
Metabolic Fingerprinting for the Diagnosis of Clinically Similar Long COVID and Fibromyalgia Using a Portable FT-MIR Spectroscopic Combined with Chemometrics
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Sample Recruitment and Sample Storage
2.2. Sample Preparation
2.3. Spectral Data Acquisition
2.4. Chemometrics Analysis
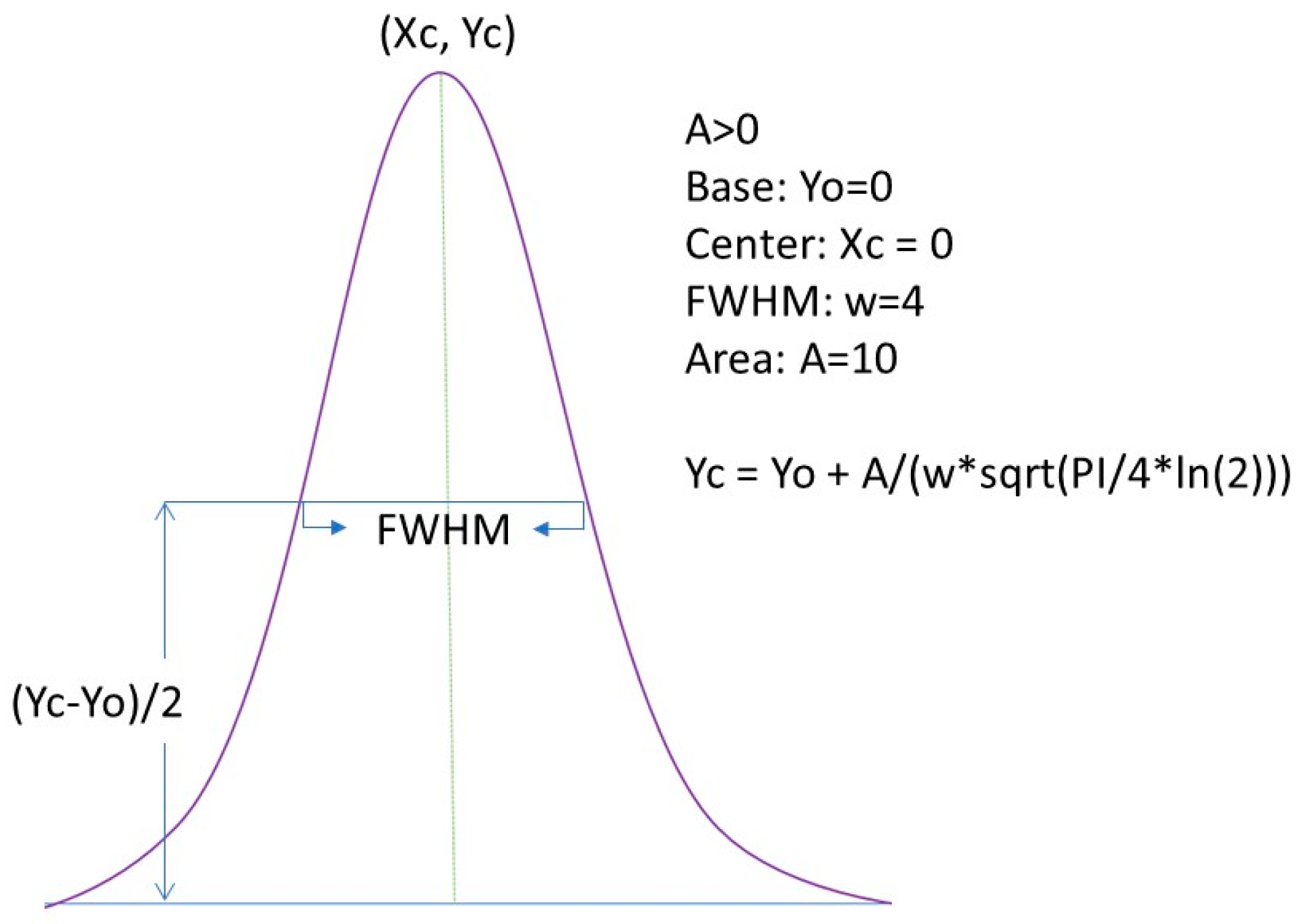
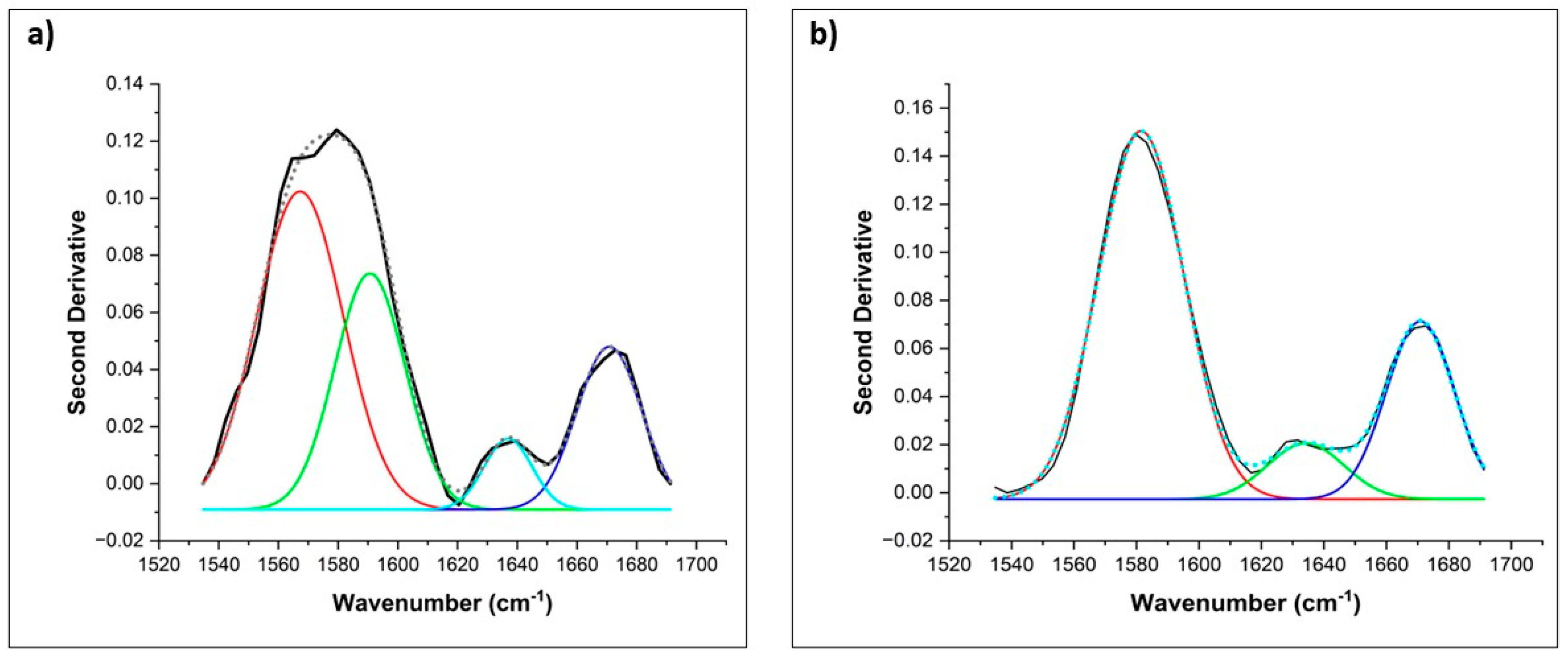
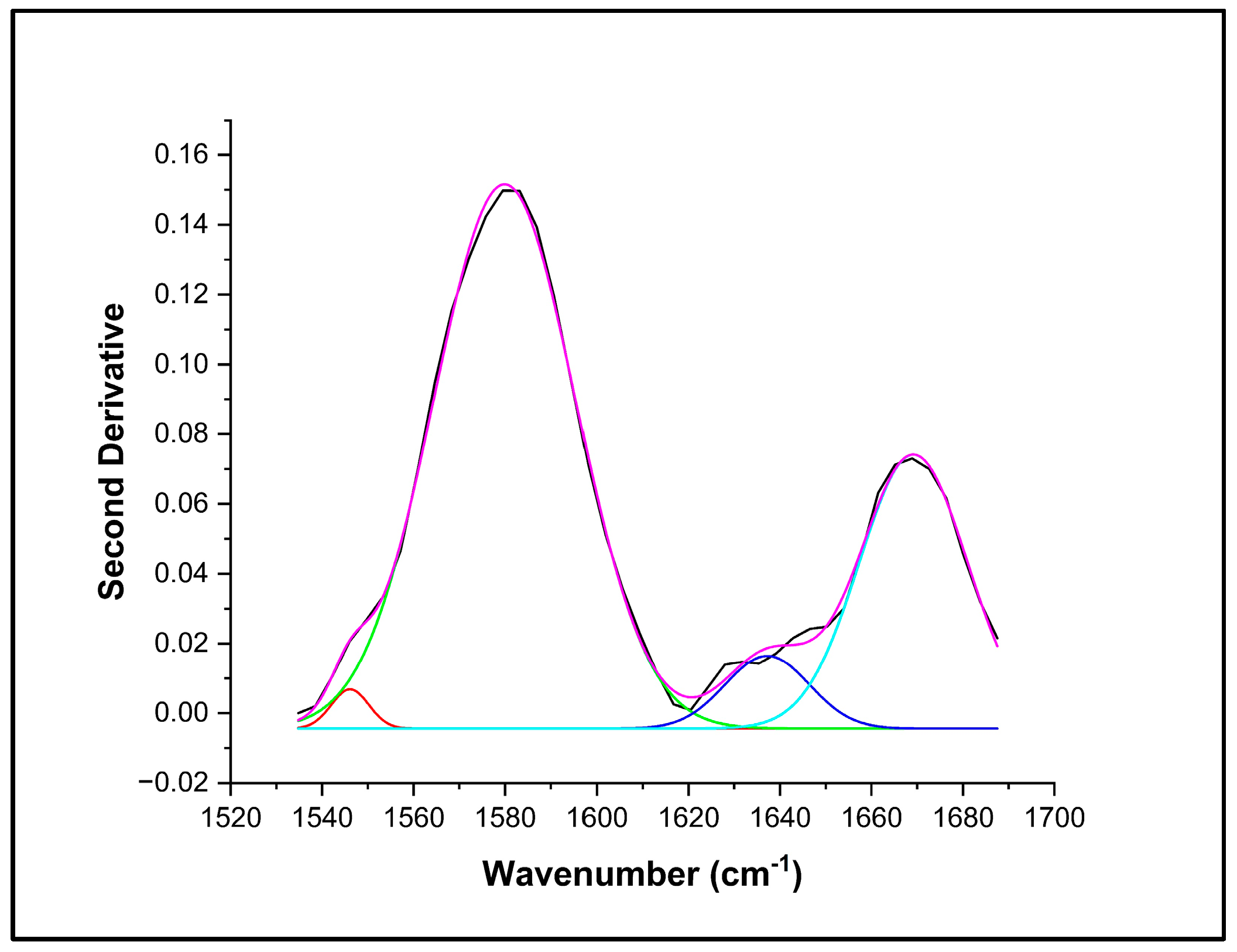
2.5. Spectra Deconvolution Analysis
3. Results
3.1. Clinical Characteristics of Subjects
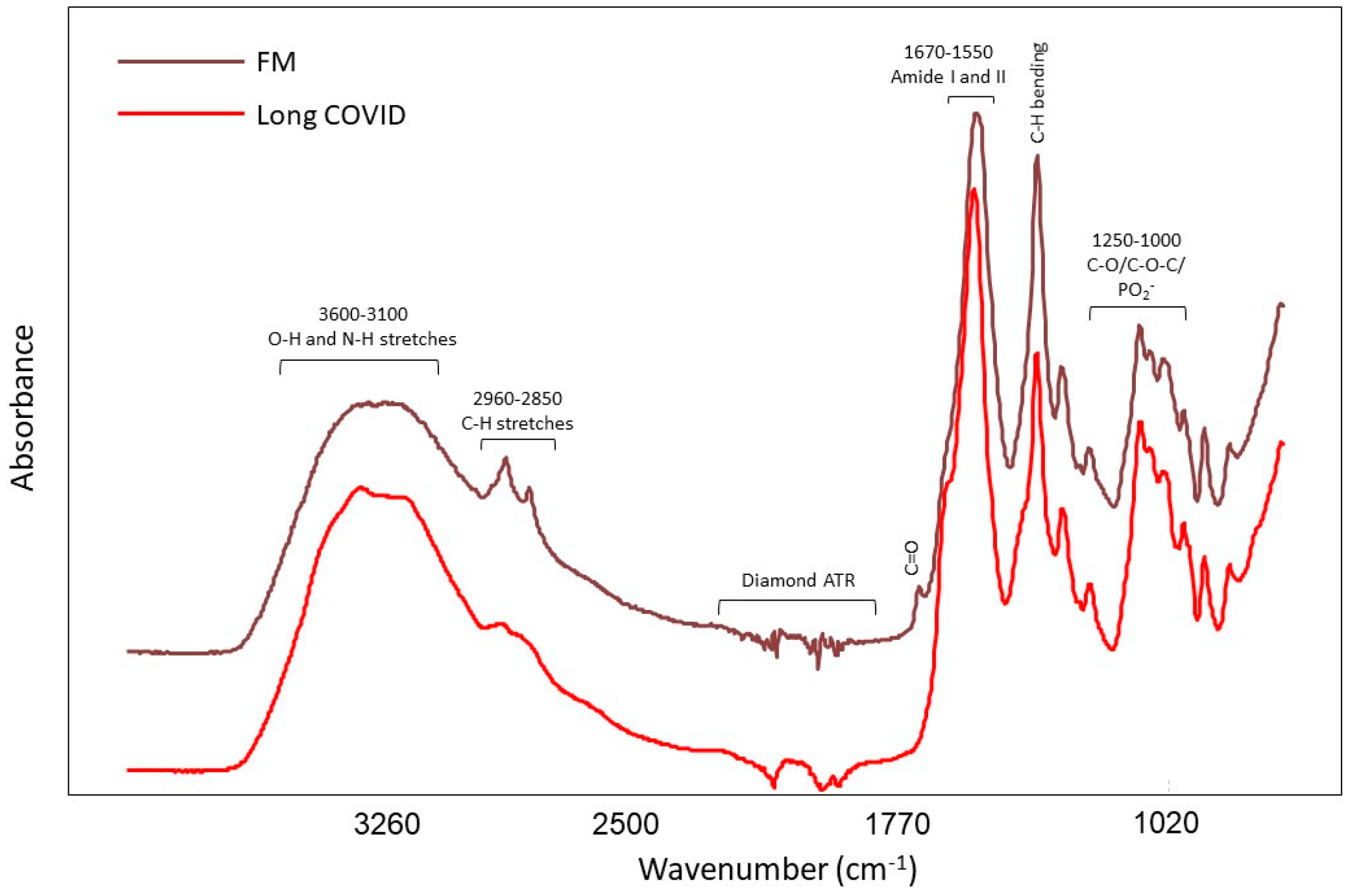
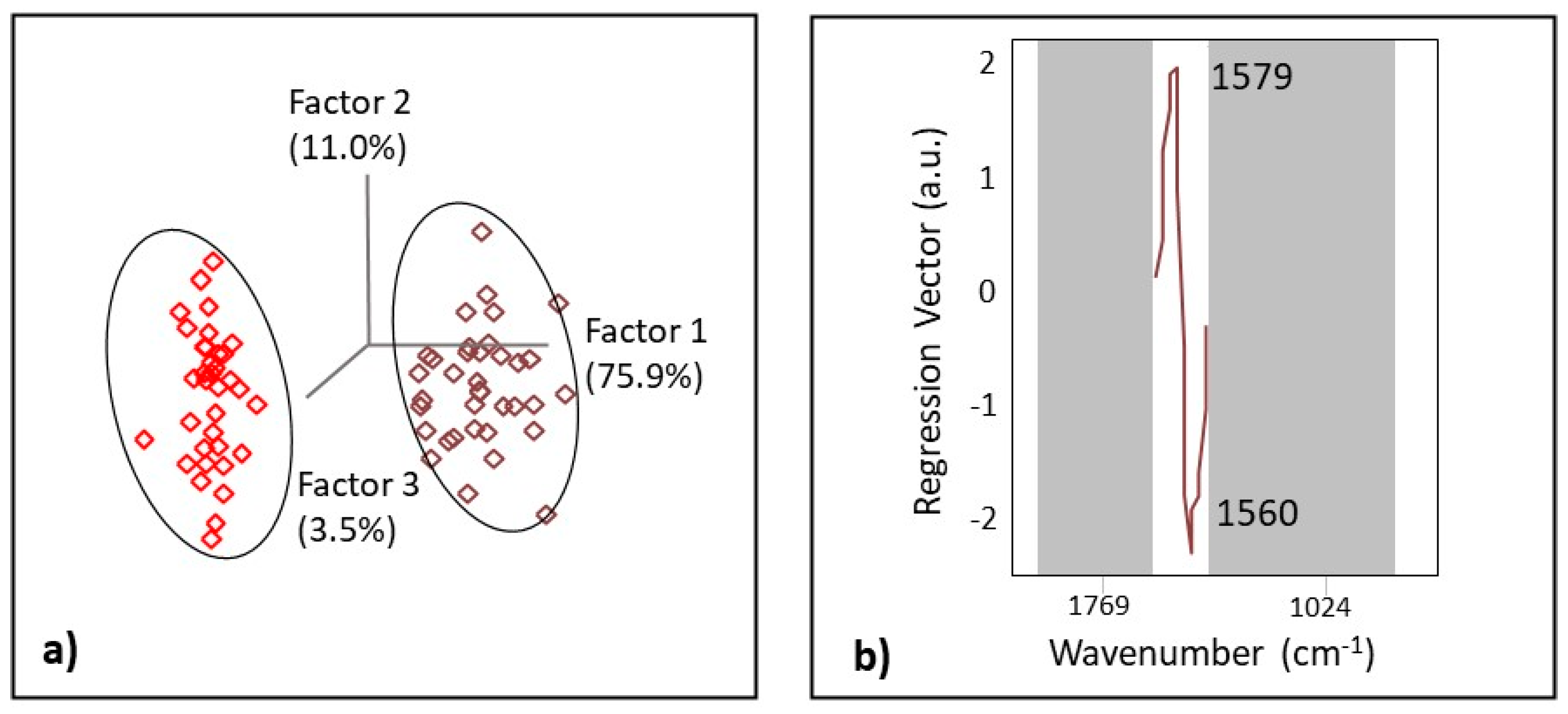
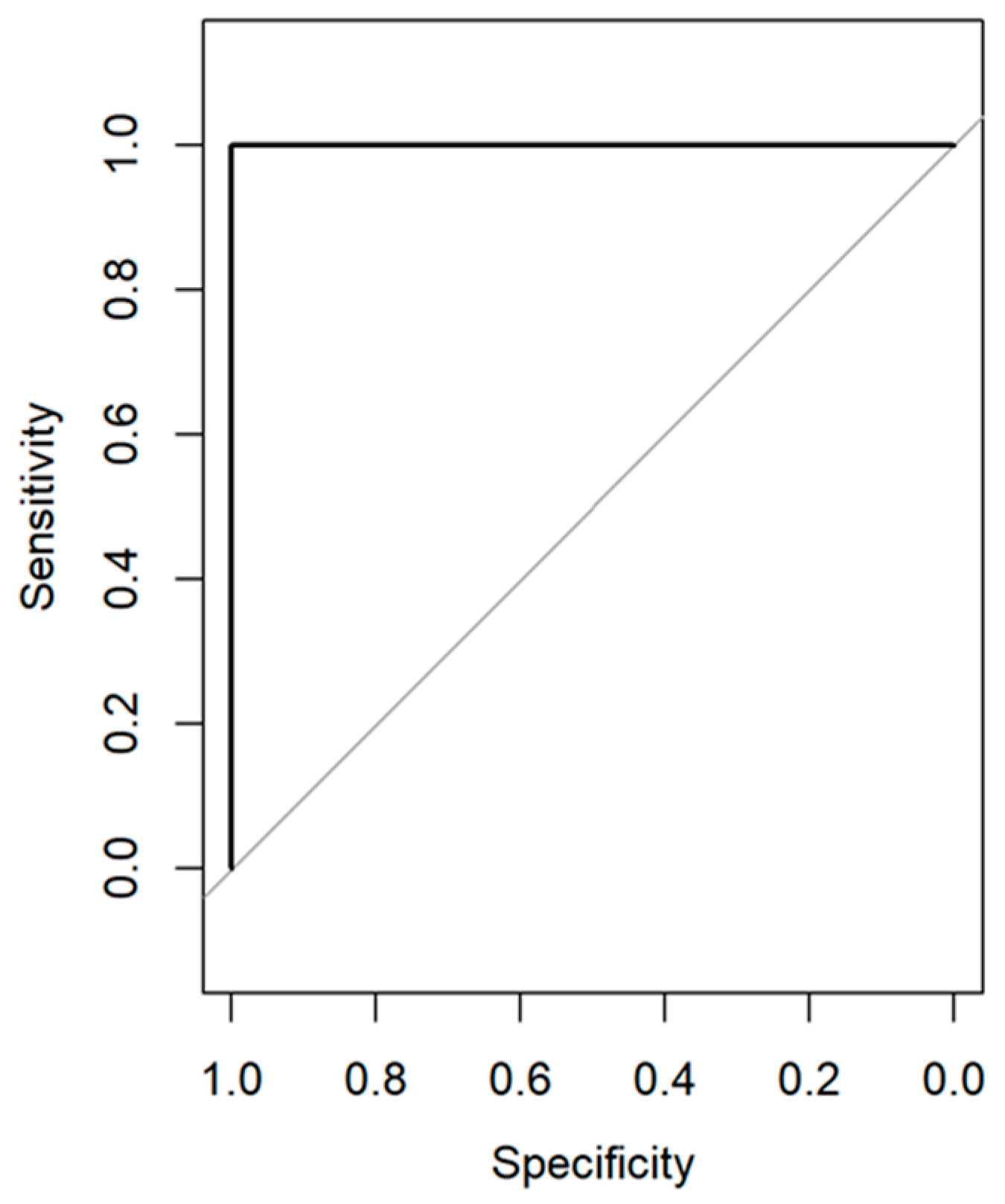
3.2. IR Spectroscopy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Institute for Health and Care Excellence; Scottish Intercollegiate Guidelines Network; Royal College of General Practitioners. COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19. Available online: https://www.nice.org.uk/guidance/ng188/resources/covid19-rapid-guideline-managing-the-longterm-effects-of-covid19-pdf-51035515742 (accessed on 12 May 2023).
- Chen, C.; Haupert, S.R.; Zimmermann, L.; Shi, X.; Fritsche, L.G.; Mukherjee, B. Global prevalence of post-coronavirus disease 2019 (COVID-19) condition or long COVID: A meta-analysis and systematic review. J. Infect. Dis. 2022, 226, 1593–1607. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-Las-Peñas, C.; Palacios-Ceña, D.; Gómez-Mayordomo, V.; Florencio, L.L.; Cuadrado, M.L.; Plaza-Manzano, G.; Navarro-Santana, M. Prevalence of post-COVID-19 symptoms in hospitalized and non-hospitalized COVID-19 survivors: A systematic review and meta-analysis. Eur. J. Intern. Med. 2021, 92, 55–70. [Google Scholar] [CrossRef] [PubMed]
- Michelen, M.; Manoharan, L.; Elkheir, N.; Cheng, V.; Dagens, A.; Hastie, C.; O’Hara, M.; Suett, J.; Dahmash, D.; Bugaeva, P.; et al. Characterising long COVID: A living systematic review. BMJ Glob. Health 2021, 6, e005427. [Google Scholar] [CrossRef] [PubMed]
- Alkodaymi, M.S.; Omrani, O.A.; Fawzy, N.A.; Shaar, B.A.; Almamlouk, R.; Riaz, M.; Obeidat, M.; Obeidat, Y.; Gerberi, D.; Taha, R.M.; et al. Prevalence of post-acute COVID-19 syndrome symptoms at different follow-up periods: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2022, 28, 657–666. [Google Scholar] [CrossRef]
- Han, Q.; Zheng, B.; Daines, L.; Sheikh, A. Long-term sequelae of COVID-19: A systematic review and meta-analysis of one-year follow-up studies on post-COVID symptoms. Pathogens 2022, 11, 269. [Google Scholar] [CrossRef]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major findings, mechanisms and recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. [Google Scholar] [CrossRef]
- World Health Organization. COVID-19 Weekly Epidemiological Update on COVID-19. 4 January 2023. Edition 124. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-COVID-19-4.january-2023 (accessed on 15 May 2023).
- Komaroff, A.L.; Lipkin, W.I. ME/CFS and Long COVID share similar symptoms and biological abnormalities: Road map to the literature. Front. Med. 2023, 10, 1187163. [Google Scholar] [CrossRef]
- Haider, S.; Janowski, A.J.; Lesnak, J.B.; Hayashi, K.; Dailey, D.L.; Chimenti, R.; Frey-Law, L.A.; Sluka, K.A.; Berardi, G. A comparison of pain, fatigue, and function between post–COVID-19 condition, fibromyalgia, and chronic fatigue syndrome: A survey study. Pain 2023, 164, 385–401. [Google Scholar] [CrossRef]
- Lambert, N.; Corps, S.; El-Azab, S.A.; Ramrakhiani, N.S.; Barisano, A.; Yu, L.; Pinto, M.D. COVID-19 surviors’ report of the timing duration, and health impacts of Post-Acute Sequelae of ASRS-CoV-2 (PASC) infection. MedRxiv, 2021. [Google Scholar] [CrossRef]
- Crook, H.; Raza, S.; Nowell, J.; Young, M.; Edison, P. Long COVIDmechanisms, risk factors, and management. BMJ 2021, 374, n1648. [Google Scholar] [CrossRef]
- El Tallawy, S.N.; Perglozzi, J.V.; Ahmed, R.S.; Kaki, A.M.; Naglub, M.S.; Lequang, J.K.; Hadarah, M.M. Pain Management in the Post-COVID Era- An Update: A Narrative Review. Pain Ther. 2021, 12, 423–448. [Google Scholar] [CrossRef]
- Galvez-Sánchez, C.M.; Reyes del Paso, G.A. Diagnostic Criteria for Fibromyalgia: Critical Review and Future Perspectives. J. Clin. Med. 2020, 9, 1219. [Google Scholar] [CrossRef] [PubMed]
- Ablin, J.N.; Wolfe, F. A Comparative Evaluation of the 2011 and 2016 Criteria for Fibromyalgia. J. Rheumatol. 2017, 44, 1271–1276. [Google Scholar] [CrossRef] [PubMed]
- Häuser, W.; Ablin, J.; Fitzcharles, M.-A.; Littlejohn, G.; Luciano, J.V.; Usui, C.; Walitt, B. Fibromyalgia. Nat. Rev. Dis. Prim. 2015, 1, 15022. [Google Scholar] [CrossRef] [PubMed]
- Smith, H.S.; Harris, R.; Clauw, D. Fibromyalgia: An afferent processing disorder leading to a complex pain generalized syndrome. Pain Physician 2011, 14, 217–246. [Google Scholar] [CrossRef]
- Wolfe, F.; Fitzcharles, M.A.; Goldenberg, D.L.; Hauser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Jon Russell, I.; Walitt, B. Comparison of physician-based and patient-based criteria for the diagnosis of fibromyalgia. Arthritis Care Res. 2016, 68, 652–659. [Google Scholar] [CrossRef]
- Wolfe, F.; Schmukler, J.; Jamal, S.; Castrejon, I.; Gibson, K.A.; Srinivasan, S.; Hauser, W.; Pincus, T. Diagnosis of fibromyalgia: Disagreement between fibromyalgia criteria and clinician-based fibromyalgia diagnosis in a university clinic. Arthritis Care Res. 2019, 71, 343–351. [Google Scholar] [CrossRef]
- Walitt, B.; Katz, R.S.; Bergman, M.J.; Wolfe, F. Three-quarters of persons in the US population reporting a clinical diagnosis of fibromyalgia do not satisfy fibromyalgia criteria: The 2012 national health interview survey. PLoS ONE 2016, 11, e0157235. [Google Scholar] [CrossRef]
- Copley, M.; Kozminski, B.; Gentile, N.; Geyer, R.; Friedly, J. Post-Acute Sequelae of SARS-CoV-2 (PASC): Musculoskeletal Conditions and Pain. Phys. Med. Rehabil. Clin. 2023. [Google Scholar] [CrossRef]
- Mohabbat, A.B.; Mohabbat, N.M.L.; Wight, E.C. Fibromyalgia and chronic fatigue syndrome in the age of COVID-19. Mayo Clin. Proc. Innov. Qual. Outcomes 2020, 4, 764–766. [Google Scholar] [CrossRef]
- Karaarslan, F.; Güneri, F.D.; Kardeş, S. Long COVID: Rheumatologic/musculoskeletal symptoms in hospitalized COVID-19 survivors at 3 and 6 months. Clin. Rheumatol. 2022, 41, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-las-Peñas, C.; Nijs, J.; Giordano, R.; Arendt-Nielsen, L. Precision management of post-COVID pain: An evidence and clinical-based approach. Eur. J. Pain 2023, 27, 9. [Google Scholar] [CrossRef] [PubMed]
- Magdy, R.; Eid, R.A.; Fathy, W.; Abdel-Aziz, M.M.; Ibrahim, R.E.; Yehia, A.; Hussein, M. Characteristics and risk factors of persistent neuropathic pain in recovered COVID-19 patients. Pain Med. 2022, 23, 774–781. [Google Scholar] [CrossRef] [PubMed]
- Bileviciute-Ljungar, I.; Norrefalk, J.R.; Borg, K. Pain burden in post-COVID-19 syndrome following mild COVID-19 infection. J. Clin. Med. 2022, 11, 771. [Google Scholar] [CrossRef]
- Johnson, E.; Lam, C.; Axeen, S.; Vosooghi, A.; Schneberk, T. 28EMF The Opioid Epidemic Meets the Coronavirus Pandemic: Rates and Patient Characteristics of Emergency Department Visits for Opiate Use Disorder During the COVID-19 Pandemic in the Los Angeles County Public Hospital System. Ann. Emerg. Med. 2021, 78, S14. [Google Scholar] [CrossRef]
- Wasserman, R.A.; Brummett, C.M.; Goesling, J.; Tsodikov, A.; Hassett, A.L. Characteristics of chronic pain patients who take opioids and persistently report high pain intensity. Reg. Anesth. Pain Med. 2014, 39, 13–17. [Google Scholar] [CrossRef]
- Fitzcharles, M.A.; Gamsa, P.A.; Ware, M.A.; Shir, Y. Opioid use, misuse, and abuse in patients labeled as fibromyalgia. Am. J. Med. 2011, 124, 955–960. [Google Scholar] [CrossRef]
- Phillips, K.; Clauw, D.J. Central pain mechanisms in the rheumatic diseases: Future directions. Arthritis Rheum. 2013, 65, 291–302. [Google Scholar] [CrossRef]
- Institute of Medicine (IOM). Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education and Research; National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Mezei, L.; Murinson, B.B. Pain education in North American medical schools. J. Pain 2011, 12, 1199–1208. [Google Scholar] [CrossRef]
- Morley-Forster, P.K.; Pergolizzi, J.V.; Taylor, R., Jr.; Axford-Gatley, R.A.; Sellers, E.M. Mitigating the risk of opioid abuse through a balanced undergraduate pain medicine curriculum. J. Pain Res. 2013, 6, 791–801. [Google Scholar] [CrossRef]
- Hackshaw, K.V.; Miller, J.S.; Aykas, D.P.; Rodriguez-Saona, L. vibrational spectroscopy for identification of metabolites in biologic samples. Molecules 2020, 25, 4725. [Google Scholar] [CrossRef] [PubMed]
- Hackshaw, K.V. The search for biomarkers in fibromyalgia. Diagnostics 2021, 11, 156. [Google Scholar] [CrossRef] [PubMed]
- Qiu, S.; Cai, Y.; Yao, H.; Lin, C.; Xie, Y.; Tang, S.; Zhang, A. Small molecule metabolites: Discovery of bi-omarkers and therapeutic targets. Signal Transduct. Target. Ther. 2023, 8, 132. [Google Scholar] [CrossRef] [PubMed]
- Yao, S.; Bao, H.; Nuguri, S.M.; Yu, L.; Mikulik, Z.; Osuna-Diaz, M.M.; Sebastian, K.R.; Hackshaw, K.V.; Rodriguez-Saona, L. Rapid biomarker-based diagnosis of fibromyalgia syndrome and related rheumatologic disorders by portable FT-IR spectroscopic techniques. Biomedicines 2023, 11, 712. [Google Scholar] [CrossRef] [PubMed]
- Pullano, S.A.; Bianco, M.G.; Greco, M.; Mazzuca, D.; Nisticò, S.P.; Fiorillo, A.S. FT-IR saliva analysis for the diagnosis of psoriasis: A pilot study. Biomed. Signal Process. Control. 2022, 74, 103525. [Google Scholar] [CrossRef]
- Falamas, A.; Faur, C.I.; Ciupe, S.; Chirila, M.; Rotaru, H.; Hedesiu, M.; Cinta Pinzaru, S. Rapid and noninva-sive diagnosis of oral and oropharyngeal cancer based on micro-Raman and FT-IR spectra of saliva. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2021, 252, 119477. [Google Scholar] [CrossRef]
- Lilo, T.; Morais, C.L.M.; Shenton, C.; Ray, A.; Gurusinghe, N. Revising Fourier-transform infrared (FT-IR) and Raman spectroscopy towards brain cancer detection. Photodiagnosis Photodyn. Ther. 2022, 38, 102785. [Google Scholar] [CrossRef]
- Rodriguez-Saona, L.; Aykas, D.P.; Borba, K.R.; Urtubia, A. Miniaturization of optical sensors and their poten-tial for high-throughput screening of foods. Curr. Opin. Food Sci. 2020, 31, 136–150. [Google Scholar] [CrossRef]
- Hackshaw, K.V.; Aykas, D.P.; Sigurdson, G.T.; Plans, M.; Madiai, F.; Yu, L.; Buffington, C.A.T.; Giusti, M.M.; Rodriguez-Saona, L. Metabolic fingerprinting for diagnosis of fibromyalgia and other rheumatologic disor-ders. J. Biol. Chem. 2019, 294, 2555–2568. [Google Scholar] [CrossRef]
- Hackshaw, K.V.; Rodriguez-Saona, L.; Plans, M.; Bell, L.N.; Buffington, C.A.T. A bloodspot-based diagnostic test for fibromyalgia syndrome and related disorders. Analyst 2013, 138, 4453. [Google Scholar] [CrossRef]
- Zhang, L.; Xiao, M.; Wang, Y.; Peng, S.; Chen, Y.; Zhang, D.; Zhang, D.; Guo, Y.; Wang, X.; Luo, H.; et al. Fast Screening and Primary Diagnosis of COVID-19 by ATR–FT-IR. Anal. Chem. 2021, 93, 2191–2199. [Google Scholar] [CrossRef]
- Wood, B.R.; Kochan, K.; Bedolla, D.E.; Salazar-Quiroz, N.; Grimley, S.L.; Perez-Guaita, D.; Baker, M.J.; Vongsvivut, J.; Tobin, M.J.; Bambery, K.R.; et al. Infrared Based Saliva Screening Test for COVID-19. Angew. Chem. Int. Ed. 2021, 60, 17102–17107. [Google Scholar] [CrossRef]
- Nascimento, M.H.C.; Marcarini, W.D.; Folli, G.S.; da Silva Filho, W.G.; Barbosa, L.L.; de Paulo, E.H.; Vassallo, P.F.; Mill, J.G.; Barauna, V.G.; Martin, F.L.; et al. Noninvasive Diagnostic for COVID-19 from Saliva Biofluid via FTIR Spectroscopy and Multivariate Analysis. Anal. Chem. 2022, 94, 2425–2433. [Google Scholar] [CrossRef]
- Barauna, V.G.; Singh, M.N.; Barbosa, L.L.; Marcarini, W.D.; Vassallo, P.F.; Mill, J.G.; Ribeiro-Rodrigues, R.; Campos, L.C.G.; Warnke, P.H.; Martin, F.L. Ultrarapid On-Site Detection of SARS-CoV-2 Infection Using Simple ATR-FTIR Spectroscopy and an Analysis Algorithm: High Sensitivity and Specificity. Anal. Chem. 2021, 93, 2950–2958. [Google Scholar] [CrossRef]
- Dierckx, T.; van Elslande, J.; Salmela, H.; Decru, B.; Wauters, E.; Gunst, J.; Van Herck, Y.; Wauters, J.; Stessel, B.; Vermeersch, P. The metabolic fingerprint of COVID-19 severity. MedRxiv 2020, 12, 2020-11. [Google Scholar] [CrossRef]
- Bennett, R.M.; Friend, R.; Jones, K.D.; Ward, R.; Han, B.K.; Ross, R.L. The Revised Fibromyalgia Impact Questionnaire (FIQR): Validation and psychometric properties. Arthritis Res. Ther. 2009, 11, R120. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T. An Inventory for Measuring Depression. Arch. Gen. Psychiatry 1961, 4, 561. [Google Scholar] [CrossRef] [PubMed]
- Friend, R.; Bennett, R.M. Distinguishing fibromyalgia from rheumatoid arthritis and systemic lupus in clinical questionnaires: An analysis of the revised Fibromyalgia Impact Questionnaire (FIQR) and its variant, the Symptom Impact Questionnaire (SIQR), along with pain locations. Arthritis Res. Ther. 2011, 13, R58. [Google Scholar] [CrossRef]
- Perrot, S.; Bouhassira, D.; Fermanian, J. CEDR (Cercle d’Etude de la Douleur en Rhumatologie) Development and validation of the Fibromyalgia Rapid Screening Tool (FiRST). Pain 2010, 150, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Greening, D.W.; Simpson, R.J. A centrifugal ultrafiltration strategy for isolating the low-molecular weight (≤25K) component of human plasma proteome. J. Proteom. 2010, 73, 637–648. [Google Scholar] [CrossRef]
- Wold, S.; Antti, H.; Lindgren, F.; Öhman, J. Orthogonal signal correction of near-infrared spectra. Chemom. Intell. Lab. Syst. 1998, 44, 175–185. [Google Scholar] [CrossRef]
- Schoot, M.; Kapper, C.; van Kollenburg, G.H.; Postma, G.J.; van Kessel, G.; Buydens, L.M.C.; Jansen, J.J. In-vestigating the need for preprocessing of near-infrared spectroscopic data as a function of sample size. Chemom. Intell. Lab. Syst. 2020, 204, 104105. [Google Scholar] [CrossRef]
- Shariff, M.I.F.; Ladep, N.G.; Cox, I.J.; Williams, H.R.T.; Okeke, E.; Malu, A.; Thillainayagam, A.V.; Crossey, M.M.E.; Khan, S.A.; Thomas, H.C.; et al. Characterization of Urinary Biomarkers of Hepatocellular Carcino-ma Using Magnetic Resonance Spectroscopy in a Nigerian Population. J. Proteome Res. 2010, 9, 1096–1103. [Google Scholar] [CrossRef]
- Westerhuis, J.A.; Hoefsloot, H.C.J.; Smit, S.; Vis, D.J.; Smilde, A.K.; van Velzen, E.J.J.; van Duijnhoven, J.P.M.; van Dorsten, F.A. Assessment of PLSDA cross validation. Metabolomics 2008, 4, 81–89. [Google Scholar] [CrossRef]
- Hopkins, J.; Brenner, L.; Tumosa, C.S. Variation of the Amide I and Amide II peak absorbance ratio in human hair as measured by Fourier transform infrared spectroscopy. Forensic Sci. Int. 1991, 50, 61–65. [Google Scholar] [CrossRef]
- Takada, T.; Nijman, S.; Denaxas, S.; Snell, K.I.E.; Uijl, A.; Nguyen, T.-L.; Asselbergs, F.W.; Debray, T.P.A. In-ternal-external cross-validation helped to evaluate the generalizability of prediction models in large clus-tered datasets. J. Clin. Epidemiol. 2021, 137, 83–91. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022. [Google Scholar]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Yang, S.; Kong, J.; Dong, A.; Yu, S. Obtaining information about protein secondary structures in aqueous solution using Fourier transform IR spectroscopy. Nat. Protoc. 2015, 10, 382–396. [Google Scholar] [CrossRef] [PubMed]
- Ren, S.; Hinzman, A.A.; Kang, E.L.; Szczesniak, R.D.; Lu, L.J. Computational and statistical analysis of metabo-lomics data. Metabolomics 2015, 11, 1492–1513. [Google Scholar] [CrossRef]
- Ando, T.; Ishii, M.; Kamo, M.; Sato, Y. H-D exchange reaction on diamond surfaces studied by diffuse reflec-tance Fourier transform IR spectroscopy. Diam. Relat. Mater. 1995, 4, 607–611. [Google Scholar] [CrossRef]
- Mayo, D.W. Characteristic Frequencies of Alkanes. In Course Notes on the Interpretation of Infrared and Raman Spectra; John Wiley & Sons: New Jersey, NJ, USA, 2004; pp. 33–72. [Google Scholar] [CrossRef]
- West Virginia University. Background. In Infrared Spectroscopy; West Virginia University: Morgantown, WV, USA, 2016; pp. 1–7. [Google Scholar]
- Roy, S.; Perez-Guaita, D.; Bowden, S.; Heraud, P.; Wood, B.R. Spectroscopy goes viral: Diagnosis of hepatitis B and C virus infection from human sera using ATR-FTIR spectroscopy. Clin. Spectrosc. 2019, 1, 100001. [Google Scholar] [CrossRef]
- Liu, K.Z.; Shaw, R.A.; Man, A.; Dembinski, T.C.; Mantsh, H.H. Reagent-free, simultaneous determination of serum cholesterol in HDL and LDL by infrared spectroscopy. Clin. Chem. 2002, 48, 499–506. [Google Scholar] [CrossRef] [PubMed]
- California State University Stanislaus. Interpretation of Infrared Spectra; California State University Stanislaus: Turlock, CA, USA, 2023. [Google Scholar]
- Amalanathan, M.; Joe, I.H.; Kostova, I. Density functional theory calculation and vibrational spectral analysis of 4-hydroxy-3-(3-oxo-1-phenylbutyl)-2H-1-benzopyran-2-one. J. Raman Spectrosc. 2010, 41, 1076–1084. [Google Scholar] [CrossRef]
- Jayaraman, V.; Thiran, S.; Madden, D.R. Fourier transform infrared spectroscopic characteriza-tion of a photolabile precursor of glutamate. FEBS Lett. 2000, 475, 278–282. [Google Scholar] [CrossRef]
- Lorenz-Fonfria, V.A. Infrared Difference Spectroscopy of Proteins: From Bands to Bonds. Chem. Rev. 2020, 120, 3466–3576. [Google Scholar] [CrossRef]
- Pushie, M.J.; Messmer, M.; Sylvain, N.J.; Heppner, J.; Newton, J.M.; Hou, H.; Hackett, M.J.; Kelly, M.E.; Peeling, L. Multimodal imaging of hemorrhagic transformation biomarkers in an ischemic stroke model. Metallomics 2022, 14, mfac007. [Google Scholar] [CrossRef]
- Sen, I.; Tokatli, F. Differentiation of wines with the use of combined data of UV–visible spectra and color characteristics. J. Food Compost. Anal. 2016, 45, 101–107. [Google Scholar] [CrossRef]
- Mandrekar, J.N. Receiver operating characteristic curve in diagnostic test assessment. J. Thorac. Oncol. 2010, 5, 1315–1316. [Google Scholar] [CrossRef]
- Ferreira, I.C.C.; Aguiar, E.M.G.; Silva, A.T.F.; Santos, L.L.D.; Cardoso-Sousa, L.; Araújo, T.G.; Santos, D.W.; Goulart, L.R.; Sabino-Silva, R.; Maia, Y.C.P. Attenuated Total Reflection-Fourier Transform Infrared (ATR-FTIR) spectroscopy analysis of saliva for breast cancer diagnosis. J. Oncol. 2020, 2020, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Naseer, K.; Ali, S.; Qazi, J. ATR-FTIR spectroscopy as the future of diagnostics: A systematic review of the approach using bio-fluids. Appl. Spectrosc. Rev. 2021, 56, 85–97. [Google Scholar] [CrossRef]
- Fitzgerald, C.T.; Carter, L.P. Possible role for glutamic acid decarboxylase in fibromyalgia symptoms: A conceptual model for chronic pain. Med. Hypotheses 2011, 77, 409–415. [Google Scholar] [CrossRef]
- Pyke, T.L.; Osmotherly, P.G.; Baines, S. Measuring Glutamate Levels in the Brains of Fibromyalgia Patients and a Potential Role for Glutamate in the Pathophysiology of Fibromyalgia Symptoms: A Systematic Review. Clin. J. Pain 2017, 33, 944–954. [Google Scholar] [CrossRef] [PubMed]
- Holton, K.F.; Taren, D.L.; Thomson, C.A.; Bennett, R.M.; Jones, K.D. The effect of dietary glutamate on fibromyalgia and irritable bowel symptoms. Clin. Exp. Rheumatol. 2012, 30 (Suppl. 74), 10–17. [Google Scholar] [PubMed]
- Radhakrishnan, R.; Sluka, K.A. Increased glutamate and decreased glycine release in the rostral ventromedial medulla during induction of a pre-clinical model of chronic widespread muscle pain. Neurosci. Lett. 2009, 457, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Skyba, D.A.; Lisi, T.L.; Sluka, K.A. Excitatory amino acid concentrations increase in the spinal cord dorsal horn after repeated intramuscular injection of acidic saline. Pain 2005, 119, 142–149. [Google Scholar] [CrossRef]
- Ruggiero, V.; Mura, M.; Cacace, E.; Era, B.; Peri, M.; Sanna, G.; Fais, A. Free amino acids in fibromyalgia syndrome: Relationship with clinical picture. Scand. J. Clin. Lab. Inv. 2017, 77, 93–97. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | N(M/F) [%M/%F] | BMI | FIRST | SIQR | FIQR | BDI | |
|---|---|---|---|---|---|---|---|
| LC | 49.5 ± 14.59 | 50 (18/32) [36/64] | 29.47 ± 8.3 | 18/50 | 44.63 ± 21.4 | ||
| FM | 44.9.0 ± 12.8 | 50 (0/50) [0/100] | 31.57 ± 8.0 | 49.52 ± 21.5 | 18.31 ± 9.9 | ||
| HC | 45.8 ± 19.1 | 6(4/2) [67/33] | 25.3 ± 2.4 | 13.95 ± 27.0 | 0.5 ± 0.5 |
| LC | Age | BMI | SIQR |
|---|---|---|---|
| Male | 51.8 ± 11.6 | 28.9 ± 4.8 | 41.1 ± 15.9 |
| Female | 48.6 ± 16.0 | 29.6 ± 10.0 | 44.8 ± 23.0 |
| p value | 0.232 | 0.389 | 0.301 |
| Shapiro–Wilk normality test | p = 0.319 |
| FIQR/SIQR | Age | BMI | |
|---|---|---|---|
| p value | 0.158 | 0.055 | 0.140 |
| Medications a | Medications a | Medications a | ||||||
|---|---|---|---|---|---|---|---|---|
| Subject No. | LC | FM | Subject No. | LC | FM | Subject No. | LC | FM |
| 1 | 1, 3, 8, 10, 12 | 2, 4, 17, 18, 21 | 21 | 2, 7, 8, 10, 15 | 23, 26, 31 | 41 | 1 | 1 |
| 2 | 2, 5, 22 | 10, 26 | 22 | 2, 6, 13 | 4 | 42 | 2, 14, 15, 26 | 3, 18, 20, 21 |
| 3 | 8, 14, 23, 24 | 29 | 23 | 14, 17, 20, 24 | 2, 4, 26 | 43 | X | X |
| 4 | 7, 13, 25 | 1, 2, 10 | 24 | 7 | X | 44 | X | 4, 21 |
| 5 | 4, 26 | 3 | 25 | 2, 5, 18, 20, 22 | X | 45 | 2, 9, 14, 27, 30 | 4 |
| 6 | 13, 15, 18, 19, 27 | 1, 8, 12, 15, 21 | 26 | 1, 2, 13, 15, 26 | 4, 12 | 46 | 10, 13, 14 | 3, 4, 16 |
| 7 | 2, 10, 18, 21, 23 | X | 27 | X | 2, 4, 5, 16, 30 | 47 | 4, 15, 21 | 21, 26 |
| 8 | 9, 19, 23 | 18, 24 | 28 | 12, 13, 14, 20, 23 | X | 48 | 7, 9, 20 | 2, 4, 26, 29 |
| 9 | 14, 16, 29 | 2, 5, 18 | 29 | 19 | 1, 4 | 49 | X | 2, 4, 7, 10, 20 |
| 10 | 15 | 2, 29 | 30 | 10 | 1, 2, 21, 27 | 50 | 2 | X |
| 11 | 6 | 26, 29 | 31 | 1, 15 | 1, 5, 10 | |||
| 12 | 4, 15 | 2, 7, 15 | 32 | 8 | 1, 3 | |||
| 13 | 7, 13, 22 | 2, 4, 21 | 33 | 2, 9, 15, 20 | 1, 3, 18 | |||
| 14 | 2, 13, 18, 19, 20 | 15 | 34 | 2, 9, 16 | 4 | |||
| 15 | 7, 12, 14, 20 | 2, 18 | 35 | X | 4, 7, 14, 20 | |||
| 16 | 21, 26 | X | 36 | 2, 13, 18, 19 | 11 | |||
| 17 | X | 4 | 37 | 8, 10, 18, 22, 23 | 17 | |||
| 18 | 8, 19, 29 | 3, 7, 12, 19, 20, 21 | 38 | 15, 19, 20, 21, 23, 24 | 12, 13, 26 | |||
| 19 | 15 | 3 | 39 | X | 2, 12, 14 | |||
| 20 | 5, 23, 26, 27 | 4, 10 | 40 | 24 | 9 | |||
| Wavenumber (cm−1) | Area (%) | Wavenumber (cm−1) | Area (%) | Wavenumber (cm−1) | Area (%) | Wavenumber (cm−1) | Area (%) | |
|---|---|---|---|---|---|---|---|---|
| FM | * 1565 a ± 3 # | 36.1 A ± 18.1 | 1588 b ± 4 | 38.2 A ± 15.6 | 1639 d ± 5 | 4.7 C ± 1.6 | 1670 f ± 2 | 21.3 D ± 7.5 |
| LC | - | - | 1581 B ± 2 | 70.3 B ± 8.9 | 1635 e ± 7 | 9.9 C ± 9.2 | 1670 f ± 2 | 23.9 D ± 5.3 |
| Figures of Merit | Calibration Set n = 80 Samples | Prediction Set n = 20 Samples |
|---|---|---|
| SECV/SEP | 0.10 | 0.18 |
| R2 | 0.98 | 0.96 |
| Sensitivity (%) | 100 | 100 |
| Specificity (%) | 100 | 100 |
| Accuracy (%) | 100 | 100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hackshaw, K.V.; Yao, S.; Bao, H.; de Lamo Castellvi, S.; Aziz, R.; Nuguri, S.M.; Yu, L.; Osuna-Diaz, M.M.; Brode, W.M.; Sebastian, K.R.; et al. Metabolic Fingerprinting for the Diagnosis of Clinically Similar Long COVID and Fibromyalgia Using a Portable FT-MIR Spectroscopic Combined with Chemometrics. Biomedicines 2023, 11, 2704. https://doi.org/10.3390/biomedicines11102704
Hackshaw KV, Yao S, Bao H, de Lamo Castellvi S, Aziz R, Nuguri SM, Yu L, Osuna-Diaz MM, Brode WM, Sebastian KR, et al. Metabolic Fingerprinting for the Diagnosis of Clinically Similar Long COVID and Fibromyalgia Using a Portable FT-MIR Spectroscopic Combined with Chemometrics. Biomedicines. 2023; 11(10):2704. https://doi.org/10.3390/biomedicines11102704
Chicago/Turabian StyleHackshaw, Kevin V., Siyu Yao, Haona Bao, Silvia de Lamo Castellvi, Rija Aziz, Shreya Madhav Nuguri, Lianbo Yu, Michelle M. Osuna-Diaz, W. Michael Brode, Katherine R. Sebastian, and et al. 2023. "Metabolic Fingerprinting for the Diagnosis of Clinically Similar Long COVID and Fibromyalgia Using a Portable FT-MIR Spectroscopic Combined with Chemometrics" Biomedicines 11, no. 10: 2704. https://doi.org/10.3390/biomedicines11102704