
Role of Cytokines, Chemokines and IFN-γ+ IL-17+ Double-Positive CD4+ T Cells in Patients with Multiple Sclerosis

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
2.2. Exclusion Criteria
2.3. Blood Collection
2.4. Isolation of Mononuclear Cells
2.5. Production of Chemokines, Cytokines, and BDNF
2.6. Characterization of Cytokine Double-Producers CD4+ T Lymphocytes
2.7. Statistical Analysis
3. Results
3.1. Clinical and Epidemiological Profile of Individuals Enrolled in the Study
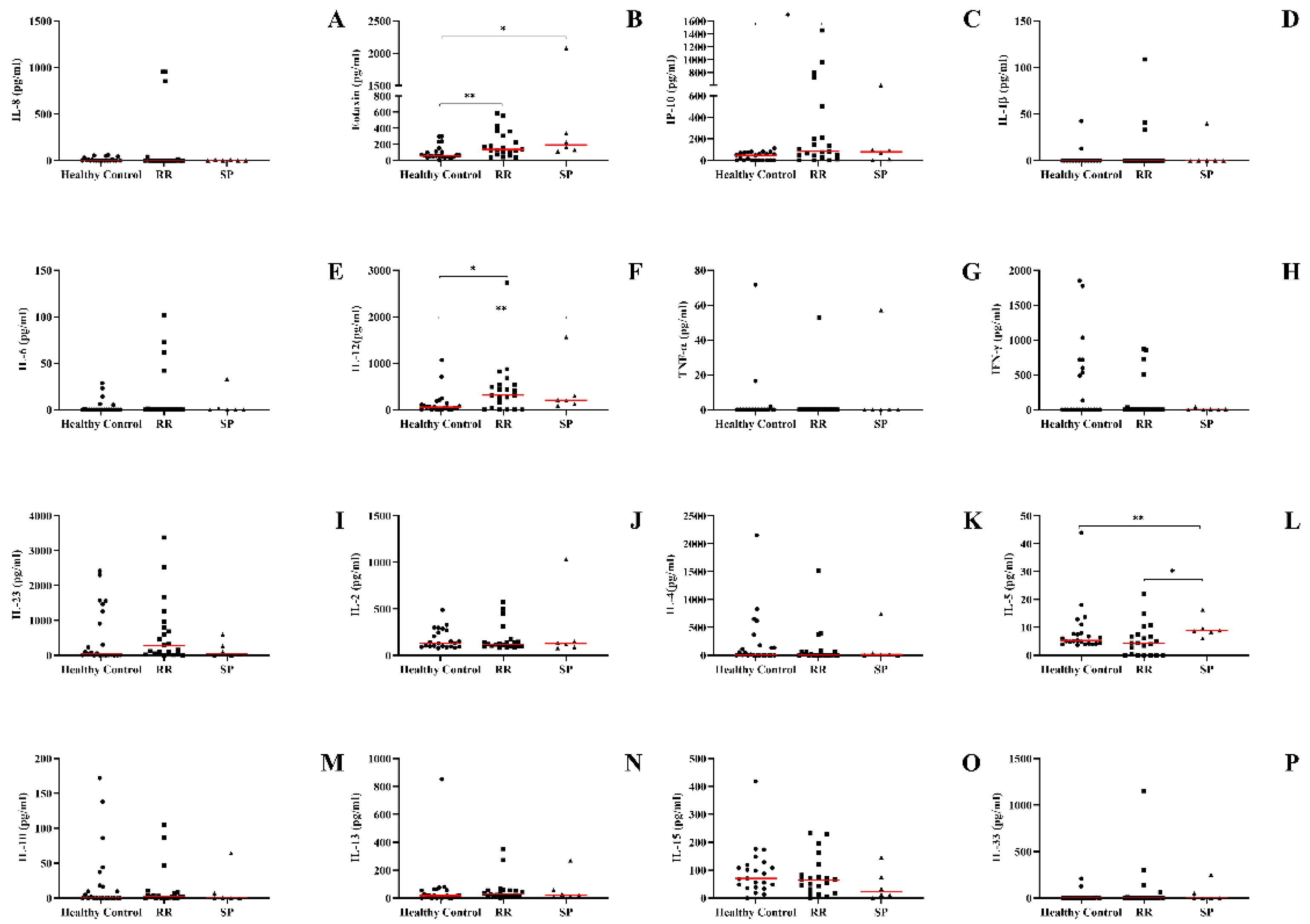
3.2. The Recurrent Relapsing Form of MS Demonstrates an Increase in the Production of Pro-Inflammatory Chemokines and Cytokines (IP-10, IL-12, and Eotaxin)
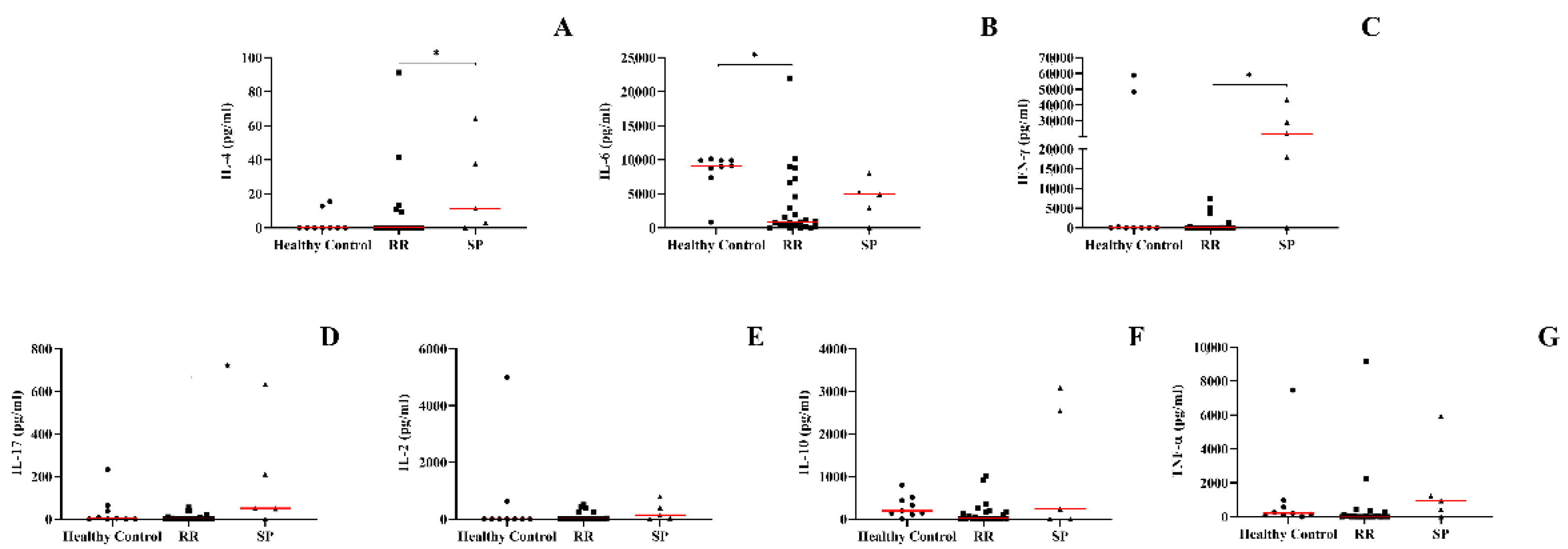
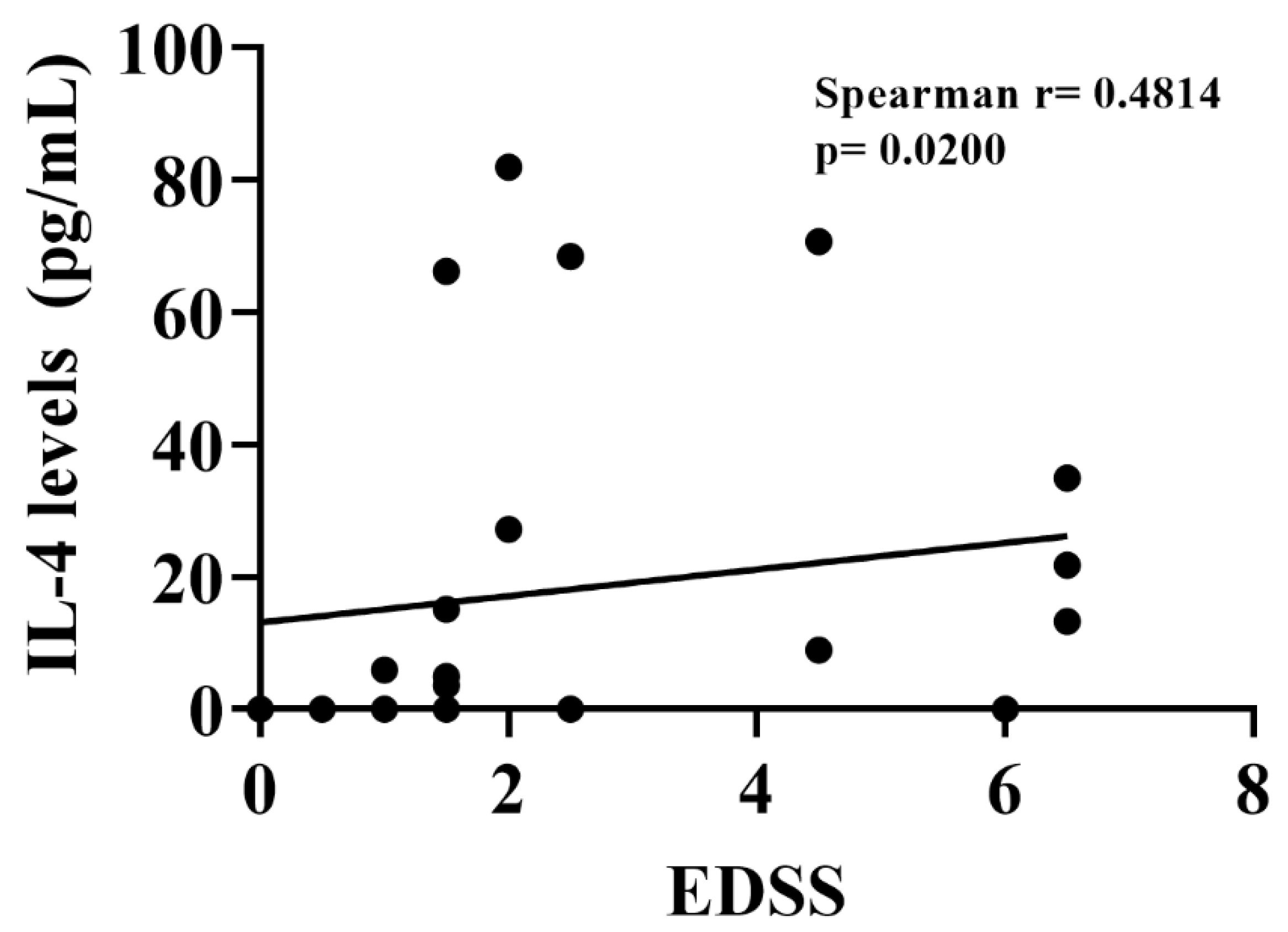
3.3. Secondary Progressive Form of MS Positively Regulates Levels of IL-4, IL-17, and IFN-γ in the Supernatant of PBMCs from MS Patients
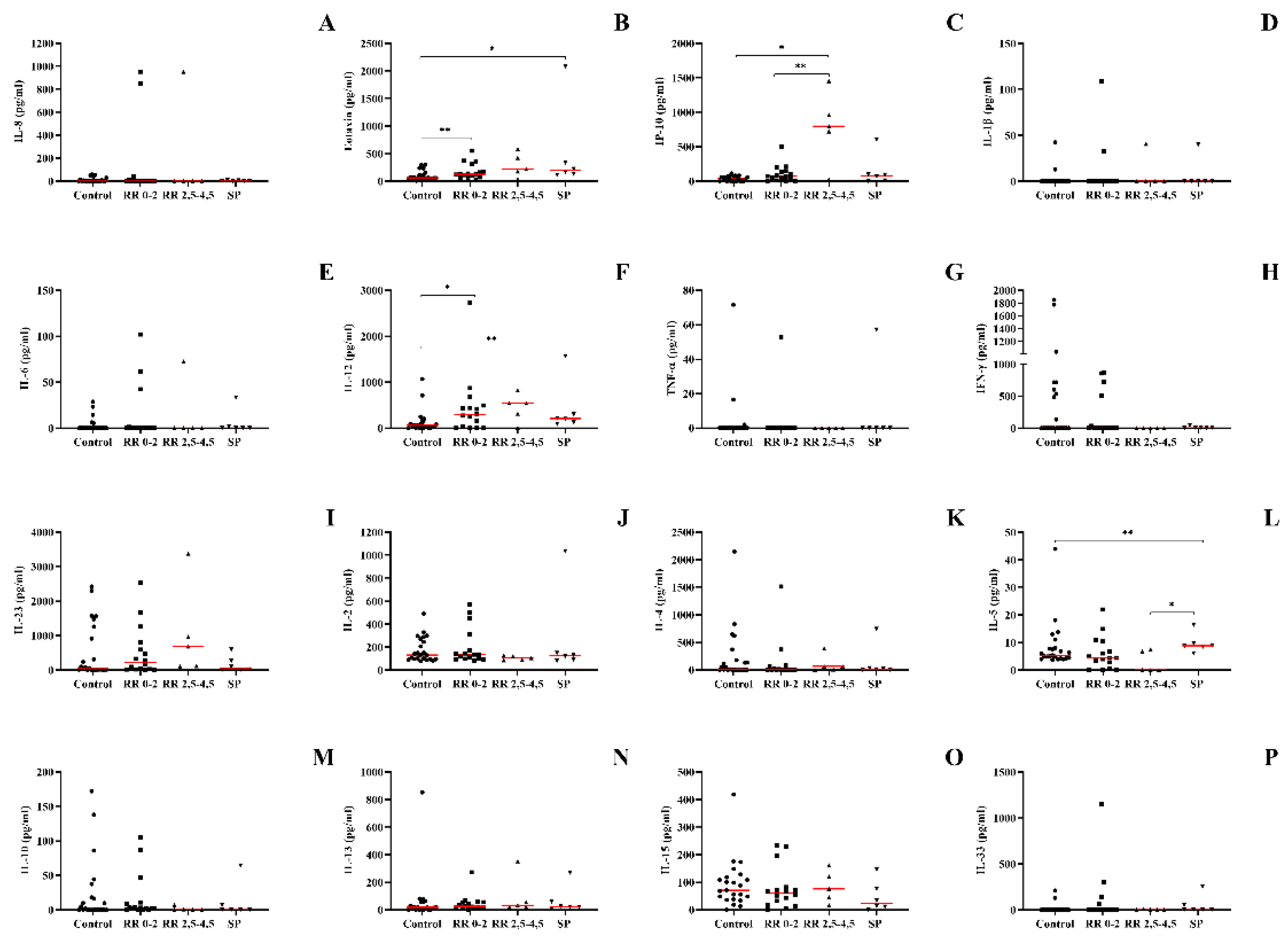
3.4. IL-12, Eotaxin, and IP-10 Were Increased in Patients with a Higher Degree on the EDSS Scale, While IL-5 Was Increased in Patients with the SP Form
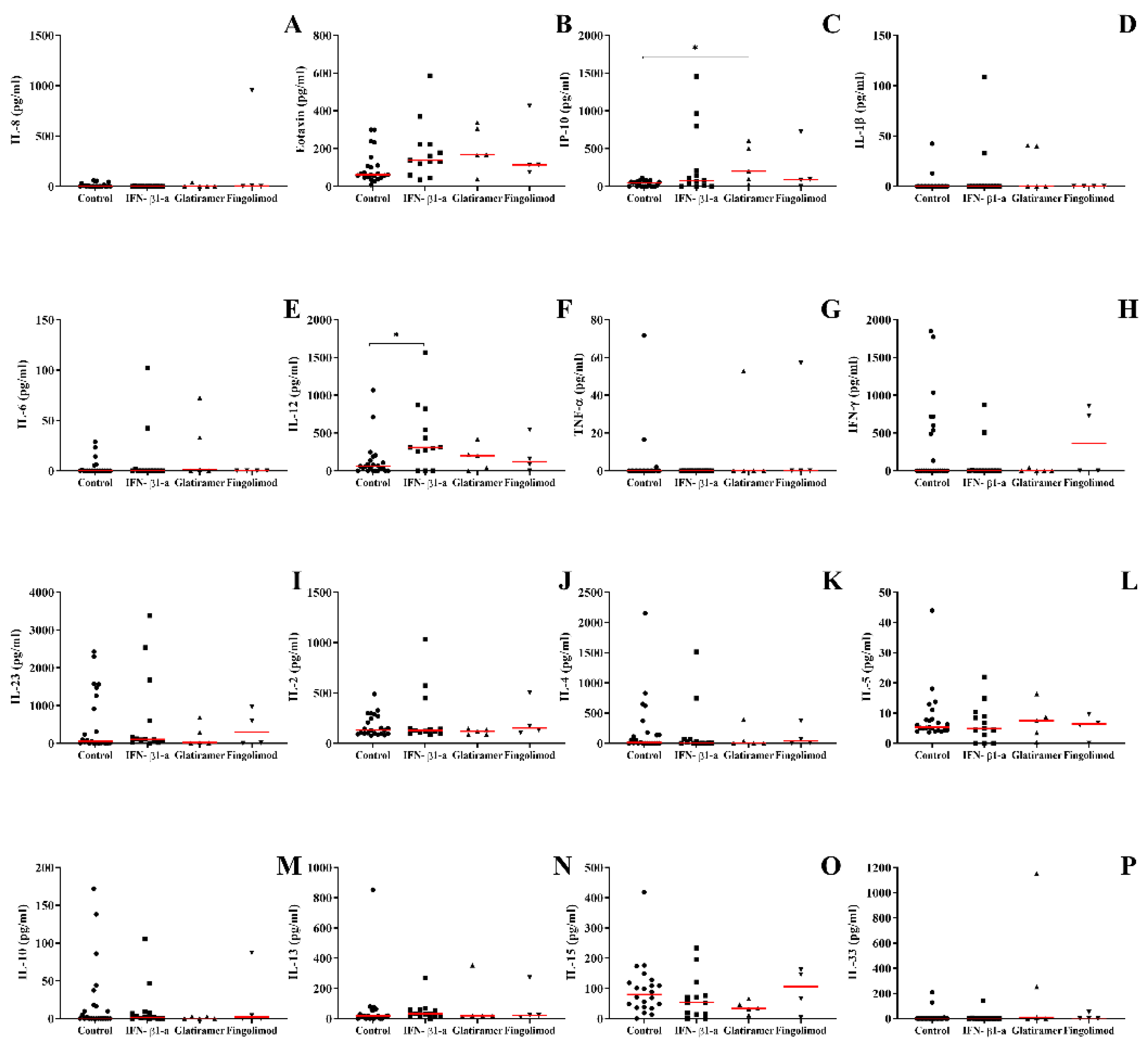
3.5. Cytokine and Chemokine Profile in the Plasma of Patients with MS Changes According to Treatment
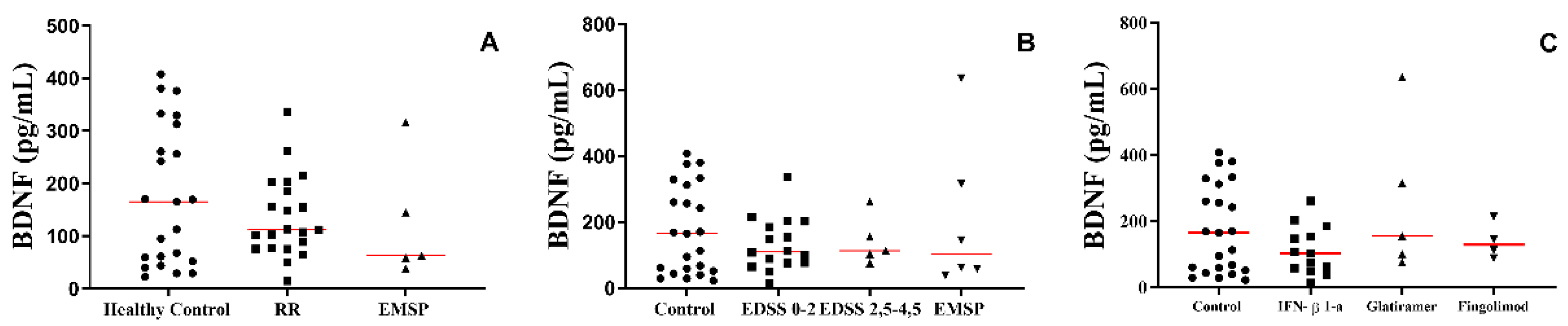
3.6. The Production of BDNF in the Plasma of Patients with MS Was Not Altered According to the Clinical Form or Treatment Used
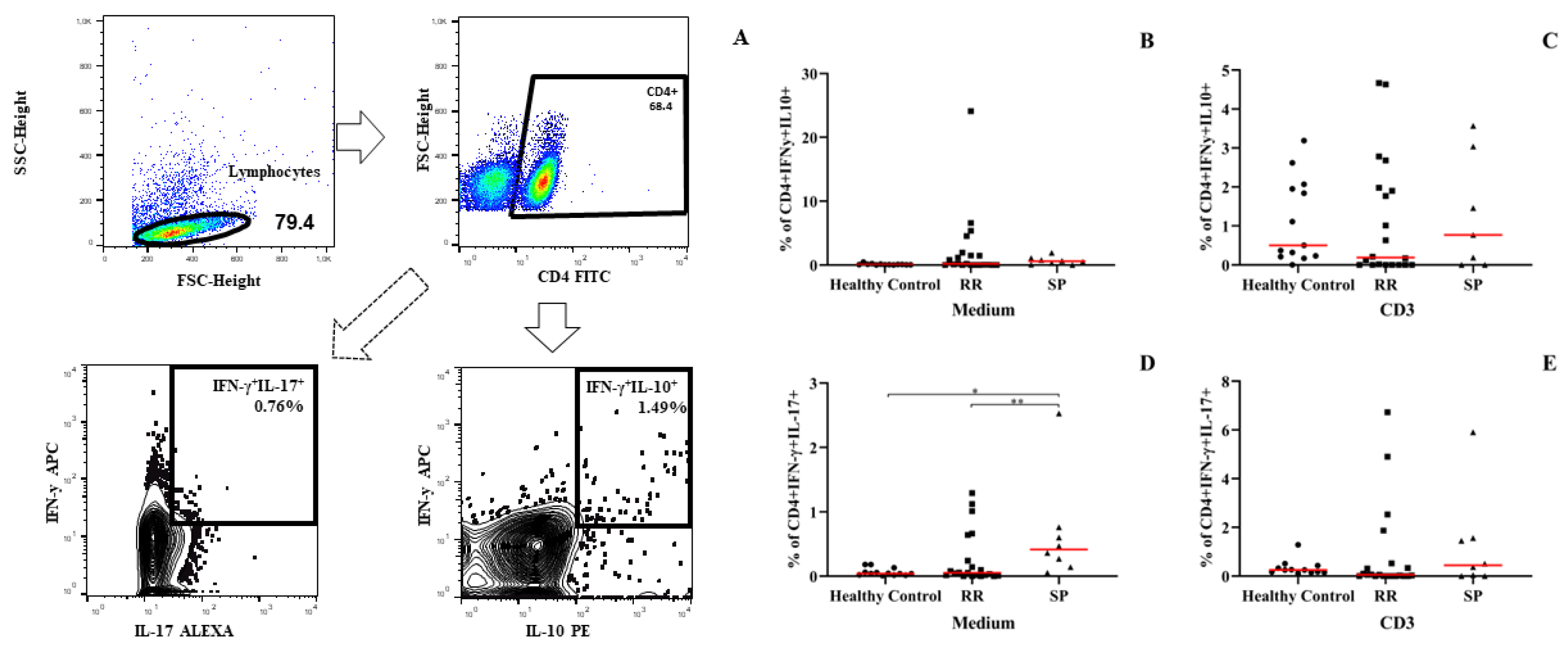
3.7. PBMCs from Patients with the Secondarily Progressive Form Shows an Increase in the Percentage of IFN-γ- and IL-17–Producing Dual Auxiliary T Lymphocytes (TCD4+IFN-γ+IL-17+)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Reich, D.S.; Lucchinetti, C.F.; Calabresi, P.A. Multiple Sclerosis. N. Engl. J. Med. 2018, 378, 169–180. [Google Scholar] [CrossRef]
- da Gama Pereira, A.B.; Sampaio Lacativa, M.C.; da Costa Pereira, F.F.; Papais Alvarenga, R.M. Prevalence of multiple sclerosis in Brazil: A systematic review. Mult. Scler. Relat. Disord. 2015, 4, 572–579. [Google Scholar] [CrossRef]
- Kobelt, G.; Teich, V.; Cavalcanti, M.; Canzonieri, A.M. Burden and cost of multiple sclerosis in Brazil. PLoS ONE 2019, 14, e0208837. [Google Scholar] [CrossRef]
- Lublin, F.D.; Reingold, S.C.; Cohen, J.A.; Cutter, G.R.; Sorensen, P.S.; Thompson, A.J.; Wolinsky, J.S.; Balcer, L.J.; Banwell, B.; Barkhof, F.; et al. Defining the clinical course of multiple sclerosis: The 2013 revisions. Neurology 2014, 83, 278–286. [Google Scholar] [CrossRef] [Green Version]
- Dendrou, C.A.; Fugger, L.; Friese, M.A. Immunopathology of multiple sclerosis. Nat. Rev. Immunol. 2015, 15, 545–558. [Google Scholar] [CrossRef]
- Brasil. Ministério Da Saúde Secretaria De Atenção à Saúde Secretaria De Ciência, Tecnologia e Insumos Estratégicos. 2001. Available online: https://bvsms.saude.gov.br/bvs/saudelegis/sas/2018/poc0011_09_04_2018.html (accessed on 3 March 2022).
- Degre, M.; Dahl, H.; Vandvik, B. Interferon in the serum and cerebrospinal fluid in patients with multiple sclerosis and other neurological disorders. Acta Neurol. Scand. 1976, 53, 152–160. [Google Scholar] [CrossRef]
- Chofflon, M.; Juillard, C.; Juillard, P.; Gauthier, G.; Grau, G.E. Tumor necrosis factor alpha production as a possible predictor of relapse in patients with multiple sclerosis. Eur. Cytokine Netw. 1992, 3, 523–531. [Google Scholar]
- Huang, W.X.; Huang, P.; Link, H.; Hillert, J. Cytokine analysis in multiple sclerosis by competitive RT–PCR: A decreased expression of IL-10 and an increased expression of TNF-alpha in chronic progression. Mult. Scler. 1999, 5, 342–348. [Google Scholar] [CrossRef]
- Kahl, K.G.; Kruse, N.; Faller, H.; Weiss, H.; Rieckmann, P. Expression of tumor necrosis factor-alpha and interferon-gamma mRNA in blood cells correlates with depression scores during an acute attack in patients with multiple sclerosis. Psychoneuroendocrinology 2002, 27, 671–681. [Google Scholar] [CrossRef]
- Cannella, B.; Raine, C.S. The adhesion molecule and cytokine profile of multiple sclerosis lesions. Ann. Neurol. 1995, 37, 424–435. [Google Scholar] [CrossRef]
- Link, J.; Soderstrom, M.; Olsson, T.; Hojeberg, B.; Ljungdahl, A.; Link, H. Increased transforming growth factor-beta, interleukin-4, and interferon-gamma in multiple sclerosis. Ann. Neurol. 1994, 36, 379–386. [Google Scholar] [CrossRef]
- Navikas, V.; Link, H. Review: Cytokines and the pathogenesis of multiple sclerosis. J. Neurosci. Res. 1996, 45, 322–333. [Google Scholar] [CrossRef]
- Killestein, J.; Den Drijver, B.F.; Van der Graaff, W.L.; Uitdehaag, B.M.; Polman, C.H.; Van Lier, R.A. Intracellular cytokine profile in T-cell subsets of multiple sclerosis patients: Different features in primary progressive disease. Mult. Scler. 2001, 7, 145–150. [Google Scholar] [CrossRef]
- Kallaur, A.P.; Oliveira, S.R.; Colado Simao, A.N.; Delicato de Almeida, E.R.; Kaminami Morimoto, H.; Lopes, J.; de Carvalho Jennings Pereira, W.L.; Marques Andrade, R.; Muliterno Pelegrino, L.; Donizete Borelli, S.; et al. Cytokine profile in r multiple sclerosis patients and the association between progression and activity of the disease. Mol. Med. Rep. 2013, 7, 1010–1020. [Google Scholar] [CrossRef] [Green Version]
- Alatab, S.; Maghbooli, Z.; Hossein-Nezhad, A.; Khosrofar, M.; Mokhtari, F. Cytokine profile, Foxp3 and nuclear factor-kB ligand levels in multiple sclerosis subtypes. Minerva Med. 2011, 102, 461–468. [Google Scholar]
- Soldan, S.S.; Alvarez Retuerto, A.I.; Sicotte, N.L.; Voskuhl, R.R. Dysregulation of IL-10 and IL-12p40 in secondary progressive multiple sclerosis. J. Neuroimmunol. 2004, 146, 209–215. [Google Scholar] [CrossRef]
- Huber, A.K.; Wang, L.; Han, P.; Zhang, X.; Ekholm, S.; Srinivasan, A.; Irani, D.N.; Segal, B.M. Dysregulation of the IL-23/IL-17 axis and myeloid factors in secondary progressive MS. Neurology 2014, 83, 1500–1507. [Google Scholar] [CrossRef] [Green Version]
- Babaloo, Z.; Aliparasti, M.R.; Babaiea, F.; Almasi, S.; Baradaran, B.; Farhoudi, M. The role of Th17 cells in patients with relapsing-remitting multiple sclerosis: Interleukin-17A and interleukin-17F serum levels. Immunol. Lett. 2015, 164, 76–80. [Google Scholar] [CrossRef]
- Kallaur, A.P.; Oliveira, S.R.; Simao, A.N.C.; Alfieri, D.F.; Flauzino, T.; Lopes, J.; de Carvalho Jennings Pereira, W.L.; de Meleck Proenca, C.; Borelli, S.D.; Kaimen-Maciel, D.R.; et al. Cytokine Profile in Patients with Progressive Multiple Sclerosis and Its Association with Disease Progression and Disability. Mol. Neurobiol. 2017, 54, 2950–2960. [Google Scholar] [CrossRef]
- Comabella, M.; Balashov, K.; Issazadeh, S.; Smith, D.; Weiner, H.L.; Khoury, S.J. Elevated interleukin-12 in progressive multiple sclerosis correlates with disease activity and is normalized by pulse cyclophosphamide therapy. J. Clin. Investig. 1998, 102, 671–678. [Google Scholar] [CrossRef]
- Fernandez-Paredes, L.; Casrouge, A.; Decalf, J.; de Andres, C.; Villar, L.M.; Perez de Diego, R.; Alonso, B.; Alvarez Cermeno, J.C.; Arroyo, R.; Tejera-Alhambra, M.; et al. Multimarker risk stratification approach at multiple sclerosis onset. Clin. Immunol. 2017, 181, 43–50. [Google Scholar] [CrossRef]
- Dhaiban, S.; Al-Ani, M.; Elemam, N.M.; Maghazachi, A.A. Targeting Chemokines and Chemokine Receptors in Multiple Sclerosis and Experimental Autoimmune Encephalomyelitis. J. Inflamm. Res. 2020, 13, 619–633. [Google Scholar] [CrossRef]
- Adzemovic, M.Z.; Ockinger, J.; Zeitelhofer, M.; Hochmeister, S.; Beyeen, A.D.; Paulson, A.; Gillett, A.; Thessen Hedreul, M.; Covacu, R.; Lassmann, H.; et al. Expression of Ccl11 associates with immune response modulation and protection against neuroinflammation in rats. PLoS ONE 2012, 7, e39794. [Google Scholar] [CrossRef] [Green Version]
- Tejera-Alhambra, M.; Casrouge, A.; de Andres, C.; Seyfferth, A.; Ramos-Medina, R.; Alonso, B.; Vega, J.; Fernandez-Paredes, L.; Albert, M.L.; Sanchez-Ramon, S. Plasma biomarkers discriminate clinical forms of multiple sclerosis. PLoS ONE 2015, 10, e0128952. [Google Scholar] [CrossRef] [Green Version]
- Ochi, H.; Osoegawa, M.; Wu, X.M.; Minohara, M.; Horiuchi, I.; Murai, H.; Furuya, H.; Kira, J. Increased IL-13 but not IL-5 production by CD4-positive T cells and CD8-positive T cells in multiple sclerosis during relapse phase. J. Neurol. Sci. 2002, 201, 45–51. [Google Scholar] [CrossRef]
- Olsson, T. Cytokines in neuroinflammatory disease: Role of myelin autoreactive T cell production of interferon-gamma. J. Neuroimmunol. 1992, 40, 211–218. [Google Scholar] [CrossRef]
- Sanvito, L.; Constantinescu, C.S.; Gran, B.; Hart, B.A. The multifaceted role of interferon-γ in central nervous system autoimmune demyelination. Open Autoimmun. J. 2010, 2, 151–159. [Google Scholar] [CrossRef] [Green Version]
- Panitch, H.S.; Hirsch, R.L.; Schindler, J.; Johnson, K.P. Treatment of multiple sclerosis with gamma interferon: Exacerbations associated with activation of the immune system. Neurology 1987, 37, 1097–1102. [Google Scholar] [CrossRef] [Green Version]
- Arellano, G.; Ottum, P.A.; Reyes, L.I.; Burgos, P.I.; Naves, R. Stage-Specific Role of Interferon-Gamma in Experimental Autoimmune Encephalomyelitis and Multiple Sclerosis. Front. Immunol. 2015, 6, 492. [Google Scholar] [CrossRef] [Green Version]
- Harrington, L.E.; Hatton, R.D.; Mangan, P.R.; Turner, H.; Murphy, T.L.; Murphy, K.M.; Weaver, C.T. Interleukin 17-producing CD4+ effector T cells develop via a lineage distinct from the T helper type 1 and 2 lineages. Nat. Immunol. 2005, 6, 1123–1132. [Google Scholar] [CrossRef]
- Donninelli, G.; Studer, V.; Brambilla, L.; Zecca, C.; Peluso, D.; Laroni, A.; Michelis, D.; Mantegazza, R.; Confalonieri, P.; Volpe, E. Immune Soluble Factors in the Cere-brospinal Fluid of Progressive Multiple Sclerosis Patients Segregate into Two Groups. Front. Immunol. 2021, 12, 633167. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | Clinical Form | N | Mean | Median | SD | Minimum | Maximum | |
|---|---|---|---|---|---|---|---|---|
| Age (year) | F | CIS | 1 | 27.0 | 27 | NaN | 27 | 27 |
| HC | 20 | 41.1 | 43 | 10.6 | 21 | 57 | ||
| RR | 17 | 40.1 | 39 | 11.6 | 24 | 62 | ||
| SP | 5 | 52.2 | 57 | 14.3 | 36 | 67 | ||
| M | CIS | 1 | 37.0 | 37 | NaN | 37 | 37 | |
| HC | 1 | 34.0 | 34 | NaN | 34 | 34 | ||
| PP | 1 | 39.0 | 39 | NaN | 39 | 39 | ||
| RR | 4 | 32.8 | 33.0 | 11.5 | 19 | 46 | ||
| SP | 1 | 60.0 | 60 | NaN | 60 | 60 |
| Clinical Form | N | Mean | Median | SD | Minimum | Maximum | |
|---|---|---|---|---|---|---|---|
| Treatment time (Months) | CIS | 2 | 1.50 | 1.50 | 2.12 | 0 | 3 |
| PP | 1 | 21.00 | 21 | NaN | 21 | 21 | |
| RR | 21 | 48.05 | 31 | 52.34 | 0 | 162 | |
| SP | 6 | 106.17 | 102.50 | 67.99 | 24 | 206 |
| Treatment type | N | Mean | Median | SD | Minimum | Maximum | |
|---|---|---|---|---|---|---|---|
| Treatment time (months) | Untreated | 3 | 0.00 | 0 | 0.00 | 0 | 0 |
| IFN-β 1a | 14 | 83.57 | 82.0 | 65.49 | 2 | 206 | |
| Glatiramer Acetate | 7 | 56.57 | 45 | 51.95 | 3 | 156 | |
| Dimethyl Fumarate | 1 | 5.00 | 5 | NaN | 5 | 5 | |
| Fingolimod (FTY720) | 4 | 22.50 | 24.0 | 8.35 | 11 | 31 | |
| Corticosteroids | 1 | 9.00 | 9 | NaN | 9 | 9 |
| Cytokine | R Spearman | p Value | p Value Summary |
|---|---|---|---|
| IL-1β | 0.05285 | 0.7935 | ns |
| IL-2 | −0.2934 | 0.1374 | ns |
| IL-4 | 0.4814 | 0.0200 | * |
| IL-5 | 0.3669 | 0.0597 | ns |
| IL-6 | −0.05699 | 0.7777 | ns |
| IL-8 | −0.05260 | 0.7944 | ns |
| IL-10 | −0.3281 | 0.0947 | ns |
| IL-12 | 0.1336 | 0.5066 | ns |
| IL-13 | 0.1654 | 0.4096 | ns |
| IL-15 | −0.03531 | 0.8612 | ns |
| IL-23 | −0.005240 | 0.9793 | ns |
| IL-33 | −0.09314 | 0.6440 | ns |
| EOTAXIN | 0.1187 | 0.5555 | ns |
| IP-10 | −0.08088 | 0.6884 | ns |
| IFN-γ | 0.04964 | 0.8058 | ns |
| TNF-α | −0.05021 | 0.8036 | ns |
| BDNF | 0.001696 | 0.9933 | ns |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dias de Sousa, M.A.; Desidério, C.S.; da Silva Catarino, J.; Trevisan, R.O.; Alves da Silva, D.A.; Rocha, V.F.R.; Bovi, W.G.; Timoteo, R.P.; Bonatti, R.C.F.; da Silva, A.E.; et al. Role of Cytokines, Chemokines and IFN-γ+ IL-17+ Double-Positive CD4+ T Cells in Patients with Multiple Sclerosis. Biomedicines 2022, 10, 2062. https://doi.org/10.3390/biomedicines10092062
Dias de Sousa MA, Desidério CS, da Silva Catarino J, Trevisan RO, Alves da Silva DA, Rocha VFR, Bovi WG, Timoteo RP, Bonatti RCF, da Silva AE, et al. Role of Cytokines, Chemokines and IFN-γ+ IL-17+ Double-Positive CD4+ T Cells in Patients with Multiple Sclerosis. Biomedicines. 2022; 10(9):2062. https://doi.org/10.3390/biomedicines10092062
Chicago/Turabian StyleDias de Sousa, Marlos Aureliano, Chamberttan Souza Desidério, Jonatas da Silva Catarino, Rafael Obata Trevisan, Djalma Alexandre Alves da Silva, Vinicius Ferreira Resende Rocha, Weslley Guimarães Bovi, Rodolfo Pessato Timoteo, Renata Cristina Franzon Bonatti, Alex Eduardo da Silva, and et al. 2022. "Role of Cytokines, Chemokines and IFN-γ+ IL-17+ Double-Positive CD4+ T Cells in Patients with Multiple Sclerosis" Biomedicines 10, no. 9: 2062. https://doi.org/10.3390/biomedicines10092062