
Expression of E4 Protein and HPV Major Capsid Protein (L1) as A Novel Combination in Squamous Intraepithelial Lesions
 , ,
, ,  , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Specimen Collection and Handling
2.2.1. LBC and HPV Genotyping Test
2.2.2. Colposcopy and Punch Biopsy
2.3. Immunohistochemistry
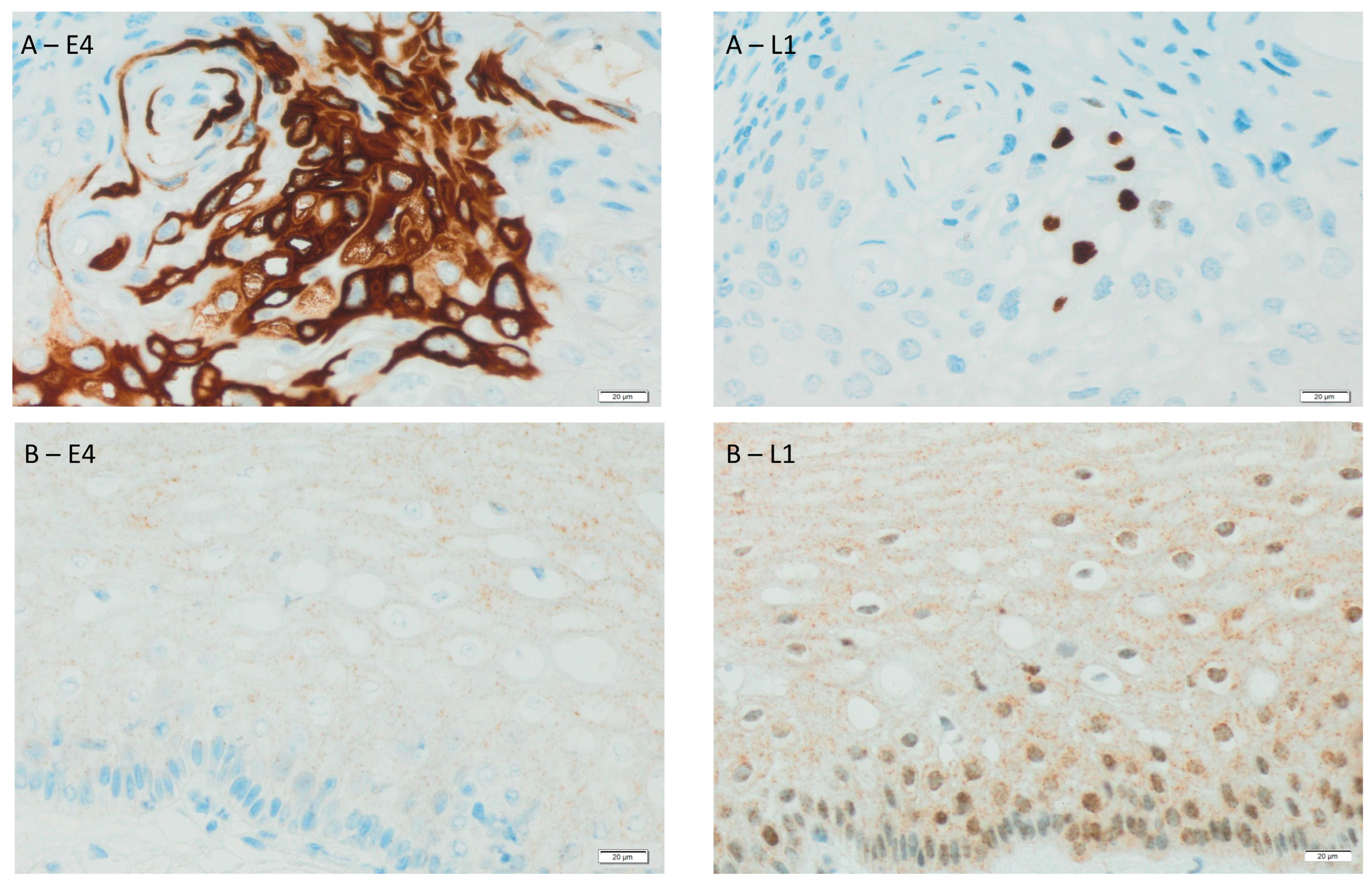
2.3.1. Immunohistochemistry: HPV Major Capsid Protein (L1) and E4 Protein
2.3.2. Light Microscopy Techniques for Cell Imaging
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bernard, H.-U. The clinical importance of the nomenclature, evolution and taxonomy of human papillomaviruses. J. Clin. Virol. 2005, 32, 1–6. [Google Scholar] [CrossRef]
- zur Hausen, H. Papillomaviruses in the causation of human cancers—A brief historical account. Virology 2009, 384, 260–265. [Google Scholar] [CrossRef] [Green Version]
- Chesson, H.W.; Dunne, E.F.; Hariri, S.; Markowitz, L.E. The Estimated Lifetime Probability of Acquiring Human Papillomavirus in the United States. Sex. Transm. Dis. 2014, 41, 660–664. [Google Scholar] [CrossRef]
- Schiller, J.T.; Day, P.M.; Kines, R.C. Current understanding of the mechanism of HPV infection. Gynecol. Oncol. 2010, 118, S12–S17. [Google Scholar] [CrossRef] [Green Version]
- de Villiers, E.-M.; Fauquet, C.; Broker, T.R.; Bernard, H.-U.; zur Hausen, H. Classification of papillomaviruses. Virology 2004, 324, 17–27. [Google Scholar] [CrossRef] [Green Version]
- Doorbar, J. Molecular biology of human papillomavirus infection and cervical cancer. Clin. Sci. 2006, 110, 525–541. [Google Scholar] [CrossRef] [Green Version]
- Perkins, R.B.; Guido, R.S.; Castle, P.E.; Chelmow, D.; Einstein, M.H.; Garcia, F.; Huh, W.K.; Kim, J.J.; Moscicki, A.-B.; Nayar, R.; et al. 2019 ASCCP Risk-Based Management Consensus Guidelines for Abnormal Cervical Cancer Screening Tests and Cancer Precursors. J. Low. Genit. Tract Dis. 2020, 24, 102–131. [Google Scholar] [CrossRef] [Green Version]
- Haręża, D.A.; Wilczyński, J.R.; Paradowska, E. Human Papillomaviruses as Infectious Agents in Gynecological Cancers. Oncogenic Properties of Viral Proteins. Int. J. Mol. Sci. 2022, 23, 1818. [Google Scholar] [CrossRef]
- Broniarczyk, J.; Koczorowska, M.M.; Durzyńska, J.; Warowicka, A.; Goździcka-Józefiak, A. Struktura i właoeciwości wirusa brodawczaka ludzkiego. Biotechnologia 2010, 3, 126–145. [Google Scholar]
- Doorbar, J. Host control of human papillomavirus infection and disease. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 47, 27–41. [Google Scholar] [CrossRef] [Green Version]
- Wilson, R.; Fehrmann, F.; Laimins, L.A. Role of the E1 ∧ E4 Protein in the Differentiation-Dependent Life Cycle of Human Papillomavirus Type 31. J. Virol. 2005, 79, 6732–6740. [Google Scholar] [CrossRef] [PubMed]
- Doorbar, J. The E4 protein; structure, function and patterns of expression. Virology 2013, 445, 80–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vink, F.J.; Dick, S.; Heideman, D.A.M.; De Strooper, L.M.A.; Steenbergen, R.D.M.; Lissenberg-Witte, B.I.; Floore, A.; Bonde, J.H.; Valenčak, A.O.; Poljak, M.; et al. Classification of high-grade cervical intraepithelial neoplasia by p16ink4a, Ki-67, HPV E4 and FAM19A4/miR124-2 methylation status demonstrates considerable heterogeneity with potential consequences for management. Int. J. Cancer 2021, 149, 707–716. [Google Scholar] [CrossRef] [PubMed]
- Doorbar, J. The papillomavirus life cycle. J. Clin. Virol. 2005, 32 (Suppl. 1), 7–15. [Google Scholar] [CrossRef] [PubMed]
- Jach, R.; Mazurec, M.; Trzeszcz, M.; Zimmer, M.; Kedzia, W.; Wolski, H. Cervical cancer screening in Poland in current SARS-CoV-2 pandemic: Interim guidelines of the Polish Society of Gynecologists and Obstetricians and the Polish Society of Colposcopy and Cervical Pathophysiology—A summary January 2021. Ginekol. Polska 2021, 92, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Jach, R.; Mazurec, M.; Trzeszcz, M.; Bartosinska-Dyc, A.; Galarowicz, B.; Kedzia, W.; Nowakowski, A.; Pitynski, K. COLPOSCOPY 2020-COLPOSCOPY protocols a summary of the clinical experts consensus guidelines of the Polish society of colposcopy and cervical pathophysiology and the Polish society of gynecologists and obstetricians. Ginekol. Polska 2020, 91, 362371. [Google Scholar] [CrossRef] [PubMed]
- Chalcarz, M.; Żurawski, J. Injection of Aquafilling® for Breast Augmentation Causes Inflammatory Responses Independent of Visible Symptoms. Aesthetic Plast. Surg. 2020, 45, 481–490. [Google Scholar] [CrossRef]
- Leeman, A.; Jenkins, D.; Del Pino, M.; Ordi, J.; Torné, A.; Doorbar, J.; Meijer, C.J.L.M.; Van Kemenade, F.J.; Quint, W.G.V. Expression of p16 and HPV E4 on biopsy samples and methylation of FAM19A4 and miR124-2 on cervical cytology samples in the classification of cervical squamous intraepithelial lesions. Cancer Med. 2020, 9, 2454–2461. [Google Scholar] [CrossRef]
- Griffin, H.; Soneji, Y.; Van Baars, R.; Arora, R.; Jenkins, D.; van de Sandt, M.; Wu, Z.; Quint, W.; Jach, R.; Okon, K.; et al. Stratification of HPV-induced cervical pathology using the virally encoded molecular marker E4 in combination with p16 or MCM. Mod. Pathol. 2015, 28, 977–993. [Google Scholar] [CrossRef] [Green Version]
- Leeman, A.; Pirog, E.C.; Doorbar, J.; Van De Sandt, M.M.; Van Kemenade, F.J.; Jenkins, D.; Quint, W.G. Presence or Absence of Significant HPVE4 Expression in High-grade Anal Intraepithelial Neoplasia with p16/Ki-67 Positivity Indicates Distinct Patterns of Neoplasia. Am. J. Surg. Pathol. 2018, 42, 463–471. [Google Scholar] [CrossRef]
- van Baars, R.; Griffin, H.; Wu, Z.; Soneji, Y.; van de Sandt, M.M.; Arora, R.; van der Marel, J.; ter Harmsel, B.; Jach, R.; Okon, K.; et al. Investigating Diagnostic Problems of CIN1 and CIN2 Associated with High-risk HPV by Combining the Novel Molecular Biomarker PanHPVE4 with P16INK4a. Am. J. Surg. Pathol. 2015, 39, 1518–1528. [Google Scholar] [CrossRef] [PubMed]
- van Zummeren, M.; Kremer, W.W.; Leeman, A.; Bleeker, M.C.G.; Jenkins, D.; van de Sandt, M.; Doorbar, J.; Heideman, D.A.M.; Steenbergen, R.D.M.; Snijders, P.J.F.; et al. HPV E4 expression and DNA hypermethylation of CADM1, MAL, and miR124-2 genes in cervical cancer and precursor lesions. Mod. Pathol. 2018, 31, 1842–1850. [Google Scholar] [CrossRef] [PubMed]
- Jochmus-Kudielka, I.; Schneider, A.; Braun, R.; Kimmig, R.; Koldovsky, U.; Schneweis, K.E.; Seedorf, K.; Gissmann, L. Antibodies Against the Human Papillomavirus Type 16 Early Proteins in Human Sera: Correlation of Anti-E7 Reactivity with Cervical Cancer. Gynecol. Oncol. 1989, 81, 1698–1704. [Google Scholar] [CrossRef] [PubMed]
- Müller, M.; Viscidi, R.P.; Ulken, V.; Bavinck, J.N.B.; Hill, P.M.; Fisher, S.G.; Reid, R.; Munoz, N.; Schneider, A.; Shah, K.V.; et al. Antibodies to the E4, E6, and E7 Proteins of Human Papillomavirus (HPV) Type 16 in Patients with HPV-Associated Diseases and in the Normal Population. J. Investig. Dermatol. 1995, 104, 138–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Köchel, H.G.; Monazahian, M.; Sievert, K.; Höhne, M.; Thomssen, C.; Teichmann, A.; Arendt, P.; Thomssen, R. Occurrence of antibodies TO L1, L2, E4 and E7 gene products of human papillomavirus types 6b, 16 and 18 among cervical cancer patients and controls. Int. J. Cancer 1991, 48, 682–688. [Google Scholar] [CrossRef] [PubMed]
- Onda, T.; Kanda, T.; Zanma, S.; Yasugi, T.; Watanabe, S.; Kawana, T.; Ueda, K.; Yoshikawai, H.; Taketani, Y.; Yoshiike, K. Association of the antibodies against human papillomavirus 16 E4 and E7 proteins with cervical cancer positive for human papillomavirus DNA. Int. J. Cancer 1993, 54, 624–628. [Google Scholar] [CrossRef] [PubMed]
- Ren, S.; Gaykalova, D.A.; Guo, T.; Favorov, A.V.; Fertig, E.J.; Tamayo, P.; Callejas-Valera, J.L.; Allevato, M.; Gilardi, M.; Santos, J.; et al. HPV E2, E4, E5 drive alternative carcinogenic pathways in HPV positive cancers. Oncogene 2020, 39, 6327–6339. [Google Scholar] [CrossRef]
- Hilfrich, R. HPV L1 Detection as a Prognostic Marker for Management of HPV High Risk Positive Abnormal Pap Smears. In Human Papillomavirus and Related Diseases from Bench to Bedside: A Diagnostic and Preventive Perspective; InTech: London, UK, 2013. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value |
|---|---|
| Mean age | 32.00 |
| Histological outcome | |
| CIN 1 | 38 (44.7%) |
| CIN 2 | 24 (28.2%) |
| CIN 3 | 19 (22.4%) |
| No pathology | 4 (4.7%) |
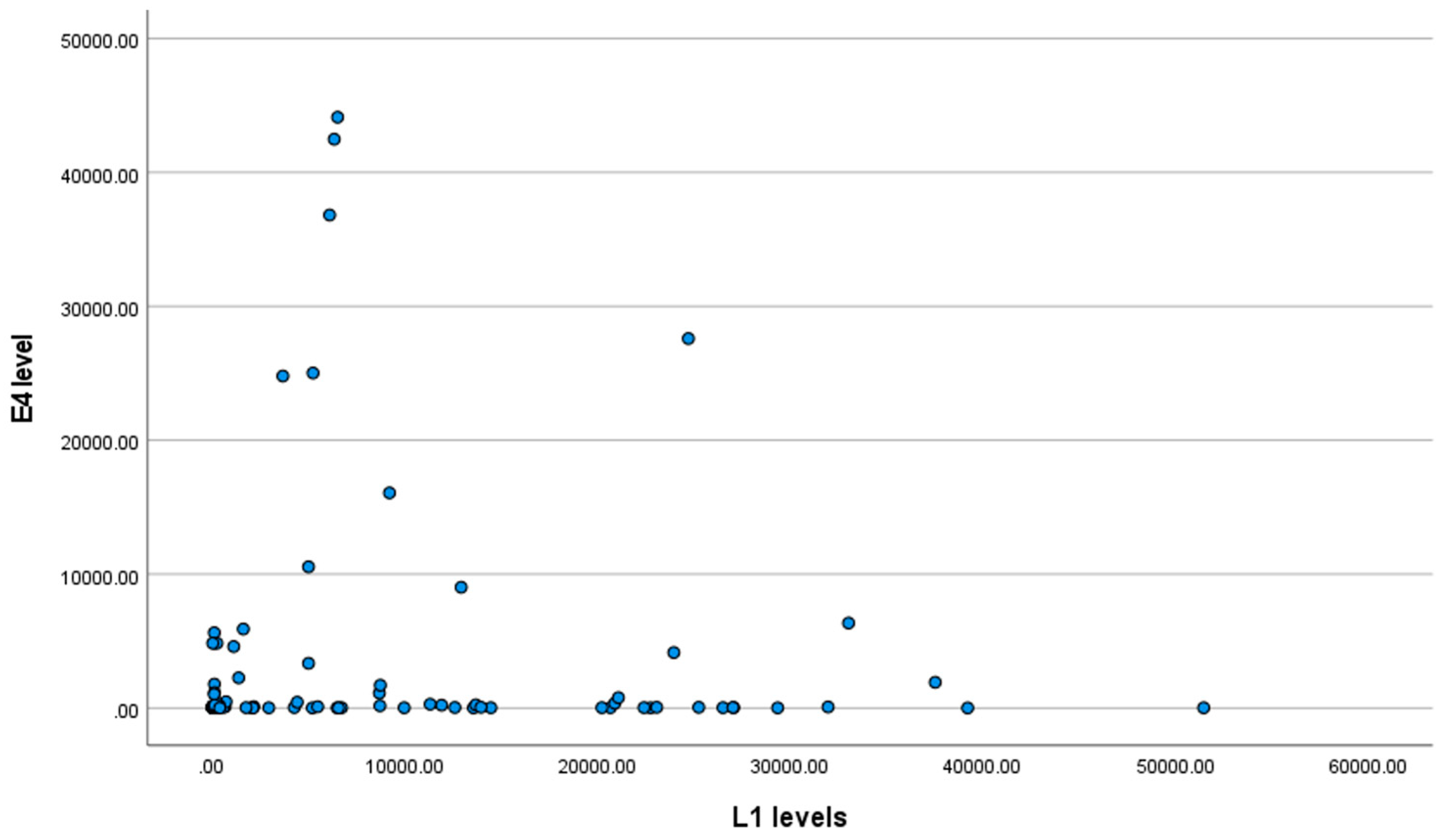
| E4 protein level, Me (Q1; Q3) | 108.02 (35.60; 1712.73) |
| HPV L1 level, Me (Q1; Q3) | 5008.66 (154.65; 13,688.40) |
| LBC result, n (%) | |
| NILM | 3 (3.5%) |
| ASC-US | 15 (17.6%) |
| ASC-H | 16 (18.8%) |
| LSIL | 37 (43.5%) |
| HSIL | 13 (15.3%) |
| None | 1 (1.2%) |
| HPV status | |
| PV (+) | 75 (88.2%) |
| PV (−) | 10 (11.8%) |
| HPV genotype, n (%) | |
| 16 | 40 (53.3%) |
| 18 | 5 (6.7%) |
| 31 | 12 (16.0%) |
| 45 | 4 (5.3%) |
| 6 | 9 (12.0%) |
| Other genotypes | 5 (6.7%) |
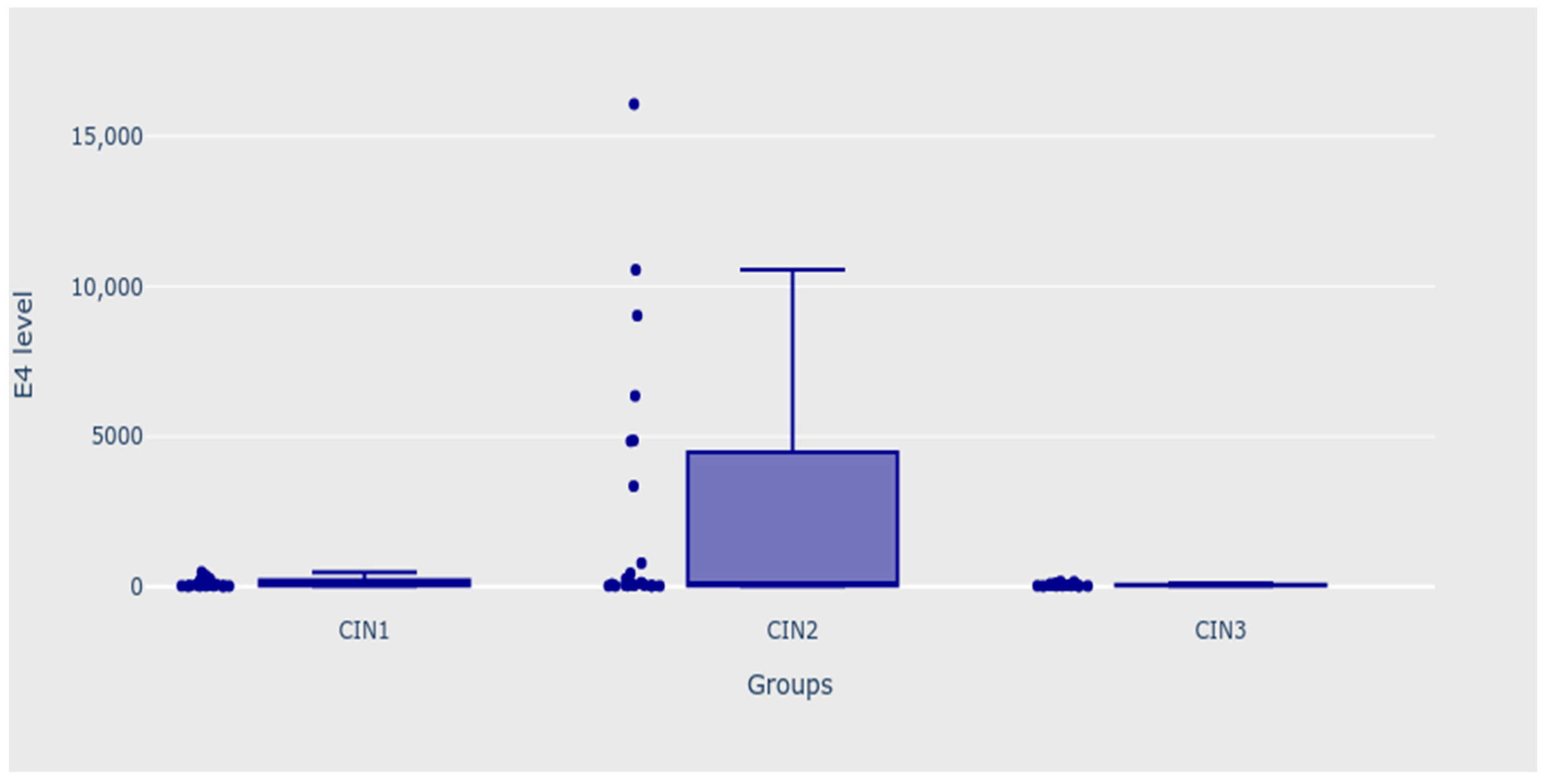
| Variable | E4 Protein Level | MD (95% CI) | p |
|---|---|---|---|
| Histological outcome (with outliers) | |||
| CIN 1 (n = 38) | 226.89 (36.83; 1795.09) | 0.156 | |
| CIN 2 (n = 24) | 120.95 (39.48; 4857.83) | ||
| CIN 3 (n = 19) | 45.06 (31.68; 102.28) | ||
| No pathology (n = 4) | 200.72 (29.70; 1147; 08) | ||
| Histological outcome (with outliers) | |||
| CIN 1 (n = 38) | 226.89 (36.83; 1795.09) | 0.079 | |
| CIN 2 (n = 24) CIN 3 (n = 19) | 120.95 (39.48; 4857.83) 45.06 (31.68; 102.28) | ||
| Histological outcome (with outliers) | |||
| CIN 1 + CIN 2 (n = 62) | 215.69 (37.37; 3348.77) | −170.63 (−426.55; −3.69) | 0.024 |
| CIN 3 (n = 19) | 45.06 (31.68; 102.28) | ||
| HPV status | |||
| Negative (n = 10) | 70.23 (35.18; 111.75) | 59.93 (−21.23; 783.87) | 0.354 |
| Positive (n = 75) | 130.16 (36.12; 2029.93) | ||
| HPV genotypes | |||
| 16 | |||
| Yes (n = 40) | 57.67 (32.42; 388.17) | 150.49 (−0.59; 312.10) | 0.056 |
| No (n = 45) | 208.16 (38.22; 4151.30) | ||
| 18 | |||
| Yes (n = 5) | 3348.77 (2254.76; 9026.87) | −3273.52 (−8990.23; −138.01) | 0.017 |
| No (n = 80) | 75.25 (35.37; 1084.38) | ||
| 31 | |||
| Yes (n = 12) | 1262.60 (76.26; 15688.67) | −1188.83 (−4843.74; 4.19) | 0.067 |
| No (n = 73) | 73.77 (35.18; 1045.23) | ||
| 45 | |||
| Yes (n = 4) | 1141.35 (953.21; 5093.02) | −1064.62 (−4180.16; 671.57) | 0.062 |
| No (n = 81) | 76.73 (35.56; 1712.73) | ||
| 6 | |||
| Yes (n = 9) | 41.59 (25.22; 66.89) | 103.06 (1.91; 1106.53) | 0.036 |
| No (n = 76) | 144.65 (36.22; 2097.55) | ||
| More than one HPV genotype | |||
| Yes (37) | 260.44 (33.80; 4850.36) | −185.19 (−1121.81; 14.02) | 0.321 |
| No (48) | 75.25 (37.49; 335.01) | ||
| Comorbidities | |||
| Yes (26) | 108.02 (32.32; 3348.77) | −18.60 (−220.85; 42.94) | 0.934 |
| No (59) | 89.42 (36.74; 1141.35) |
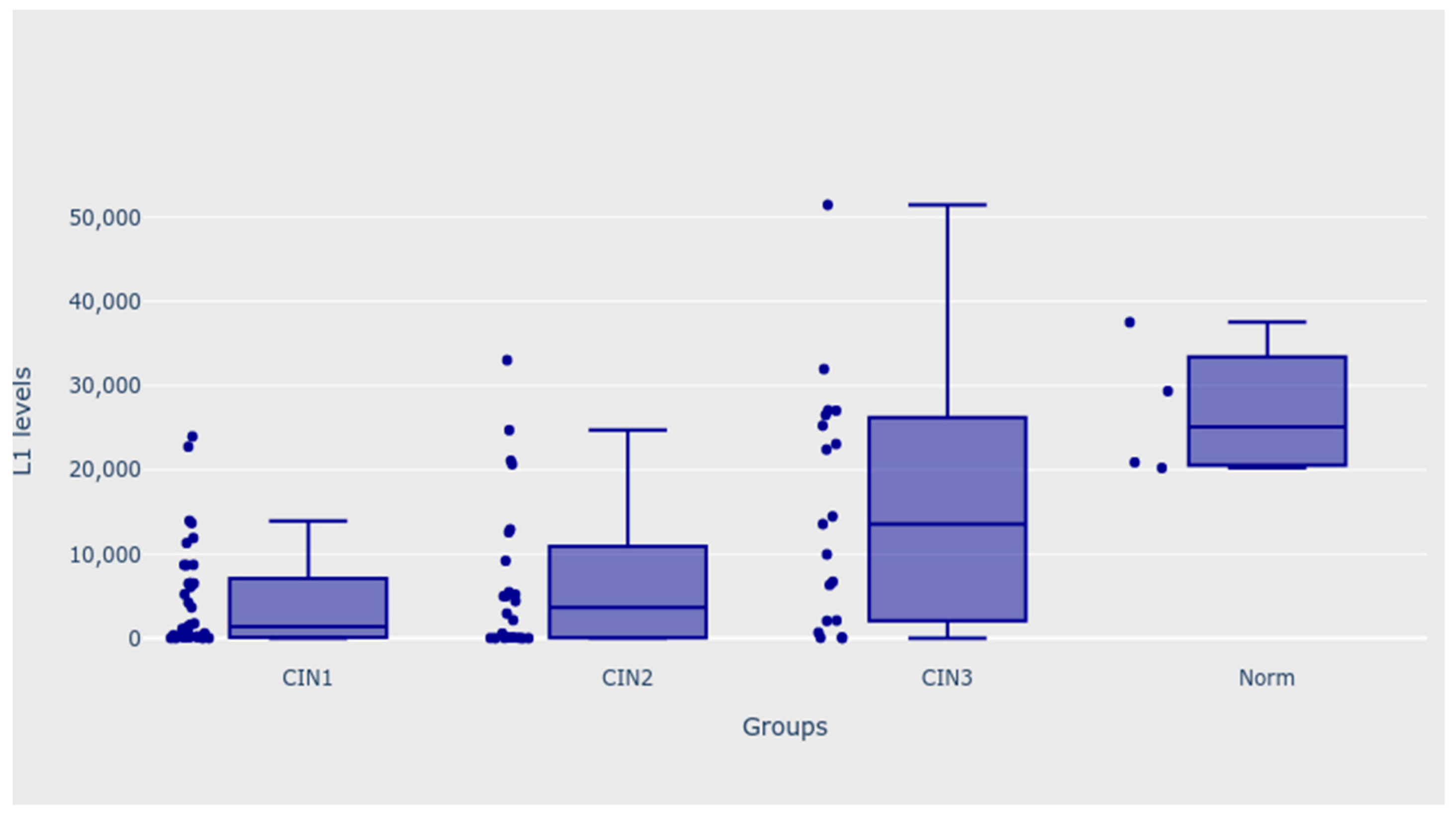
| Variable | L1 Level | MD (95% CI) | p |
|---|---|---|---|
| Histological outcome (with outliers) | |||
| CIN 1 (n = 38) | 1504.62 (154.65; 8683.80) | - | 0.002 |
| CIN 2 (n = 24) | 3684.91 (90.45; 10,905.76) | ||
| CIN 3 (n = 19) | 13,566.25 (2099.17; 25,884.17) | ||
| No pathology (n = 4) | 25,123.51 (20,563.59; 33,437.23) | ||
| Histological outcome (with outliers) | |||
| CIN 1 (n = 38) | 1504.62 (154.65; 8683.80) 3684.91 (90.45; 10,905.76) | 0.022 | |
| CIN 2 (n = 24) CIN 3 (n = 19) | 13,566.25 (2099.17; 25,884.17) | ||
| Histological outcome (with outliers) | |||
| CIN 1 + CIN 2 (n = 62) | 1967.74 (133.21; 8713.67) | 11,598.51 (949.47; 14,437.27) | 0.006 |
| CIN 3 (n = 19) | 13,566.25 (2099.17; 25,884.17) | ||
| 16 | |||
| Yes (n = 40) | 5107.77 (136.04; 17,349.82) | −685.53 (−4112.92; 795.55) | 0.666 |
| No (n = 45) | 4422.24 (229.53; 13,566.25) | ||
| 18 | |||
| Yes (n = 5) | 8713.67 (5009.37; 9210.31) | −4368.77 (−8457.52; 9937.55) | 0.519 |
| No (n = 80) | 4344.90 (145.63; 14,213.32) | −685.53 (−4112.92; 795.55) | 0.666 |
| 31 | |||
| Yes (n = 12) | 1753.24 (351.93; 6430.07) | 3256.13 (−1259.63; 6586.21) | 0.579 |
| No (n = 73) | 5009.37 (154.65; 13,957.17) | −4368.77 (−8457.52; 9937.55) | 0.519 |
| 45 | |||
| Yes (n = 4) | 10,806.31 (4408.50; 17,007.96) | −6384.07 (−12,808.30; 8262.89) | 0.514 |
| No (n = 81) | 4422.24 (154.65; 13,688.40) | 3256.13 (−1259.63; 6586.21) | 0.579 |
| 6 | |||
| Yes (n = 9) | 593.55 (117.89; 13,566.25) | 4514.22 (−2642.35; 6453.08) | 0.424 |
| No (n = 76) | 5107.77 (192.09; 13,822.78) | −6384.07 (−12,808.30; 8262.89) | 0.514 |
| More than one HPV genotype | |||
| Yes (n = 37) | 5008.66 (402.65; 12,928.81) | −55.34 (−2553.91; 2034.14) | 0.601 |
| No (n = 48) | 4953.32 (115.79; 17,093.67) | 4514.22 (−2642.35; 6453.08) | 0.424 |
| Comorbidities | |||
| Yes (n = 26) | 5206.17 (1126.42; 14,469.47) | −3038.83 (−4752.51; 1344.42) | 0.442 |
| No (n = 59) | 2167.34 (192.09; 13,247.53) | −55.34 (−2553.91; 2034.14) | 0.601 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Przybylski, M.; Pruski, D.; Millert-Kalińska, S.; Krzyżaniak, M.; de Mezer, M.; Frydrychowicz, M.; Jach, R.; Żurawski, J. Expression of E4 Protein and HPV Major Capsid Protein (L1) as A Novel Combination in Squamous Intraepithelial Lesions. Biomedicines 2023, 11, 225. https://doi.org/10.3390/biomedicines11010225
Przybylski M, Pruski D, Millert-Kalińska S, Krzyżaniak M, de Mezer M, Frydrychowicz M, Jach R, Żurawski J. Expression of E4 Protein and HPV Major Capsid Protein (L1) as A Novel Combination in Squamous Intraepithelial Lesions. Biomedicines. 2023; 11(1):225. https://doi.org/10.3390/biomedicines11010225
Chicago/Turabian StylePrzybylski, Marcin, Dominik Pruski, Sonja Millert-Kalińska, Monika Krzyżaniak, Mateusz de Mezer, Magdalena Frydrychowicz, Robert Jach, and Jakub Żurawski. 2023. "Expression of E4 Protein and HPV Major Capsid Protein (L1) as A Novel Combination in Squamous Intraepithelial Lesions" Biomedicines 11, no. 1: 225. https://doi.org/10.3390/biomedicines11010225