
Developing Models to Predict BRAFV600E and RAS Mutational Status in Papillary Thyroid Carcinoma Using Clinicopathological Features and pERK1/2 Immunohistochemistry Expression
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
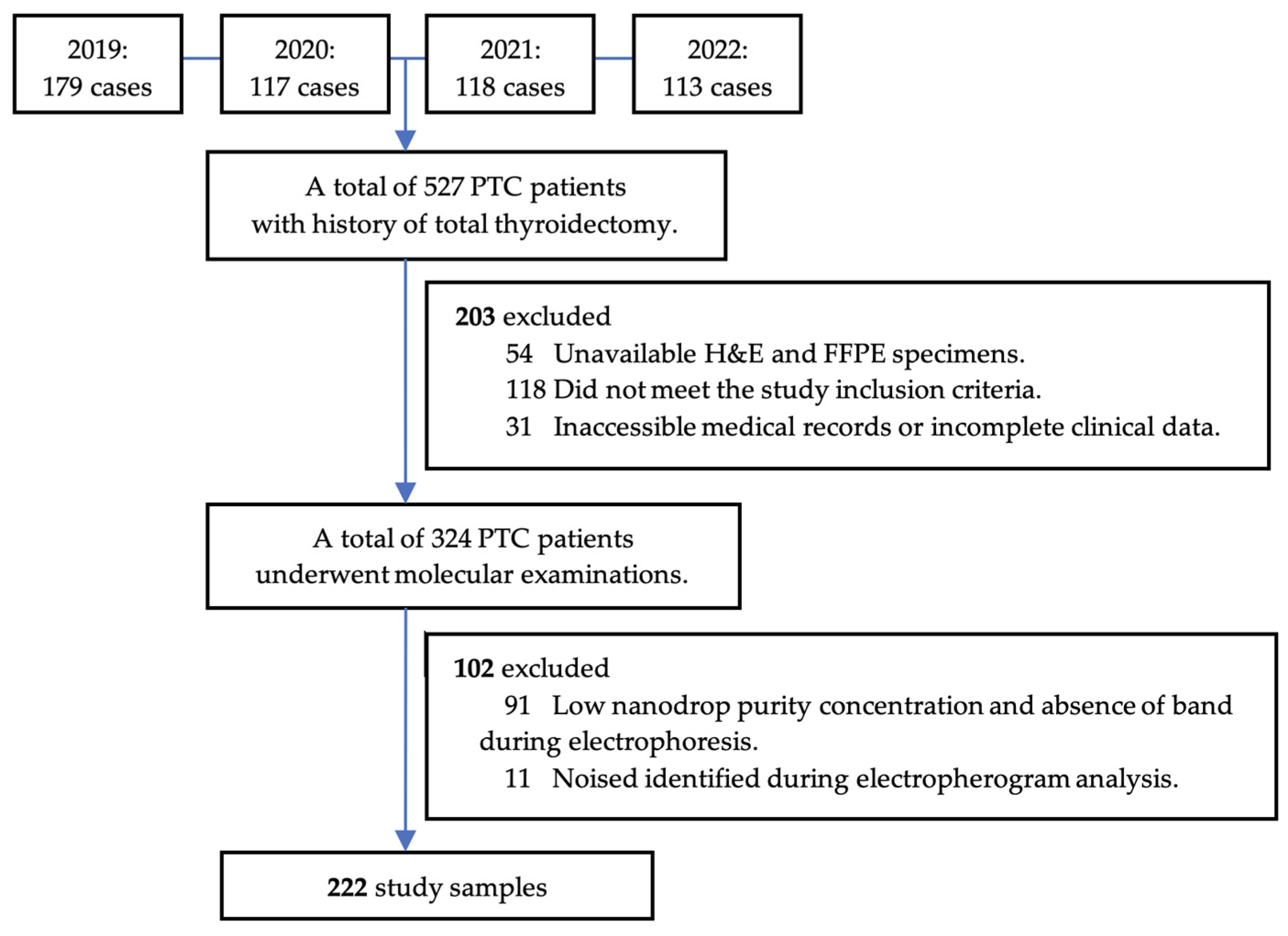
2.2. Study Design and Population
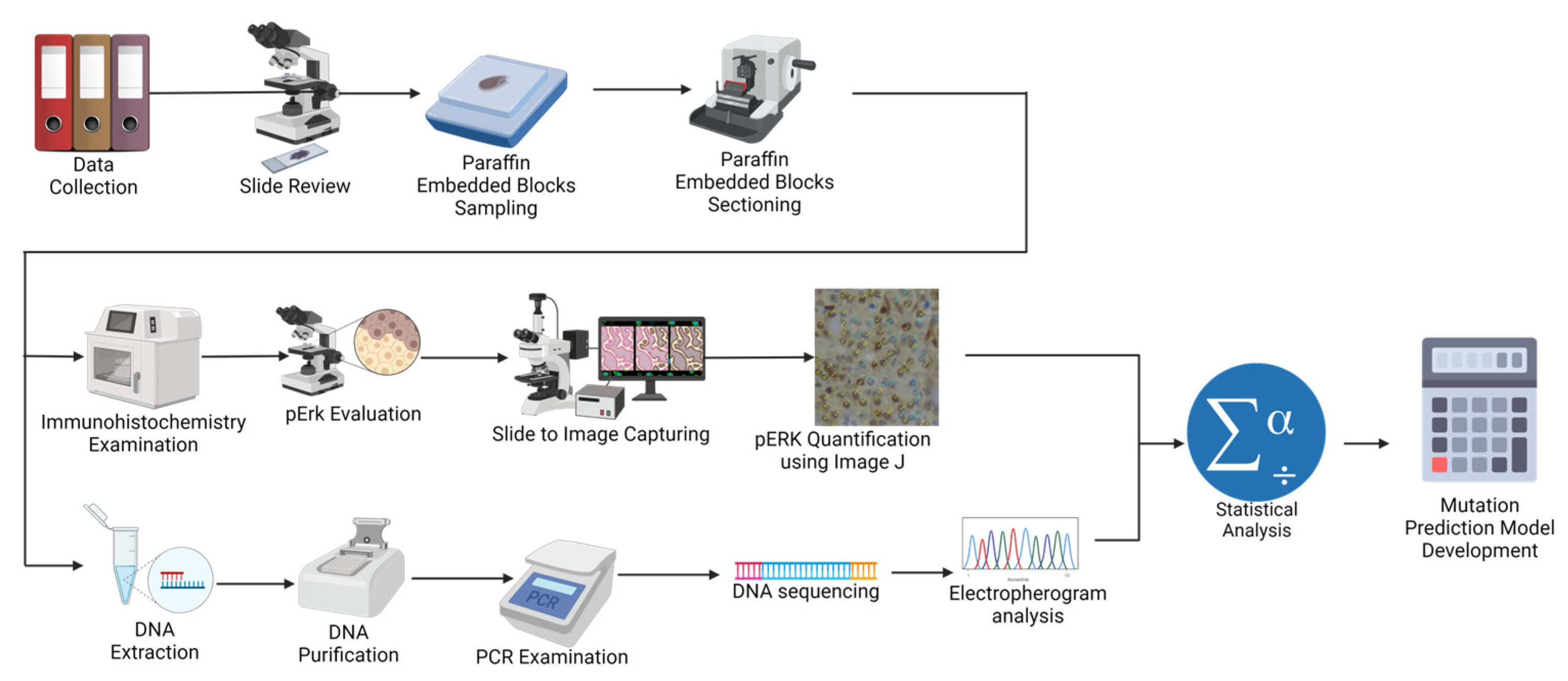
2.3. pERK1/2 Immunohistochemistry Examination
2.4. Mutational Analysis
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Bivariate Analysis: Correlation between Clinico-Histopathology Characteristics with BRAFV600E and RAS Mutational Status
3.3. Multivariate Analysis: Establishing the BRAFV600E Prediction Model
3.4. Multivariate Analysis: Establishing the RAS Mutation Prediction Model
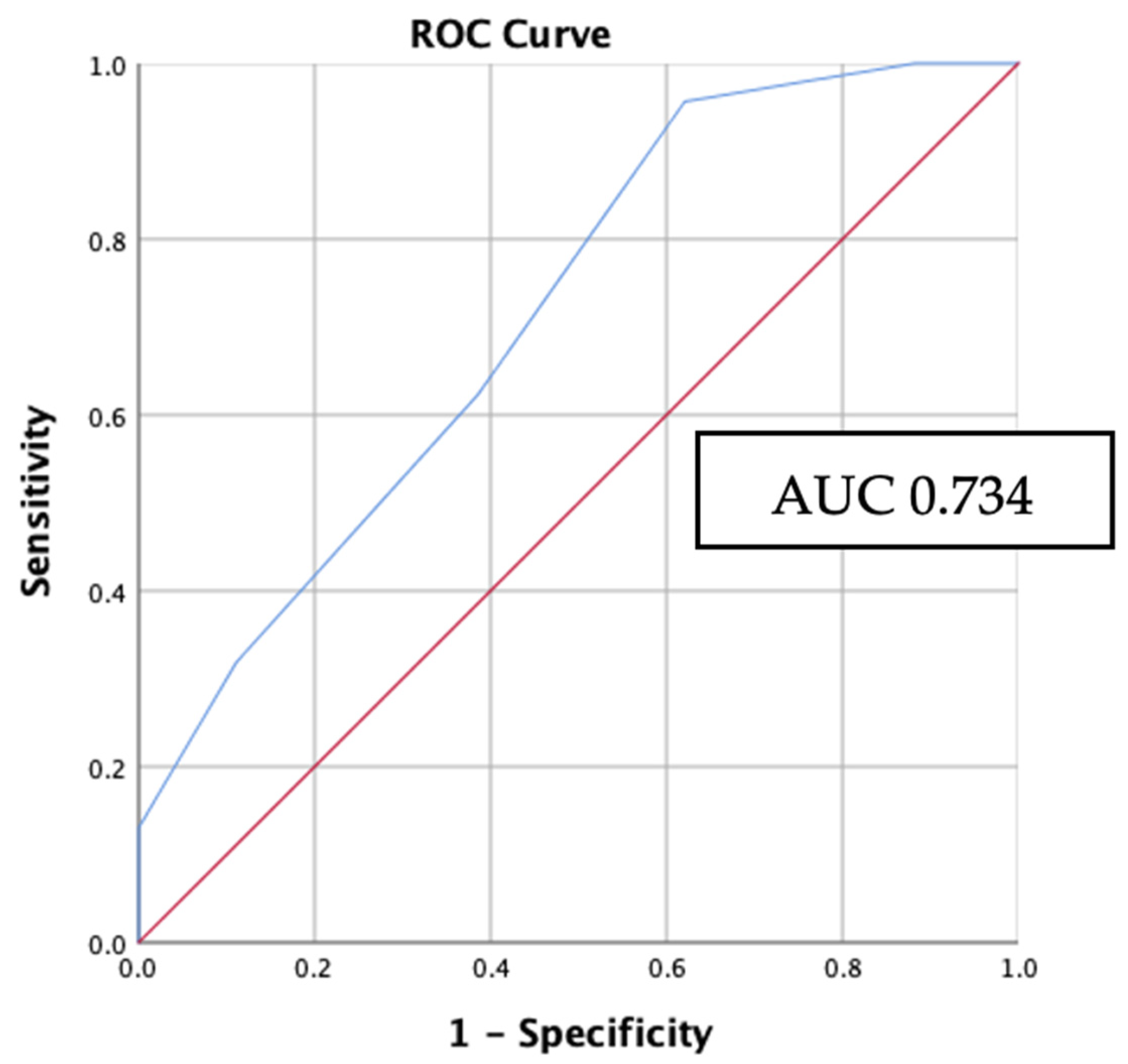
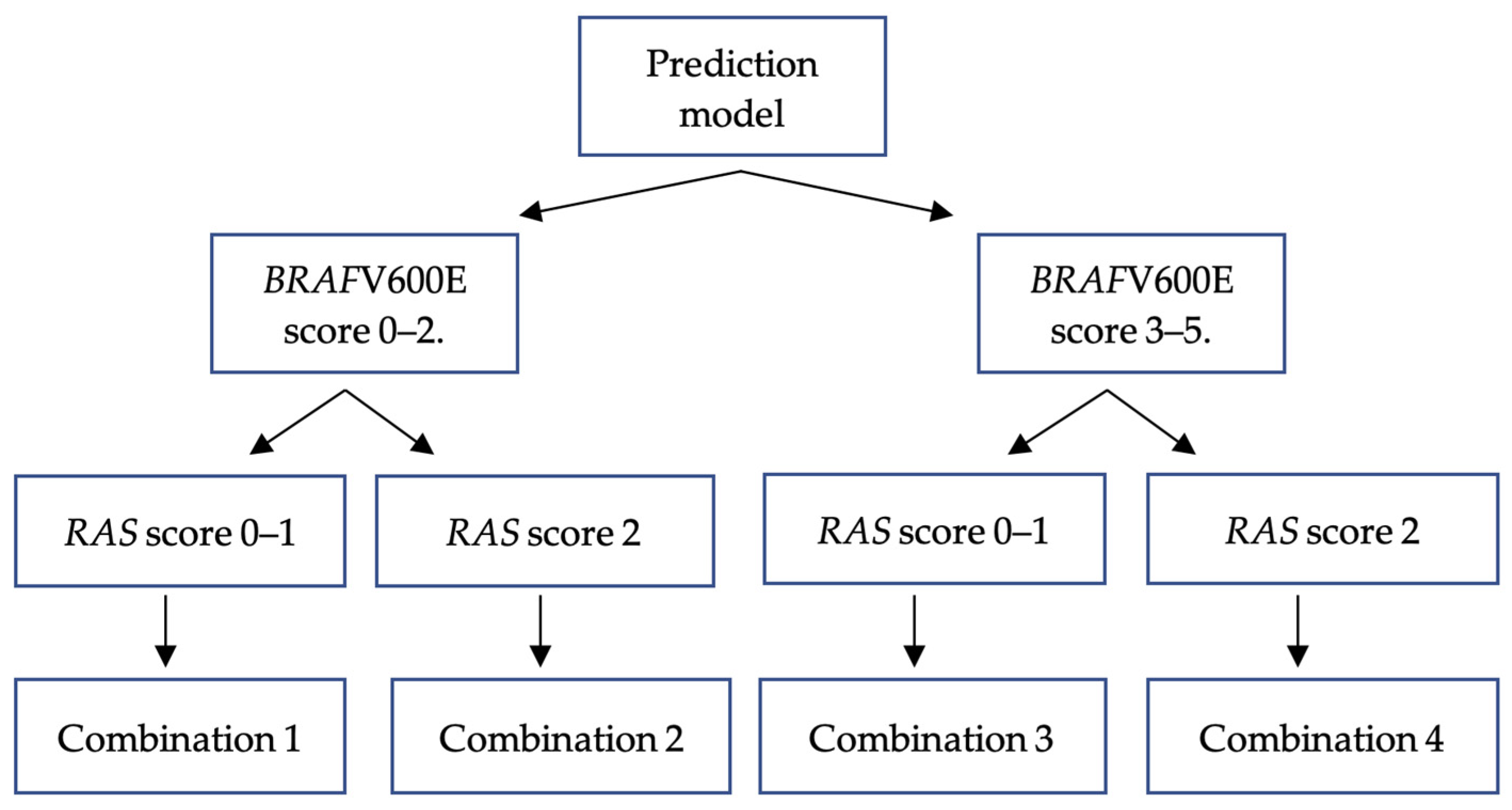
3.5. Internal Validation: Applying BRAFV600E and RAS Mutation Prediction Model to Study Samples
3.6. Correlation between Combination Groups with Clinical Endpoint of PTC
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nuclear Features (1 Point Each) | Criteria |
|---|---|
| 1. Size and shape | Enlargement, elongation, crowding, overlapping |
| 2. Membrane irregularities | Irregular contours, grooves, folds, intranuclear cytoplasmic inclusions |
| 3. Chromatin features | Chromatin clearing, margination to nuclear membranes, glassy nuclei |
| Score | 0: Absent or only slightly expressed 1: Present or well developed |
| PTC nuclear score: | 0 or 1: Not diagnostic 2 or 3: Diagnostic of PTC nuclei |
References
- Olson, E.; Wintheiser, G.; Wolfe, K.M.; Droessler, J.; Silberstein, P.T. Epidemiology of Thyroid Cancer: A Review of the National Cancer Database, 2000–2013. Cureus 2019, 11, e4127. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, N.; Akbani, R.; Aksoy, B.A.; Ally, A.; Arachchi, H.; Asa, S.L.; Auman, J.T.; Balasundaram, M.; Balu, S.; Baylin, S.B.; et al. Integrated Genomic Characterization of Papillary Thyroid Carcinoma. Cell 2014, 159, 676–690. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.K.; Little, M.P.; Lubin, J.H.; Brenner, A.V.; Wells, S.A.; Sigurdson, A.J.; Nikiforov, Y.E. The Increase in Thyroid Cancer Incidence during the Last Four Decades Is Accompanied by a High Frequency of BRAF Mutations and a Sharp Increase in RAS Mutations. J. Clin. Endocrinol. Metab. 2014, 99, E276–E285. [Google Scholar] [CrossRef] [PubMed]
- Xing, M. BRAF Mutation in Thyroid Cancer. Endocr. Relat. Cancer 2005, 12, 245–262. [Google Scholar] [CrossRef]
- Xie, H.; Wei, B.; Shen, H.; Gao, Y.; Wang, L.; Liu, H. BRAF Mutation in Papillary Thyroid Carcinoma (PTC) and Its Association with Clinicopathological Features and Systemic Inflammation Response Index (SIRI). Am. J. Transl. Res. 2018, 10, 2726–2736. [Google Scholar]
- Brehar, A.C.; Brehar, F.M.; Bulgar, A.C.; Dumitrache, C. Genetic and Epigenetic Alterations in Differentiated Thyroid Carcinoma. J. Med. Life 2013, 6, 403–408. [Google Scholar]
- Marotta, V.; Bifulco, M.; Vitale, M. Significance of RAS Mutations in Thyroid Benign Nodules and Non-Medullary Thyroid Cancer. Cancers 2021, 13, 3785. [Google Scholar] [CrossRef]
- Soares, P.; Trovisco, V.; Rocha, A.S.; Lima, J.; Castro, P.; Preto, A.; Máximo, V.; Botelho, T.; Seruca, R.; Sobrinho-Simões, M. BRAF Mutations and RET/PTC Rearrangements Are Alternative Events in the Etiopathogenesis of PTC. Oncogene 2003, 22, 4578–4580. [Google Scholar] [CrossRef]
- Wang, P.; Han, L.; Yu, M.; Cao, Z.; Li, X.; Shao, Y.; Zhu, G. The Prognostic Value of PERK in Cancer and Its Relationship with Immune Cell Infiltration. Front. Mol. Biosci. 2021, 8, 648752. [Google Scholar] [CrossRef]
- Wan, P.T.C.; Garnett, M.J.; Roe, S.M.; Lee, S.; Niculescu-Duvaz, D.; Good, V.M.; Jones, C.M.; Marshall, C.J.; Springer, C.J.; Barford, D.; et al. Cancer Genome Project. Mechanism of Activation of the RAF-ERK Signaling Pathway by Oncogenic Mutations of B-RAF. Cell 2004, 116, 855–867. [Google Scholar] [CrossRef]
- Cao, Y.-M.; Zhang, T.-T.; Li, B.-Y.; Qu, N.; Zhu, Y.-X. Prognostic Evaluation Model for Papillary Thyroid Cancer: A Retrospective Study of 660 Cases. Gland Surg. 2021, 10, 2170–2179. [Google Scholar] [CrossRef] [PubMed]
- Xing, M.; Alzahrani, A.S.; Carson, K.A.; Viola, D.; Elisei, R.; Bendlova, B.; Yip, L.; Mian, C.; Vianello, F.; Tuttle, R.M.; et al. Association between BRAF V600E Mutation and Mortality in Patients with Papillary Thyroid Cancer. JAMA 2013, 309, 1493–1501. [Google Scholar] [CrossRef] [PubMed]
- WHO Classification of Tumours Editorial Board. Endocrine and Neuroendocrine Tumours; International Agency for Research on Cancer: Lyon, France; Available online: https://tumourclassification.iarc.who.int/chapters/53 (accessed on 24 January 2023).
- Li, C.; Lee, K.C.; Schneider, E.B.; Zeiger, M.A. BRAF V600E Mutation and Its Association with Clinicopathological Features of Papillary Thyroid Cancer: A Meta-Analysis. J. Clin. Endocrinol. Metab. 2012, 97, 4559–4570. [Google Scholar] [CrossRef] [PubMed]
- Adeniran, A.J.; Zhu, Z.; Gandhi, M.; Steward, D.L.; Fidler, J.P.; Giordano, T.J.; Biddinger, P.W.; Nikiforov, Y.E. Correlation between Genetic Alterations and Microscopic Features, Clinical Manifestations, and Prognostic Characteristics of Thyroid Papillary Carcinomas. Am. J. Surg. Pathol. 2006, 30, 216–222. [Google Scholar] [CrossRef]
- Jung, C.K.; Bychkov, A.; Song, D.E.; Kim, J.H.; Zhu, Y.; Liu, Z.; Keelawat, S.; Lai, C.R.; Hirokawa, M.; Kameyama, K.; et al. Molecular Correlates and Nuclear Features of Encapsulated Follicular-Patterned Thyroid Neoplasms. Endocrinol. Metab. 2021, 36, 123–133. [Google Scholar] [CrossRef]
- Rivera, M.; Ricarte-Filho, J.; Knauf, J.; Shaha, A.; Tuttle, M.; Fagin, J.A.; Ghossein, R.A. Molecular Genotyping of Papillary Thyroid Carcinoma Follicular Variant According to Its Histological Subtypes (Encapsulated vs Infiltrative) Reveals Distinct BRAF and RAS Mutation Patterns. Mod. Pathol. 2010, 23, 1191–1200. [Google Scholar] [CrossRef]
- Schulten, H.-J.; Salama, S.; Al-Ahmadi, A.; Al-Mansouri, Z.; Mirza, Z.; Al-Ghamdi, K.; Al-Hamour, O.A.; Huwait, E.; Gari, M.; Al-Qahtani, M.H.; et al. Comprehensive Survey of HRAS, KRAS, and NRAS Mutations in Proliferative Thyroid Lesions from an Ethnically Diverse Population. Anticancer Res. 2013, 33, 4779–4784. [Google Scholar]
- Hara, H.; Fulton, N.; Yashiro, T.; Ito, K.; DeGroot, L.J.; Kaplan, E.L. N-Ras Mutation: An Independent Prognostic Factor for Aggressiveness of Papillary Thyroid Carcinoma. Surgery 1994, 116, 1010–1016. [Google Scholar]
- Odate, T.; Oishi, N.; Vuong, H.G.; Mochizuki, K.; Kondo, T. Genetic Differences in Follicular Thyroid Carcinoma between Asian and Western Countries: A Systematic Review. Gland Surg. 2020, 9, 1813–1826. [Google Scholar] [CrossRef]
- Gomes, C.C.; Gayden, T.; Bajic, A.; Harraz, O.F.; Pratt, J.; Nikbakht, H.; Bareke, E.; Diniz, M.G.; Castro, W.H.; St-Onge, P.; et al. TRPV4 and KRAS and FGFR1 Gain-of-Function Mutations Drive Giant Cell Lesions of the Jaw. Nat. Commun. 2018, 9, 4572. [Google Scholar] [CrossRef]
- Harahap, A.S.; Subekti, I.; Panigoro, S.S.; Asmarinah; Lisnawati; Werdhani, R.A.; Agustina, H.; Khoirunnisa, D.; Mutmainnah, M.; Salinah; et al. Profile of BRAFV600E, BRAFK601E, NRAS, HRAS, and KRAS Mutational Status, and Clinicopathological Characteristics of Papillary Thyroid Carcinoma in Indonesian National Referral Hospital. Appl. Clin. Genet. 2023, 16, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Yip, L.; Nikiforova, M.N.; Yoo, J.Y.; McCoy, K.L.; Stang, M.T.; Armstrong, M.J.; Nicholson, K.J.; Ohori, N.P.; Coyne, C.; Hodak, S.P.; et al. Tumor Genotype Determines Phenotype and Disease-Related Outcomes in Thyroid Cancer: A Study of 1510 Patients. Ann. Surg. 2015, 262, 519–525; discussion 524–525. [Google Scholar] [CrossRef] [PubMed]
- Maik-Rachline, G.; Hacohen-Lev-Ran, A.; Seger, R. Nuclear ERK: Mechanism of Translocation, Substrates, and Role in Cancer. Int. J. Mol. Sci. 2019, 20, 1194. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.W.; Mendoza, R.A.; Aman, S.; Hsu, R.; Liu, L. Thyroid Cancer Incidence Disparities among Ethnic Asian American Populations, 1990–2014. Ann. Epidemiol. 2022, 66, 28–36. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef]
- Pessôa-Pereira, D.; Medeiros, M.F.d.S.; Lima, V.M.S.; Silva, J.C.d.; Cerqueira, T.L.d.O.; Silva, I.C.d.; Fonseca, L.E.; Sampaio, L.J.L.; Lima, C.R.A.d.; Ramos, H.E. Association between BRAF (V600E) Mutation and Clinicopathological Features of Papillary Thyroid Carcinoma: A Brazilian Single-Centre Case Series. Arch. Endocrinol. Metab. 2019, 63, 97–106. [Google Scholar] [CrossRef]
- Silver, J.A.; Bogatchenko, M.; Pusztaszeri, M.; Forest, V.-I.; Hier, M.P.; Yang, J.W.; Tamilia, M.; Payne, R.J. BRAF V600E Mutation Is Associated with Aggressive Features in Papillary Thyroid Carcinomas ≤ 1.5 cm. J. Otolaryngol.—Head Neck Surg. 2021, 50, 63. [Google Scholar] [CrossRef]
- Thompson, L.D.R.; Poller, D.N.; Kakudo, K.; Burchette, R.; Nikiforov, Y.E.; Seethala, R.R. An International Interobserver Variability Reporting of the Nuclear Scoring Criteria to Diagnose Noninvasive Follicular Thyroid Neoplasm with Papillary-Like Nuclear Features: A Validation Study. Endocr. Pathol. 2018, 29, 242–249. [Google Scholar] [CrossRef]







| Characteristics | BRAFV600E N = 64 (%) | Control N = 116 (%) | p | OR | 95% CI |
|---|---|---|---|---|---|
| Clinical features | |||||
| Age (years) | |||||
| ≥55 | 17 (35.4) | 31 (64.4) | 0.981 a | 0.992 | 0.497–1.978 |
| <55 | 47 (35.6) | 85 (64.4) | 1.000 | Reference | |
| Gender | |||||
| Man | 18 (36.0) | 32 (64.0) | 0.938 a | 1.027 | 0.520–2.028 |
| Woman | 46 (35.4) | 84 (64.6) | 1.000 | Reference | |
| Clinical stage | |||||
| Clinical stage IV | 7 (58.3) | 5 (41.7) | 0.114 b | 2.930 | 0.879–9.766 |
| Clinical stage III | 1 (20) | 4 (80) | 0.523 | 0.057–4.824 | |
| Clinical stage II | 13 (43.3) | 17 (56.7) | 1.601 | 0.713–3.592 | |
| Clinical stage I | 43 (32.3) | 90 (67.7) | 1.000 | Reference | |
| Stage group | |||||
| Late stage (III–IV) | 8 (47.1) | 9 (52.9) | 0.298 a | 1.698 | 0.621–4.643 |
| Early stage (I–II) | 56 (34.4) | 107 (65.6) | 1.000 | Reference | |
| Histopathology features | |||||
| Tumor size (cm) | |||||
| ≥4 | 16 (34.8) | 30 (64.2) | 0.899 a | 0.956 | 0.474–1.928 |
| <4 | 48 (35.8) | 86 (65.2) | 1.000 | Reference | |
| Nuclear score | |||||
| 3 | 56 (43.4) | 73 (56.6) | <0.001 a | 4.123 | 1.796–9.466 |
| 2 | 8 (15.7) | 43 (84.3) | 1.000 | Reference | |
| Capsule | |||||
| Absent | 52 (44.1) | 66 (55.9) | <0.001 a | 3.283 | 1.586–6.794 |
| Present | 12 (19.4) | 50 (80.6) | 1.000 | Reference | |
| Histology subtype | |||||
| Solid | 2 (33.3) | 4 (66.7) | <0.001 b | 2.938 | 0.459–18.786 |
| Oncocytic | 1 (10) | 9 (90) | 0.653 | 0.072–5.878 | |
| Classic | 21 (37.5) | 35 (62.5) | 3.525 | 1.399–8.885 | |
| Tall cell | 32 (60.4) | 21 (39.6) | 8.952 | 3.532–22.690 | |
| Follicular | 8 (14.5) | 47 (85.5) | 1.000 | Reference | |
| Histology group | |||||
| Aggressive | 35 (50.7) | 34 (49.3) | <0.001 a | 2.911 | 1.544–5.488 |
| Non-aggressive | 29 (26.1) | 82 (73.9) | 1.000 | Reference | |
| Multifocality | |||||
| Present | 50 (35.7) | 90 (64.3) | 0.934 a | 1.032 | 0.494–2.154 |
| Absent | 14 (35.0) | 26 (65.0) | 1.000 | Reference | |
| Lymphovascular invasion | |||||
| Present | 31 (43.1) | 41 (56.9) | 0.086 a | 1.718 | 0.924–3.197 |
| Absent | 33 (30.6) | 75 (69.4) | 1.000 | Reference | |
| Extrathyroidal extension | |||||
| Present | 28 (49.1) | 29 (50.9) | 0.010 a | 2.333 | 1.220–4.463 |
| Absent | 36 (29.3) | 87 (70.7) | 1.000 | Reference | |
| Node metastases | |||||
| Present | 34 (47.2) | 38 (52.8) | 0.008 a | 2.326 | 1.244–4.349 |
| Absent | 30 (27.8) | 78 (72.2) | 1.000 | Reference | |
| pERK1/2 expression | |||||
| High (>10%) | 25 (51) | 24 (49) | 0.008 a | 2.457 | 1.253–4.820 |
| Low (<10%) | 39 (29.8) | 92 (70.2) | Reference |
| Characteristics | RAS Mutation N = 42 (%) | Control N = 116 (%) | p | OR | 95% CI |
|---|---|---|---|---|---|
| Clinical factors | |||||
| Age (years) | |||||
| <55 | 31 (26.7) | 85 (73.3) | 0.947 a | 1.028 | 0.461–2.291 |
| ≥55 | 11 (26.2) | 31 (73.8) | 1.000 | Reference | |
| Gender | |||||
| Woman | 32 (27.6) | 84 (72.4) | 0.635 a | 1.219 | 0.538–2.764 |
| Man | 10 (23.8) | 32 (76.2) | 1.000 | Reference | |
| Clinical stage | |||||
| Clinical stage I | 33 (26.8) | 90 (73.2) | 0.981 b | 0.458 | 0.116–1.811 |
| Clinical stage II | 5 (22.7) | 17 (77.3) | 0.368 | 0.071–1.915 | |
| Clinical stage III | 0 (0) | 4 (100) | 0.556 | 0.310–0.997 | |
| Clinical stage IV | 4 (44.4) | 5 (55.6) | 1.000 | Reference | |
| Stage group | |||||
| Early stage (I–II) | 38 (26.2) | 107 (73.8) | 0.721 a | 0.799 | 0.232–2.746 |
| Late stage (III–IV) | 4 (30.8) | 9 (69.2) | 1.000 | Reference | |
| Histopathology factors | |||||
| Tumor size (cm) | |||||
| <4 | 32 (27.1) | 86 (72.9) | 0.696 a | 1.116 | 0.490–2.541 |
| ≥4 | 10 (25.0) | 30 (75.0) | 1.000 | Reference | |
| Nuclear score | |||||
| 2 | 19 (30.6) | 43 (69.4) | 0.353 a | 1.402 | 0.686–2.867 |
| 3 | 23 (24.0) | 73 (76.0) | 1.000 | Reference | |
| Capsule | |||||
| Present | 22 (30.6) | 50 (69.4) | 0.302 a | 1.452 | 0.715–2.948 |
| Absent | 20 (23.3) | 66 (76.7) | 1.000 | Reference | |
| Histology subtype | |||||
| Follicular | 32 (40.5) | 47 (59.5) | <0.001 b | 2.648 | 1.121–6.253 |
| Solid | 1 (20) | 4 (80) | 0.972 | 0.960–9.799 | |
| Oncocytic | 0 (0) | 9 (100) | 1.257 | 1.082–1.460 | |
| Tall cell | 0 (0) | 21 (100) | 1.257 | 1.082–1.460 | |
| Classic | 9 (20.5) | 35 (79.5) | 1.000 | Reference | |
| Histology group | |||||
| Non-aggressive | 41 (33.3) | 82 (66.7) | <0.001 a | 17.000 | 2.247–128.615 |
| Aggressive | 1 (2.9) | 34 (97.1) | 1.000 | Reference | |
| Multifocality | |||||
| Present | 28 (23.7) | 90 (76.3) | 0.163 a | 0.578 | 0.266–1.255 |
| Absent | 14 (35.0) | 26 (65.0) | 1.000 | Reference | |
| Lymphovascular invasion | |||||
| Present | 15 (25.4) | 41 (73.2) | 0.966 a | 1.016 | 0.486–2.124 |
| Absent | 27 (26.5) | 75 (73.5) | 1.000 | Reference | |
| Extrathyroidal extension | |||||
| Absent | 35 (28.5) | 87 (71.3) | 0.270 a | 1.667 | 0.668–4.157 |
| Present | 7 (19.4) | 29 (80.6) | 1.000 | Reference | |
| Node metastasis | |||||
| Absent | 26 (25.0) | 78 (75.0) | 0.532 a | 0.792 | 0.380–1.649 |
| Present | 16 (29.6) | 38 (70.4) | 1.00 | Reference | |
| pERK1/2 expression | |||||
| High (>10%) | 28 (53.8) | 24 (46.2) | <0.001 a | 7.667 | 3.503–16.778 |
| Low (<10%) | 14 (13.2) | 92 (86.8) | Reference |
| Variables | B Coefficient | SE | Wald | p | adjOR | 95% CI | B/SE | Score |
|---|---|---|---|---|---|---|---|---|
| Nuclear score (3) | 1.213 | 0.480 | 6.375 | 0.012 | 3.364 | 1.312–8.626 | 2.527 | 1 |
| Capsule (absent) | 0.975 | 0.412 | 5.605 | 0.018 | 2.651 | 1.183–5.941 | 2.366 | 1 |
| Histology subtypes (aggressive) | 0.858 | 0.375 | 5.218 | 0.022 | 2.358 | 1.130–4.921 | 2.288 | 1 |
| pERK1/2 (>10%) | 1.460 | 0.410 | 12.668 | ≤0.001 | 4.308 | 1.927–9.627 | 3.560 | 2 |
| Total Score | Probability | Sensitivity | Specificity |
|---|---|---|---|
| 0 | 5% | 100% | 0% |
| 1 | 12.33% | 100% | 12% |
| 2 | 25.25% | 95% | 39% |
| 3 | 43% | 63% | 65% |
| 4 | 62% | 30% | 94% |
| 5 | 82% | 14% | 100% |
| Variables | B Coefficient | SE | Wald | p | adjOR | 95% CI | B/SE | Score |
|---|---|---|---|---|---|---|---|---|
| pERK1/2 (>10%) | 2.101 | 0.430 | 23.865 | ≤0.001 | 8.171 | 3.518–18.981 | 4.886 | 1 |
| Histology subtype (follicular) | 1.628 | 0.454 | 12.877 | ≤0.001 | 5.092 | 2.092–12.387 | 3.585 | 1 |
| Total Score | Probability | Sensitivity | Specificity |
|---|---|---|---|
| 0 | 5% | 100% | 0% |
| 1 | 27% | 98% | 48% |
| 2 | 70% | 45% | 91% |
| Model Outcome | BRAFV600E N (%) | p | adjOR | 95% CI | RAS N (%) | p | adjOR | 95% CI | Control N (%) |
|---|---|---|---|---|---|---|---|---|---|
| Comb. 1 | 22 (34.4) | Ref | Ref | Reference | 14 (33.3) | Ref | 1.00 | Reference | 68 (58.6) |
| Comb. 2 | 2 (3.1) | 0.882 | 0.883 | 0.171–4.568 | 7 (16.7) | 0.010 | 4.857 | 1.470–16.049 | 7 (6) |
| Comb. 3 | 37 (57.8) | ≤0.001 | 3.091 | 1.594–5.995 | 9 (21.4) | 0.725 | 1.181 | 0.467–2.989 | 37 (31.9) |
| Comb. 4 | 3 (4.7) | 0.295 | 2.318 | 0.481–11.168 | 12 (28.6) | ≤0.001 | 14.571 | 4.095–51.855 | 4 (3.4) |
| Model Outcome | Clinical Stage | Node Metastasis | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Early N (%) | Late N (%) | p | adjOR | 95% CI | No N (%) | Yes N (%) | p | adjOR | 95% CI | |
| Comb. 1 | 99 (95.2) | 5 (4.8) | 0.008 a | 1.000 | Reference | 76 (73) | 28 (27) | <0.001 a | 1.000 | Reference |
| Comb. 2 | 16 (100) | 0 (0) | 1.162 | 1.079–1.250 | 14 (87.5) | 2 (12.5) | 0.388 | 0.083–1.815 | ||
| Comb. 3 | 67 (80.7) | 16 (19.3) | 4.728 | 1.653–13.525 | 32 (38.5) | 51 (61.5) | 4.326 | 2.330–8.033 | ||
| Comb. 4 | 17 (89.5) | 2 (10.5) | 2.329 | 0.418–12.991 | 12 (63.1) | 7 (36.9) | 1.583 | 0.566–4.426 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harahap, A.S.; Subekti, I.; Panigoro, S.S.; Asmarinah; Lisnawati; Werdhani, R.A.; Agustina, H.; Khoirunnisa, D.; Mutmainnah, M.; Gultom, F.L.; et al. Developing Models to Predict BRAFV600E and RAS Mutational Status in Papillary Thyroid Carcinoma Using Clinicopathological Features and pERK1/2 Immunohistochemistry Expression. Biomedicines 2023, 11, 2803. https://doi.org/10.3390/biomedicines11102803
Harahap AS, Subekti I, Panigoro SS, Asmarinah, Lisnawati, Werdhani RA, Agustina H, Khoirunnisa D, Mutmainnah M, Gultom FL, et al. Developing Models to Predict BRAFV600E and RAS Mutational Status in Papillary Thyroid Carcinoma Using Clinicopathological Features and pERK1/2 Immunohistochemistry Expression. Biomedicines. 2023; 11(10):2803. https://doi.org/10.3390/biomedicines11102803
Chicago/Turabian StyleHarahap, Agnes Stephanie, Imam Subekti, Sonar Soni Panigoro, Asmarinah, Lisnawati, Retno Asti Werdhani, Hasrayati Agustina, Dina Khoirunnisa, Mutiah Mutmainnah, Fajar Lamhot Gultom, and et al. 2023. "Developing Models to Predict BRAFV600E and RAS Mutational Status in Papillary Thyroid Carcinoma Using Clinicopathological Features and pERK1/2 Immunohistochemistry Expression" Biomedicines 11, no. 10: 2803. https://doi.org/10.3390/biomedicines11102803