
Long-Term Radiological Pulmonary Changes in Mechanically Ventilated Patients with Respiratory Failure due to SARS-CoV-2 Infection

 , , ,
, , ,
Abstract
:1. Introduction
- (1)
- The alveolar epithelium situated on its basement membrane.
- (2)
- The capillary endothelium that lays on its basement membrane.
- (3)
- A thin interstitium separating the two basement membranes, a connective tissue containing fibroblasts, macrophages, collagen, and elastic fibers [17].
- (1)
- An exudative, early phase with disruption of the alveolocapillary membrane and edematous flooding of the alveolar spaces, followed by
- (2)
- A proliferative phase, with clearance of exudative fluid and an attempt to reestablish the alveolar barrier; then, in patients who survive,
- (3)
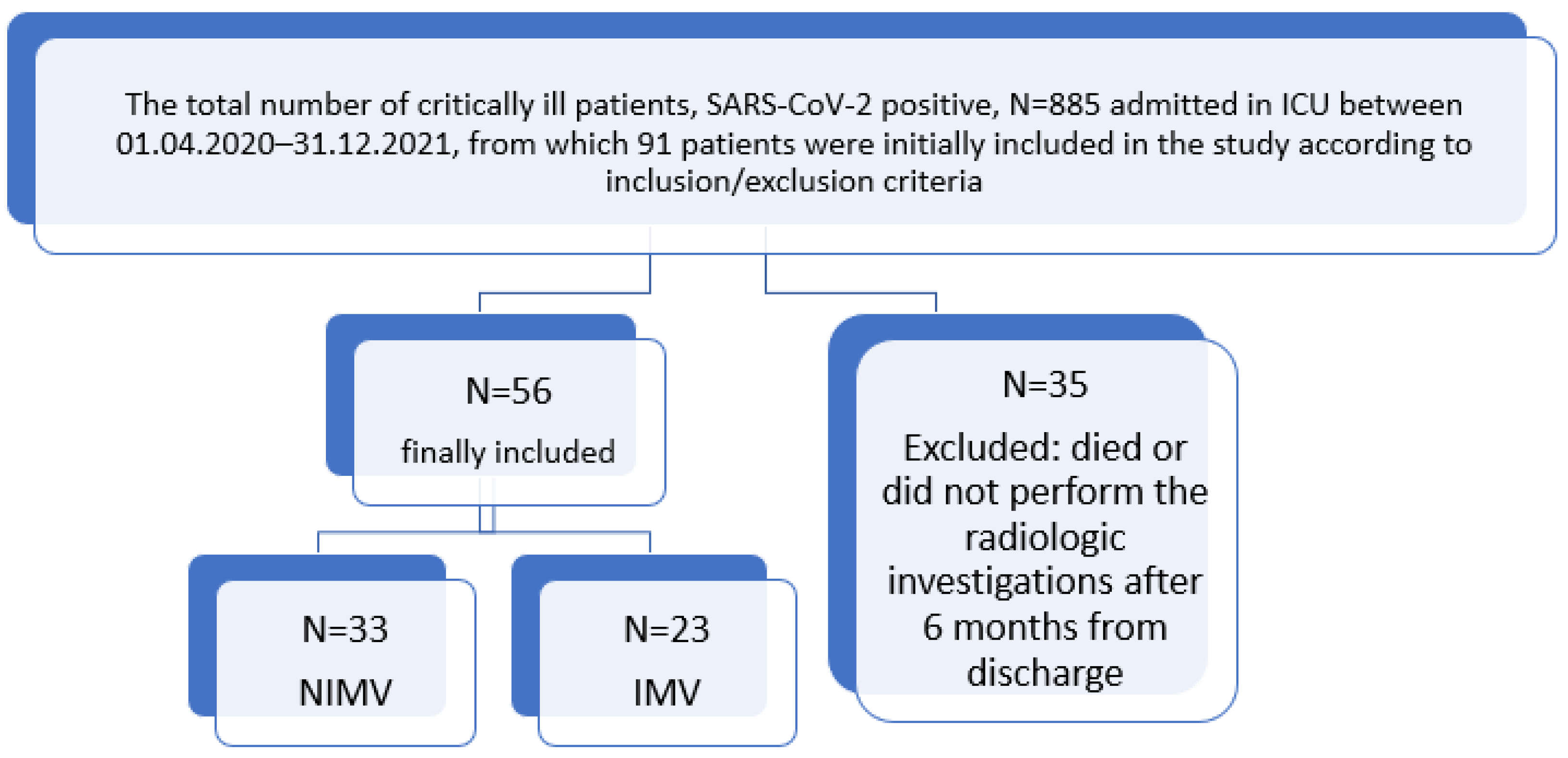
2. Materials and Methods
2.1. Data Collection
- (1)
- Mild-to-moderate forms in those who presented pulmonary radiological changes of 10–50%.
- (2)
- Severe forms in patients presenting more than 50% pulmonary radiological changes.
- (1)
- Those with NIMV
- (2)
- Those with IMV
2.2. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Associated Pre-Existing Comorbidities
3.3. The Duration of Mechanical Ventilation
3.4. Number of Days Spent in the ICU
3.5. PaO2/FiO2 Ratio
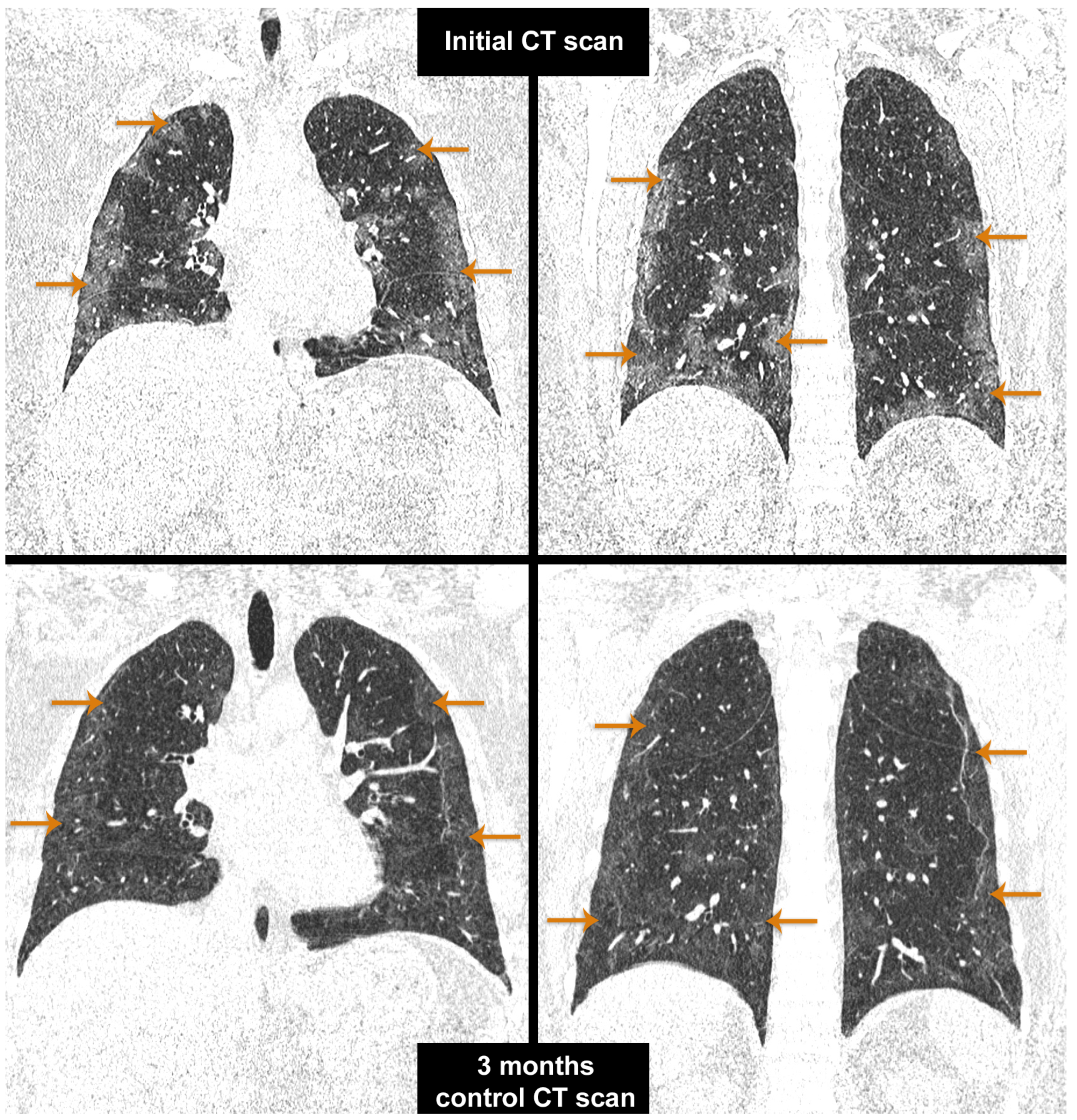
3.6. Radiological Evaluation of Patients 6 Months after Discharge
3.7. Evaluation of the Patients with NIMV
3.8. Evaluation of the Patients with IMV
3.9. Paraclinical Laboratory Examinations
4. Discussion
4.1. Risk Factors for Pulmonary Fibrosis
4.1.1. ARDS
4.1.2. Hypercoagulability
4.1.3. Role of Oxygen
4.1.4. Age and Sex
4.1.5. Associated Comorbidities
4.1.6. Treatment and Ventilatory Support
4.1.7. Disease Severity
4.2. Follow Up
4.3. Preliminary Findings
4.4. General Considerations and Pathophysiological Aspects of Pulmonary Fibrosis
4.4.1. Role of Immune Cells and Cytokines
- (1)
- M1 (classical)
- (2)
- M2 (alternative)
4.4.2. Pulmonary Fibrosis Mechanism
4.5. Therapeutic Perspective
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACE2 | angiotensin-converting enzyme 2 |
| AECIIs | type II alveolar epithelial cells |
| AECIs | Type I alveolar epithelial cells |
| ALT | alanine transaminase |
| APACHE II | acute physiology and chronic health evaluation II |
| APCs | antigen-presenting cells |
| ARDS | acute respiratory distress syndrome |
| AST | aspartate aminotransferase |
| BCL2L.15 | b-cell lymphoma 2 (BCL-2) like protein 15 |
| COPD | chronic obstructive pulmonary disease |
| COVID-19 | Corona virus disease 2019 |
| CRISP3 | cysteine-rich secretory protein 3 |
| CRP | C-reactive protein |
| CT | computerized tomography |
| DAD | diffuse alveolar damage |
| ECM | extracellular matrix |
| EGF | epidermal growth factor |
| EGFR | Epidermal growth factor receptor |
| FGF | fibroblast growth factor |
| FVC | forced vital capacity |
| H7N9 | avian influenza A |
| HIF-1-α | hypoxia-inducible factor 1-alpha |
| ICAM-1 | intercellular adhesion molecule 1 |
| ICU | intensive care unit |
| IFN-γ | Interferon-gamma |
| IMV | invasive mechanical ventilation |
| IPF | idiopathic pulmonary fibrosis |
| LDH | lactate dehydrogenase |
| MHCII | major histocompatibility complex II |
| MMP | matrix metallopeptidase |
| MMP-8 | matrix metalloproteinase-8 |
| NF-KB | nuclear-factor kappa B |
| NIMV | non-invasive mechanical ventilation |
| PaO2/FiO2 | the ratio of arterial oxygen partial pressure PaO2 to fractional inspired oxygen FiO2 |
| PCIII | procollagen type III |
| PCIV | procollagen type IV |
| PDE4D | phosphodiesterase 4D |
| PDGF | platelet-derived growth factor |
| qSOFA | Quick Sequential Organ Failure Assessment |
| ROS | Reactive oxygen species |
| RT-PCR | reverse transcription polymerase chain-reaction |
| SARS-CoV-1 | Severe acute respiratory syndrome coronavirus 1 |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| SD | standard deviation |
| TGF-β1 | transforming growth factor β |
| Th | T helper |
| TLC | total lung capacity |
| TLR | toll-like receptor |
| TNF | Tumor necrosis factor |
| VCAM-1 | vascular adhesion molecule 1 |
| VEGF | vascular endothelial growth factor |
| VILI | ventilation-induced lung injury |
| WBC | white blood cell |
References
- World Health Organization. Available online: https://covid19.who.int/ (accessed on 27 July 2023).
- Wilde, H.; Mellan, T.; Hawryluk, I.; Dennis, J.M.; Denaxas, S.; Pagel, C.; Duncan, A.; Bhatt, S.; Flaxman, S.; Mateen, B.A.; et al. The association between mechanical ventilator compatible bed occupancy and mortality risk in intensive care patients with COVID-19: A national retrospective cohort study. BMC Med. 2021, 19, 213. [Google Scholar] [CrossRef]
- Stoian, A.; Stoian, M.; Bajko, Z.; Maier, S.; Andone, S.; Cioflinc, R.A.; Motataianu, A.; Barcutean, L.; Balasa, R. Autoimmune Encephalitis in COVID-19 Infection: Our Experience and Systematic Review of the Literature. Biomedicines 2022, 10, 774. [Google Scholar] [CrossRef]
- Stoian, A.; Bajko, Z.; Stoian, M.; Cioflinc, R.A.; Niculescu, R.; Arbănași, E.M.; Russu, E.; Botoncea, M.; Bălașa, R. The Occurrence of Acute Disseminated Encephalomyelitis in SARS-CoV-2 Infection/Vaccination: Our Experience and a Systematic Review of the Literature. Vaccines 2023, 11, 1225. [Google Scholar] [CrossRef]
- Roman, A.; Moldovan, S.; Stoian, M.; Tilea, B.; Dobru, D. SARS-CoV-2 associated liver injury: A six-month follow-up analysis of liver function recovery. Med. Pharm. Rep. 2022, 95, 393–399. [Google Scholar] [CrossRef]
- Boeriu, A.; Roman, A.; Dobru, D.; Stoian, M.; Voidăzan, S.; Fofiu, C. The Impact of Clostridioides Difficile Infection in Hospitalized Patients: What Changed during the Pandemic? Diagnostics 2022, 12, 3196. [Google Scholar] [CrossRef]
- Roman, A.; Georgescu, A.M.; Moldovan, S.; Stoian, M.; Dobru, D. Liver injury in COVID-19 patients—A multidisciplinary experience and a call for national consensus. J. Gastrointest. Liver Dis. 2020, 29, 688–690. [Google Scholar] [CrossRef]
- Roman, A.; Moldovan, S.; Santini, A.; Stoian, M.; Dobru, D. Impact of the Severity of Liver Injury in COVID-19 Patients Admitted to an Intensive Care Unit During the SARS-CoV2 Pandemic Outbreak. J. Crit. Care Med. 2021, 7, 211–216. [Google Scholar] [CrossRef]
- He, W.; Liu, X.; Hu, B.; Li, D.; Chen, L.; Li, Y.; Tu, Y.; Xiong, S.; Wang, G.; Deng, J.; et al. Mechanisms of SARS-CoV-2 Infection-Induced Kidney Injury: A Literature Review. Front. Cell. Infect. Microbiol. 2022, 12, 838213. [Google Scholar] [CrossRef]
- Dhakal, B.P.; Sweitzer, N.K.; Indik, J.H.; Acharya, D.; William, P. SARS-CoV-2 Infection and Cardiovascular Disease: COVID-19 Heart. Heart Lung Circ. 2020, 29, 973–987. [Google Scholar] [CrossRef]
- Amin, B.J.H.; Kakamad, F.H.; Ahmed, G.S.; Ahmed, S.F.; Abdulla, B.A.; Mohammed, S.H.; Mikael, T.M.; Salih, R.Q.; Ali, R.K.; Salh, A.M.; et al. Post COVID-19 pulmonary fibrosis; a meta-analysis study. Ann. Med. Surg. 2022, 77, 103590. [Google Scholar] [CrossRef]
- Ojo, A.S.; Balogun, S.A.; Williams, O.T.; Ojo, O.S. Pulmonary Fibrosis in COVID-19 Survivors: Predictive Factors and Risk Reduction Strategies. Pulm. Med. 2020, 2020, 6175964. [Google Scholar] [CrossRef] [PubMed]
- Hui, D.S.; Wong, K.T.; Ko, F.W.; Tam, L.S.; Chan, D.P.; Woo, J.; Sung, J.J. The 1-Year Impact of Severe Acute Respiratory Syndrome on Pulmonary Function, Exercise Capacity, and Quality of Life in a Cohort of Survivors. Chest 2005, 128, 2247–2261. [Google Scholar] [CrossRef] [PubMed]
- Duong-Quy, S.; Vo-Pham-Minh, T.; Tran-Xuan, Q.; Huynh-Anh, T.; Vo-Van, T.; Vu-Tran-Thien, Q.; Nguyen-Nhu, V. Post-COVID-19 Pulmonary Fibrosis: Facts—Challenges and Futures: A Narrative Review. Pulm. Ther. 2023, 9, 295–307. [Google Scholar] [CrossRef] [PubMed]
- McGroder, C.F.; Zhang, D.; Choudhury, M.A.; Salvatore, M.M.; D’Souza, B.M.; Hoffman, E.A.; Wei, Y.; Baldwin, M.R.; Garcia, C.K. Pulmonary fibrosis 4 months after COVID-19 is associated with severity of illness and blood leucocyte telomere length. Thorax 2021, 76, 1242–1245. [Google Scholar] [CrossRef] [PubMed]
- Sturgill, J.L.; Mayer, K.P.; Kalema, A.G.; Dave, K.; Mora, S.; Kalantar, A.; Carter, D.J.; Montgomery-Yates, A.A.; Morris, P.E. Post-intensive care syndrome and pulmonary fibrosis in patients surviving ARDS-pneumonia of COVID-19 and non-COVID-19 etiologies. Sci. Rep. 2023, 13, 6554. [Google Scholar] [CrossRef]
- Kligerman, S.J.; Franks, T.J.; Galvin, J.R. From the Radiologic Pathology Archives: Organization and Fibrosis as a Response to Lung Injury in Diffuse Alveolar Damage, Organizing Pneumonia, and Acute Fibrinous and Organizing Pneumonia. RadioGraphics 2013, 33, 1951–1975. [Google Scholar] [CrossRef]
- Tran, S.; Ksajikian, A.; Overbey, J.; Li, P.; Li, Y. Pathophysiology of Pulmonary Fibrosis in the Context of COVID-19 and Implications for Treatment: A Narrative Review. Cells 2022, 11, 2489. [Google Scholar] [CrossRef]
- ARDS Definition of Task Force; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- Cabrera-Benitez, N.E.; Laffey, J.G.; Parotto, M.; Spieth, P.M.; Villar, J.; Zhang, H.; Slutsky, A.S. Mechanical ventilation-associated lung fibrosis in acute respiratory distress syndrome: A significant contributor to poor outcome. Anesthesiology 2014, 121, 189–198. [Google Scholar] [CrossRef]
- Michalski, J.E.; Kurche, J.S.; Schwartz, D.A. From ARDS to pulmonary fibrosis: The next phase of the COVID-19 pandemic? Transl. Res. 2022, 241, 13–24. [Google Scholar] [CrossRef]
- Zirpe, K.G.; Tiwari, A.M.; Gurav, S.K.; Deshmukh, A.M.; Suryawanshi, P.B.; Wankhede, P.P.; Kapse, U.S.; Bhoyar, A.P.; Khan, A.Z.; Malhotra, R.V.; et al. Timing of Invasive Mechanical Ventilation and Mortality among Patients with Severe COVID-19-associated Acute Respiratory Distress Syndrome. Indian J. Crit. Care Med. 2021, 25, 493–498. [Google Scholar] [CrossRef] [PubMed]
- Kangelaris, K.N.M.; Ware, L.B.; Wang, C.Y.M.; Janz, D.R.M.; Zhuo, H.; Matthay, M.A.; Calfee, C.S.M. Timing of Intubation and Clinical Outcomes in Adults With Acute Respiratory Distress Syndrome*. Crit. Care Med. 2016, 44, 120–129. [Google Scholar] [CrossRef]
- Wunsch, H. Mechanical Ventilation in COVID-19: Interpreting the Current Epidemiology. Am. J. Respir. Crit. Care Med. 2020, 202, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Lu, X.; Li, Y.; Chen, H.; Chen, T.; Su, N.; Huang, F.; Zhou, J.; Zhang, B.; Yan, F.; et al. Clinical Course and Outcomes of 344 Intensive Care Patients with COVID-19. Am. J. Respir. Crit. Care Med. 2020, 201, 1430–1434. [Google Scholar] [CrossRef]
- Udi, J.; Lang, C.N.; Zotzmann, V.; Krueger, K.; Fluegler, A.; Bamberg, F.; Bode, C.; Duerschmied, D.; Wengenmayer, T.; Staudacher, D.L. Incidence of Barotrauma in Patients With COVID-19 Pneumonia During Prolonged Invasive Mechanical Ventilation—A Case-Control Study. J. Intensiv. Care Med. 2020, 36, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Sirayder, U.; Inal-Ince, D.; Kepenek-Varol, B.; Acik, C. Long-Term Characteristics of Severe COVID-19: Respiratory Function, Functional Capacity, and Quality of Life. Int. J. Environ. Res. Public Health 2022, 19, 6304. [Google Scholar] [CrossRef]
- Seymour, C.W.; Liu, V.X.; Iwashyna, T.J.; Brunkhorst, F.M.; Rea, T.D.; Scherag, A.; Rubenfeld, G.; Kahn, J.M.; Shankar-Hari, M.; Singer, M.; et al. Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 762–774. [Google Scholar] [CrossRef]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Barkauskas, C.E.; Cronce, M.J.; Rackley, C.R.; Bowie, E.J.; Keene, D.R.; Stripp, B.R.; Randell, S.H.; Noble, P.W.; Hogan, B.L.M. Type 2 alveolar cells are stem cells in adult lung. J. Clin. Investig. 2013, 123, 3025–3036. [Google Scholar] [CrossRef]
- Zou, X.; Chen, K.; Zou, J.; Han, P.; Hao, J.; Han, Z. Single-cell RNA-seq data analysis on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable to 2019-nCoV infection. Front. Med. 2020, 14, 185–192. [Google Scholar] [CrossRef]
- Hamming, I.; Timens, W.; Bulthuis, M.L.C.; Lely, A.T.; Navis, G.J.; van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Sungnak, W.; Huang, N.; Becavin, C.; Berg, M.; Queen, R.; Litvinukova, M.; Talavera-Lopez, C.; Maatz, H.; Reichart, D.; Sampaziotis, F.; et al. HCA Lung Biological Network. SARS-CoV-2 entry factors are highly expressed in nasal epithelial cells together with innate immune genes. Nat. Med. 2020, 26, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Kakamad, F.H.; Mahmood, S.O.; Rahim, H.M.; Abdulla, B.A.; Abdullah, H.O.; Othman, S.; Mohammed, S.H.; Kakamad, S.H.; Mustafa, S.M.; Salih, A.M. Post covid-19 invasive pulmonary Aspergillosis: A case report. Int. J. Surg. Case Rep. 2021, 82, 105865. [Google Scholar] [CrossRef] [PubMed]
- Venkataraman, T.; Frieman, M.B. The role of epidermal growth factor receptor (EGFR) signaling in SARS coronavirus-induced pulmonary fibrosis. Antivir. Res. 2017, 143, 142–150. [Google Scholar] [CrossRef]
- Mo, X.; Jian, W.; Su, Z.; Chen, M.; Peng, H.; Peng, P.; Lei, C.; Chen, R.; Zhong, N.; Li, S. Abnormal pulmonary function in COVID-19 patients at time of hospital discharge. Eur. Respir. J. 2020, 55, 2001217. [Google Scholar] [CrossRef]
- Frija-Masson, J.; Debray, M.-P.; Gilbert, M.; Lescure, F.-X.; Travert, F.; Borie, R.; Khalil, A.; Crestani, B.; D’Ortho, M.-P.; Bancal, C. Functional characteristics of patients with SARS-CoV-2 pneumonia at 30 days post-infection. Eur. Respir. J. 2020, 56, 2001754. [Google Scholar] [CrossRef]
- Stoian, A.; Motataianu, A.; Bajko, Z.; Balasa, A. Guillain–Barré and Acute Transverse Myelitis Overlap Syndrome Following Obstetric Surgery. J. Crit. Care Med. 2020, 6, 74–79. [Google Scholar] [CrossRef]
- Ahmed, O.F.; Kakamad, F.H.; Amin, B.J.H.; Abdullah, B.A.; Hassan, M.N.; Salih, R.Q.; Mohammed, S.H.; Othman, S.; Ahmed, G.S.; Salih, A.M. Post COVID-19 pulmonary complications; a single center experience. Ann. Med. Surg. 2021, 72, 103052. [Google Scholar] [CrossRef]
- Antonio, G.E.; Wong, K.T.; Hui, D.S.C.; Wu, A.; Lee, N.; Yuen, E.H.Y.; Leung, C.B.; Rainer, T.H.; Cameron, P.; Chung, S.S.C.; et al. Thin-Section CT in Patients with Severe Acute Respiratory Syndrome Following Hospital Discharge: Preliminary Experience. Radiology 2003, 228, 810–815. [Google Scholar] [CrossRef]
- Ambardar, S.R.; Hightower, S.L.; Huprikar, N.A.; Chung, K.K.; Singhal, A.; Collen, J.F. Post-COVID-19 Pulmonary Fibrosis: Novel Sequelae of the Current Pandemic. J. Clin. Med. 2021, 10, 2452. [Google Scholar] [CrossRef]
- Crooks, M.G.; Hart, S.P. Coagulation and anticoagulation in idiopathic pulmonary fibrosis. Eur. Respir. Rev. 2015, 24, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Aquino-Gálvez, A.; González-Ávila, G.; Jiménez-Sánchez, L.L.; Maldonado-Martínez, H.A.; Cisneros, J.; Toscano-Marquez, F.; Castillejos-López, M.; Torres-Espíndola, L.M.; Velázquez-Cruz, R.; Rodríguez, V.H.O.; et al. Dysregulated expression of hypoxia-inducible factors augments myofibroblasts differentiation in idiopathic pulmonary fibrosis. Respir. Res. 2019, 20, 130. [Google Scholar] [CrossRef] [PubMed]
- Chen, I.-T.; Huang, L.-T.; Chen, C.-C.; Chen, C.-M. Molecular mechanisms underlying hyperoxia-induced lung fibrosis. Pediatr. Neonatol. 2022, 63, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Mach, W.J.; Thimmesch, A.R.; Pierce, J.T.; Pierce, J.D. Consequences of Hyperoxia and the Toxicity of Oxygen in the Lung. Nurs. Res. Pr. 2011, 2011, 260482. [Google Scholar] [CrossRef]
- Chernyak, B.V.; Popova, E.N.; Prikhodko, A.S.; Grebenchikov, O.A.; Zinovkina, L.A.; Zinovkin, R.A. COVID-19 and Oxidative Stress. Biochemistry 2020, 85, 1543–1553. [Google Scholar] [CrossRef]
- Fukumoto, J.; Leung, J.; Cox, R.; Czachor, A.; Parthasarathy, P.T.; Lagishetty, V.; Mandry, M.; Hosseinian, N.; Patel, P.; Perry, B.; et al. Oxidative stress induces club cell proliferation and pulmonary fibrosis in Atp8b1 mutant mice. Aging 2019, 11, 209–229. [Google Scholar] [CrossRef]
- Voshaar, T.; Stais, P.; Köhler, D.; Dellweg, D. Conservative management of COVID-19 associated hypoxaemia. ERJ Open Res. 2021, 7, 00026–02021. [Google Scholar] [CrossRef]
- Vianello, A.; Guarnieri, G.; Braccioni, F.; Lococo, S.; Molena, B.; Cecchetto, A.; Giraudo, C.; De Marchi, L.B.; Caminati, M.; Senna, G. The pathogenesis, epidemiology and biomarkers of susceptibility of pulmonary fibrosis in COVID-19 survivors. Clin. Chem. Lab. Med. 2021, 60, 307–316. [Google Scholar] [CrossRef]
- John, A.E.; Joseph, C.; Jenkins, G.; Tatler, A.L. COVID-19 and pulmonary fibrosis: A potential role for lung epithelial cells and fibroblasts. Immunol. Rev. 2021, 302, 228–240. [Google Scholar] [CrossRef]
- Xu, J.; Gonzalez, E.T.; Iyer, S.S.; Mac, V.; Mora, A.L.; Sutliff, R.L.; Reed, A.; Brigham, K.L.; Kelly, P.; Rojas, M. Use of Senescence-Accelerated Mouse Model in Bleomycin-Induced Lung Injury Suggests That Bone Marrow-Derived Cells Can Alter the Outcome of Lung Injury in Aged Mice. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64, 731–739. [Google Scholar] [CrossRef]
- Cilli, A.; Hanta, I.; Uzer, F.; Coskun, F.; Sevinc, C.; Deniz, P.P.; Parlak, M.; Altunok, E.; Tertemiz, K.C.; Ursavas, A. Characteristics and outcomes of COVID-19 patients with IPF: A multi-center retrospective study. Respir. Med. Res. 2022, 81, 100900. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Shen, C.; Wang, L.; Majumder, S.; Zhang, D.; Deen, M.J.; Li, Y.; Qing, L.; Zhang, Y.; Chen, C.; et al. Pulmonary fibrosis and its related factors in discharged patients with new corona virus pneumonia: A cohort study. Respir. Res. 2021, 22, 203. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. RETRACTED: 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Rajagopal, K.; Bryant, A.J.; Sahay, S.; Wareing, N.; Zhou, Y.; Pandit, L.M.; Karmouty-Quintana, H. Idiopathic pulmonary fibrosis and pulmonary hypertension: Heracles meets the Hydra. Br. J. Pharmacol. 2021, 178, 172–186. [Google Scholar] [CrossRef]
- Jdiaa, S.S.; Mansour, R.; El Alayli, A.; Gautam, A.; Thomas, P.; Mustafa, R.A. COVID-19 and chronic kidney disease: An updated overview of reviews. J. Nephrol. 2022, 35, 69–85. [Google Scholar] [CrossRef] [PubMed]
- Zou, J.-N.; Sun, L.; Wang, B.-R.; Zou, Y.; Xu, S.; Ding, Y.-J.; Shen, L.-J.; Huang, W.-C.; Jiang, X.-J.; Chen, S.-M. The characteristics and evolution of pulmonary fibrosis in COVID-19 patients as assessed by AI-assisted chest HRCT. PLoS ONE 2021, 16, e0248957. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Grasselli, G.; Pesenti, A.; Cecconi, M. Critical Care Utilization for the COVID-19 Outbreak in Lombardy, Italy: Early experience and forecast during an emergency response. JAMA 2020, 323, 1545–1546. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. China Medical Treatment Expert Group for Covid-19. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Aul, R.; Gates, J.; Draper, A.; Dunleavy, A.; Ruickbie, S.; Meredith, H.; Walters, N.; van Zeller, C.; Taylor, V.; Bridgett, M.; et al. Complications after discharge with COVID-19 infection and risk factors associated with development of post-COVID pulmonary fibrosis. Respir. Med. 2021, 188, 106602. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.; Liu, Y.; Xu, D.; Zhang, R.; Lan, L.; Xu, H. Prediction of the Development of Pulmonary Fibrosis Using Serial Thin-Section CT and Clinical Features in Patients Discharged after Treatment for COVID-19 Pneumonia. Korean J. Radiol. 2020, 21, 746–755. [Google Scholar] [CrossRef] [PubMed]
- Torres-Castro, R.; Vasconcello-Castillo, L.; Alsina-Restoy, X.; Solis-Navarro, L.; Burgos, F.; Puppo, H.; Vilaró, J. Respiratory function in patients post-infection by COVID-19: A systematic review and meta-analysis. Pulmonology 2020, 27, 328–337. [Google Scholar] [CrossRef] [PubMed]
- Stoian, A.; Bajko, Z.; Maier, S.; Cioflinc, R.A.; Grigorescu, B.L.; Moțățăianu, A.; Bărcuțean, L.; Balașa, R.; Stoian, M. High-dose intravenous immunoglobulins as a therapeutic option in critical illness polyneuropathy accompanying SARS-CoV-2 infection: A case-based review of the literature (Review). Exp. Ther. Med. 2021, 22, 1182. [Google Scholar] [CrossRef] [PubMed]
- Stoian, A.; Moțățăianu, A.; Bărcuțean, L.; Maier, S.; Bajko, Z.; Voidăzan, S.; Fărcaș, A.; Bălașa, R. Understandig the mechanism of action of intravenous immunoglobulins: A ten years’ experience in treating Guillain Barrésyndrome. Farmacia 2020, 68, 426–435. [Google Scholar] [CrossRef]
- Papazian, L.; Doddoli, C.; Chetaille, B.; Gernez, Y.; Thirion, X.; Roch, A.; Donati, Y.; Bonnety, M.; Zandotti, C.; Thomas, P. A contributive result of open-lung biopsy improves survival in acute respiratory distress syndrome patients. Crit. Care Med. 2007, 35, 755–762. [Google Scholar] [CrossRef]
- Madtes, D.K.; Rubenfeld, G.; Klima, L.D.; Milberg, J.A.; Steinberg, K.P.; Martin, T.R.; Raghu, G.; Hudson, L.D.; Clark, J.G. Elevated Transforming Growth Factor- alpha Levels in Bronchoalveolar Lavage Fluid of Patients with Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 1998, 158, 424–430. [Google Scholar] [CrossRef]
- Martin, C.; Papazian, L.; Payan, M.-J.; Saux, P.; Gouin, F. Pulmonary fibrosis correlates with outcome in adult respiratory distress syndrome. A study in mechanically ventilated patients. Chest 1995, 107, 196–200. [Google Scholar] [CrossRef]
- Li, H.-H.; Wang, C.-W.; Chang, C.-H.; Huang, C.-C.; Hsu, H.-S.; Chiu, L.-C. Relationship between Mechanical Ventilation and Histological Fibrosis in Patients with Acute Respiratory Distress Syndrome Undergoing Open Lung Biopsy. J. Pers. Med. 2022, 12, 474. [Google Scholar] [CrossRef]
- Copland, I.B.; Reynaud, D.; Pace-Asciak, C.; Post, M. Mechanotransduction of stretch-induced prostanoid release by fetal lung epithelial cells. Am. J. Physiol. Lung Cell Mol. Physiol. 2006, 291, L487–L495. [Google Scholar] [CrossRef]
- Cavanaugh, K.J., Jr.; Oswari, J.; Margulies, S.S. Role of Stretch on Tight Junction Structure in Alveolar Epithelial Cells. Am. J. Respir. Cell Mol. Biol. 2001, 25, 584–591. [Google Scholar] [CrossRef]
- Heise, R.L.; Stober, V.; Cheluvaraju, C.; Hollingsworth, J.W.; Garantziotis, S. Mechanical Stretch Induces Epithelial-Mesenchymal Transition in Alveolar Epithelia via Hyaluronan Activation of Innate Immunity. J. Biol. Chem. 2011, 286, 17435–17444. [Google Scholar] [CrossRef] [PubMed]
- Parker, J.C.; Breen, E.C.; West, J.B.; Maina, J.N.; Farias, L.L.; Faffe, D.S.; Xisto, D.G.; Santana, M.C.E.; Lassance, R.; Prota, L.F.M.; et al. High vascular and airway pressures increase interstitial protein mRNA expression in isolated rat lungs. J. Appl. Physiol. 1997, 83, 1697–1705. [Google Scholar] [CrossRef]
- Tschumperlin, D.J.; Dai, G.; Maly, I.V.; Kikuchi, T.; Laiho, L.H.; McVittie, A.K.; Haley, K.J.; Lilly, C.M.; So, P.T.C.; Lauffenburger, D.A.; et al. Mechanotransduction through growth-factor shedding into the extracellular space. Nature 2004, 429, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Schild, C.; Trueb, B. Mechanical Stress Is Required for High-Level Expression of Connective Tissue Growth Factor. Exp. Cell Res. 2002, 274, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Garcia, C.S.; Rocco, P.R.; Facchinetti, L.D.; Lassance, R.M.; Caruso, P.; Deheinzelin, D.; Morales, M.M.; Romero, P.V.; Faffe, D.S.; Zin, W.A. What increases type III procollagen mRNA levels in lung tissue: Stress induced by changes in force or amplitude? Respir. Physiol. Neurobiol. 2004, 144, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Cruz, F.F.; Rocco, P.R.M.; Pelosi, P. Role of the extracellular matrix in the genesis of ventilator-induced lung injury. Med. Klin. Intensiv. Notfmed. 2018, 113 (Suppl. 1), 2–6. [Google Scholar] [CrossRef]
- Tatler, A.L.; Jenkins, G. TGF-β Activation and Lung Fibrosis. Proc. Am. Thorac. Soc. 2012, 9, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Berg, J.T.; Fu, Z.; Breen, E.C.; Tran, H.-C.; Mathieu-Costello, O.; West, J.B.; Leuenberger, A.; Gazdhar, A.; Herrmann, G.; Ochs, M.; et al. High lung inflation increases mRNA levels of ECM components and growth factors in lung parenchyma. J. Appl. Physiol. 1997, 83, 120–128. [Google Scholar] [CrossRef]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. COVID-19 Lombardy ICU Network. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581, Erratum in JAMA 2021, 325, 2120. [Google Scholar] [CrossRef]
- Desai, S.R.; Wells, A.U.; Rubens, M.B.; Evans, T.W.; Hansell, D.M. Acute Respiratory Distress Syndrome: CT Abnormalities at Long-term Follow-up. Radiology 1999, 210, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Stoian, A.; Bălașa, R.; Grigorescu, B.L.; Maier, S.; Andone, S.; Cocuz, I.G.; Bajko, Z.; Filep, C.R.; Stoian, M. Guillain-Barré syndrome associated with Covid-19: A close relationship or just a coincidence? (Review). Exp. Ther. Med. 2021, 22, 916. [Google Scholar] [CrossRef]
- Nabahati, M.; Ebrahimpour, S.; Khaleghnejad Tabari, R.; Mehraeen, R. Post-COVID-19 pulmonary fibrosis and its predictive factors: A prospective study. Egypt J. Radiol. Nucl. Med. 2021, 52, 248. [Google Scholar] [CrossRef]
- Fang, Y.; Zhou, J.; Ding, X.; Ling, G.; Yu, S. Pulmonary fibrosis in critical ill patients recovered from COVID-19 pneumonia: Preliminary experience. Am. J. Emerg. Med. 2020, 38, 2134–2138. [Google Scholar] [CrossRef] [PubMed]
- Ali, R.M.M.; Ghonimy, M.B.I. Post-COVID-19 pneumonia lung fibrosis: A worrisome sequelae in surviving patients. Egypt J. Radiol. Nucl. Med. 2021, 52, 101. [Google Scholar] [CrossRef]
- Udwadia, Z.; Pokhariyal, P.; Tripathi, A.R.; Kohli, A. Fibrotic interstitial lung disease occurring as sequelae of COVID-19 pneumonia despite concomitant steroids. Lung India 2021, 38 (Suppl. 1). [Google Scholar] [CrossRef] [PubMed]
- Patrucco, F.; Solidoro, P.; Gavelli, F.; Apostolo, D.; Bellan, M. Idiopathic Pulmonary Fibrosis and Post-COVID-19 Lung Fibrosis: Links and Risks. Microorganisms 2023, 11, 895. [Google Scholar] [CrossRef] [PubMed]
- Zumla, A.; Hui, D.S.; Azhar, E.I.; Memish, Z.A.; Maeurer, M. Reducing mortality from 2019-nCoV: Host-directed therapies should be an option. Lancet 2020, 395, e35–e36. [Google Scholar] [CrossRef]
- Strieter, R.M.; Mehrad, B. New Mechanisms of Pulmonary Fibrosis. Chest 2009, 136, 1364–1370. [Google Scholar] [CrossRef]
- Wang, J.; Wang, B.J.; Yang, J.C.; Wang, M.Y.; Chen, C.; Luo, G.X.; He, W.F. Research advances in the mechanism of pulmonary fibrosis induced by coronavirus disease 2019 and the corresponding therapeutic measures. Zhonghua Shao Shang Za Zhi 2020, 36, 691–697. (In Chinese) [Google Scholar] [CrossRef]
- Romagnani, S. Th1/Th2 Cells. Inflamm. Bowel Dis. 1999, 5, 285–294. [Google Scholar] [CrossRef] [PubMed]
- Guglani, L.; A Khader, S. Th17 cytokines in mucosal immunity and inflammation. Curr. Opin. HIV AIDS 2010, 5, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Fontanet, A.; Zhang, P.-H.; Zhan, L.; Xin, Z.-T.; Baril, L.; Tang, F.; Lv, H.; Cao, W.-C. Two-Year Prospective Study of the Humoral Immune Response of Patients with Severe Acute Respiratory Syndrome. J. Infect. Dis. 2006, 193, 792–795. [Google Scholar] [CrossRef] [PubMed]
- Martinez, F.O.; Helming, L.; Gordon, S. Alternative Activation of Macrophages: An Immunologic Functional Perspective. Annu. Rev. Immunol. 2009, 27, 451–483. [Google Scholar] [CrossRef] [PubMed]
- Pechkovsky, D.V.; Prasse, A.; Kollert, F.; Engel, K.M.; Dentler, J.; Luttmann, W.; Friedrich, K.; Müller-Quernheim, J.; Zissel, G. Alternatively activated alveolar macrophages in pulmonary fibrosis—Mediator production and intracellular signal transduction. Clin. Immunol. 2010, 137, 89–101. [Google Scholar] [CrossRef]
- Mohammadi, A.; Balan, I.; Yadav, S.; Matos, W.F.; Kharawala, A.; Gaddam, M.; Sarabia, N.; Koneru, S.C.; Suddapalli, S.K.; Marzban, S. Post-COVID-19 Pulmonary Fibrosis. Cureus 2022, 14, e22770. [Google Scholar] [CrossRef]
- Huang, W.-T.; Akhter, H.; Jiang, C.; MacEwen, M.; Ding, Q.; Antony, V.; Thannickal, V.J.; Liu, R.-M. Plasminogen activator inhibitor 1, fibroblast apoptosis resistance, and aging-related susceptibility to lung fibrosis. Exp. Gerontol. 2015, 61, 62–75. [Google Scholar] [CrossRef]
- Venkataraman, T.; Coleman, C.M.; Frieman, M.B. Overactive epidermal growth factor receptor signaling leads to increased fibrosis after severe acute respiratory syndrome coronavirus infection. J. Virol. 2017, 91, 10–1128. [Google Scholar] [CrossRef]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J.; on behalf of theHLH Across Speciality Collaboration, UK. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Balasa, R.; Maier, S.; Barcutean, L.; Stoian, A.; Motataianu, A. The direct deleterious effect of Th17 cells in the nervous system compartment in multiple sclerosis and experimental autoimmune encephalomyelitis: One possible link between neuroinflammation and neurodegeneration. Rev. Rom. Med. Lab. 2020, 28, 9–17. [Google Scholar] [CrossRef]
- Maier, S.; Moțățăianu, A.; Bărcuțean, L.; Balint, A.; Huțanu, A.; Bajko, Z.; Stoian, A.; Andone, S.; Bălașa, R. Interferon β 1A, an immunomodulator in relapsing remitting multiple sclerosis patients: The effect on pro inflammatory cytokines. Farmacia 2020, 68, 65–75. [Google Scholar] [CrossRef]
- Wilson, M.S.; Wynn, T.A. Pulmonary fibrosis: Pathogenesis, etiology and regulation. Mucosal Immunol. 2009, 2, 103–121. [Google Scholar] [CrossRef] [PubMed]
- Grommes, J.; Soehnlein, O. Contribution of Neutrophils to Acute Lung Injury. Mol. Med. 2010, 17, 293–307. [Google Scholar] [CrossRef]
- Malech, H.L.; Gallin, J.I. Current concepts: Immunology. Neutrophils in human diseases. N. Engl. J. Med. 1987, 317, 687–694. [Google Scholar] [CrossRef] [PubMed]
- Leng, L.; Cao, R.; Ma, J.; Mou, D.; Zhu, Y.; Li, W.; Lv, L.; Gao, D.; Zhang, S.; Gong, F.; et al. Pathological features of COVID-19-associated lung injury: A preliminary proteomics report based on clinical samples. Signal Transduct. Target. Ther. 2020, 5, 240. [Google Scholar] [CrossRef] [PubMed]
- Inoue, Y.; Kaner, R.J.; Guiot, J.; Maher, T.M.; Tomassetti, S.; Moiseev, S.; Kuwana, M.; Brown, K.K. Diagnostic and Prognostic Biomarkers for Chronic Fibrosing Interstitial Lung Diseases with a Progressive Phenotype. Chest 2020, 158, 646–659. [Google Scholar] [CrossRef]
- Tanni, S.E.; Fabro, A.T.; de Albuquerque, A.; Ferreira, E.V.M.; Verrastro, C.G.Y.; Sawamura, M.V.Y.; Ribeiro, S.M.; Baldi, B.G. Pulmonary fibrosis secondary to COVID-19: A narrative review. Expert Rev. Respir. Med. 2021, 15, 791–803. [Google Scholar] [CrossRef]
- Sgalla, G.; Iovene, B.; Calvello, M.; Ori, M.; Varone, F.; Richeldi, L. Idiopathic pulmonary fibrosis: Pathogenesis and management. Respir. Res. 2018, 19, 32. [Google Scholar] [CrossRef]
- Gentile, F.; Aimo, A.; Forfori, F.; Catapano, G.; Clemente, A.; Cademartiri, F.; Emdin, M.; Giannoni, A. COVID-19 and risk of pulmonary fibrosis: The importance of planning ahead. Eur. J. Prev. Cardiol. 2020, 27, 1442–1446. [Google Scholar] [CrossRef]
- Shukla, A.; Meisler, N.; Cutroneo, K.R. Perspective article: Transforming growth factor-beta: Crossroad of glucocorticoid and bleomycin regulation of collagen synthesis in lung fibroblasts. Wound Repair. Regen 1999, 7, 133–140. [Google Scholar] [CrossRef]
- Ichikado, K.; Muranaka, H.; Gushima, Y.; Kotani, T.; Nader, H.M.; Fujimoto, K.; Johkoh, T.; Iwamoto, N.; Kawamura, K.; Nagano, J.; et al. Fibroproliferative changes on high-resolution CT in the acute respiratory distress syndrome predict mortality and ventilator dependency: A prospective observational cohort study. BMJ Open 2012, 2, e000545. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, L.N.; Slutsky, A.S. Ventilator-induced injury: From barotrauma to biotrauma. Proc. Assoc. Am. Physicians 1998, 110, 482–488. [Google Scholar] [PubMed]
- Cheresh, P.; Kim, S.-J.; Tulasiram, S.; Kamp, D.W. Oxidative stress and pulmonary fibrosis. Biochim. Biophys. Acta (BBA)—Mol. Basis Dis. 2013, 1832, 1028–1040. [Google Scholar] [CrossRef]
- Baum, J.B.; Duffy, H.S. Fibroblasts and Myofibroblasts: What Are We Talking About? J. Cardiovasc. Pharmacol. 2011, 57, 376–379. [Google Scholar] [CrossRef]
- Phan, S. Fibroblast phenotypes in pulmonary fibrosis. Am. J. Respir. Cell Mol. Biol. 2003, 29 (Suppl. 3), S87–S92. [Google Scholar] [PubMed]
- Basil, M.H.; Hantash, B.M.; Zhao, L.; A Knowles, J.; Lorenz, H.P. Adult and fetal wound healing. Front. Biosci. 2008, 13, 51–61. [Google Scholar] [CrossRef]
- Hashimoto, N.; Jin, H.; Liu, T.; Chensue, S.W.; Phan, S.H. Bone marrow–derived progenitor cells in pulmonary fibrosis. J. Clin. Investig. 2004, 113, 243–252. [Google Scholar] [CrossRef]
- Phillips, R.J.; Burdick, M.D.; Hong, K.; Lutz, M.A.; Murray, L.A.; Xue, Y.Y.; Belperio, J.A.; Keane, M.P.; Strieter, R.M. Circulating fibrocytes traffic to the lungs in response to CXCL12 and mediate fibrosis. J. Clin. Investig. 2004, 114, 438–446. [Google Scholar] [CrossRef]
- Quesnel, C.; Piednoir, P.; Gelly, J.; Nardelli, L.; Garnier, M.; Leçon, V.; Lasocki, S.; Bouadma, L.; Philip, I.; Elbim, C.; et al. Alveolar fibrocyte percentage is an independent predictor of poor outcome in patients with acute lung injury*. Crit. Care Med. 2012, 40, 21–28. [Google Scholar] [CrossRef]
- Barrientos, S.; Stojadinovic, O.; Golinko, M.S.; Brem, H.; Tomic-Canic, M. Growth factors and cytokines in wound healing. Wound Repair. Regen 2008, 16, 585–601. [Google Scholar] [CrossRef]
- Raja, R.; Sivamani, K.; Garcia, M.S.; Isseroff, R.R. Wound re-epithelialization: Modulating kerationcyte migration in wound healing. Front. Biosci. 2007, 12, 2849–2868. [Google Scholar] [CrossRef] [PubMed]
- Kooistra, E.J.; Dahm, K.; van Herwaarden, A.E.; Gerretsen, J.; Nuesch Germano, M.; Mauer, K.; Smeets, R.L.; van der Velde, S.; van den Berg, M.J.W.; van der Hoeven, J.G.; et al. Molecular mechanisms and treatment responses of pulmonary fibrosis in severe COVID-19. Respir. Res. 2023, 24, 196. [Google Scholar] [CrossRef] [PubMed]
- Craig, V.J.; Quintero, P.A.; Fyfe, S.E.; Patel, A.S.; Knolle, M.D.; Kobzik, L.; Owen, C.A. Profibrotic Activities for Matrix Metalloproteinase-8 during Bleomycin-Mediated Lung Injury. J. Immunol. 2013, 190, 4283–4296. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Zuo, J.; Tang, W. Phosphodiesterase-4 Inhibitors for the Treatment of Inflammatory Diseases. Front. Pharmacol. 2018, 9, 1048. [Google Scholar] [CrossRef] [PubMed]
- Dülger, S.U.; Mutlu, N.; Ceylan, I.; Özhan, E. The relationship between lung fibrosis, the epidermal growth factor receptor, and disease outcomes in COVID-19 pneumonia: A postmortem evaluation. Clin. Exp. Med. 2023, 23, 1181–1188. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable (n = 56) | Mean ± Standard Deviation (Min–Max) |
|---|---|
| Age (years) | 56.54 ± 12.83 (24–81) |
| APACHE II | 22.41 ± 9.48 (10–45) |
| q-SOFA | 1.96 ± 0.73 (1–3) |
| Variable (n = 56) | Count (Number of Patients) | Percentage (%) |
|---|---|---|
| Sex (Male:Female) | 33:23 | 58.93%:41.07% |
| ICU admission days | ||
| <10 days | 45 | 80.36% |
| ≥10 days | 11 | 19.64% |
| Patients with mechanical ventilation | ||
| <100 h | 15 | 26.79% |
| ≥100 h | 41 | 73.21% |
| Patients with NIMV vs. IMV | ||
| NIMV:IMV | 33:23 | 58.93%:41.07% |
| Oxygen dependency at discharge | 28 | 50% |
| Pulmonary fibrosis | ||
| No fibrosis | 7 | 12.50% |
| Minor–Moderate | 38 | 67.86% |
| Severe | 11 | 19.64% |
| PaO2/FiO2 | ||
| <100 | 15 | 26.79% |
| 100–200 | 32 | 57.14% |
| 200–300 | 8 | 14.29% |
| Comorbidities | ||
| Cardiovascular | 26 | 46.43% |
| Pulmonary | 13 | 23.21% |
| Neurological | 4 | 7.14% |
| Renal | 8 | 14.29% |
| Hematological | 12 | 21.43% |
| Rheumatological | 8 | 14.29% |
| Metabolic syndrome | 31 | 55.36% |
| Endocrine | 5 | 8.93% |
| Other comorbidities | 26 | 46.43% |
| Cut-Off Value | Day 1 (Number of Patients) | Day 3 (Number of Patients) | Evolution | |
|---|---|---|---|---|
| CRP (mg/dL) | <0.5 | 7 | 7 | ↔ |
| ≥0.5 | 49 | 49 | ↔ | |
| Fibrinogen (mg/dL) | <196 | 3 | 3 | ↔ |
| 196–372 | 14 | 16 | ↗ | |
| >372 | 39 | 37 | ↘ | |
| Ferritin (ng/mL) | <300 | 7 | 8 | ↗ |
| ≥300 | 49 | 48 | ↘ | |
| Procalcitonin (ng/mL) | <0.5 | 31 | 32 | ↗ |
| ≥0.5 | 25 | 24 | ↘ | |
| D-Dimers | Negative | 27 | 23 | ↘ |
| Positive | 29 | 33 | ↗ | |
| LDH (U/L) | <220 | 9 | 12 | ↗ |
| ≥220 | 47 | 44 | ↘ | |
| Leucocytes (/mm3) | <4000 | 3 | 2 | ↘ |
| 4000–10000 | 11 | 17 | ↗ | |
| >10000 | 42 | 37 | ↘ | |
| Lymphocytes (%) | <25% | 47 | 46 | ↘ |
| 25–45% | 4 | 9 | ↗ | |
| >45% | 5 | 1 | ↗ | |
| Neutrophils (%) | <40% | 3 | 1 | ↗ |
| 40–75% | 15 | 10 | ↘ | |
| >75% | 38 | 45 | ↗ | |
| AST (U/L) | <34 | 19 | 20 | ↗ |
| ≥34 | 37 | 36 | ↘ | |
| ALT (U/L) | <55 | 27 | 27 | ↔ |
| ≥55 | 29 | 29 | ↔ | |
| Creatinine (mg/dL) | <1 | 38 | 45 | ↗ |
| ≥1 | 18 | 11 | ↘ | |
| Urea (mg/dL) | <55 | 29 | 23 | ↘ |
| ≥55 | 27 | 33 | ↗ | |
| Glucose (mg/dL) | <80 | 0 | 1 | ↗ |
| 80–110 | 15 | 11 | ↘ | |
| >110 | 41 | 44 | ↗ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stoian, M.; Roman, A.; Boeriu, A.; Onișor, D.; Bandila, S.R.; Babă, D.F.; Cocuz, I.; Niculescu, R.; Costan, A.; Laszlo, S.Ș.; et al. Long-Term Radiological Pulmonary Changes in Mechanically Ventilated Patients with Respiratory Failure due to SARS-CoV-2 Infection. Biomedicines 2023, 11, 2637. https://doi.org/10.3390/biomedicines11102637
Stoian M, Roman A, Boeriu A, Onișor D, Bandila SR, Babă DF, Cocuz I, Niculescu R, Costan A, Laszlo SȘ, et al. Long-Term Radiological Pulmonary Changes in Mechanically Ventilated Patients with Respiratory Failure due to SARS-CoV-2 Infection. Biomedicines. 2023; 11(10):2637. https://doi.org/10.3390/biomedicines11102637
Chicago/Turabian StyleStoian, Mircea, Adina Roman, Alina Boeriu, Danusia Onișor, Sergio Rareș Bandila, Dragoș Florin Babă, Iuliu Cocuz, Raluca Niculescu, Anamaria Costan, Sergiu Ștefan Laszlo, and et al. 2023. "Long-Term Radiological Pulmonary Changes in Mechanically Ventilated Patients with Respiratory Failure due to SARS-CoV-2 Infection" Biomedicines 11, no. 10: 2637. https://doi.org/10.3390/biomedicines11102637