
Incident Atrial Fibrillation and In-Hospital Mortality in SARS-CoV-2 Patients

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Outcomes and Covariates
2.3. Compliance with Ethical Standards
2.4. Statistical Analysis
3. Results
3.1. Incident Atrial Fibrillation
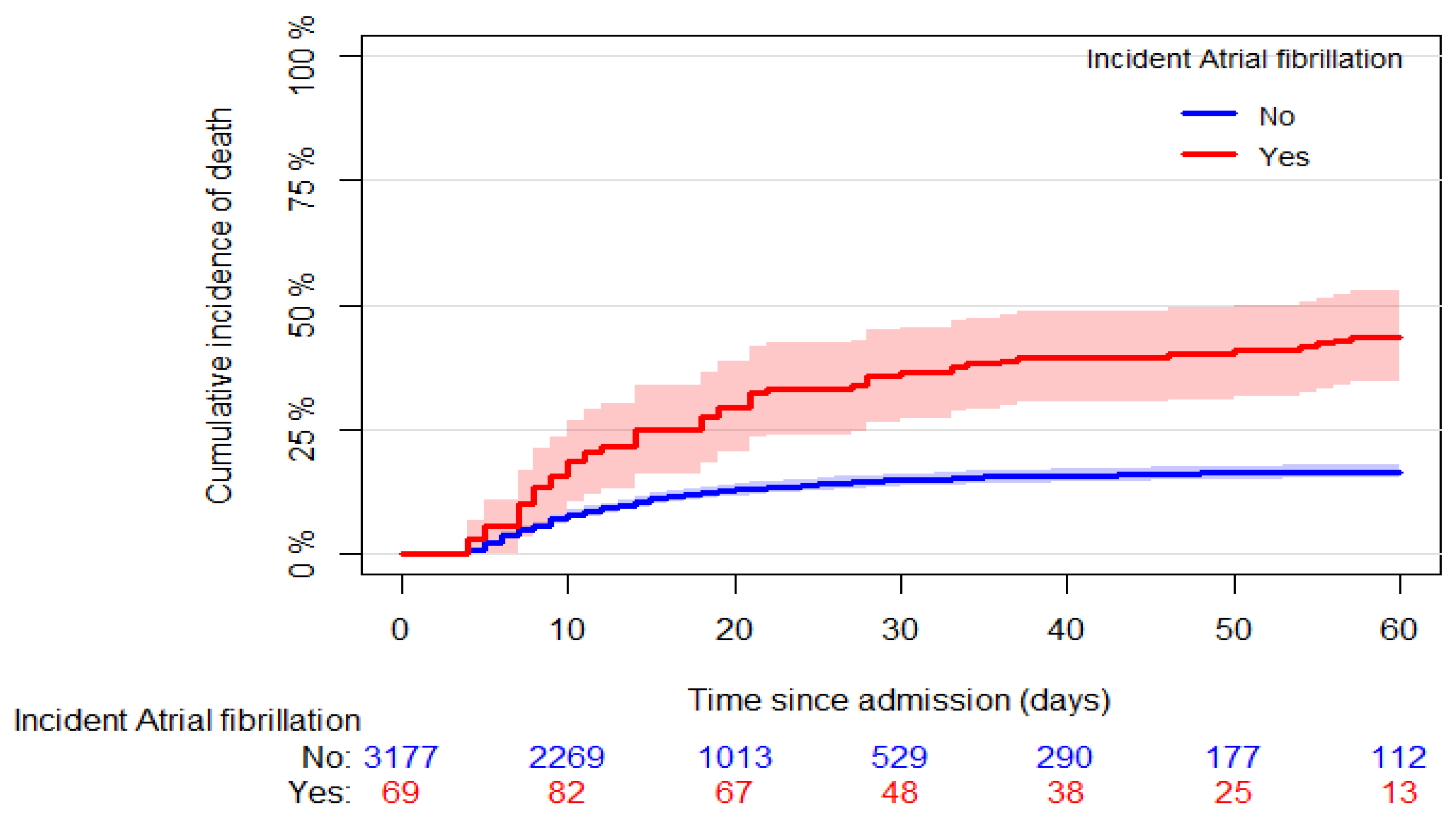
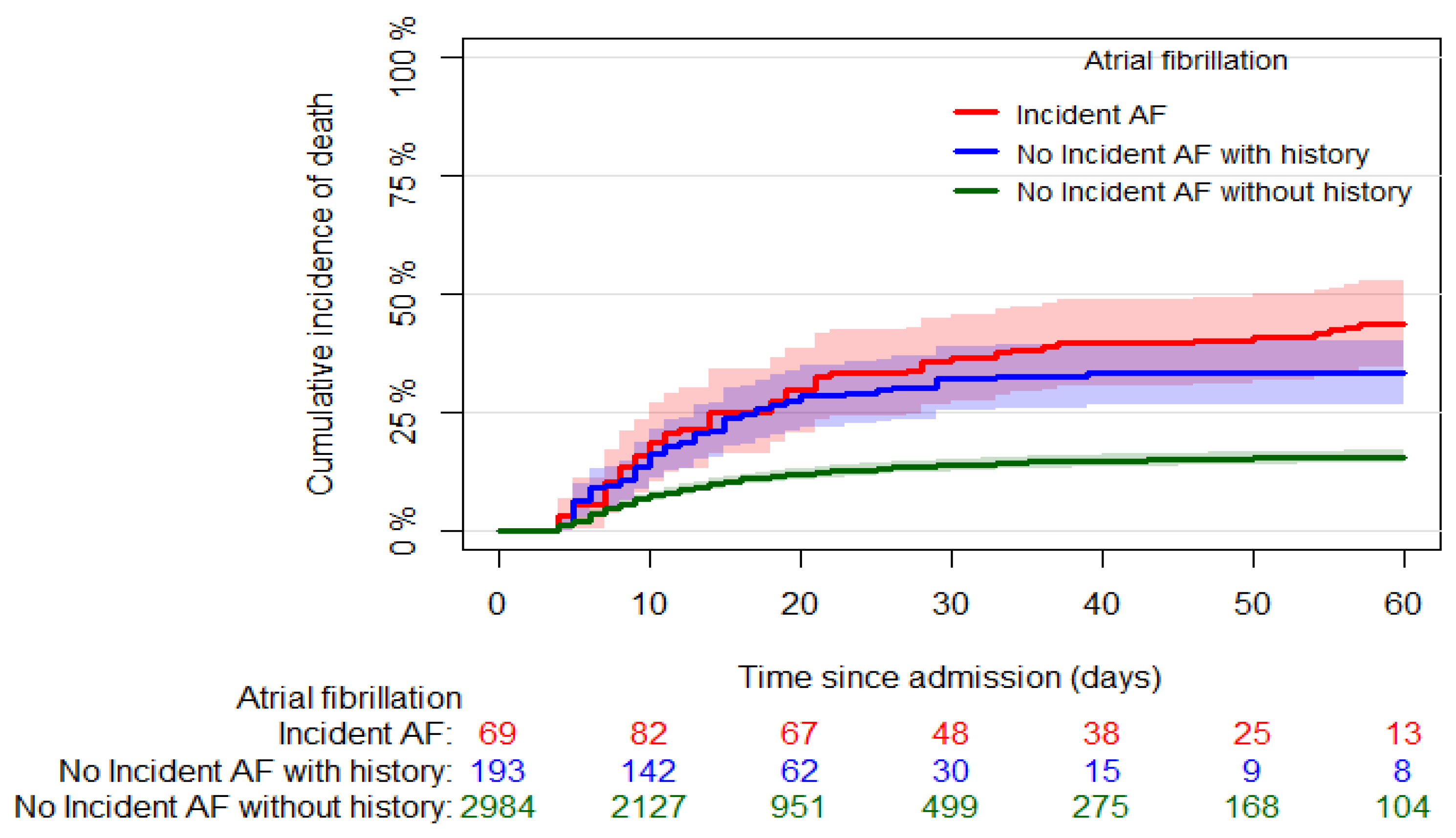
3.2. All-Cause Mortality
4. Discussion
4.1. Incident AF in COVID-19 Patients
4.2. Incident AF and In-Hospital Death in COVID-19 Patients
4.3. Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sardu, C.; Gambardella, J.; Morelli, M.B.; Wang, X.; Marfella, R.; Santulli, G. Hypertension, Thrombosis, Kidney Failure, and Diabetes: Is COVID-19 an Endothelial Disease? A Comprehensive Evaluation of Clinical and Basic Evidence. J. Clin. Med. 2020, 9, 1417. [Google Scholar] [CrossRef] [PubMed]
- Ruzzenenti, G.; Maloberti, A.; Giani, V.; Biolcati, M.; Leidi, F.; Monticelli, M.; Grasso, E.; Cartella, I.; Palazzini, M.; Garatti, L.; et al. COVID and Cardiovascular Diseases: Direct and Indirect Damages and Future Perspective. High Blood Press. Cardiovasc. Prev. 2021, 28, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Mancusi, C.; Grassi, G.; Borghi, C.; Ferri, C.; Muiesan, M.L.; Volpe, M.; Iaccarino, G.; SARS-RAS Investigator Group. Clinical Characteristics and Outcomes of Patients with COVID-19 Infection: The Results of the SARS-RAS Study of the Italian Society of Hypertension. High Blood Press. Cardiovasc. Prev. 2021, 28, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Lakkireddy, D.R.; Chung, M.K.; Gopinathannair, R.; Patton, K.K.; Gluckman, T.J.; Turagam, M.; Cheung, J.; Patel, P.; Sotomonte, J.; Lampert, R.; et al. Guidance for Cardiac Electrophysiology During the COVID-19 Pandemic from the Heart Rhythm Society COVID-19 Task Force; Electrophysiology Section of the American College of Cardiology; and the Electrocardiography and Arrhythmias Committee of the Council on Clinical Cardiology, American Heart Association. Circulation 2020, 141, e823–e831. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus—Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Xiong, T.-Y.; Redwood, S.; Prendergast, B.; Chen, M. Coronaviruses and the cardiovascular system: Acute and long-term implications. Eur. Heart J. 2020, 41, 1798–1800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maloberti, A.; Ughi, N.; Bernasconi, D.P.; Rebora, P.; Cartella, I.; Grasso, E.; Lenoci, D.; Del Gaudio, F.; Algeri, M.; Scarpellini, S.; et al. Heart Rate in Patients with SARS-CoV-2 Infection: Prevalence of High Values at Discharge and Relationship with Disease Severity. J. Clin. Med. 2021, 10, 5590. [Google Scholar] [CrossRef]
- Musikantow, D.R.; Turagam, M.K.; Sartori, S.; Chu, E.; Kawamura, I.; Shivamurthy, P.; Bokhari, M.; Oates, C.; Zhang, C.; Pumill, C.; et al. Atrial Fibrillation in Patients Hospitalized With COVID-19. JACC Clin. Electrophysiol. 2021, 7, 1120–1130. [Google Scholar] [CrossRef]
- Li, Z.; Shao, W.; Zhang, J.; Ma, J.; Huang, S.; Yu, P.; Zhu, W.; Liu, X. Prevalence of Atrial Fibrillation and Associated Mortality among Hospitalized Patients With COVID-19: A Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2021, 8, 720129. [Google Scholar] [CrossRef]
- Pepe, M.; Napoli, G.; Brindicci, G.; Carulli, E.; Nestola, P.L.; Santoro, C.R.; Biondi-Zoccai, G.; Giordano, A.; D’Ascenzo, F.; Cirillo, P.; et al. Prognostic value of 12-leads admission electrocardiogram in low-risk patients hospitalized for COVID-19. Minerva Medica 2021. Epub ahead of print. [Google Scholar] [CrossRef]
- Paris, S.; Inciardi, R.M.; Lombardi, C.M.; Tomasoni, D.; Ameri, P.; Carubelli, V.; Agostoni, P.; Canale, C.; Carugo, S.; Danzi, G.; et al. Implications of atrial fibrillation on the clinical course and outcomes of hospitalized COVID-19 patients: Results of the Cardio-COVID-Italy multicentre study. EP Eur. 2021, 23, 1603–1611. [Google Scholar] [CrossRef]
- Zuin, M.; Rigatelli, G.; Bilato, C.; Zanon, F.; Zuliani, G.; Roncon, L. Pre-existing atrial fibrillation is associated with increased mortality in COVID-19 Patients. J. Interv. Card. Electrophysiol. 2021, 62, 231–238. [Google Scholar] [CrossRef]
- Mountantonakis, S.E.; Saleh, M.; Fishbein, J.; Gandomi, A.; Lesser, M.; Chelico, J.; Gabriels, J.; Qiu, M.; Epstein, L.M.; Northwell COVID-19 Research Consortium. Atrial fibrillation is an independent predictor for in-hospital mortality in patients admitted with SARS-CoV-2 infection. Heart Rhythm 2021, 18, 501–507. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612, Erratum in Ann. Intern. Med. 2011, 155, 408. [Google Scholar] [CrossRef]
- Bhatla, A.; Mayer, M.M.; Adusumalli, S.; Hyman, M.C.; Oh, E.; Tierney, A.; Moss, J.; Chahal, A.A.; Anesi, G.; Denduluri, S.; et al. COVID-19 and cardiac arrhythmias. Heart Rhythm 2020, 17, 1439–1444. [Google Scholar] [CrossRef]
- Lip, G.Y.; Genaidy, A.; Tran, G.; Marroquin, P.; Estes, C. Incident atrial fibrillation and its risk prediction in patients developing COVID-19: A machine learning based algorithm approach. Eur. J. Intern. Med. 2021, 91, 53–58. [Google Scholar] [CrossRef]
- Sanz, A.P.; Tahoces, L.S.; Pérez, R.O.; Ferrer, E.G.; Recalde, S.; Gómez, J.L.Z. New-onset atrial fibrillation during COVID-19 infection predicts poor prognosis. Cardiol. J. 2021, 28, 34–40. [Google Scholar] [CrossRef]
- Chen, Q.; Xu, L.; Dai, Y.; Ling, Y.; Mao, J.; Qian, J.; Zhu, W.; Di, W.; Ge, J. Cardiovascular manifestations in severe and critical patients with COVID-19. Clin. Cardiol. 2020, 43, 796–802. [Google Scholar] [CrossRef]
- Boriani, G.; Fauchier, L.; Aguinaga, L.; Beattie, J.M.; Lundqvist, C.B.; Cohen, A.; Dan, G.-A.; Genovesi, S.; Israel, C.; Joung, B.; et al. European Heart Rhythm Association (EHRA) consensus document on management of arrhythmias and cardiac electronic devices in the critically ill and post-surgery patient, endorsed by Heart Rhythm Society (HRS), Asia Pacific Heart Rhythm Society (APHRS), Cardiac Arrhythmia Society of Southern Africa (CASSA), and Latin American Heart Rhythm Society (LAHRS). Europace 2018, 21, 7–8. [Google Scholar] [CrossRef]
- Ambrus, D.B.; Benjamin, E.; Bajwa, E.K.; Hibbert, K.A.; Walkey, A.J. Risk factors and outcomes associated with new-onset atrial fibrillation during acute respiratory distress syndrome. J. Crit. Care 2015, 30, 994–997. [Google Scholar] [CrossRef] [Green Version]
- Klouwenberg, P.M.C.K.; Frencken, J.F.; Kuipers, S.; Ong, D.S.Y.; Peelen, L.M.; van Vught, L.A.; Schultz, M.J.; van der Poll, T.; Bonten, M.J.; Cremer, O.L.; et al. Incidence, Predictors, and Outcomes of New-Onset Atrial Fibrillation in Critically Ill Patients with Sepsis. A Cohort Study. Am. J. Respir. Crit. Care Med. 2017, 195, 205–211. [Google Scholar] [CrossRef]
- Walkey, A.J.; Hammill, B.G.; Curtis, L.H.; Benjamin, E.J. Long-term Outcomes Following Development of New-Onset Atrial Fibrillation During Sepsis. Chest 2014, 146, 1187–1195. [Google Scholar] [CrossRef] [Green Version]
- Steinberg, I.; Brogi, E.; Pratali, L.; Trunfio, D.; Giuliano, G.; Bignami, E.; Forfori, F. Atrial Fibrillation in Patients with Septic Shock: A One-Year Observational Pilot Study. Turk. J. Anaesthesiol. Reanim. 2019, 47, 213–219. [Google Scholar] [CrossRef]
- Meierhenrich, R.; Steinhilber, E.; Eggermann, C.; Weiss, M.; Voglic, S.; Bögelein, D.; Gauss, A.; Georgieff, M.; Stahl, W. Incidence and prognostic impact of new-onset atrial fibrillation in patients with septic shock: A prospective observational study. Crit. Care 2010, 14, R108. [Google Scholar] [CrossRef] [Green Version]
- Xiao, F.-P.; Chen, M.-Y.; Wang, L.; He, H.; Jia, Z.-Q.; Kuai, L.; Zhou, H.-B.; Liu, M.; Hong, M. Outcomes of new-onset atrial fibrillation in patients with sepsis: A systematic review and meta-analysis of 225,841 patients. Am. J. Emerg. Med. 2021, 42, 23–30. [Google Scholar] [CrossRef]
- Wu, Z.; Fang, J.; Wang, Y.; Chen, F. Prevalence, Outcomes, and Risk Factors of New-Onset Atrial Fibrillation in Critically Ill Patients. Int. Heart J. 2020, 61, 476–485. [Google Scholar] [CrossRef]
- Kanjanahattakij, N.; Rattanawong, P.; Krishnamoorthy, P.; Horn, B.; Chongsathidkiet, P.; Garvia, V.; Putthapiban, P.; Sirinvaravong, N.; Figueredo, V.M. New-onset atrial fibrillation is associated with increased mortality in critically ill patients: A systematic review and meta-analysis. Acta Cardiol. 2018, 74, 162–169. [Google Scholar] [CrossRef]
- Yoshida, T.; Fujii, T.; Uchino, S.; Takinami, M. Epidemiology, prevention, and treatment of new-onset atrial fibrillation in critically ill: A systematic review. J. Intensiv. Care 2015, 3, 19. [Google Scholar] [CrossRef] [Green Version]
- Noori, M.; Nejadghaderi, S.A.; Sullman, M.J.M.; Carson-Chahhoud, K.; Kolahi, A.; Safiri, S. Epidemiology, prognosis and management of potassium disorders in COVID-19. Rev. Med. Virol. 2021, 32, e2262. [Google Scholar] [CrossRef]
- Genovesi, S.; Rebora, P.; Occhino, G.; Rossi, E.; Maloberti, A.; Belli, M.; Bonfanti, P.; Giannattasio, C.; Rossetti, C.; Epis, O.M.; et al. Atrial Fibrillation and Clinical Outcomes in a Cohort of Hospitalized Patients with SARS-CoV-2 Infection and Chronic Kidney Disease. J. Clin. Med. 2021, 10, 4108. [Google Scholar] [CrossRef]
- Kelesoglu, S.; Yilmaz, Y.; Ozkan, E.; Calapkorur, B.; Gok, M.; Dursun, Z.B.; Kilic, A.U.; Demirelli, S.; Simsek, Z.; Elcık, D. New onset atrial fibrilation and risk faktors in COVID-19. J. Electrocardiol. 2021, 65, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Peltzer, B.; Manocha, K.K.; Ying, X.; Kirzner, J.; Ip, J.E.; Thomas, G.; Liu, C.F.; Markowitz, S.M.; Lerman, B.B.; Safford, M.M.; et al. Outcomes and mortality associated with atrial arrhythmias among patients hospitalized with COVID-19. J. Cardiovasc. Electrophysiol. 2020, 31, 3077–3085. [Google Scholar] [CrossRef] [PubMed]
- Gawałko, M.; Kapłon-Cieślicka, A.; Hohl, M.; Dobrev, D.; Linz, D. COVID-19 associated atrial fibrillation: Incidence, putative mechanisms and potential clinical implications. IJC Heart Vasc. 2020, 30, 100631. [Google Scholar] [CrossRef] [PubMed]
- South, A.M.; Diz, D.I.; Chappell, M.C. COVID-19, ACE2, and the cardiovascular consequences. Am. J. Physiol. Heart Circ. Physiol. 2020, 318, H1084–H1090. [Google Scholar] [CrossRef] [Green Version]
- Seizer, P.; Gawaz, M.; May, A.E. Cyclophilin A and EMMPRIN (CD147) in cardiovascular diseases. Cardiovasc. Res. 2014, 102, 17–23. [Google Scholar] [CrossRef] [Green Version]
- Bagnato, G.; Imbalzano, E.; Aragona, C.O.; Ioppolo, C.; Di Micco, P.; La Rosa, D.; Costa, F.; Micari, A.; Tomeo, S.; Zirilli, N.; et al. New-Onset Atrial Fibrillation and Early Mortality Rate in COVID-19 Patients: Association with IL-6 Serum Levels and Respiratory Distress. Medicina 2022, 58, 530. [Google Scholar] [CrossRef]
- Sano, T.; Matsumoto, S.; Ikeda, T.; Kuroda, S.; Kitai, T.; Yonetsu, T.; Kohsaka, S.; Torii, S.; Node, K.; Matsue, Y. New-Onset Atrial Fibrillation in Patients With Coronavirus Disease 2019 (COVID-19) and Cardiovascular Disease―Insights From the CLAVIS-COVID Registry. Circ. J. 2022. Epub ahead of print. [Google Scholar] [CrossRef]
- Ergün, B.; Ergan, B.; Sözmen, M.K.; Küçük, M.; Yakar, M.N.; Cömert, B.; Gökmen, A.N.; Yaka, E. New-onset atrial fibrillation in critically ill patients with coronavirus disease 2019 (COVID-19). J. Arrhythmia 2021, 37, 1196–1204. [Google Scholar] [CrossRef]
- García-Granja, P.E.; Veras, C.; Aparisi, Á.; Amat-Santos, I.J.; Catalá, P.; Marcos, M.; Cabezón, G.; Candela, J.; Gil, J.F.; Uribarri, A.; et al. Atrial fibrillation in patients with SARS-CoV-2 infection. Med. Clínica 2021, 157, 58–63. [Google Scholar] [CrossRef]
- Capotosto, L.; Nguyen, B.L.; Ciardi, M.R.; Mastroianni, C.; Vitarelli, A. Heart, COVID-19, and echocardiography. Echocardiography 2020, 37, 1454–1464. [Google Scholar] [CrossRef]
- Polcwiartek, C.; Krogager, M.L.; Andersen, M.P.; Butt, J.H.; Pallisgaard, J.; Fosbøl, E.; Schou, M.; Bhatt, D.L.; Singh, A.; Køber, L.; et al. Prognostic implications of serial high-sensitivity cardiac troponin testing among patients with COVID-19: A Danish nationwide registry-based cohort study. Am. Heart J. Plus Cardiol. Res. Pract. 2022, 14, 100131. [Google Scholar] [CrossRef]
- Selçuk, M.; Keskin, M.; Çınar, T.; Günay, N.; Doğan, S.; Çiçek, V.; Kılıç, Ş.; Asal, S.; Yavuz, S.; Keser, N.; et al. Prognostic significance of N-Terminal Pro-BNP in patients with COVID-19 pneumonia without previous history of heart failure. J. Cardiovasc. Thorac. Res. 2021, 13, 141–145. [Google Scholar] [CrossRef]
- Khamis, F.; Memish, Z.; Al Bahrani, M.; Al Dowaiki, S.; Pandak, N.; Al Bolushi, Z.; Al Salmi, I.; Al-Zakwani, I. Prevalence and predictors of in-hospital mortality of patients hospitalized with COVID-19 infection. J. Infect. Public Health 2021, 14, 759–765. [Google Scholar] [CrossRef]
- Armstrong, R.A.; Kane, A.D.; Cook, T.M. Outcomes from intensive care in patients with COVID-19: A systematic review and meta-analysis of observational studies. Anaesthesia 2020, 75, 1340–1349. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Overall | Incident AF = No | Incident AF = Yes | p | Missing (%) | ||
|---|---|---|---|---|---|---|
| n | 3435 | 3290 | 145 | |||
| Demographic variables | ||||||
| Male, n (%) | 2233 (65.0) | 2129 (64.7) | 104 (71.7) | 0.1 | 0 | |
| Age (years) (median (I–III quartiles)) | 65 (53, 77) | 64 (53, 76) | 73 (64, 81) | <0.001 | 0 | |
| Anamnestic variables | ||||||
| Time to incident AF (days) (median (I–III quartiles)) | 3 (0, 12) | - | 30 (0, 12) | - | 0 | |
| History of AF, n (%) | 218 (6.3) | 203 (6.2) | 15 (10.3) | 0.065 | 0 | |
| Non-permanent AF, n (%) | 101 (46.3) | 86 (42.3) | 15 (100.0) | <0.001 | 0 | |
| Permanent AF, n (%) | 117 (53.7) | 117 (57.6) | 0 (0.0) | - | 0 | |
| Chronic Coronary Syndrome, n (%) | 314 (9.2) | 299 (9.1) | 15 (10.3) | 0.733 | 0.6 | |
| Heart failure, n (%) | 160 (4.7) | 148 (4.5) | 12 (8.3) | 0.059 | 0.6 | |
| Peripheral vascular disease, (%) | 226 (6.6) | 215 (6.6) | 11 (7.6) | 0.759 | 0.6 | |
| Previous stroke, n (%) | 287 (8.4) | 270 (8.3) | 17 (11.7) | 0.188 | 0.6 | |
| Dementia, n (%) | 235 (6.9) | 224 (6.9) | 11 (7.6) | 0.862 | 0.6 | |
| COPD, n (%) | 298 (8.7) | 283 (8.7) | 15 (10.3) | 0.579 | 0.6 | |
| Advanced liver disease, n (%) | 133 (3.9) | 131 (4.0) | 2 (1.4) | 0.17 | 0.8 | |
| Cancer (%) | 341 (10.1) | 326 (10.0) | 15 (10.4) | 0.998 | 1.3 | |
| Diabetes mellitus, n (%) | 584 (17.1) | 554 (17.0) | 30 (20.7) | 0.291 | 0.6 | |
| Biochemical variables | ||||||
| Creatinine (mg/dL) (mean (SD)) | 1.17 (1.03) | 1.16 (1.02) | 1.42 (1.19) | 0.005 | 6.6 | |
| eGFR (mL/min) (mean (SD)) | 73.9 (26.4) | 74.4 (26.4) | 62.0 (25.6) | <0.001 | 6.6 | |
| CKD (eGFR < 60 mL/min), n (%) | 929 (28.9) | 871 (28.3) | 58 (43.0) | <0.001 | 6.6 | |
| Hemoglobin (g/dL) (mean (SD)) | 12.7 (1.9) | 12.7 (1.9) | 12.4 (2.0) | 0.08 | 4.5 | |
| Platelet (103/µL) (mean (SD)) | 221.9 (96.4) | 222.9 (96.3) | 199.6 (95.4) | 0.005 | 4.5 | |
| Lymphocytes (103/µL) (median (I–III quartiles)) | 1.01 (0.70, 1.42) | 1.03 (0.72, 1.43) | 0.75 (0.55, 1.07) | <0.001 | 7 | |
| C Reactive Protein (mg/L) (median (I–III quartiles)) | 64.2 (25.0, 121.6) | 63.1 (24.5, 119.0) | 90.0 (51.5, 168.0) | <0.001 | 11.2 | |
| Therapies | ||||||
| RAAS inhibitors, n (%) | 1050 (32.9) | 994 (32.5) | 56 (41.2) | 0.045 | 7.1 | |
| Beta blockers, n (%) | 731 (21.8) | 677 (21.1) | 54 (37.8) | <0.001 | 2.6 | |
| Antiarrhythmic, n (%) | 108 (3.2) | 95 (3.0) | 13 (9.0) | <0.001 | 2.5 | |
| Digoxin, n (%) | 15 (0.5) | 15 (0.5) | 0 (0.0) | 0.907 | 9.4 | |
| Anticoagulant, n (%) | 360 (10.7) | 351 (10.9) | 9 (6.3) | 0.111 | 1.8 | |
| Antiplatelet, n (%) | 567 (18.2) | 535 (17.8) | 32 (26.2) | 0.025 | 9.2 | |
| Antidiabetic, n (%) | 422 (13.4) | 404 (13.4) | 18 (14.8) | 0.765 | 8.6 | |
| Statins, n (%) | 361 (11.5) | 339 (11.2) | 22 (18.0) | 0.031 | 8.6 | |
| Hospitalization variables | ||||||
| Hospital length (days) (median (I–III quartiles)) | 13 (8, 22) | 12 (7, 21) | 22 (13, 41) | <0.001 | 0 | |
| ICU admission, n (%) | 454 (13.6) | 397 (12.4) | 57 * (39.3) | <0.001 | 2.7 | |
| Time to ICU admission (days) (median (I–III quartiles)) | 1 (0, 4) | 1 (0, 4) | 4 (0, 7) | 0.003 | 0.9 | |
| Outcome | ||||||
| All-cause death, n (%) | 611 (17.8) | 557 (16.9) | 54 (37.2) | <0.001 | 0 | |
| Number = 2725; Incident AF = 121 | ||||
|---|---|---|---|---|
| Parameter | HR | 95% Confidence Interval | p-Value | |
| Male (yes vs. no) | 1.217 | 0.806 | 1.838 | 0.3497 |
| Age (years) | 1.041 | 1.022 | 1.060 | <0.0001 |
| History of non-permanent AF (yes vs. no) | 2.720 | 1.508 | 4.907 | 0.0009 |
| Lymphocytes (103/µL) | 0.584 | 0.384 | 0.888 | 0.0119 |
| eGFR (mL/min) | 0.988 | 0.980 | 0.996 | 0.0019 |
| ICU admission (yes vs. no-time dependent) | 5.311 | 3.397 | 8.302 | <0.0001 |
| Number = 2755; Death = 472. | ||||
|---|---|---|---|---|
| Parameter | HR | 95% Confidence Interval | p-Value | |
| Male (yes vs. no) | 1.315 | 1.064 | 1.626 | 0.0114 |
| Age (years) | 1.057 | 1.047 | 1.067 | <0.0001 |
| Dementia (yes vs. no) | 1.373 | 1.045 | 1.803 | 0.0228 |
| Platelet (103/µL) | 0.997 | 0.996 | 0.998 | <0.00001 |
| Lymphocytes (103/µL) | 0.843 | 0.725 | 0.982 | 0.0279 |
| CRP (mg/L) | 1.004 | 1.003 | 1.005 | <0.0001 |
| eGFR (mL/min) | 0.990 | 0.986 | 0.994 | <0.0001 |
| Incident AF (yes vs. no-time dependent) | 1.405 | 1.027 | 1.922 | 0.0333 |
| ICU admission directly from ED (yes vs. no) | 1.759 | 1.292 | 2.395 | 0.0003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maloberti, A.; Giannattasio, C.; Rebora, P.; Occhino, G.; Ughi, N.; Biolcati, M.; Gualini, E.; Rizzi, J.G.; Algeri, M.; Giani, V.; et al. Incident Atrial Fibrillation and In-Hospital Mortality in SARS-CoV-2 Patients. Biomedicines 2022, 10, 1940. https://doi.org/10.3390/biomedicines10081940
Maloberti A, Giannattasio C, Rebora P, Occhino G, Ughi N, Biolcati M, Gualini E, Rizzi JG, Algeri M, Giani V, et al. Incident Atrial Fibrillation and In-Hospital Mortality in SARS-CoV-2 Patients. Biomedicines. 2022; 10(8):1940. https://doi.org/10.3390/biomedicines10081940
Chicago/Turabian StyleMaloberti, Alessandro, Cristina Giannattasio, Paola Rebora, Giuseppe Occhino, Nicola Ughi, Marco Biolcati, Elena Gualini, Jacopo Giulio Rizzi, Michela Algeri, Valentina Giani, and et al. 2022. "Incident Atrial Fibrillation and In-Hospital Mortality in SARS-CoV-2 Patients" Biomedicines 10, no. 8: 1940. https://doi.org/10.3390/biomedicines10081940