short Run Low Gray Level Emphasis (SRLGLE), Short Run High Gray Level Emphasis (SRHGLE), Long Run Low Gray Level Emphasis (LRLGLE), Long Run High Gray Level Emphasis (LRHGLE);
- Neighboring Gray Tone Difference Matrix (NGTDM) features, including Coarseness, Contrast, Busyness, Complexity, Strength;
- Gray Level Dependence Matrix (GLDM) features, including Small Dependence Emphasis (SDE), Large Dependence Emphasis (LDE), Gray Level Non-Uniformity (GLN), Dependence Non-Uniformity (DN), Dependence Non-Uniformity Normalized (DNN), Gray Level Variance (GLV), Dependence Variance (DV), Dependence Entropy (DE), Low Gray Level Emphasis (LGLE), High Gray Level Emphasis (HGLE), Small Dependence Low Gray Level Emphasis (SDLGLE), Small Dependence High Gray Level Emphasis (SDHGLE), Large Dependence Low Gray Level Emphasis (LDLGLE), Large Dependence High Gray Level Emphasis (LDHGLE).

2.4. Statistical Analysis
3. Results
3.1. MRI Sialography Grades by the Tonami Scale
3.2. ADC Values
- 1–healthy (p = 0.005),
- 1–3 (p = 0.046),
- 0–3 (p = 0.035),
- 0–healthy (p = 0.001).


{kind=link}
{kind=link}
| Parameters | Tonami Scale | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Healthy | 0 | 1 | 2 | 3 | ||||||
| Mean | Std. Deviation | Mean | Std. Deviation | Mean | Std. Deviation | Mean | Std. Deviation | Mean | Std. Deviation | |
| Mean [10−3 mm2/s] | 1.04 | 0.10 | 0.88 | 0.14 | 0.86 | 0.09 | 0.97 | 0.17 | 1.04 | 0.19 |
| Median [10−3 mm2/s] | 1.06 | 0.10 | 0.86 | 0.14 | 0.88 | 0.09 | 0.96 | 0.17 | 1.03 | 0.19 |
| Entropy | 0.01 | 0.00 | 2.95 | 4.05 | 5.46 | 4.74 | 0.04 | 0.01 | 0.97 | 0.27 |
| Kurtosis | 3.86 | 1.19 | 9.24 | 6.63 | 6.48 | 1.97 | 5.03 | 0.35 | 1.23 | 0.17 |
| Skewness | −0.39 | 0.28 | 0.99 | 0.09 | 0.57 | 0.07 | 0.36 | 0.07 | 0.17 | 0.03 |
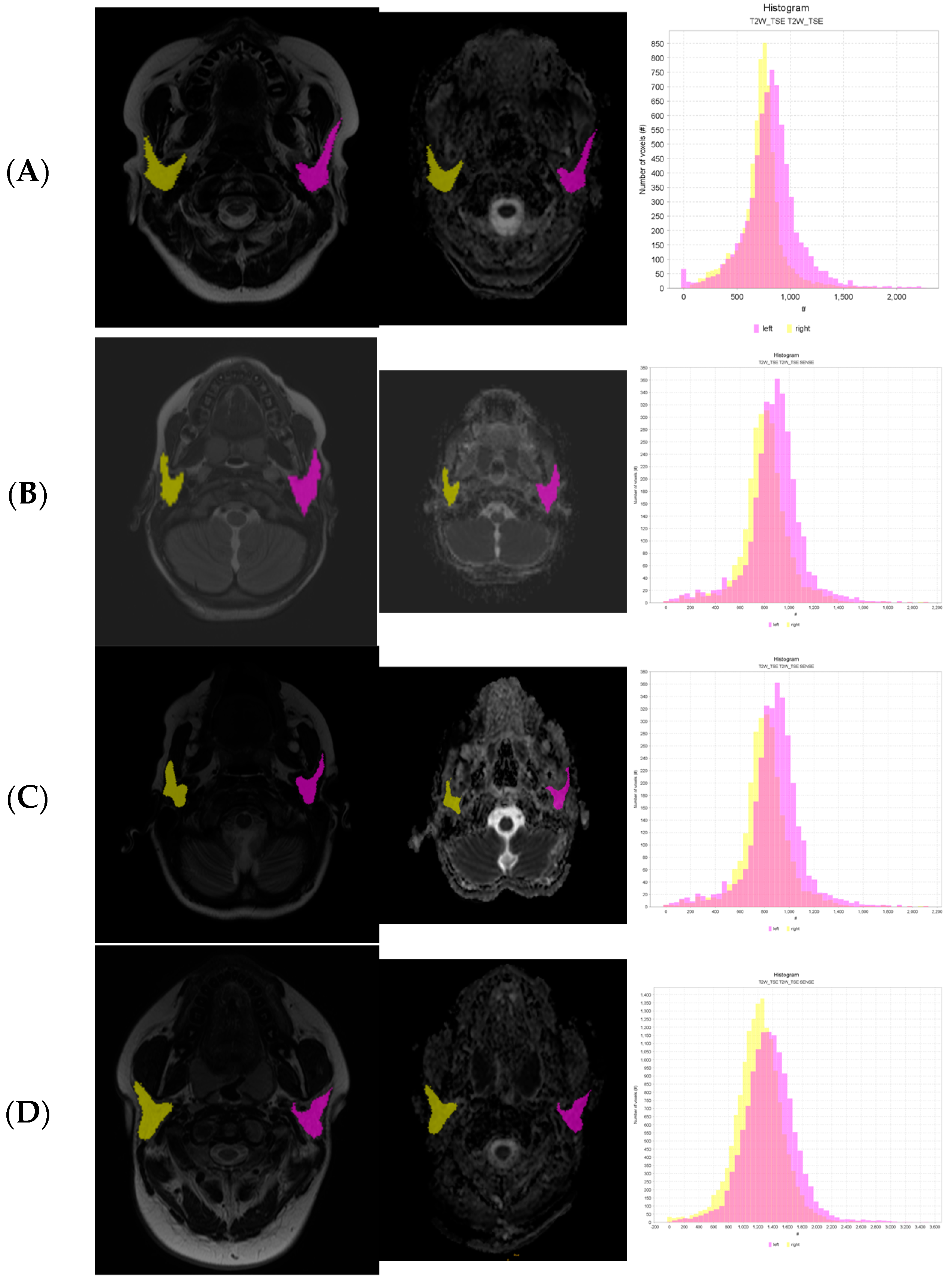
3.3. Whole-Volume ADC Image for Texture Analysis
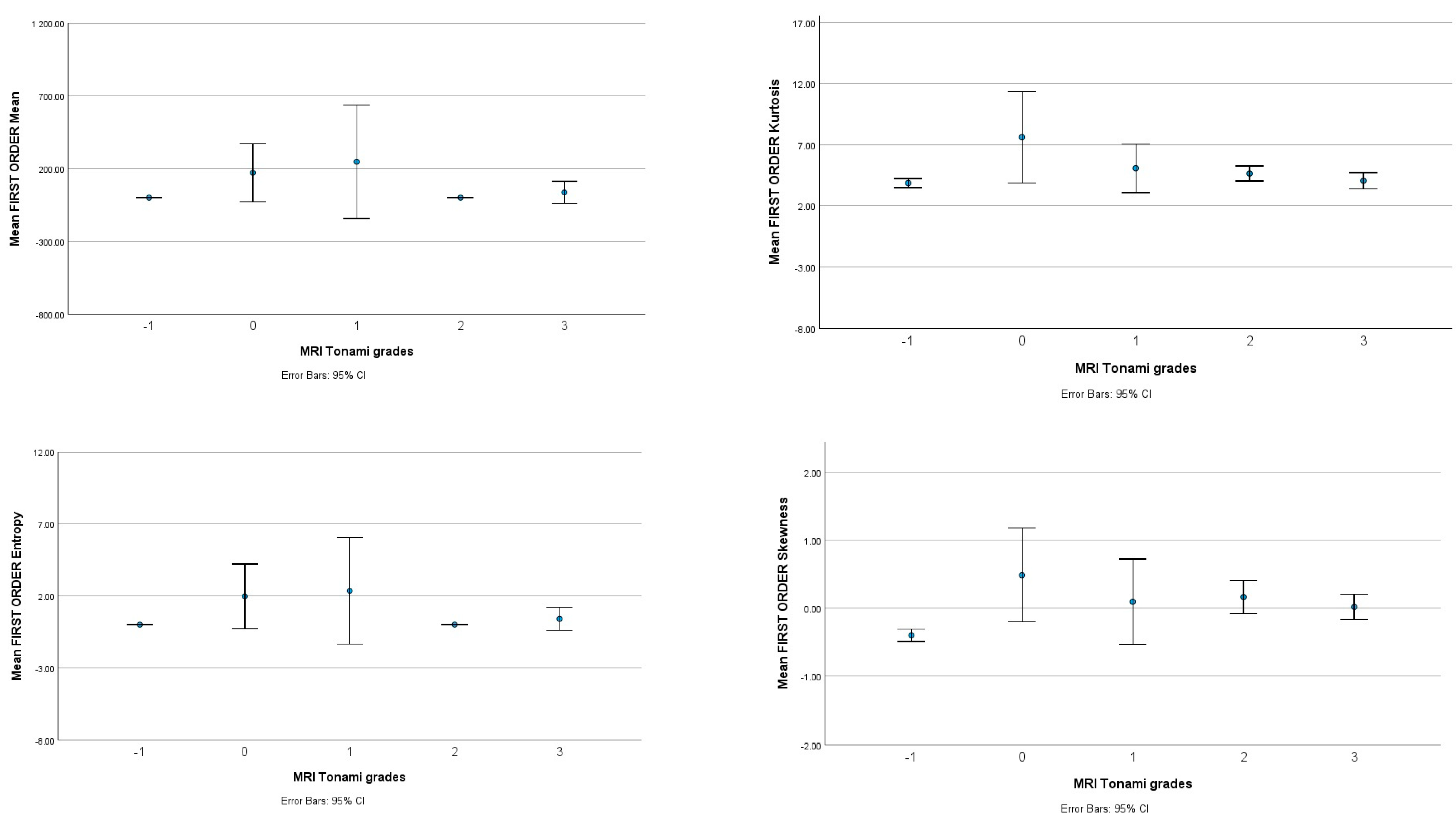
3.4. Whole-Volume T2 for Texture Analysis
4. Discussion
5. Conclusions
- Early diagnosis of Sjögren’s Syndrome (grade 1): One of the most significant implications of this study is the prospect of early diagnosis of Sjögren’s Syndrome, especially in children. This is crucial because Sjögren’s Syndrome is known for its nonspecific symptoms in the early stage of inflammation. Using MRI-based texture analysis, we can detect subtle changes at a microstructural level within parotid glands, which allows us to identify Sjögren’s Syndrome in the early stages. This can lead to prompt intervention and a better prognosis for young patients.
- Monitoring of remodeling salivary glands in the process of Sjögren’s Syndrome: Because Sjögren’s Syndrome is characterized by the progressive remodeling and destruction of the salivary glands, texture analysis can be a valuable tool for monitoring these changes over time by quantifying the heterogeneity and eventual microstructural changes in the glands. Our study suggests that we can track the disease’s progression and possible impact on the glandular tissue. This information will significantly impact the individual treatment strategy and therapeutic intervention.
- Reducing radiation exposure: Traditional diagnostics like sialography and scintigraphy can be replaced by magnetic resonance imaging only. This can be a safer approach for the pediatric population.
- Treatment planning can be more individualized: The ability to assess microstructures through textural analysis can be essential for better understanding the characteristics of each patient’s condition.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stefanski, A.-L.; Tomiak, C.; Pleyer, U.; Dietrich, T.; Burmester, G.R.; Dörner, T. The Diagnosis and Treatment of Sjögren’s Syndrome. Dtsch. Ärzteblatt Int. 2017, 114, 354. [Google Scholar] [CrossRef]
- Shiboski, C.H.; Shiboski, S.C.; Seror, R.; Criswell, L.A.; Labetoulle, M.; Lietman, T.M.; Rasmussen, A.; Scofield, H.; Vitali, C.; Bowman, S.J.; et al. 2016 American College of Rheumatology/European League Against Rheumatism Classification Criteria for Primary Sjögren’s Syndrome: A Consensus and Data-Driven Methodology Involving Three International Patient Cohorts. Arthritis. Rheumatol. 2017, 69, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Jonsson, M.V.; Baldini, C. Major Salivary Gland Ultrasonography in the Diagnosis of Sjögren’s Syndrome: A Place in the Diagnostic Criteria? Rheum. Dis. Clin. N. Am. 2016, 42, 501–517. [Google Scholar]
- Pomorska, A.; Świętoń, D.; Lieberman, S.M.; Bryl, E.; Kosiak, W.; Pęksa, R.; Chorążewicz, J.; Kochańska, B.; Kowalska-Skabara, J.; Szumera, M.; et al. Recurrent or persistent salivary gland enlargement in children: When is it Sjögren’s? Semin. Arthritis Rheum. 2022, 52, 151945. [Google Scholar] [CrossRef] [PubMed]
- Świecka, M.; Maślińska, M.; Paluch, Ł.; Zakrzewski, J.; Kwiatkowska, B. Imaging methods in primary Sjögren’s Syndrome as potential tools of disease diagnostics and monitoring. Reumatologia/Rheumatology 2019, 57, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Buus, S.; Grau, C.; Munk, O.L.; Bender, D.; Jensen, K.; Keiding, S. 11C-methionine PET, a novel method for measuring regional salivary gland function after radiotherapy of head and neck cancer. Radiother. Oncol. 2004, 73, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Takashima, S.; Takeuchi, N.; Morimoto, S.; Tomiyama, N.; Ikezoe, J.; Shogen, K.; Kozuka, T.; Okumura, T. MR Imaging of Sjögren Syndrome. J. Comput. Assist. Tomogr. 1991, 15, 393–400. [Google Scholar] [CrossRef]
- Chu, C.; Feng, Q.; Zhang, H.; Zhu, Y.; Chen, W.; He, J.; Sun, L.; Zhou, Z. Whole-Volume ADC Histogram Analysis in Parotid Glands to Identify Patients with Sjögren’s Syndrome. Sci. Rep. 2019, 9, 9614. [Google Scholar] [CrossRef]
- Chu, C.; Wang, F.; Zhang, H.; Zhu, Y.; Wang, C.; Chen, W.; He, J.; Sun, L.; Zhou, Z. Whole-volume ADC Histogram and Texture Analyses of Parotid Glands as an Image Biomarker in Evaluating Disease Activity of Primary Sjögren’s Syndrome. Sci. Rep. 2018, 8, 15387. [Google Scholar] [CrossRef]
- Ganeshan, B.; Skogen, K.; Pressney, I.; Coutroubis, D.; Miles, K. Tumour heterogeneity in oesophageal cancer assessed by CT texture analysis: Preliminary evidence of an association with tumour metabolism, stage, and survival. Clin. Radiol. 2012, 67, 157–164. [Google Scholar] [CrossRef]
- Chen, P.; Dong, B.; Zhang, C.; Tao, X.; Wang, P.; Zhu, L. The histogram analysis of apparent diffusion coefficient in differential diagnosis of parotid tumor. Dentomaxillofacial. Radiol. 2020, 49, 20190420. [Google Scholar] [CrossRef]
- Tonami, H.; Higashi, K.; Matoba, M.; Yokota, H.; Yamamoto, I.; Sugai, S. A Comparative Study Between MR Sialography and Salivary Gland Scintigraphy in the Diagnosis of Sjögren Syndrome. J. Comput. Assist. Tomogr. 2001, 25, 262–268. [Google Scholar] [CrossRef]
- Tustison, N.J.; Avants, B.B.; Cook, P.A.; Zheng, Y.; Egan, A.; Yushkevich, P.A.; Gee, J.C. N4ITK: Improved N3 bias correction. IEEE Trans. Med. Imaging 2010, 29, 1310e20. [Google Scholar] [CrossRef] [PubMed]
- Pyradiomics Organization. Pyradiomics Documentation. 2019. Available online: https://pyradiomics.readthedocs.io/en/latest/ (accessed on 1 April 2023).
- Castellano, G.; Bonilha, L.; Li, L.M.; Cendes, F. Texture analysis of medical images. Clin. Radiol. 2004, 59, 1061e9. [Google Scholar] [CrossRef] [PubMed]
- Kalk, W.W.; Vissink, A.; Spijkervet, F.K.; Bootsma, H.; Kallenberg, C.G.; Roodenburg, J.L. Parotid sialography for diagnosing Sjögren syndrome. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2002, 94, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Ng, F.; Ganeshan, B.; Kozarski, R.; Miles, K.A.; Goh, V. Assessment of primary colorectal cancer heterogeneity by using whole-tumor texture analysis: Contrast-enhanced CT texture as a biomarker of 5-year survival. Radiology 2013, 266, 177–184. [Google Scholar] [CrossRef]
- Márton, K.; Boros, I.; Fejérdy, P.; Madléna, M. Evaluation of unstimulated flow rates of whole and palatal saliva in healthy patients wearing complete dentures and in patients with Sjogren’s Syndrome. J. Prosthet. Dent. 2004, 91, 577–581. [Google Scholar] [CrossRef]
- Tzioufas, A.G.; Moutsopoulos, H.M. Salivary gland imaging techniques for the diagnosis of Sjögren’s Syndrome. Int. J. Clin. Rheumtol. 2009, 4, 321–327. [Google Scholar] [CrossRef]
- Makanyanga, J.; Ganeshan, B.; Rodriguez-Justo, M.; Bhatnagar, G.; Groves, A.; Halligan, S.; Miles, K.; Taylor, S.A. MRI texture analysis (MRTA) of T2-weighted images in Crohn’s disease may provide information on histological and MRI disease activity in patients undergoing ileal resection. Eur. Radiol. 2017, 27, 589. [Google Scholar] [CrossRef]
- de Figueiredo, E.H.; Borgonovi, A.F.; Doring, T.M. Basic Concepts of MR Imaging, Diffusion MR Imaging, and Diffusion Tensor Imaging. Magn. Reason. Imaging Clin. N. Am. 2011, 19, 1–22. [Google Scholar] [CrossRef]
- Cohen, J.; Cohen, P.; West, S.G.; Aiken, L.S. Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences, 3rd ed.; Lawrence Erlbaum Associates, Inc.: Mahwah, NJ, USA, 2003. [Google Scholar]
- Cho, S.H.; Kim, G.C.; Jang, Y.-J.; Ryeom, H.; Kim, H.J.; Shin, K.-M.; Park, J.S.; Choi, G.-S.; Kim, S.H. Locally advanced rectal cancer: Post-chemoradiotherapy ADC histogram analysis for predicting a complete response. Acta Radiol. 2015, 56, 1042–1050. [Google Scholar] [CrossRef]
- Zhong, W.; Zhang, H.; Ran, H. Advances in imaging of the lacrimal gland in Sjögren’s Syndrome: A narrative review. J. Clin. Ultrasound 2023, 1–10. [Google Scholar] [CrossRef]
- Muntean, D.D.; Bădărînză, M.; Ștefan, P.A.; Lenghel, M.L.; Rusu, G.M.; Csutak, C.; Coroian, P.A.; Lupean, R.A.; Fodor, D. The Diagnostic Value of MRI-Based Radiomic Analysis of Lacrimal Glands in Patients with Sjögren’s Syndrome. Int. J. Mol. Sci. 2022, 23, 10051. [Google Scholar] [CrossRef]
- Freni, F.; Gazia, F.; D’alcontres, F.S.; Galletti, B.; Galletti, F. Use of botulinum toxin in Frey’s syndrome. Clin. Case Rep. 2019, 7, 482–485. [Google Scholar] [CrossRef]
- Furness, S.; Bryan, G.; McMillan, R.; Worthington, H.V. Interventions for the Management of Dry Mouth: Non-Pharmacological Interventions. In Cochrane Database of Systematic Reviews; Furness, S., Ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2013. [Google Scholar]
- Hammenfors, D.S.; Valim, V.; Bica, B.E.R.G.; Pasoto, S.G.; Lilleby, V.; Nieto-González, J.C.; Silva, C.A.; Mossel, E.; Pereira, R.M.R.; Coelho, A.; et al. Juvenile Sjögren’s Syndrome: Clinical Characteristics with Focus on Salivary Gland Ultrasonography. Arthritis. Care Res. 2020, 72, 78–87. [Google Scholar] [CrossRef]
| Index | Value SS Group | Value Healthy Group | |
|---|---|---|---|
| Age | n.a.* | 12.5 ± 3.4 yrs | 13.5 ± 2.4 yrs |
| Gender | female | 20 | 8 |
| male | 16 | 12 | |
| Tonami scale | 0 | 12 | n.a. |
| 1 | 8 | n.a. | |
| 2 | 30 | n.a. | |
| 3 | 22 | n.a. |
| Sequence | FOV (mm) | Slice Thickness/Gap (mm) | Voxel (mm) | Suppress Fat | Flip Angle | Number of Averages | TE/TR (ms) | Matrix | Plane |
|---|---|---|---|---|---|---|---|---|---|
| Survey/localizer | 250/250 | 10 | 0.98 × 1.95 × 10 | - | 15 | 1 | 4.6/11 | 256 | Coronal, transverse, sagittal |
| T2_TSE | 210/210 | 3/0.5 | 0.80 × 1.15 × 3 | - | 90 | 2 | 90/2500 | 512 | Coronal |
| T2_TSE | 240/240 | 3/0.6 | 0.70 × 0.87 × 3 | - | 90 | 2 | 90/3000–4500 | 640 | Transverse |
| T2_STIR | 210/210 | 3/0.6 | 0.78 × 0.98 × 3 | STIR | - | 2 | 90/1400–4000 | 560 | Transverse |
| 3D_TSE_SPIR_obligue | 300/245/48 | 2 | 1 × 1.24 × 2 | SPIR | 90 | 2 | 90/120 | 1008 | Sagittal |
| mDIXON | 250/250/130 | 1 | 1 × 1 × 2 | - | 10 | 3 | Shortest/shortest | 256 | Transverse |
| DWI | 240/240 | 4.5/1 | 1.5 × 2.18 × 4.5 | SPIR | 90 | 1 | Shortest/shortest | 288 | Transverse |
| Texture Parameters | Tonami Scale | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Healthy | 0 | 1 | 2 | 3 | ||||||
| Mean | Std. Deviation | Mean | Std. Deviation | Mean | Std. Deviation | Mean | Std. Deviation | Mean | Std. Deviation | |
| Median | 891.53 | 244.23 | 698.58 | 252.43 | 890.44 | 481.32 | 849.78 | 344.92 | 897.32 | 300.99 |
| Entropy | 7.51 | 1.76 | 8.21 | 0.44 | 8.48 | 0.49 | 8.49 | 0.69 | 8.72 | 0.70 |
| Kurtosis | 4.79 | 1.57 | 7.33 | 3.58 | 4.89 | 0.68 | 6.02 | 1.56 | 5.24 | 1.78 |
| Mean | 887.56 | 242.88 | 697.16 | 246.50 | 880.58 | 451.04 | 850.80 | 345.87 | 911.03 | 303.55 |
| GLDM_Dependence NonUniformity | 5791 | 3201 | 13,600 | 669 | 11,600 | 2390 | 13,400 | 7720 | 14,200 | 6530 |
| GLDM_Small Dependence High Gray Level Emphasis | 95,569 | 563,232 | 115,000 | 887,000 | 203,000 | 202,000 | 191,000 | 162,000 | 209,000 | 144,000 |
| GLCM_Imc1 | −0.32 | 0.09 | −0.27 | 0.06 | −0.31 | 0.07 | −0.32 | 0.08 | −0.34 | 0.06 |
| GLRLM_Run Entropy | 7.67 | 1.21 | 8.26 | 0.43 | 8.53 | 0.48 | 8.53 | 0.67 | 8.76 | 0.68 |
| GLSZM_Zone Entropy | 8.11 | 1.19 | 8.69 | 0.38 | 8.89 | 0.37 | 8.92 | 0.54 | 9.07 | 0.58 |
| Sample 1–Sample 2 | Test Statistic | Std. Error | Std. Test Statistic | Sig. | Adj. Sig. a |
|---|---|---|---|---|---|
| 1–3 | −39.756 | 14.033 | −2.833 | 0.005 | 0.046 |
| 1–healthy | 46.178 | 13.180 | 3.504 | <0.001 | 0.005 |
| 0–3 | −33.905 | 11.605 | −2.922 | 0.003 | 0.035 |
| 0–healthy | 40.327 | 10.558 | 3.820 | <0.001 | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grzywińska, M.; Karwecka, M.; Pomorska, A.; Irga-Jaworska, N.; Świętoń, D. Textural Analysis of Magnetic Resonance Images as an Additional Evaluation Tool of Parotid Glands in Sjögren—Primarily Findings. Biomedicines 2023, 11, 3132. https://doi.org/10.3390/biomedicines11123132
Grzywińska M, Karwecka M, Pomorska A, Irga-Jaworska N, Świętoń D. Textural Analysis of Magnetic Resonance Images as an Additional Evaluation Tool of Parotid Glands in Sjögren—Primarily Findings. Biomedicines. 2023; 11(12):3132. https://doi.org/10.3390/biomedicines11123132
Chicago/Turabian StyleGrzywińska, Małgorzata, Magdalena Karwecka, Anna Pomorska, Ninela Irga-Jaworska, and Dominik Świętoń. 2023. "Textural Analysis of Magnetic Resonance Images as an Additional Evaluation Tool of Parotid Glands in Sjögren—Primarily Findings" Biomedicines 11, no. 12: 3132. https://doi.org/10.3390/biomedicines11123132