
Assessment of Preoperative TSH Serum Level and Thyroid Cancer Occurrence in Patients with AUS/FLUS Thyroid Nodule Diagnosis

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
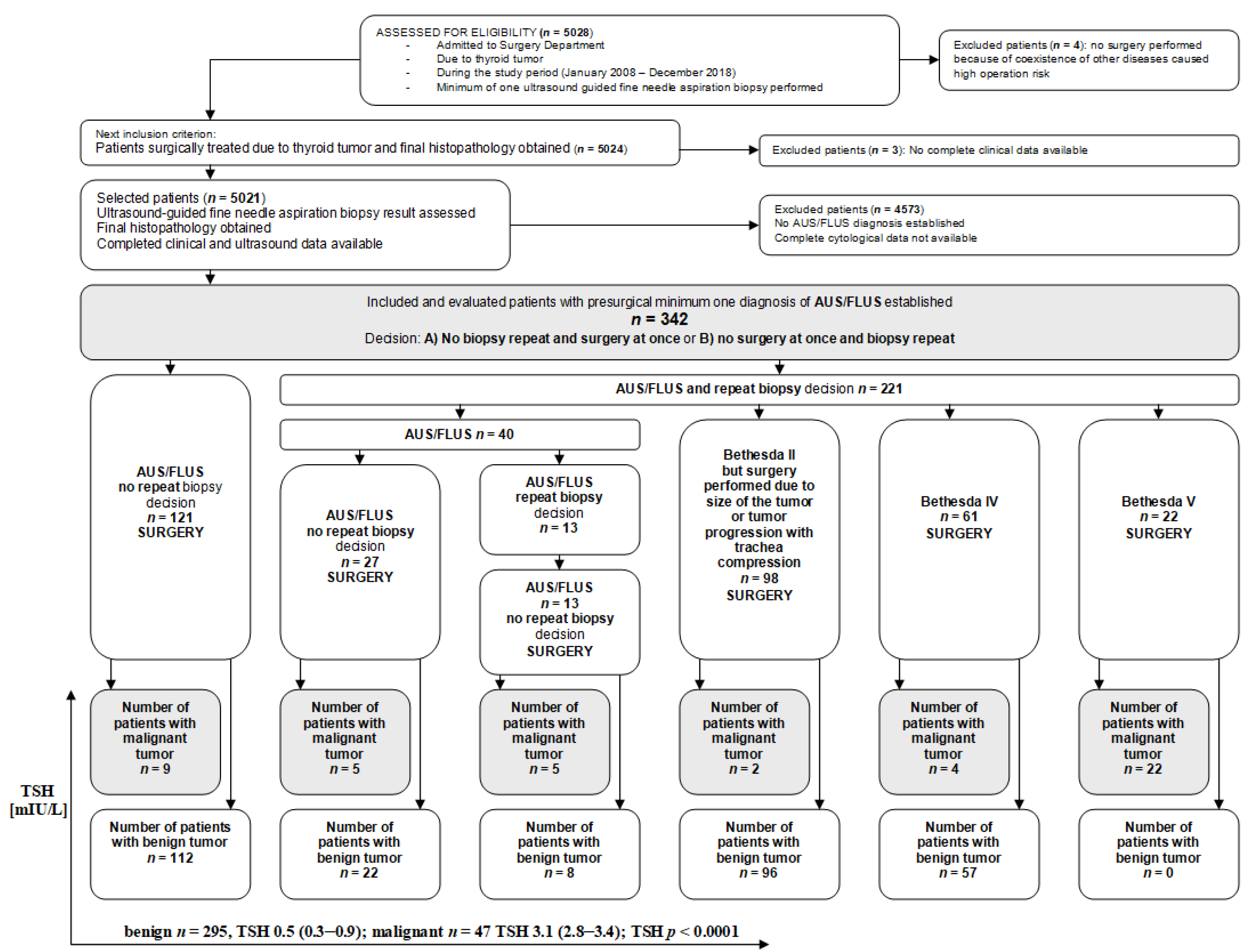
2.1. Study Population
2.2. Data Collection
2.3. Thyroid-Stimulating Hormone (TSH) Levels
2.4. The Bethesda System for Reporting Thyroid Cytopathology (TBSRT) 2nd Edition
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| TSH | thyroid-stimulating hormone |
| WDTC | well-differentiated thyroid cancer |
| AUS | atypia of undetermined significance |
| FLUS | follicular lesion of undetermined significance |
| ROM | risk of malignancy |
| TBSRTC | The Bethesda System for Reporting Thyroid Cytopathology |
| FDA | Food and Drug Administration |
| TC | thyroid cancer |
| UG-FNAB | ultrasound-guided fine-needle aspiration biopsy |
| NIFTP | noninvasive follicular neoplasms with papillary-like feature |
| SD | standard deviation |
| PTC | papillary thyroid cancer |
| FTC | follicular thyroid cancer |
References
- Huhtamella, R.; Kholová, I. Thyroid Bethesda category AUS/FLUS in our microscopes: Three-year-experience and cyto-histological correlation. Cancers 2019, 11, 1670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Dawish, M.; Robert, A.A.; Al Shehri, K.; Hawsawi, S.; Mujammami, M.; Al Basha, I.A.; Alrasheed, M.; Asiri, S.; Alzouman, M.; Alkharashi, E. Risk stratification of thyroid nodules with Bethesda III category: The experience of a territorial healthcare hospital. Cureus 2020, 12, e8202. [Google Scholar] [CrossRef] [PubMed]
- Guo, A.; Kaminoh, Y.; Forward, T.; Schwartz, F.L.; Jenkinson, S. Fine needle aspiration of thyroid nodules using the Bethesda system for reporting thyroid cytopathology: An institutional experience in a rural setting. Int. J. Endocrinol. 2017, 2017, 9601735. [Google Scholar] [CrossRef] [PubMed]
- Krane, F.J.; Nayar, R.; Renshaw, A.A. Atypia of undetermined siginificance/follicular lesions of undetermined siginificance. In The Bethesda System for Reporting Thyroid Cytopathology; Ali, S.Z., Cibas, E.S., Eds.; Springer: Cham, Switzerland, 2018; pp. 49–70. [Google Scholar]
- Almahari, S.A.; Harb, Z.; Alshaikh, S. Evaluation of thyroid nodules classified as Bethesda category III on cytology and their malignancy rate: An institutional experience. Cytojournal 2019, 16, 18. [Google Scholar] [CrossRef]
- Mosca, L.; Silva, L.; Carneiro, P.C.; Chacon, D.A.; Araujo-Neto, V.J.F.; Araujo-Filho, V.J.F.; Cernea, C.R. Malignancy rates for Bethesda III subcategories in thyroid fine needle aspiration biopsy (FNAB). Clinics 2018, 73, e370. [Google Scholar] [CrossRef]
- Cibas, E.S.; Ali, S.Z. The 2017 Bethesda system for reporting thyroid cytopathology. Thyroid 2017, 27, 1341–1346. [Google Scholar] [CrossRef]
- Cibas, E.S.; Ali, S.Z. The Bethesda system for reporting thyroid cytopathology. Am. J. Clin. Pathol. 2009, 132, 658–665. [Google Scholar] [CrossRef] [Green Version]
- Garg, S.; Naik, L.P.; Kothari, K.S.; Fernandes, G.C.; Agnihotri, M.A.; Gokhale, J.C. Evaluation of thyroid nodules classified as Bethesda category III on FNAC. J. Cytol. 2017, 34, 5–9. [Google Scholar] [CrossRef]
- Shrestha, R.T.; Evasovich, M.R.; Amin, K.; Radulescu, A.; Sanghvi, T.S.; Nelson, A.C.; Shahi, M.; Burmeister, L.A. Correlation between histological diagnosis and mutational panel testing of thyroid nodules: A two-year institutional experience. Thyroid 2016, 26, 1068–1076. [Google Scholar] [CrossRef] [Green Version]
- Krane, J.F.; Vanderlaan, P.A.; Faquin, W.C.; Renshaw, A.A. The atypia of undetermined significance/follicular lesion of undetermined significance: Malignant ratio: A proposed performance measure for reporting in the Bethesda System for thyroid cytopathology. Cancer Cytopathol. 2012, 120, 111–116. [Google Scholar] [CrossRef]
- Alshahrani, A.S.; Alamri, A.S.; Balkhoyor, A.H.; Mahzari, M.M.; Alshieban, S.S.; Majed, P.M. The prediction of malignancy risk in thyroid nodules classified as Bethesda system category III (AUS/FLUS) and the role of ultrasound finding for prediction of malignancy risk. Cureus 2021, 13, e17924. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Q.; Liu, J.; Zhu, J.; Hu, G. Association between preoperative serum thyroid-stimulating hormone level and nonfunctioning malignant nodule thyroid disease. Lin Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 2014, 28, 1931–1933. [Google Scholar] [PubMed]
- Zhou, Q.; Chen, J.; Feng, J.; Wang, J. Long noncoding RNA PVT1 modulates thyroid cancer cell proliferation by recruiting EZH2 and regulating thyroid-stimulating hormone receptor (TSHR). Tumour Biol. 2016, 37, 3105–3113. [Google Scholar] [CrossRef] [PubMed]
- Xiang, Y.; Xu, Y.; Bhandari, A.; Sindan, N.; Hirachan, S.; Yang, Q.; Guo, G.; Shen, Y. Serum TSH levels are associated with postoperative recurrence and lymph node metastasis of papillary thyroid carcinoma. Am. J. Transl. Res. 2021, 13, 6108–6116. [Google Scholar] [PubMed]
- Baser, H.; Topaloglu, O.; Tam, A.A.; Evranos, B.; Alkan, A.; Sungu, N.; Dumlu, E.G.; Ersoy, R.; Cakir, B. Higher TSH can be used as an additional risk factor in prediction of malignancy in euthyroid thyroid nodules evaluated by cytology based on Bethesda system. Endocrine 2016, 53, 520–529. [Google Scholar] [CrossRef]
- Oler, G.; Cerutti, J.M. High prevalence of BRAF mutation in a Brazilian cohort of patients with sporadic papillary thyroid carcinomas: Correlation with more aggressive phenotype and decreased expression of iodide-metabolizing genes. Cancer 2009, 115, 972–980. [Google Scholar] [CrossRef]
- Kaliszewski, K.; Diakowska, D.; Wojtczak, B.; Sutkowski, K.; Knychalski, B.; Forkasiewicz, Z. Patients with III and IV category of the Bethesda System under levothyroxine non-suppressive therapy have a lower rate of thyroid malignancy. Sci. Rep. 2019, 9, 8409. [Google Scholar] [CrossRef] [Green Version]
- Kuru, B.; Kefeli, M. Risk factors associated with malignancy and with triage to surgery in thyroid nodules classified as Bethesda category IV (FN/SFN). Diagn. Cytopathol. 2018, 46, 489–494. [Google Scholar] [CrossRef]
- Fiore, E.; Rago, T.; Provenzale, M.A.; Scutari, M.; Ugolini, C.; Basolo, F.; Di Coscio, G.; Berti, P.; Grasso, L.; Elisei, R.; et al. Lower levels of TSH are associated with a lower risk of papillary thyroid cancer in patients with thyroid nodular disease: Thyroid autonomy may play a protective role. Endocr. Relat. Cancer 2009, 16, 1251–1260. [Google Scholar] [CrossRef] [Green Version]
- Kaliszewski, K.; Diakowska, D.; Rzeszutko, M.; Nowak, Ł.; Tokarczyk, U.; Rudnicki, J. Atypia and Follicular Lesions of Undetermined Significance in Subsequent Biopsy Result: What Clinicians Need to Know. J. Clin. Med. 2021, 10, 3082. [Google Scholar] [CrossRef]
- Grob, F.; Deladoëy, J.; Legault, L.; Spigelblatt, L.; Fournier, A.; Vassart, G.; Van Vliet, G. Autonomous adenomas caused by somatic mutations of the thyroid-stimulating hormone receptor in children. Horm. Res. Paediatr. 2014, 81, 73–79. [Google Scholar] [CrossRef] [PubMed]
- He, H.; Li, W.; Liyanarachchi, S.; Jendrzejewski, J.; Srinivas, M.; Davuluri, R.V.; Nagy, R.; de la Chapelle, A. Genetic predisposition to papillary thyroid carcinoma: Involvement of FOXE1, TSHR, and a novel lincRNA gene, PTCSC2. J. Clin. Endocrinol. Metab. 2015, 100, E164–E172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, D.S.; Doherty, G.M.; Haugen, B.R.; Kloos, R.T.; Lee, S.L.; Mandel, S.J.; Mazzaferri, E.L.; McIver, B.; Pacini, F.; Schlumberger, M.; et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 2009, 19, 1167–1214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Agostino, M.; Sponziello, M.; Puppin, C.; Celano, M.; Maggisano, V.; Baldan, F.; Biffoni, M.; Bulotta, S.; Durante, C.; Filetti, S.; et al. Different expression of TSH receptor and NIS genes in thyroid cancer: Role of epigenetics. J. Mol. Endocrinol. 2014, 52, 121–131. [Google Scholar] [CrossRef] [Green Version]
- Gudmundsson, J.; Sulem, P.; Gudbjartsson, D.F.; Jonasson, J.G.; Sigurdsson, A.; Bergthorsson, J.T.; He, H.; Blondal, T.; Geller, F.; Jakobsdottir, M.; et al. Common variants on 9q22.33 and 14q13.3 predispose to thyroid cancer in European populations. Nat. Genet. 2009, 41, 460–464. [Google Scholar] [CrossRef]
- Gudmundsson, J.; Sulem, P.; Gudbjartsson, D.F.; Jonasson, J.G.; Masson, G.; He, H.; Jonasdottir, A.; Sigurdsson, A.; Stacey, S.N.; Johannsdottir, H.; et al. Discovery of common variants associated with low TSH levels and thyroid cancer risk. Nat. Genet. 2012, 44, 319–322. [Google Scholar] [CrossRef]
- Rahbari, R.; Zhang, L.; Kebebew, E. Thyroid cancer gender disparity. Future Oncol. 2010, 6, 1771–1779. [Google Scholar] [CrossRef] [Green Version]
- Kaliszewski, K.; Diakowska, D.; Wojtczak, B.; Forkasiewicz, Z. Evaluation of selected ultrasound features of thyroid nodules with atypia of undetermined significance/follicular lesion of undetermined significance for the Bethesda reporting system for thyroid cytology. Cancer Manag. Res. 2018, 10, 2223–2229. [Google Scholar] [CrossRef] [Green Version]
- Boelaert, K.; Horacek, J.; Holder, R.L.; Watkinson, J.C.; Sheppard, M.C.; Franklyn, J.A. Serum thyrotropin concentration as a novel predictor of malignancy in thyroid nodules investigated by fine-needle aspiration. J. Clin. Endocrinol. Metab. 2006, 91, 4295–4301. [Google Scholar] [CrossRef]
- Fiore, E.; Rago, T.; Provenzale, M.A.; Scutari, M.; Ugolini, C.; Basolo, F.; Di Coscio, G.; Miccoli, P.; Grasso, L.; Pinchera, A.; et al. L-thyroxine-treated patients with nodular goiter have lower serum TSH and lower frequency of papillary thyroid cancer: Results of a cross-sectional study on 27,914 patients. Endocr. Relat. Cancer 2010, 17, 231–239. [Google Scholar] [CrossRef] [Green Version]
- Haymart, M.R.; Repplinger, D.J.; Leverson, G.E.; Elson, D.F.; Sippel, R.S.; Jaume, J.C.; Chen, H. Higher serum thyroid stimulating hormone level in thyroid nodule patients is associated with greater risks of differentiated thyroid cancer and advanced tumor stage. J. Clin. Endocrinol. Metab. 2008, 93, 809–814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Dawish, M.A.; Alwin Robert, A.; Thabet, M.A.; Braham, R. Thyroid nodule management: Thyroid-stimulating hormone, ultrasound, and cytological classification system for predicting malignancy. Cancer Inform. 2018, 17, 1176935118765132. [Google Scholar] [CrossRef] [Green Version]
- Zafon, C.; Obiols, G.; Baena, J.A.; Castellví, J.; Dalama, B.; Mesa, J. Preoperative thyrotropin serum concentrations gradually increase from benign thyroid nodules to papillary thyroid microcarcinomas then to papillary thyroid cancers of larger size. J. Thyroid Res. 2012, 2012, 530721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, I.K.; Kim, J.H.; Cho, Y.U.; Park, S.Y.; Kim, S.J. Clinicopathological factors increased the risk of malignancy in thyroid nodules with atypical or follicular lesions of undetermined significance (AUS/FLUS) risk factor of malignancy in thyroid nodule with AUS/FLUS. Ann. Surg. Treat. Res. 2016, 90, 201–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castro, M.R.; Espiritu, R.P.; Bahn, R.S.; Henry, M.R.; Gharib, H.; Caraballo, P.J.; Morris, J.C. Predictors of malignancy in patients with cytologically suspicious thyroid nodules. Thyroid 2011, 21, 1191–1198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaya, C.; Bozkurt, E.; Türkyılmaz Mut, D.; Mihmanli, M.; Uludağ, M. Which factors are associated with malignancy in thyroid nodules classified as bethesda category 3 (AUS/FLUS) and how do they influence the patient’s management? Acta Endocrinol. 2019, 15, 491–496. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameters | Total Group (n = 47) | |
|---|---|---|
| Sex | Female | 32 (68.1) |
| Male | 15 (31.9) | |
| Age (years) | 48.8 ± 15.4 | |
| Age (years old) | <55 years old | 37 (78.7) |
| ≥55 years old | 10 (21.3) | |
| Presurgical diagnosis | AUS | 26 (12.1) |
| FLUS | 21 (87.9 | |
| Histopathological diagnosis | PTC | 46 (97.9) |
| FTC | 1 (2.1) | |
| Nodule size (cm) | ≤1.0 cm | 2 (4.2) |
| >1.0 ≤ 2.0 cm | 9 (19.2) | |
| >2.0 ≤ 4.0 cm | 15 (31.9) | |
| >4.0 cm | 21 (44.7) | |
| pTNM: | I | 11 (23.4) |
| II | 36 (76.6) | |
| III | - | |
| IV | - | |
| Parameters | Total Group (n = 342) | Benign (n = 295) | Cancer (n = 47) | p Value | |
|---|---|---|---|---|---|
| Sex | Female Male | 284 (83.0) 58 (17.0) | 252 (85.4) 43 (14.6) | 32 (68.1) 15 (31.9) | 0.003 * |
| Age (years old) | 51.3 ± 15.4 | 52.1 ± 15.5 | 46.0 ± 14.0 | 0.011 * | |
| Age | <55 years old ≥55 years old | 191 (55.9) 151 (44.2) | 154 (52.2) 141 (47.8) | 37 (78.7) 10 (21.3) | 0.0007 * |
| Microcalcifications | Yes No | 72 (21.1) 270 (78.9) | 37 (12.5) 258 (87.5) | 35 (74.5) 12 (25.5) | <0.0001 * |
| Echogenicity | Hypoechoic Hyperechoic | 125 (36.6) 217 (63.4) | 82 (27.8) 213 (72.2) | 43 (91.5) 4 (8.5) | <0.0001 * |
| Irregular margin | Yes No | 132 (38.6) 210 (61.4) | 88 (29.8) 207 (70.2) | 44 (93.6) 3 (6.4) | <0.0001 * |
| Taller than wide | Yes No | 111 (32.5) 231 (67.5) | 69 (23.4) 226 (76.6) | 42 (89.4) 5 (10.6) | <0.0001 * |
| High vascularity | Yes No | 118 (34.5) 224 (65.5) | 88 (29.8) 207 (70.2) | 30 (63.8) 17 (36.2) | <0.0001 * |
| Macrocalcifications | Yes No | 158 (46.2) 184 (53.8) | 142 (48.1) 153 (51.9) | 16 (34.0) 31 (66.0) | 0.072 |
| TSH (mIU/L) | 0.6 (0.4–1.5) | 0.5 (0.3–0.9) | 3.1 (2.8–3.4) | <0.0001 * | |
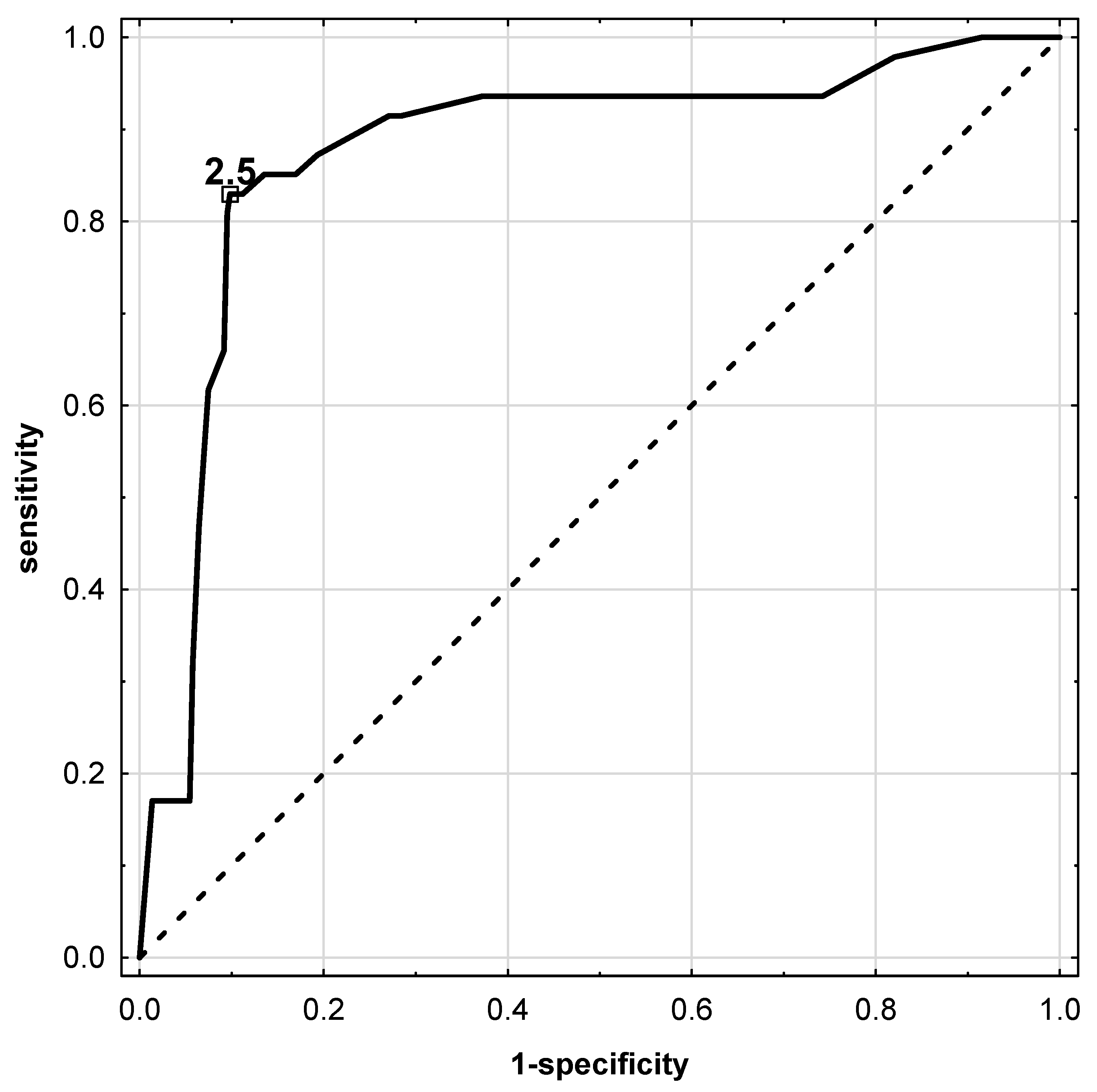
| AUC (±95% CI) | 0.877 (0.818–0.935) |
|---|---|
| p value | <0.0001 * |
| sensitivity | 0.830 |
| specificity | 0.902 |
| accuracy | 0.892 |
| PPV | 0.574 |
| NPV | 0.971 |
| Youden index | 0.731 |
| Independent Variables | Univariable Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| OR (±95% CI) | p-Value | OR (±95% CI) | p-Value | |
| Sex: for female | 0.36 (0.18–0.73) | <0.004 * | 2.36 (0.08–67.95) | 0.615 |
| Age: for <55 years old | 3.38 (1.62–7.08) | 0.001 * | 108.9 (0.99–1189.62) | 0.049 * |
| Microcalcifications | 20.33 (9.67–42.76) | <0.0001 * | 164.92 (2.62–1034.68) | 0.015 * |
| Hypoechoic | 27.92 (9.67–80.56) | <0.0001 * | 250.97 (1.50–4186.21) | 0.034 * |
| Irregular margin | 34.49 (10.38–114.56) | <0.0001 * | 12.69 (0.92–173.56) | 0.056 |
| Taller than wide | 27.51 (10.43–72.51) | <0.0001 * | 921.44 (2.36–3587.85) | 0.024 * |
| High vascularity | 4.15 (2.17–7.93) | <0.0001 * | 19.46 (0.43–872.59) | 0.124 |
| TSH for ≥2.5mUI/L | 40.26 (17.60–92.08) | <0.0001 * | 168.69 (4.56–6237.33) | 0.005 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaliszewski, K.; Diakowska, D.; Rzeszutko, M.; Nowak, Ł.; Wojtczak, B.; Sutkowski, K.; Ludwig, M.; Ludwig, B.; Mikuła, A.; Greniuk, M.; et al. Assessment of Preoperative TSH Serum Level and Thyroid Cancer Occurrence in Patients with AUS/FLUS Thyroid Nodule Diagnosis. Biomedicines 2022, 10, 1916. https://doi.org/10.3390/biomedicines10081916
Kaliszewski K, Diakowska D, Rzeszutko M, Nowak Ł, Wojtczak B, Sutkowski K, Ludwig M, Ludwig B, Mikuła A, Greniuk M, et al. Assessment of Preoperative TSH Serum Level and Thyroid Cancer Occurrence in Patients with AUS/FLUS Thyroid Nodule Diagnosis. Biomedicines. 2022; 10(8):1916. https://doi.org/10.3390/biomedicines10081916
Chicago/Turabian StyleKaliszewski, Krzysztof, Dorota Diakowska, Marta Rzeszutko, Łukasz Nowak, Beata Wojtczak, Krzysztof Sutkowski, Maksymilian Ludwig, Bartłomiej Ludwig, Agnieszka Mikuła, Maria Greniuk, and et al. 2022. "Assessment of Preoperative TSH Serum Level and Thyroid Cancer Occurrence in Patients with AUS/FLUS Thyroid Nodule Diagnosis" Biomedicines 10, no. 8: 1916. https://doi.org/10.3390/biomedicines10081916