
Clinical and Personal Predictors of Helmet-CPAP Use and Failure in Patients Firstly Admitted to Regular Medical Wards with COVID-19-Related Acute Respiratory Distress Syndrome (hCPAP-f Study)
 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Patients and Data Collection
- –
- Flow-meters using both high-pressure oxygen and high-pressure medical air, with a target flow of 60 L/min at the beginning and a FiO2 of 60%, obtained by mixing the flows of air and pure oxygen; both air and pure oxygen could generate a flow of 60 L/min, with the theoretical possibility of attaining 100% FiO2;
- –
- Flow meters using Venturi systems to generate the high flow; these systems convey oxygen in two ways with a maximum of 30 or 60 L/min to a strict canal in a Venturi valve; the high flow generates a low-pressure area, which recruits room air at high flows; this mix could generate an initial FiO2 of 60%, and upon closing the Venturi valve, we obtain a FiO2 of 100%.
- –
- If the patient, evaluated by a trained intensivist, was considered recruitable for ICU, OTI was performed.
- –
- If the patient, after collegial evaluation by the intensivist and the internist, was considered to have a scarce brief-term prognosis, was very elderly, and had multiple comorbidities, a trial for BLPAP was considered.
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tzotzos, S.J.; Fischer, B.; Fischer, H.; Zeitlinger, M. Incidence of ARDS and outcomes in hospitalized patients with COVID-19: A global literature survey. Crit. Care 2020, 24, 516. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. COVID-19 Lombardy ICU Network. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA. 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tobin, M.J.; Laghi, F.; Jubran, A. Why COVID-19 Silent Hypoxemia Is Baffling to Physicians. Am. J. Respir. Crit. Care Med. 2020, 202, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Wilkerson, R.G.; Adler, J.D.; Shah, N.G.; Brown, R. Silent hypoxia: A harbinger of clinical deterioration in patients with COVID-19. Am. J. Emerg. Med. 2020, 38, 2243.e5–2243.e6. [Google Scholar] [CrossRef]
- Komorowski, M.; Aberegg, S.K. Using applied lung physiology to understand COVID-19 patterns. Br. J. Anaesth. 2020, 125, 250–253. [Google Scholar] [CrossRef]
- Lang, M.; Som, A.; Mendoza, D.P.; Flores, E.J.; Reid, N.; Carey, D.; Li, M.D.; Witkin, A.; Rodriguez-Lopez, J.M.; Shepard, J.O.; et al. Hypoxaemia related to COVID-19: Vascular and perfusion abnormalities on dual-energy CT. Lancet Infect. Dis. 2020, 20, 1365–1366. [Google Scholar] [CrossRef]
- Dhont, S.; Derom, E.; Van Braeckel, E.; Depuydt, P.; Lambrecht, B.N. The pathophysiology of ‘happy’ hypoxemia in COVID-19. Respir. Res. 2020, 21, 198. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Coppola, S.; Cressoni, M.; Busana, M.; Rossi, S.; Chiumello, D. COVID-19 Does Not Lead to a “Typical” Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2020, 201, 1299–1300. [Google Scholar] [CrossRef] [Green Version]
- Robba, C.; Battaglini, D.; Ball, L.; Patroniti, N.; Loconte, M.; Brunetti, I.; Vena, A.; Giacobbe, D.R.; Bassetti, M.; Rocco, P.R.M.; et al. Distinct phenotypes require distinct respiratory management strategies in severe COVID-19. Respir. Physiol. Neurobiol. 2020, 279, 103455. [Google Scholar] [CrossRef]
- Azoulay, E.; de Waele, J.; Ferrer, R.; Staudinger, T.; Borkowska, M.; Povoa, P.; Iliopoulou, K.; Artigas, A.; Schaller, S.J.; Shankar-Hari, M.; et al. International variation in the management of severe COVID-19 patients. Crit. Care 2020, 24, 486. [Google Scholar] [CrossRef]
- Docherty, A.B.; Mulholland, R.H.; Lone, N.I.; Cheyne, C.P.; De Angelis, D.; Diaz-Ordaz, K.; Donegan, C.; Drake, T.M.; Dunning, J.; Funk, S.; et al. ISARIC4C Investigators. Changes in in-hospital mortality in the first wave of COVID-19: A multicentre prospective observational cohort study using the WHO Clinical Characterisation Protocol UK. Lancet Respir. Med. 2021, 9, 773–785. [Google Scholar] [CrossRef] [PubMed]
- Grieco, D.L.; Menga, L.S.; Cesarano, M.; Rosà, T.; Spadaro, S.; Bitondo, M.M.; Montomoli, J.; Falò, G.; Tonetti, T.; Cutuli, S.L.; et al. Effect of Helmet Noninvasive Ventilation vs High-Flow Nasal Oxygen on Days Free of Respiratory Support in Patients With COVID-19 and Moderate to Severe Hypoxemic Respiratory Failure: The HENIVOT Randomized Clinical Trial. JAMA 2021, 325, 1731–1743. [Google Scholar] [CrossRef] [PubMed]
- Arabi, Y.M.; Aldekhyl, S.; Al Qahtani, S.; Al-Dorzi, H.M.; Abdukahil, S.A.; Al Harbi, M.K.; Al Qasim, E.; Kharaba, A.; Albrahim, T.; Alshahrani, M.S.; et al. Effect of Helmet Noninvasive Ventilation vs Usual Respiratory Support on Mortality Among Patients with Acute Hypoxemic Respiratory Failure Due to COVID-19: The HELMET-COVID Randomized Clinical Trial. JAMA 2022, 328, 1063–1072. [Google Scholar] [CrossRef]
- ARDS Definition Task Force; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526. [Google Scholar] [CrossRef]
- Ji, D.; Zhang, D.; Xu, J.; Chen, Z.; Yang, T.; Zhao, P.; Chen, G.; Cheng, G.; Wang, Y.; Bi, J.; et al. Prediction for Progression Risk in Patients With COVID-19 Pneumonia: The CALL Score. Clin. Infect. Dis. 2020, 71, 1393–1399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Prev. Med. 2007, 45, 247–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruopp, M.D.; Perkins, N.J.; Whitcomb, B.W.; Schisterman, E.F. Youden Index and optimal cut-point estimated from observations affected by a lower limit of detection. Biometrical journal. Biom. Z. 2008, 50, 419–430. [Google Scholar] [CrossRef] [Green Version]
- The Northwell COVID-19 Research Consortium; Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- Gujski, M.; Jankowski, M.; Rabczenko, D.; Goryński, P.; Juszczyk, G. The Prevalence of Acute Respiratory Distress Syndrome (ARDS) and Outcomes in Hospitalized Patients with COVID-19-A Study Based on Data from the Polish National Hospital Register. Viruses 2022, 14, 76. [Google Scholar] [CrossRef]
- Tolossa, T.; Merdassa Atomssa, E.; Fetensa, G.; Bayisa, L.; Ayala, D.; Turi, E.; Wakuma, B.; Mulisa, D.; Seyoum, D.; Getahun, A.; et al. Acute respiratory distress syndrome among patients with severe COVID-19 admitted to treatment center of Wollega University Referral Hospital, Western Ethiopia. PLoS ONE 2022, 17, e0267835. [Google Scholar] [CrossRef]
- Ciceri, F.; Castagna, A.; Rovere-Querini, P.; De Cobelli, F.; Ruggeri, A.; Galli, L.; Conte, C.; De Lorenzo, R.; Poli, A.; Ambrosio, A.; et al. Early predictors of clinical outcomes of COVID-19 outbreak in Milan, Italy. Clin. Immunol. 2020, 217, 108509. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 7 August 2022).
- Alhazzani, W.; Evans, L.; Alshamsi, F.; Møller, M.H.; Ostermann, M.; Prescott, H.C.; Arabi, Y.M.; Loeb, M.; Ng Gong, M.; Fan, E.; et al. Rhodes, Andrew Surviving Sepsis Campaign Guidelines on the Management of Adults With Coronavirus Disease 2019 (COVID-19) in the ICU: First Update. Crit. Care Med. 2021, 49, e219–e234. [Google Scholar] [CrossRef] [PubMed]
- Frat, J.P.; Thille, A.W.; Mercat, A.; Girault, C.; Ragot, S.; Perbet, S.; Prat, G.; Boulain, T.; Morawiec, E.; Cottereau, A.; et al. REVA Network. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N. Engl. J. Med. 2015, 372, 2185–2196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perkins, G.D.; Ji, C.; Connolly, B.A.; Couper, K.; Lall, R.; Baillie, J.K.; Bradley, J.M.; Dark, P.; Dave, C.; De Soyza, A.; et al. Effect of Noninvasive Respiratory Strategies on Intubation or Mortality Among Patients With Acute Hypoxemic Respiratory Failure and COVID-19: The RECOVERY-RS Randomized Clinical Trial. JAMA 2022, 327, 546–558. [Google Scholar] [CrossRef]
- Suardi, L.R.; Pallotto, C.; Esperti, S.; Tazzioli, E.; Baragli, F.; Salomoni, E.; Botta, A.; Covani Frigieri, F.; Pazzi, M.; Stera, C.; et al. Risk factors for non-invasive/invasive ventilatory support in patients with COVID-19 pneumonia: A retrospective study within a multidisciplinary approach. Int. J. Infect. Dis. 2020, 100, 258–263. [Google Scholar] [CrossRef]
- Brusasco, C.; Corradi, F.; Di Domenico, A.; Raggi, F.; Timossi, G.; Santori, G.; Brusasco, V.; Galliera CPAP-COVID-19 Study Group. Collaborators of the Galliera CPAP-COVID-19 study group are. Continuous positive airway pressure in COVID-19 patients with moderate-to-severe respiratory failure. Eur. Respir. J. 2021, 57, 2002524. [Google Scholar] [CrossRef]
- Wagner, J.; Garcia-Rodriguez, V.; Yu, A.; Dutra, B.; Larson, S.; Cash, B.; DuPont, A.; Farooq, A. Elevated transaminases and hypoalbuminemia in Covid-19 are prognostic factors for disease severity. Sci. Rep. 2021, 11, 10308. [Google Scholar] [CrossRef]
- Henry, B.M.; Aggarwal, G.; Wong, J.; Benoit, S.; Vikse, J.; Plebani, M.; Lippi, G. Lactate dehydrogenase levels predict coronavirus disease 2019 (COVID-19) severity and mortality: A pooled analysis. Am. J. Emerg. Med. 2020, 38, 1722–1726. [Google Scholar] [CrossRef]
- Coomes, E.A.; Haghbayan, H. Interleukin-6 in COVID-19: A systematic review and meta-analysis. Rev. Med. Virol. 2020, 30, 1–9. [Google Scholar] [CrossRef]
- L′Her, E.; Duquesne, F.; Girou, E.; de Rosiere, X.D.; Le Conte, P.; Renault, S.; Allamy, J.P.; Boles, J.M. Noninvasive continuous positive airway pressure in elderly cardiogenic pulmonary edema patients. Intensive Care Med. 2004, 30, 882–888. [Google Scholar] [CrossRef]
- Lagier, J.C.; Amrane, S.; Mailhe, M.; Gainnier, M.; Arlotto, S.; Gentile, S.; Raoult, D. High-flow oxygen therapy in elderly patients infected with SARS-CoV2 with a contraindication for transfer to an intensive care unit: A preliminary report. Int. J. Infect. Dis. 2021, 108, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T. Male sex identified by global COVID-19 meta-analysis as a risk factor for death and ITU admission. Nat. Commun. 2020, 11, 6317. [Google Scholar] [CrossRef] [PubMed]
- Monserrat Villatoro, J.; Mejía-Abril, G.; Díaz García, L.; Zubiaur, P.; Jiménez González, M.; Fernandez Jimenez, G.; Cancio, I.; Arribas, J.R.; Suarez Fernández, C.; Mingorance, J.; et al. A Case-Control of Patients with COVID-19 to Explore the Association of Previous Hospitalisation Use of Medication on the Mortality of COVID-19 Disease: A Propensity Score Matching Analysis. Pharmaceuticals 2022, 15, 78. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Yang, Q.; Wang, Y.; Wu, Y.; Xu, J.; Yu, Y.; Shang, Y. Thrombocytopenia and its association with mortality in patients with COVID-19. J. Thromb. Haemost. 2020, 18, 1469–1472. [Google Scholar] [CrossRef]
- Tetaj, N.; Piselli, P.; Zito, S.; De Angelis, G.; Marini, M.C.; Rubino, D.; Gaviano, I.; Antonica, M.V.; Agostini, E.; Porcelli, C.; et al. Timing and Outcomes of Noninvasive Ventilation in 307 ARDS COVID-19 Patients: An Observational Study in an Italian Third Level COVID-19 Hospital. Medicina 2022, 58, 1104. [Google Scholar] [CrossRef] [PubMed]
- Grifoni, E.; Valoriani, A.; Cei, F.; Lamanna, R.; Gelli, A.M.G.; Ciambotti, B.; Vannucchi, V.; Moroni, F.; Pelagatti, L.; Tarquini, R.; et al. Interleukin-6 as prognosticator in patients with COVID-19. J. Infect. 2020, 81, 452–482. [Google Scholar] [CrossRef]
- Santus, P.; Pini, S.; Amati, F.; Saad, M.; Gatti, M.; Mondoni, M.; Tursi, F.; Rizzi, M.; Chiumello, D.A.; Monzani, V.; et al. Predictors of Helmet CPAP Failure in COVID-19 Pneumonia: A Prospective, Multicenter, and Observational Cohort Study. Can. Respir. J. 2022, 2022, 1499690. [Google Scholar] [CrossRef]
- Bellani, G.; Grasselli, G.; Cecconi, M.; Antolini, L.; Borelli, M.; De Giacomi, F.; Bosio, G.; Latronico, N.; Filippini, M.; Gemma, M.; et al. Noninvasive Ventilatory Support of Patients with COVID-19 outside the Intensive Care Units (WARd-COVID). Ann. Am. Thorac. Soc. 2021, 18, 1020–1026. [Google Scholar] [CrossRef]
- Zampieri, F.G.; Ferreira, J.C. Defining Optimal Respiratory Support for Patients with COVID-19. JAMA 2022, 327, 531–533. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | hCPAP | Conventional Oxygen | Younden Index | p-Value |
|---|---|---|---|---|
| Age (years) | 69 (61–78) | 73 (58–84) | <78 | 0.006 |
| Male Sex n(%) | 189/295 (64%) | 177/386 (45.9%) | 0.01 | |
| Hypertension | 142/295 (48.1%) | 188/384 (48.9%) | 0.93 | |
| Cardiovascular disease | 80/295 (27.1%) | 117/384 (30%) | 0.14 | |
| Respiratory diseases | 44/295 (14.9%) | 60/384 (15.6%) | 0.10 | |
| Chronic kidney disease | 35/295 (11.8%) | 68/386 (17.6%) | 0.04 | |
| Active cancer | 26/295 (8.8%) | 28/386 (7.3%) | 0.047 | |
| Severe obesity | 42/295 (14.2%) | 34/384 (8.9%) | 0.004 | |
| Neuropsychiatric disorders | 34/295 (11.5%) | 99/386 (25.6%) | <0.001 | |
| Diabetes | 50/295 (16.9%) | 81/384 (21%) | 0.08 | |
| Polytherapy at home | 137/295 (46.4%) | 183/384 (47.7%) | 0.62 | |
| Haemoglobin (g/dL) | 14 (13–15) | 13 (12–15) | >13 | <0.001 |
| Platelets (109/L) | 207 (157–260) | 204 (163–259) | 0.98 | |
| Neutrophils (units/L) | 5900 (4550–8600) | 4900 (3370–7650) | >4700 | <0.001 |
| Lymphocytes (units/L) | 800 (570–1100) | 860 (600–1200) | 0.30 | |
| International Normalized Ratio (INR) | 1.2 (1.1–1.3) | 1.1 (1.0–1.2) | >1.1 | 0.026 |
| D-dimer (µg/mL) | 847 (523–1550) | 900 (530–1500) | 0.95 | |
| Fibrinogen (mg/dL) | 770 (640–880) | 680 (570–790) | <0.001 | |
| Aspartate aminotransferase (U/L) | 39 (31–54) | 31 (24–46) | >33 | <0.001 |
| Alanine aminotransferase (U/L) | 31 (19–51) | 24 (16–39) | <0.001 | |
| Lactate dehydrogenase (U/L) | 620 (480–760) | 470 (380–600) | >570 | <0.001 |
| Total Bilirubin (mg/dL) | 0.6 (0.5–0.8) | 0.6 (0.5–0.8) | 0.125 | |
| C-reactive protein (mg/dL) | 8.3 (4–13) | 4.8 (2–11) | >4.6 | <0.001 |
| Procalcitonin (ng/mL) | 0.12 (0.07–0.3) | 0.09 (0.05–0.22) | >0.1 | <0.001 |
| Interleukin-6 (pg/mL) | 58 (31–100) | 34 (14–66) | >46 | <0.001 |
| Horowitz Index | 230 (130–275) | 260 (180–310) | <270 | 0.006 |
| Brain natriuretic peptide (pg/mL) | 64 (35–140) | 79 (34–190) | 0.31 | |
| Call score | 12 (10–13) | 11 (9–12) | >9 | <0.001 |
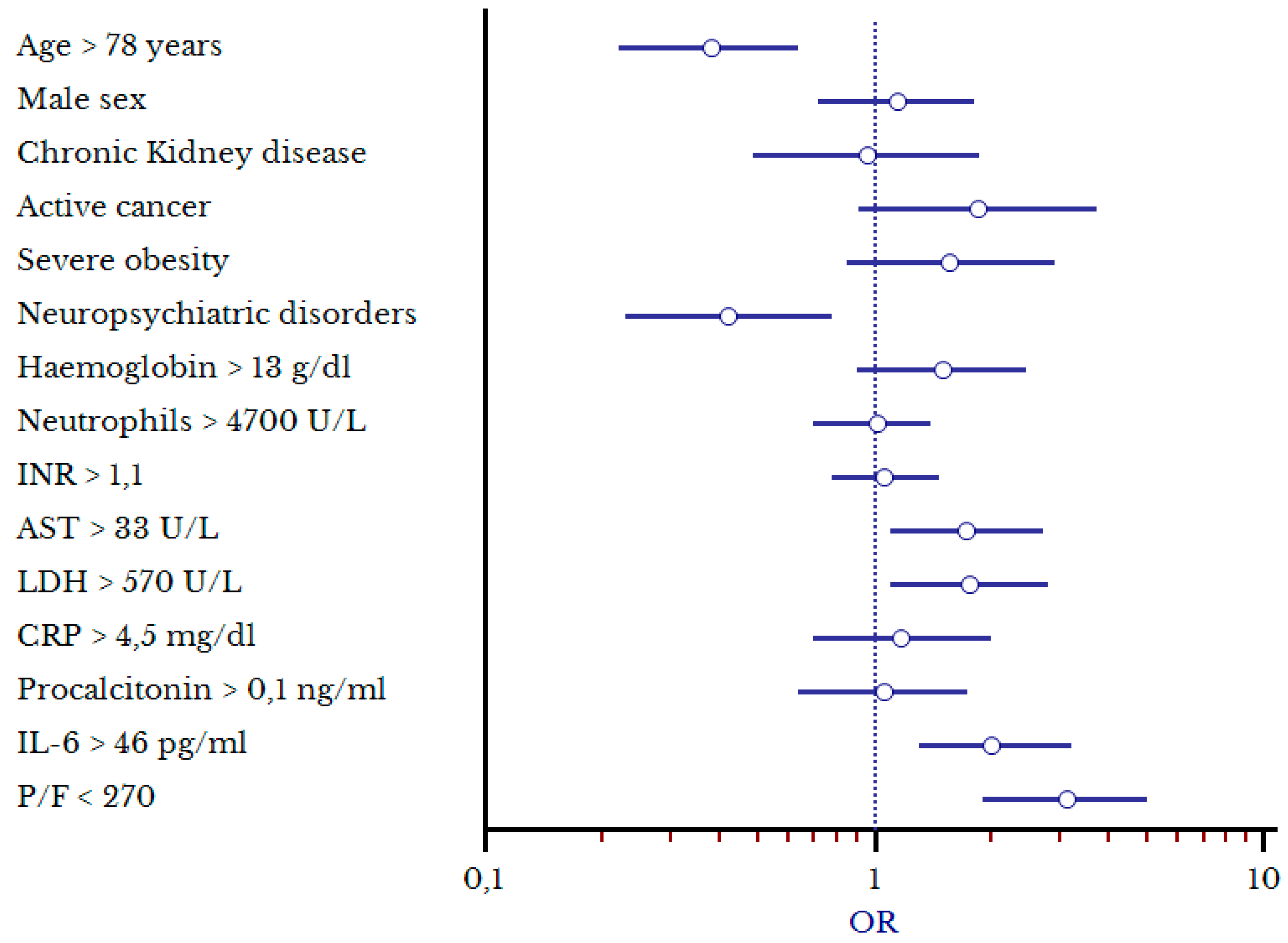
| Variables | OR (CI) | p-Value |
|---|---|---|
| Age > 78 years | 0.38 (0.23–0.64) | <0.001 |
| Male sex | 1.14 (0.72–1.81) | 0.561 |
| Cronic kidney disease | 0.95 (0.49–1.86) | 0.874 |
| Active cancer | 1.84 (0.91–3.73) | 0.088 |
| Severe obesity | 1.57 (0.84–2.9) | 0.153 |
| Neuropsychiatric disorders | 0.43 (0.23–0.78) | 0.006 |
| Hemoglobin > 13 g/dL | 1.5 (0.91–2.46) | 0.113 |
| Neutrophils > 4000 units/L | 1.02 (0.71–1.44) | 0.933 |
| INR > 1.1 | 1.06 (0.76–1.47) | 0.72 |
| Aspartate aminotransferase U/L | 1.72 (1.08–2.74) | 0.022 |
| Lactate dehydrogenase (U/L) | 1.75 (1.09–2.82) | 0.021 |
| C-reactive protein > 5 mg/dL | 1.18 (0.71–1.96) | 0.527 |
| Procalcitonin > 0.1 ng/mL | 1.06 (0.64–1.74) | 0.829 |
| Interleukin-6 > 46 pg/mL | 2.04 (1.28–3.24) | 0.003 |
| Horowitz index < 270 | 3.11 (1.95–4.95) | <0.001 |
| Variables | hCPAP Success | hCPAP Failure | Younden Index | p-Value |
|---|---|---|---|---|
| Age (years) | 66 (57–73) | 73 (63–83) | 70 | <0.001 |
| Male Sex | 98/170 | 94/125 | 0.002 | |
| Hypertension | 74/170 | 17/125 | 0.037 | |
| Cardiovascular disease | 38/170 | 44/125 | 0.021 | |
| Respiratory diseases | 21/170 | 26/125 | 0.05 | |
| Chronic kidney disease | 11/170 | 22/125 | 0.002 | |
| Active cancer | 10/170 | 18/125 | 0.048 | |
| Severe obesity | 26/170 | 16/125 | 0.53 | |
| Neuropsychiatric disorders | 15/170 | 20/125 | 0.044 | |
| Diabetes | 31/170 | 22/125 | 0.057 | |
| Polytherapy at home | 62/170 | 77/125 | <0.001 | |
| Haemoglobin (g/dL) | 14 (13–15) | 14 (13–15) | 0.37 | |
| Platelets (109/L) | 220 (180–280) | 174 (135–237) | <180 | <0.001 |
| Neutrophils (units/L) | 6000 (4400–8500) | 6000 (4400–8500) | 0.59 | |
| Lymphocytes (units/L) | 860 (600–1200) | 780 (510–1040) | 0.051 | |
| International Normalized Ratio (INR) | 1.2 (1.1–1.3) | 1.2 (1.1–1.3) | 0.46 | |
| D-dimer (µg/mL) | 730 (470–1280) | 1070 (630–1900) | >1160 | 0.001 |
| Fibrinogen (mg/dL) | 800 (660–890) | 720 (600–850) | 0.001 | |
| Aspartate aminotransferase (U/L) | 39 (25–60) | 39 (25–60) | 0.2 | |
| Alanine aminotransferase (U/L) | 31 (20–53) | 31 (20–53) | 0.44 | |
| Lactate dehydrogenase (U/L) | 620 (470–780) | 620 (470–780) | 0.11 | |
| Total Bilirubin (mg/dL) | 0.6 (0.5–0.7) | 0.7 (0.5–0.9) | 0.027 | |
| C-reactive protein (mg/dL) | 7.4 (3.7–13) | 9.4 (5–14) | >7 | 0.013 |
| Procalcitonin (ng/mL) | 0.09 (0.06–0.2) | 0.2 (0.1–0.43) | >0.1 | <0.001 |
| Interleukin-6 (pg/mL) | 48 (24–84) | 75 (40–130) | >63 | <0.01 |
| Creatinine (mg/dL) | 0.87 (0.78–1.05) | 1.07 (0.86–1.5) | >1.1 | <0.001 |
| Horowitz Index | 250 (170–290) | 190 (26–250) | <240 | 0.001 |
| Brain natriuretic peptide (pg/mL) | 58 (34–127) | 75 (34–180) | 0.16 | |
| Call Score | 11 (9–13) | 12 (10–13) | >10 | 0.002 |
| Days from hospital admission to hCPAP delivery | 2 (1–3) | 1 (1–3) | 0.58 | |
| Days from symptom onset to hCPAP delivery | 8 (5–10) | 7 (5–9) | 0.083 | |
| Days of ventilation | 8 (6–10) | 7 (3–13) | 0.233 | |
| Therapy with tocilizumab | 25/170 | 26/125 | 0.10 | |
| Therapy with antibiotics | 94/170 | 98/125 | 0.048 |
| Variables | Odds Ratio (OR) | p-Value |
|---|---|---|
| Age > 70 years | 1.86 (0.96–3.62) | 0.066 |
| Male sex | 2.24 (1.12–4.78) | 0.023 |
| Hypertension | 0.71 (0.35–1.44) | 0.345 |
| Cardiovascular diseases | 1.01 (0.44–2.36) | 0.973 |
| Respiratory diseases | 0.75 (0.31–1.81) | 0.525 |
| Cronic kidney disease | 1.48 (0.44–4.98) | 0.524 |
| Active cancer | 2.04 (0.75–5.5) | 0.161 |
| Neuropsychiatric disorders | 1.26 (0.47–3.35) | 0.646 |
| Polytherapy at home | 2.4 (1.09–5.13) | 0.03 |
| Platelet count < 180 × 109/L | 3.17 (1.58–6.34) | <0.001 |
| D-dimer > 1160 µg/mL | 1 (0.49–2.0) | 0.979 |
| C-reactive protein > 10 mg/dL | 1 (0.5–2.01) | 0.993 |
| Interleukin-6 > 63 pg/mL | 1.74 (0.89–2.45) | 0.106 |
| Procalcitonin > 0.1 ng/mL | 1.47 (0.73–2.96) | 0.281 |
| Creatinine > 1.1 mg/dL | 1.19 (0.53–2.67) | 0.669 |
| Horowitz index < 240 | 2.04 (1.04–3.99) | 0.037 |
| Therapy with antibiotics | 1.47 (0.7–3.1) | 0.31 |
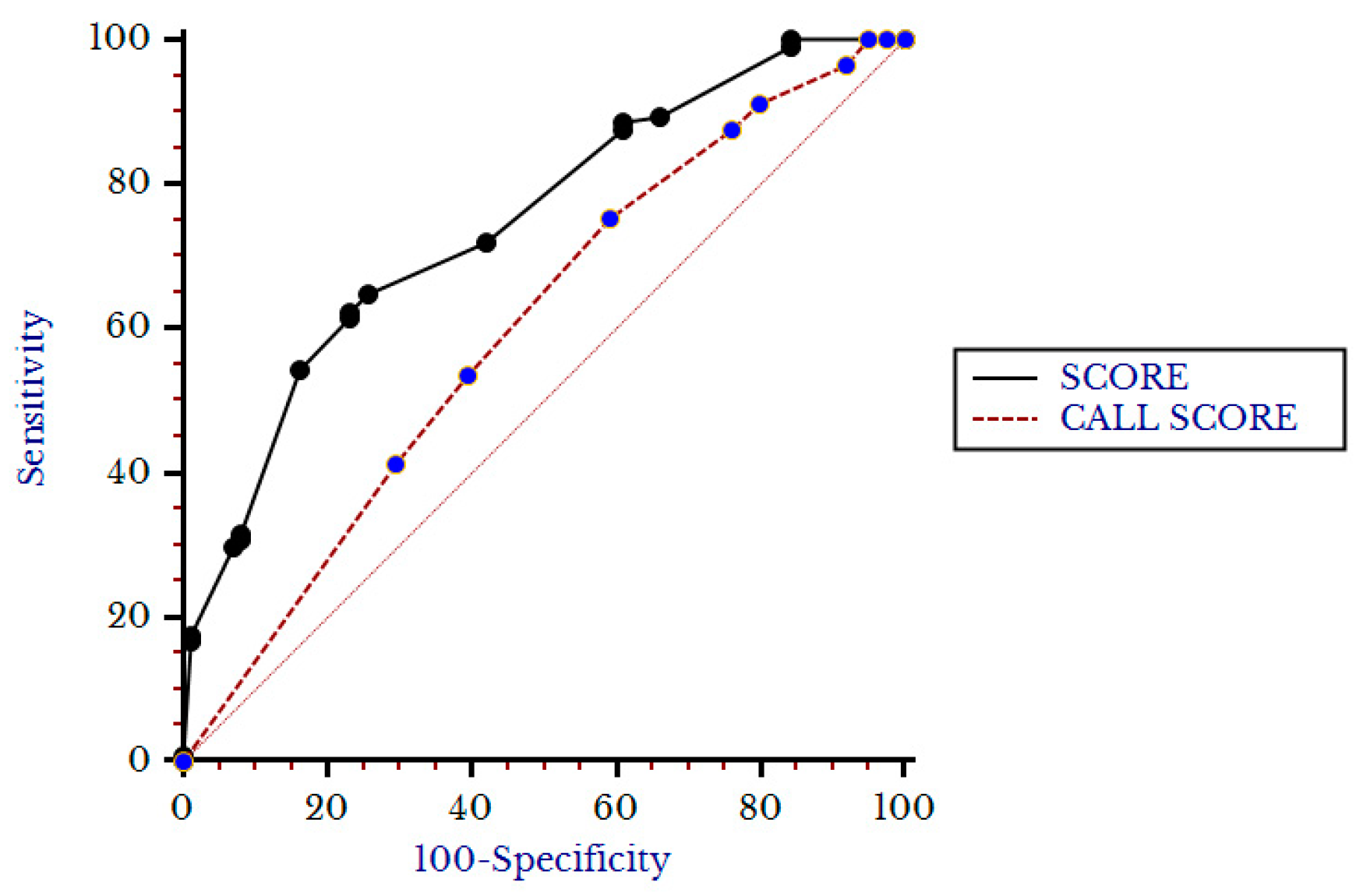
| Variable | OR | Score Points |
|---|---|---|
| Male Sex | 2.2 | 2 |
| Polytherapy at home | 2.4 | 2.5 |
| P/F <84 84–240 241–300 >300 | 3.1 2.2 1.2 0.7 | 3 2 0 0 |
| Platelet count (× 109/L) <160 160–205 206–260 >260 | 3.9 2 1.3 0.85 | 4 2 0 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cei, F.; Chiarugi, L.; Brancati, S.; Dolenti, S.; Montini, M.S.; Rosselli, M.; Filippelli, M.; Ciacci, C.; Sellerio, I.; Gucci, M.M.; et al. Clinical and Personal Predictors of Helmet-CPAP Use and Failure in Patients Firstly Admitted to Regular Medical Wards with COVID-19-Related Acute Respiratory Distress Syndrome (hCPAP-f Study). Biomedicines 2023, 11, 207. https://doi.org/10.3390/biomedicines11010207
Cei F, Chiarugi L, Brancati S, Dolenti S, Montini MS, Rosselli M, Filippelli M, Ciacci C, Sellerio I, Gucci MM, et al. Clinical and Personal Predictors of Helmet-CPAP Use and Failure in Patients Firstly Admitted to Regular Medical Wards with COVID-19-Related Acute Respiratory Distress Syndrome (hCPAP-f Study). Biomedicines. 2023; 11(1):207. https://doi.org/10.3390/biomedicines11010207
Chicago/Turabian StyleCei, Francesco, Ludia Chiarugi, Simona Brancati, Silvia Dolenti, Maria Silvia Montini, Matteo Rosselli, Mario Filippelli, Chiara Ciacci, Irene Sellerio, Marco Maria Gucci, and et al. 2023. "Clinical and Personal Predictors of Helmet-CPAP Use and Failure in Patients Firstly Admitted to Regular Medical Wards with COVID-19-Related Acute Respiratory Distress Syndrome (hCPAP-f Study)" Biomedicines 11, no. 1: 207. https://doi.org/10.3390/biomedicines11010207