
Inadequacy of Vitamin D Does Not Interfere with Body Weight Loss in Women of Reproductive Age after Roux-en-Y Gastric Bypass
 ,
,
Abstract
:1. Introduction
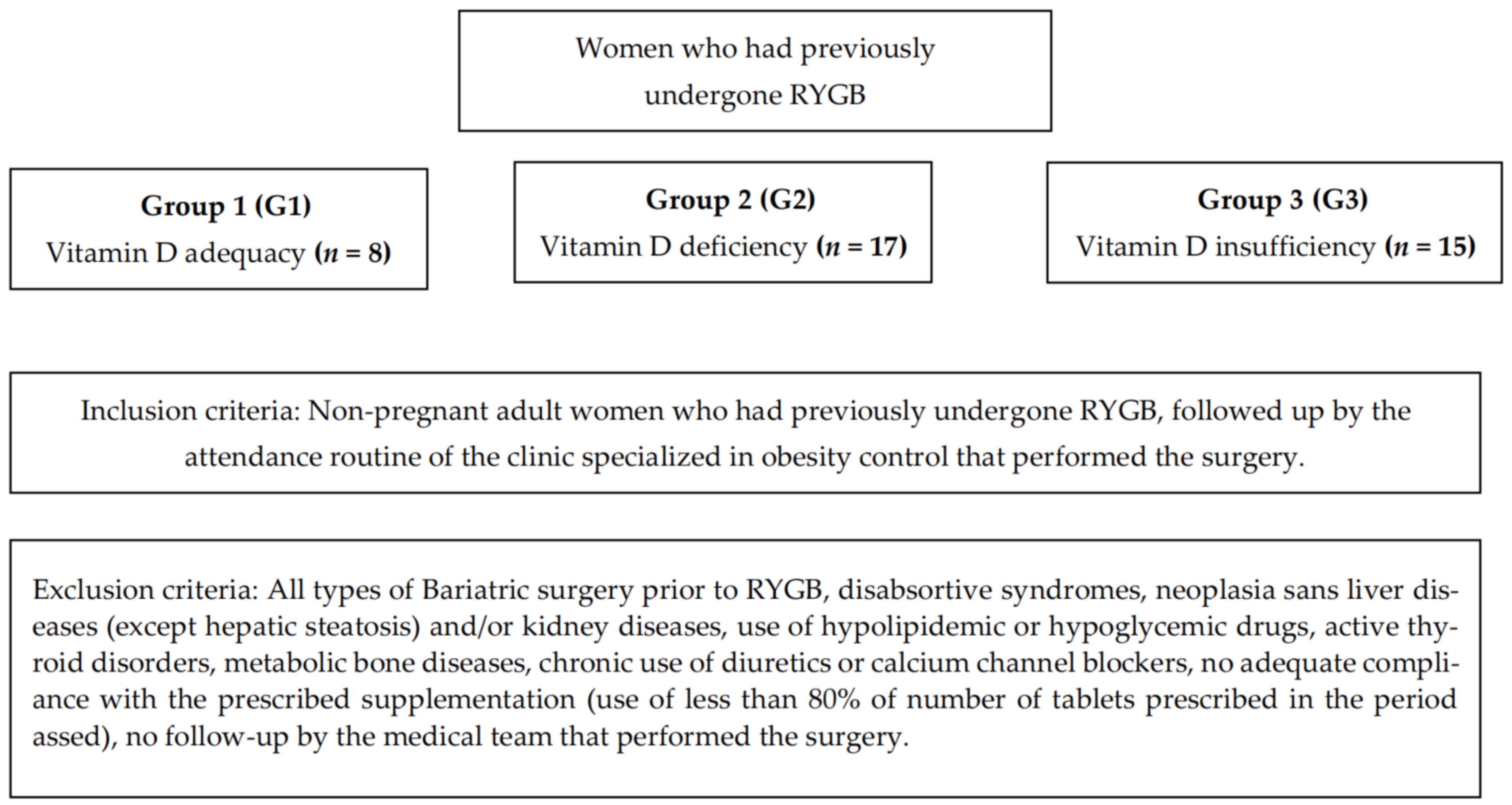
2. Methodology
3. Results
3.1. Sample Characterization and Description of Anthropometric Variables
3.2. Nutritional Status of Vitamin D
3.3. Influence of the Nutritional Status of Vitamin D on Surgical Success, Excess Weight, Weight Loss and Percentage of Weight Loss in the Assessed Times
3.4. Assessment of the Nutritional Status of Vitamin D
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Seidell, J.C.; Halberstadt, J. The global burden of obesity and the challenges of prevention. Ann. Nutr. Metab. 2015, 66, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Erkkola, M.; Kaila, M.; Nwaru, B.I.; Kronberg-Kippila, C.; Ahonen, S.; Nevalainen, J.; Veijola, R.; Pekkanen, J.; Ilonen, J.; Simell, O.; et al. Maternal vitamin D intake during pregnancy is inversely associated with asthma and allergic rhinitis in 5-year old children. Clin. Exp. Allergy 2009, 39, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Buchwald, H.; Oien, D.M. Metabolic/bariatric surgery worldwide 2011. Obes. Surg. 2013, 23, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Schaaf, C.; Gugenheim, J. Impact of Preoperative Serum Vitamin D Level on Postoperative Complications and Excess Weight Loss after Gastric Bypass. Obes. Surg. 2017, 27, 1982–1985. [Google Scholar] [CrossRef] [PubMed]
- Peterson, L.A.; Cheskin, L.J.; Furtado, M.; Papas, K.; Schwetzer, M.A.; Magnuson, T.H.; Steele, K.E. Malnutrition in bariatric surgery candidates: Multiple micronutrient deficiencies prior to surgery. Obes. Surg. 2016, 26, 833–838. [Google Scholar] [CrossRef]
- Wagner, C.L.; Taylor, S.N.; Dawodu, A.; Johnson, D.D.; Hollis, B.W. Vitamin D and its role during pregnancy in attaining optimal health of mother and fetus. Nutrients 2012, 4, 208–230. [Google Scholar] [CrossRef] [Green Version]
- Vanlint, S. Vitamin D and obesity. Nutrients 2013, 5, 949–956. [Google Scholar] [CrossRef] [Green Version]
- Heaney, R.P.; Horst, R.L.; Cullen, D.M.; Armas, L.A. Vitamin D3 distribution and status in the body. J. Am. CollNutr. 2009, 28, 252–256. [Google Scholar]
- Blum, M.; Dolnikowski, G.; Seyoum, E.; Harris, S.S.; Booth, S.L.; Peterson, J.; Saltzman, E.; Dawson-Hughes, B. Vitamin D3 in fat tissue. Endocrine 2008, 33, 90–94. [Google Scholar] [CrossRef]
- Williams, S.E. Metabolic bone disease in the bariatric surgery patient. J. Obes. 2011, 2011, 634614. [Google Scholar] [CrossRef]
- Xanthakos, S. Nutritional deficiencies in obesity and after bariatric surgery. Pediatr. Clin. N. Am. 2010, 56, 1105–1121. [Google Scholar] [CrossRef] [Green Version]
- Cipriani, C.; Pepe, J.; Piemonte, S.; Luciano, C.; Mirella, C.; Salvatore, M. Vitamin D and its relationship with obesity and muscle. Int. J. Endocrinol. 2014, 2014, 841248. [Google Scholar] [CrossRef]
- Borges, J.L.C.; Miranda, I.S.M.; Sarquis, M.M.S.; Borba, V. Obesity, Bariatric Surgery, and Vitamin D. J. Clin. Densitom. Assess. Manag. Musculoskelet. Health 2017, 21, 157–162. [Google Scholar] [CrossRef]
- Mason, C.; Tapsoba, J.; Duggan, C.; Imayama, I.; Wang, C.Y.; Korde, L.; McTiernan, A. Effects of Vitamin D3 Supplementation on Lean Mass, Muscle Strength, and Bone Mineral Density during Weight Loss: A Double-Blind Randomized Controlled Trial. J. Am. Geriatr. Soc. 2016, 64, 769–778. [Google Scholar] [CrossRef] [Green Version]
- Shapses, S.A.; Sukumar, D.; Schneider, S.H.; Schlussel, Y.; Sherrell, R.M.; Field, M.P.; Ambia-Sobhan, H. Vitamin D supplementation and calcium absorption during caloric restriction: A randomized double-blind trial. Am. J. Clin. Nutr. 2013, 97, 637–645. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine (IOM). Weight Gain During Pregnancy: Reexamining the Guidelines; National Academy Press: Washington, DC, USA, 2009. [Google Scholar]
- Organização Mundial da Saúde. Obesity: Preventing and Managing the Global Epidemic; Report of a WHO Consultation on Obesity; World Health Organization: Geneva, Switzerland, 1998. [Google Scholar]
- Gumbs, A.A.; Pomp, A.; Gagner, M. Revisional bariatric surgery for inadequate weight loss. Obes. Surg. 2007, 17, 1137–1145. [Google Scholar] [CrossRef]
- Cummings, D.E.; Overduin, O.; Foster-Schubert, K. Gastric bypass for obesity: Mechanisms of weight loss and diabetes resolution. J. Clin. Endocrinol. Metab. 2010, 89, 2608–2615. [Google Scholar] [CrossRef]
- Rocha, Q.; Mendonça, S.; Fortes, R. Perda Ponderal após Gastroplastia em Y de Roux e importância do acompanhamento nutricional—Uma revisão de literatura. Ciências Saúde 2011, 22, 61–70. [Google Scholar]
- Ferraz, E.M.; Arruda, P.C.L.; Bacelar, T.S.; Ferraz, A.A.B.; Albuquerque, A.C. Tratamento cirúrgico da obesidade mórbida. Ver Col. Bras. Cir. 2003, 30, 98–105. [Google Scholar] [CrossRef]
- Pereira-Santos, M.; Costa, P.R.; Santos, C.A.; Santos, D.B.; Assis, A.M. Obesity and vitamin D deficiency: Is there an association? Obes. Rev. 2016, 17, 484. [Google Scholar] [CrossRef] [PubMed]
- Vimaleswaran, K.S.; Berry, D.J.; Lu, C.; Tikkanen, E.; Pilz, S.; Hirak, L.T. Causal relationship between obesity and vitamin D status: Bi-directional Mendelian randomization analysis of multiple cohorts. PLoS Med. 2013, 10, e1001383. [Google Scholar] [CrossRef] [PubMed]
- Toh, S.Y.; Zarshenas, N.; Jorgensen, J. Prevalence of nutrient deficiencies in bariatric patients. Nutrition. 2009, 25, 1150–1156. [Google Scholar] [CrossRef] [PubMed]
- Costa, T.L.; Paganotto, M.; Radominski, R.B.; Kulak, C.M.; Borba, V.C. Calcium metabolism, vitamin D and bone mineral density after bariatric surgery. Osteoporos. Int. 2015, 26, 757–764. [Google Scholar] [CrossRef] [PubMed]
- Lespessailles, E.; Toumi, H. Vitamin D alteration associated with obesity and bariatric surgery. Exp. Biol. Med. 2017, 242, 1086–1094. [Google Scholar] [CrossRef] [Green Version]
- Mechanick, J.I.; Kushner, R.F.; Sugerman, H.J.; Gonzalez-Campoy, J.M.; Collazo-Clavell, M.L.; Guven, S.; Spitz, A.F.; Apovian, C.M.; Livingston, E.H.; Brolin, R.; et al. American Association of Clinical Endocrinologists, The Obesity Society, and American Society for Metabolic & Bariatric Surgery medical guidelines for clinical practice for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient. Surg. Obes. Relat. Dis. 2009, 17, S3–S72. [Google Scholar]
- Magro, D.O.; Geloneze, B.; Delfini, R.; Pareja, B.C.; Callejas, F.; Pareja, J.C. Long-term weight regain after gastric bypass: A 5-year prospective study. Obes. Surg. 2008, 18, 648–651. [Google Scholar] [CrossRef]
- Soares, A. Perfil dos Indivíduos Com Obesidade Mórbida Submetidos à Cirurgia Bariátrica Pelo SISTEMA Único de SAÚDE no Hospital Universitário da Universidade Federal de Santa Catarina Quanto à Prática de Atividade Física; Universidade Federal de Santa Catarina—UFSC Centro de Desportos—CDS Programa de Pós-Graduação em Educação Física Subárea de Atividade Física Relacionada à Saúde: Florianópolis, Brazil, 2010. [Google Scholar]
- Romacho, T.; Elsen, M.; Rohrborn, D.; Eckel, J. Adipose tissue and its role in organ crosstalk. Acta Physiol. 2014, 210, 733–753. [Google Scholar] [CrossRef]
- Earthman, C.P.; Beckman, L.M.; Masodkar, K.; Sibley, S.D. The link between obesity and low circulating 25-hydroxyvitamin D concentrations: Considerations and implications. Int. J. Obes. 2012, 36, 387–396. [Google Scholar] [CrossRef] [Green Version]
- Savastano, S.; Barrea, L.; Savanelli, M.C.; Nappi, F.; Di Somma, C.; Orio, F.; Colao, A. Low Vitamin D status and obesity: Role of nutritionist. Rev. Endocr. Metab. Disord. 2017, 18, 215–225. [Google Scholar] [CrossRef]


{kind=link}
| Vitamin D3 (ng/mL) | T0 (n = 40) | T1 (n = 40) | T2 (n = 40) | p-Value |
|---|---|---|---|---|
| Mean/Standard deviation | 22.87 ± 9.70 | 24.77 ± 6.96 | 23.75 ± 6.22 | 0.422 |
| % of Adequacy | 20 | 15 | 15 | 0.239 |
| % of Inadequacy | 80 | 85 | 85 | 0.239 |
| % of Insufficiency | 37.5 | 62.5 | 47.5 | 0.787 |
| % of Deficiency | 42.5 | 22.5 | 37.5 | 0.767 |
| Vitamin D3 in the Preoperative (ng/mL) | T0 | T1 | T2 | p-Value |
|---|---|---|---|---|
| G1 | 36.12 ± 9.84 | 23.37 ± 3.06 | 23.65 ± 6.65 | 0.001 * |
| G2 | 14.58 ± 3.85 | 25.17 ± 7.86 | 23.47± 6.56 | <0.001 * |
| G3 | 25.20 ± 2.73 | 25.06 ± 7.63 | 24.20 ± 6.00 | 0.965 |
| p-value | <0.001 * | 0.667 | 0.730 |
| Anthropometric Variables | Vitamin D3 in the Preoperative Period (ng/mL) | |||||||
|---|---|---|---|---|---|---|---|---|
| BMI (kg/m2) | G1 | T1 | G3 | p-value | G1 | T2 | G3 | p-value |
| G2 | G2 | |||||||
| 28.92 ± 4.82 | 27.24 ± 3.00 | 27.49 ± 3.61 | 0.746 | 26.84 ± 1.54 | 24.97 ± 1.93 | 26.63 ± 3.68 | 0.045 * | |
| Surgical success | 62.5% | 88.2% | 80% | 0.324 | 100% | 100% | 93.3% | |
| 0.425 | ||||||||
| Excess weight (kg) | 16.98 ± 13.36 | 14.23 ± 9.02 | 13.92 ± 10.92 | 0.868 | 11.41 ± 4.72 | 7.82 ±6.02 | 11.67 ± 11.59 | 0.248 |
| Weight loss (kg) | 44.63 ± 5.36 | 38.92 ± 7.97 | 41.07 ± 8.15 | 0.208 | 50.21± 11.21 | 45.34 ± 6.11 | 43.32 ± 8.23 | 0.353 |
| % of weight loss | 37.33 ± 5.43 | 34.13 ± 7.35 | 35.84 ± 6.56 | 0.599 | 41.23 ± 4.96 | 39.60 ± 4.80 | 37.81 ± 6.27 | 0.399 |
| Mean Vitamin D3 (ng/mL) | % of Inadequacy/Deficiency of Vitamin D3 (ng/mL) | |||||||
|---|---|---|---|---|---|---|---|---|
| BMI after 1 Year | T0 | T1 | T2 | p-value | T0 | T1 | T2 | p-Value |
| Normal weight | 22.11 ± 5.37 | 25.88 ± 6.03 | 26.88 ± 5.71 | 0.519 | 88.8/44.4 | 88.9/22.2 | 66.7/33.3 | 0.502/0.595 |
| Overweight | 21.71 ± 12.28 | 23.28 ± 7.01 | 21.71 ± 6.05 | 0.556 | 85.7/52.4 | 85.7/23.8 | 94.4/47.6 | 0.225/0.131 |
| Obesity I | 25.55 ± 5.87 | 27.11 ± 7.99 | 25.33 ± 6.30 | 0.947 | 66.7/22.2 | 77.8/22.2 | 77.8/22.2 | 0.980/1 |
| Obesity II | 30 | 25 | 24 | 0.368 | - | 4 | 5.3 | - |
| p-value | 0.205 | 0.655 | 0.143 | 0.304 | 0.981 | 0.361 | ||
| Normal weight | 22.11 ± 5.37 | 25.88 ± 6.03 | 26.88 ± 5.71 | 0.519 | 88.8/44.4 | 88.9/22.2 | 66.7/33.3 | 0.502/0.595 |
| Excess weight | 23.09 ± 10.7 | 24.45 ± 7.27 | 22.83 ± 6.14 | 0.067 | 77.4/41.9 | 83.9/22.6 | 90.3/38.7 | 0.721/0.228 |
| p-value | 0.948 | 0.505 | 0.067 | 0.734 | 0.928 | 0.207 | ||
| BMI after 2 years | T0 | T1 | T2 | p-value | T0 | T1 | T2 | p-value |
| Normal weight | 18.21 ± 5.84 | 23.35 ± 6.61 | 22.57 ± 6.68 | 0.100 | 92.6/64.3 | 85.7/28.6 | 92.9/50 | 0.443/0.163 |
| Overweight | 25.32 ± 10.72 | 25.40 ± 7.26 | 24.16 ± 6.00 | 0.898 | 72.0/32.0 | 84/20 | 84/32.0 | 0.487/0.551 |
| Obesity II | 27.00 | 29.00 | 30.00 | 1 | 100/0 | 100/0 | 0/0 | 0.386/0.223 |
| p-value | 0.039 * | 0.390 | 0.304 | 0.100 | 0.186 | 0.911 | 0.125 | 0.443/0.163 |
| Normal weight | 18.21 ± 5.84 | 23.35 ± 6.61 | 22.57 ± 6.68 | 92.6/64.3 | 85.7/28.6 | 92.9/50 | ||
| Excess weight | 25.38 ± 10.51 | 25.53 ± 7.15 | 24.38 ± 5.99 | 0.363 | 73.1/30.8 | 84.6/19.2 | 80.8/30.8 | 0.670/0.439 |
| p-value | 0.011 * | 0.296 | 0.363 | 0.098 | 0.795 | 0.390 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cruz, S.; Matos, A.C.d.; Cruz, S.P.d.; Pereira, S.; Saboya, C.; Ramalho, A. Inadequacy of Vitamin D Does Not Interfere with Body Weight Loss in Women of Reproductive Age after Roux-en-Y Gastric Bypass. Biomedicines 2023, 11, 86. https://doi.org/10.3390/biomedicines11010086
Cruz S, Matos ACd, Cruz SPd, Pereira S, Saboya C, Ramalho A. Inadequacy of Vitamin D Does Not Interfere with Body Weight Loss in Women of Reproductive Age after Roux-en-Y Gastric Bypass. Biomedicines. 2023; 11(1):86. https://doi.org/10.3390/biomedicines11010086
Chicago/Turabian StyleCruz, Sabrina, Andrea Cardoso de Matos, Suelem Pereira da Cruz, Silvia Pereira, Carlos Saboya, and Andrea Ramalho. 2023. "Inadequacy of Vitamin D Does Not Interfere with Body Weight Loss in Women of Reproductive Age after Roux-en-Y Gastric Bypass" Biomedicines 11, no. 1: 86. https://doi.org/10.3390/biomedicines11010086