
Anabolic Effects of a Novel Simvastatin Derivative on Treating Rat Bone Defects

 , ,
, ,  , and
, and 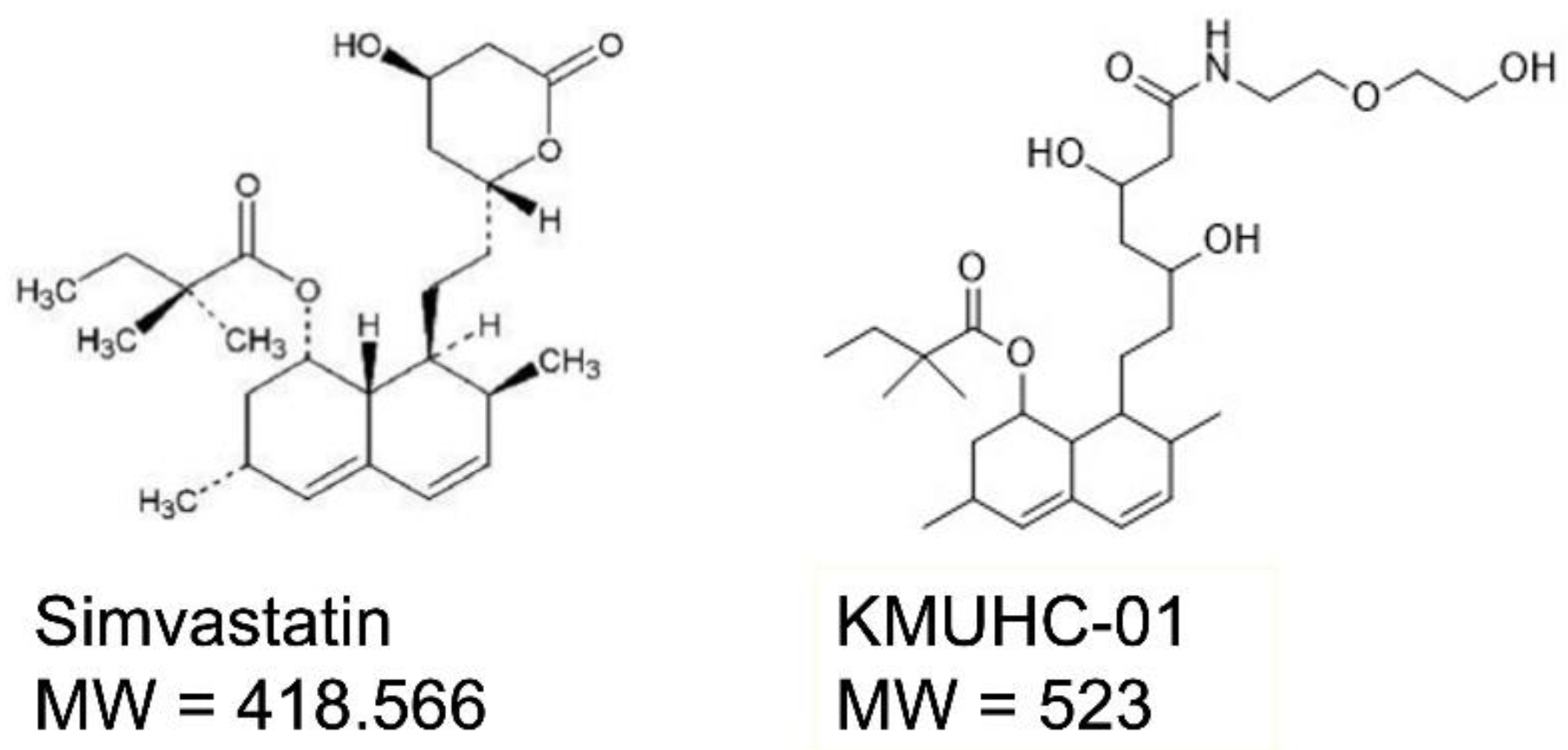{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cell Culture
2.2. Cell Viability
2.3. Bioactivity of Mineralization
2.4. Ribonucleic Acid (RNA) Extraction and Real-Time Polymerase Chain Reaction (PCR)
2.5. Animals
2.6. Critical-Sized Calvarial Defects in Rats
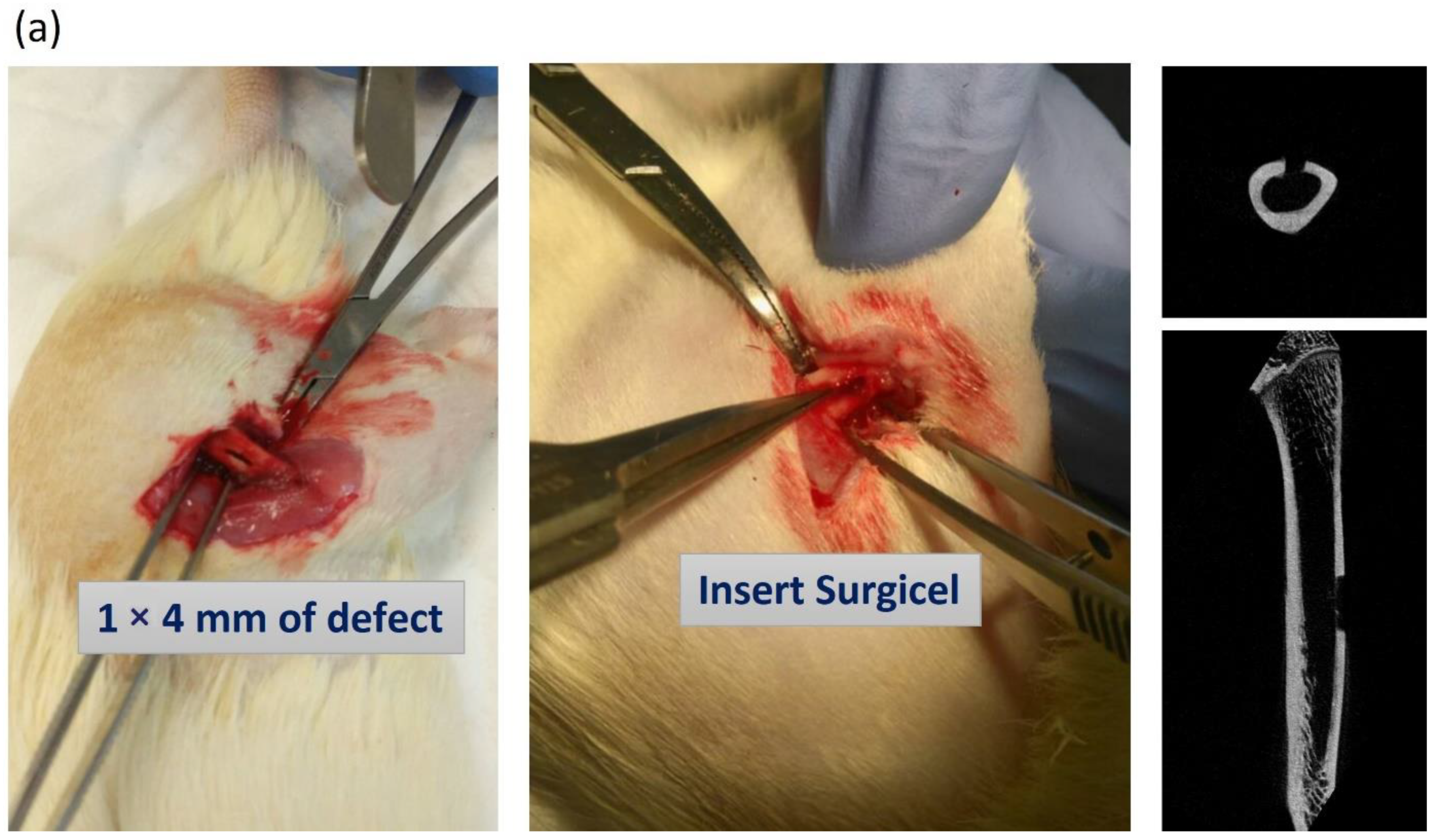
2.7. Femur Bone Defects in Rats
2.8. Micro-CT Analysis
2.9. Histological Analysis and Immunostaining of Bone Tissue
2.10. Mechanical Analysis of Femur Bone with Three-Point Bending Test
2.11. Statistical Analysis
3. Results
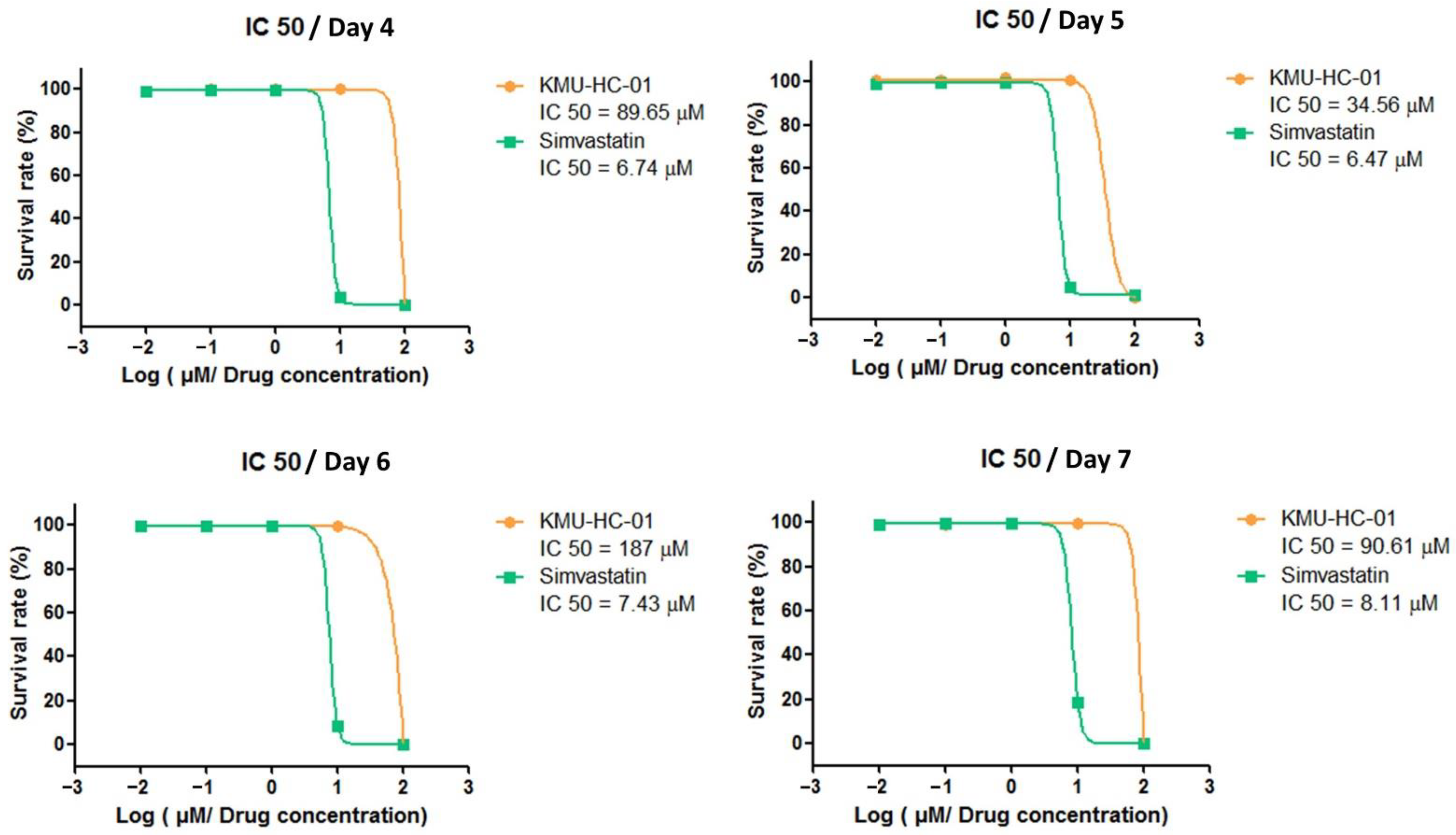
3.1. KMUHC-01 Is Less Cytotoxic Than Simvastatin
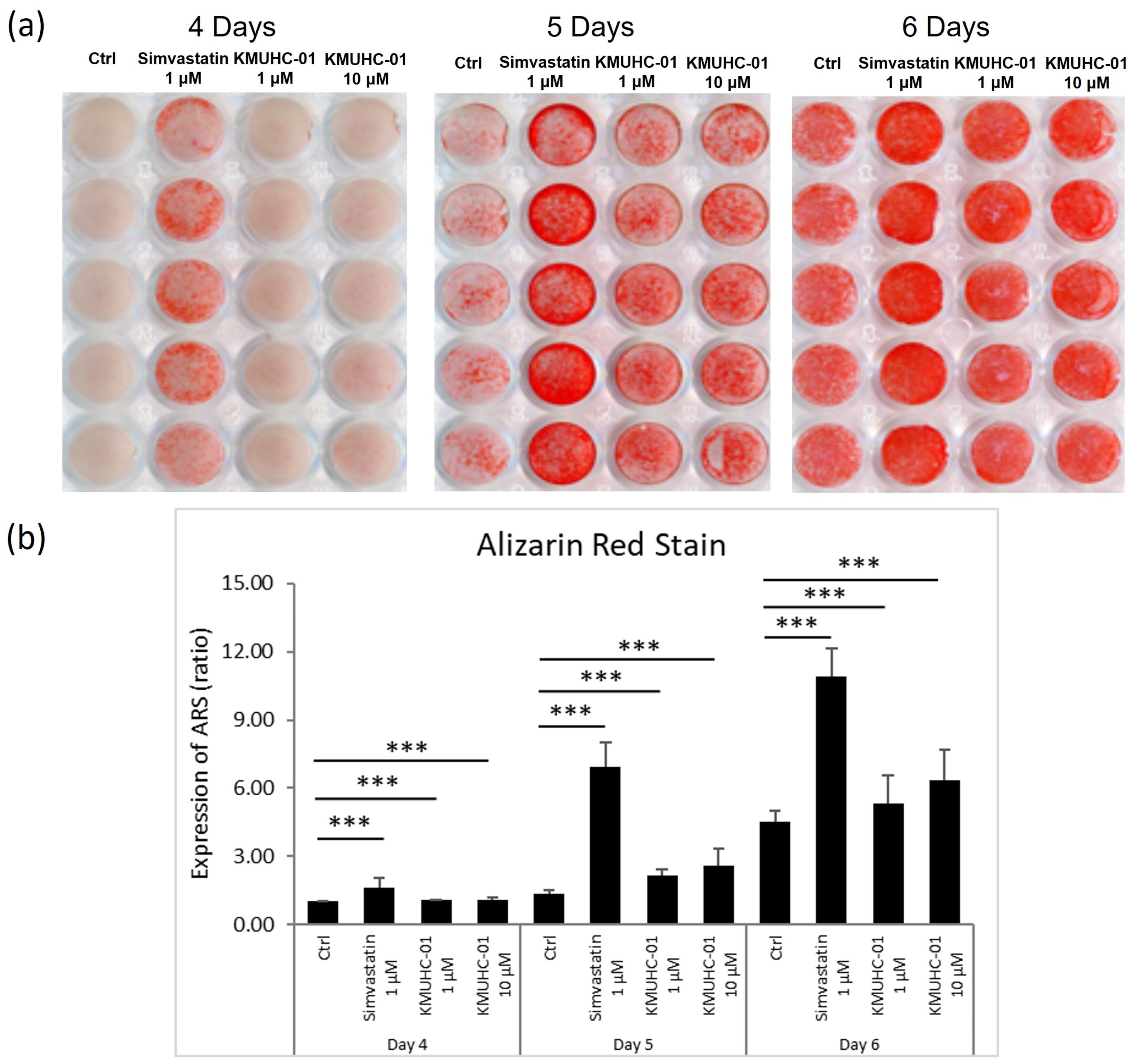
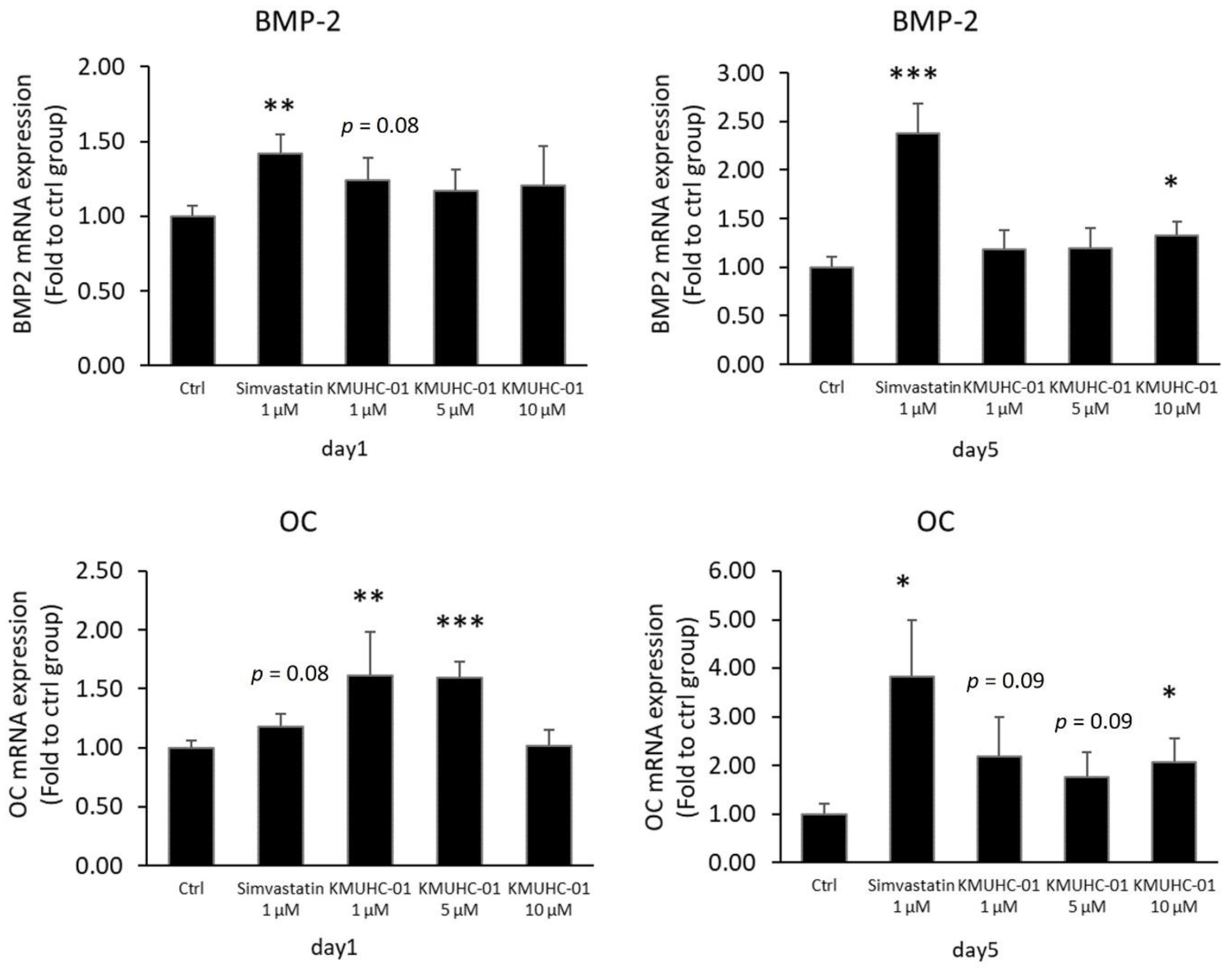
3.2. Both KMUHC-01 and Simvastatin Enhanced D1 Cell Mineralization and BMP-2 Expression
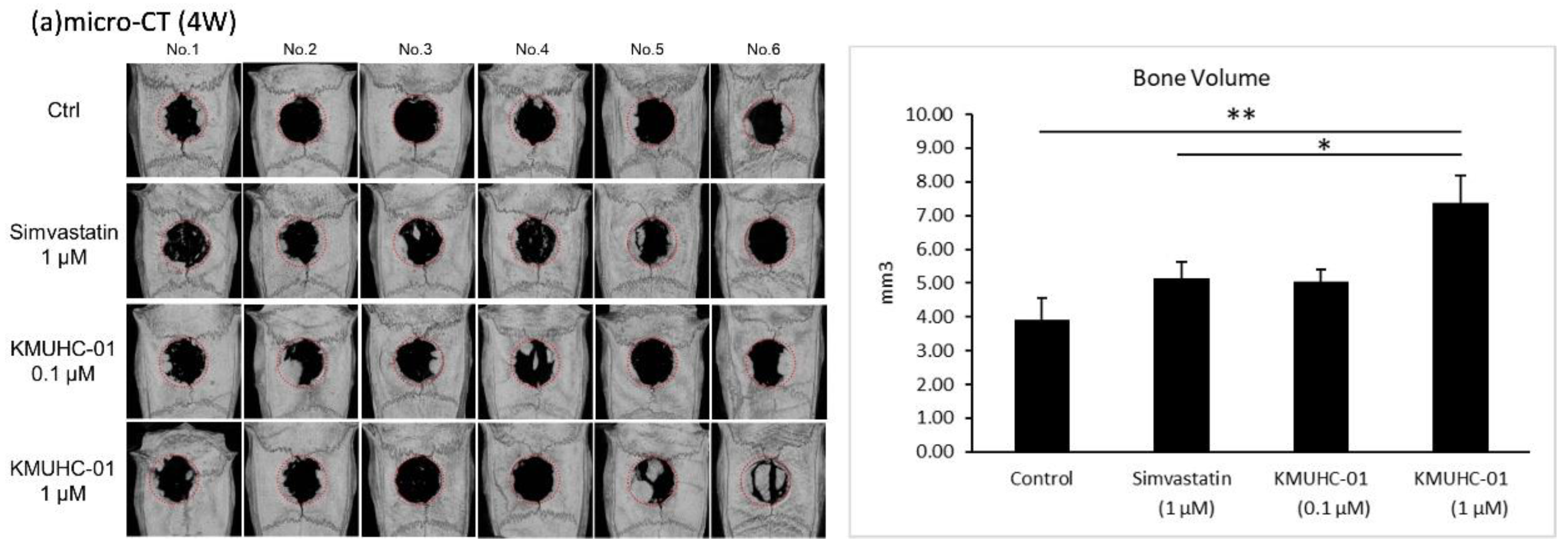
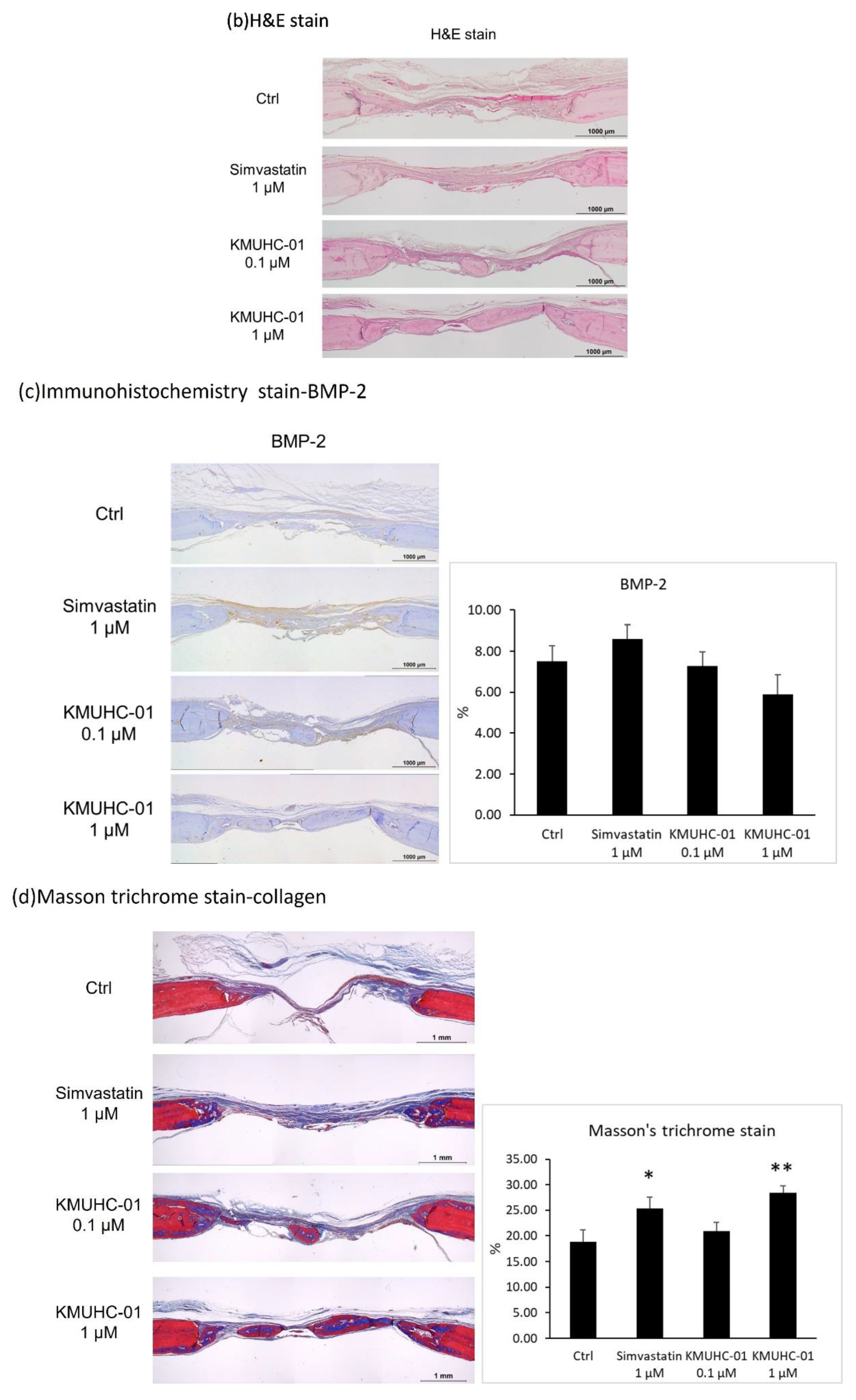
3.3. KMUHC-01 and Simvastatin Treatments Enhance Bone Formation Evidenced by Micro-CT Analysis, H&E, and Masson’s Trichrome Staining of Critical-Sized Calvarial Defects
3.4. Immunohistochemistry Staining of BMP-2 Critical-Sized Calvarial Defects
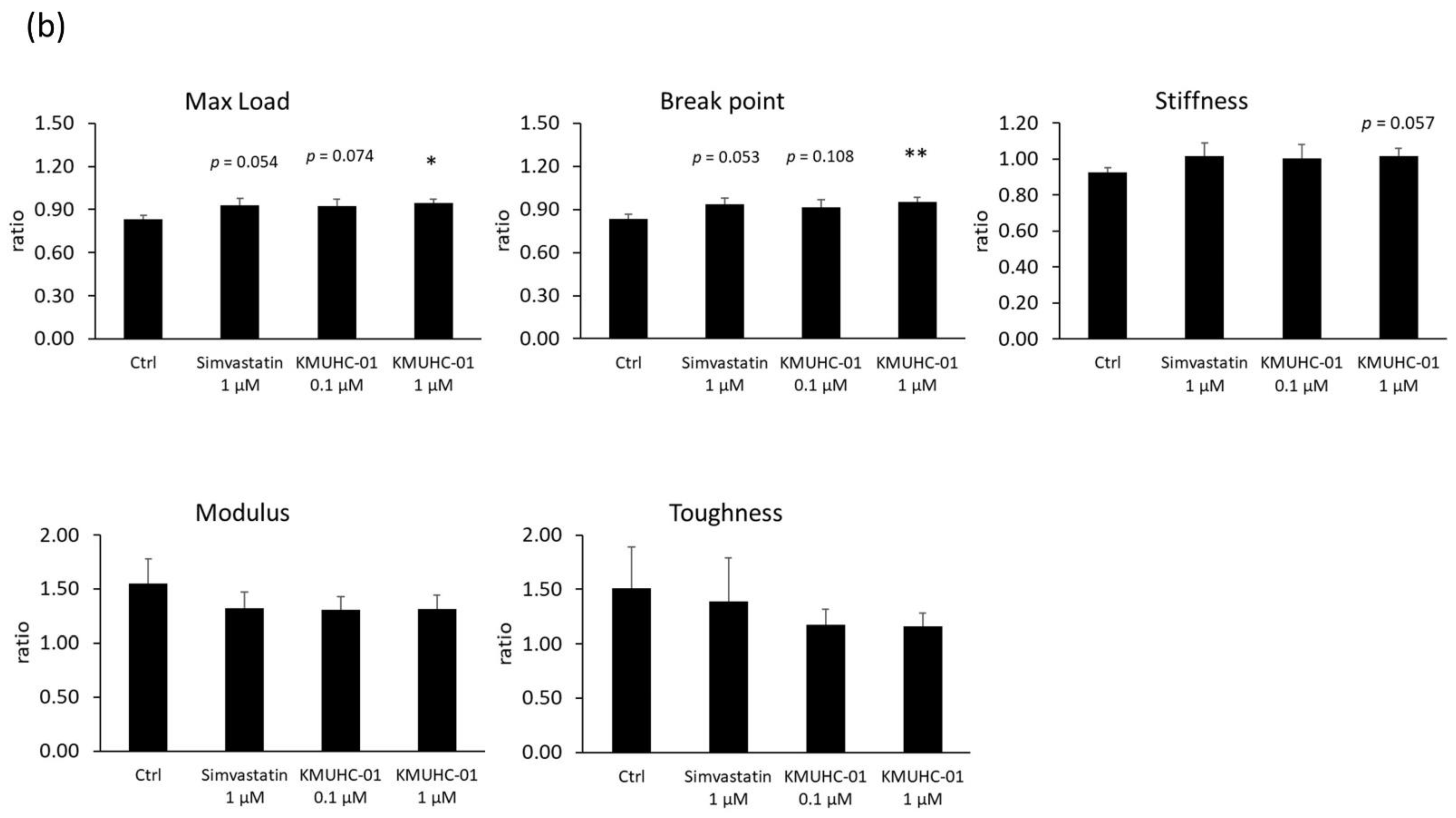
3.5. KMUHC-01 Could Help Recover the Mechanical Properties of Femur Bone Defect
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Oryan, A.; Alidadi, S.; Moshiri, A.; Maffulli, N. Bone medicine: Classic options, novel strategies, and future directions. J. Orthop. Surg. Res. 2014, 9, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oryan, A.; Monazzah, S.; Bigham-Sadegh, A. Bone injury and fracture healing biology. Biomed. Environ. Sci. 2015, 28, 57–71. [Google Scholar] [CrossRef] [PubMed]
- Bigham-Sadegh, A.; Oryan, A. Basic concepts regarding fracture healing and the current options and future directions in managing bone fractures. Int. Wound J. 2015, 12, 238–247. [Google Scholar] [CrossRef] [PubMed]
- Hak, D.J.; Fitzpatrick, D.; Bishop, J.A.; Marsh, J.L.; Tilp, S.; Schnettler, R.; Simpson, H.; Alt, V. Delayed union and nonunions: Epidemiology, clinical issues, and financial aspects. Injury 2014, 45 (Suppl. 2), S3–S7. [Google Scholar] [CrossRef]
- Moshiri, A.; Shahrezaee, M.; Shekarchi, B.; Oryan, A.; Azma, K. Three-dimensional porous Gelapin-Simvastatin scaffolds promoted bone defect healing in rabbits. Calcif. Tissue Int. 2015, 96, 552–564. [Google Scholar] [CrossRef]
- García-Gareta, E.; Coathup, M.J.; Blunn, G.W. Osteoinduction of bone grafting materials for bone repair and regeneration. Bone 2015, 81, 112–121. [Google Scholar] [CrossRef]
- Heart Protection Study Collaborative Group. Effects on 11-year mortality and morbidity of lowering LDL cholesterol with simvastatin for about 5 years in 20,536 high-risk individuals: A randomised controlled trial. Lancet 2011, 378, 2013–2020. [Google Scholar] [CrossRef] [Green Version]
- Macedo, A.F.; Taylor, F.C.; Casas, J.P.; Adler, A.; Prieto-Merino, D.; Etbrahim, S. Unintended effects of statins from observational studies in the general population: Systematic review and meta-analysis. BMC Med. 2014, 12, 51. [Google Scholar] [CrossRef] [Green Version]
- Nakashima, Y.; Haneji, T. Stimulation of osteoclast formation by RANKL requires interferon regulatory factor-4 and is inhibited by simvastatin in a mouse model of bone loss. PLoS ONE 2013, 8, e72033. [Google Scholar] [CrossRef]
- Moon, H.-J.; Kim, S.E.; Yun, Y.P.; Hwalng, Y.-S.; Bang, J.B.; Park, J.-H.; Kwon, I.K. Simvastatin inhibits osteoclast differentiation by scavenging reactive oxygen species. Exp. Mol. Med. 2011, 43, 605–612. [Google Scholar] [CrossRef]
- Hughes, A.; Rogers, M.J.; Idris, A.I.; Crockett, J.C. A comparison between the effects of hydrophobic and hydrophilic statins on osteoclast function in vitro and ovariectomy-induced bone loss in vivo. Calcif. Tissue Int. 2007, 81, 403–413. [Google Scholar] [CrossRef]
- Chuang, S.-C.; Liao, H.-J.; Li, C.-J.; Wang, G.-J.; Chang, J.-K.; Ho, M.-L. Simvastatin enhances human osteoblast proliferation involved in mitochondrial energy generation. Eur. J. Pharmacol. 2013, 714, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Ho, M.-L.; Chen, Y.-H.; Liao, H.-J.; Chen, C.-H.; Hung, S.-H.; Lee, M.-J.; Fu, Y.-C.; Wang, Y.-H.; Wang, G.-J.; Chang, J.-K. Simvastatin increases osteoblasts and osteogenic proteins in ovariectomized rats. Eur. J. Clin. Investig. 2009, 39, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Ho, M.-L.; Tai, I.-C.; Fu, Y.-C.; Wang, C.-K.; Chang, J.-K. Local delivery of controlled-release simvastatin/PLGA/HAp microspheres enhances bone repair. Int. J. Nanomed. 2013, 8, 3895–3904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukui, T.; Ii, M.; Shoji, T.; Matsumoto, T.; Mifune, Y.; Kawakami, Y.; Akimaru, H.; Kawamoto, A.; Kuroda, T.; Saito, T.; et al. Therapeutic effect of local administration of low-dose simvastatin-conjugated gelatin hydrogel for fracture healing. J. Bone Miner. Res. 2012, 27, 1118–1131. [Google Scholar] [CrossRef] [PubMed]
- Oka, S.; Matsumoto, T.; Kubo, S.; Matsushita, T.; Sasaki, H.; Nishizawa, Y.; Matsuzaki, T.; Saito, T.; Nishida, K.; Tabata, Y.; et al. Local administration of low-dose simvastatin-conjugated gelatin hydrogel for tendon-bone healing in anterior cruciate ligament reconstruction. Tissue Eng. Part A 2013, 19, 1233–1243. [Google Scholar] [CrossRef] [Green Version]
- Fuentes, I.; Aguilera, C. Myopathy secondary to the treatment with inhibitors of HMG-CoA reductase. Med. Clin. 1998, 111, 700. [Google Scholar]
- Duell, P.B.; Connor, W.E.; Illingworth, D.R. Rhabdomyolysis after taking atorvastatin with gemfibrozil. Am. J. Cardiol. 1998, 81, 368–369. [Google Scholar] [CrossRef]
- Jacobson, R.H.; Wang, P.; Glueck, C.J. Myositis and rhabdomyolysis associated with concurrent use of simvastatin and nefazodone. JAMA 1997, 277, 296–297. [Google Scholar] [CrossRef]
- Hsieh, K.-C.; Kao, C.-L.; Feng, C.-W.; Wen, Z.-H.; Chang, H.-F.; Chuang, S.-C.; Wang, G.-J.; Ho, M.-L.; Wu, S.-M.; Chang, J.-K.; et al. A novel anabolic agent: A simvastatin analogue without HMG-CoA reductase inhibitory activity. Org. Lett. 2014, 16, 4376–4379. [Google Scholar] [CrossRef]
- Wang, Y.-H.; Rajalakshmanan, E.; Wang, C.-K.; Chen, C.-H.; Fu, Y.-C.; Tsai, T.-L.; Chang, J.-K.; Ho, M.-L. PLGA-linked alendronate enhances bone repair in diaphysis defect model. J. Tissue Eng. Regen. Med. 2017, 11, 2603–2612. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-Z.; Chen, S.-M.; Chen, C.-H.; Wang, C.-K.; Wang, G.-J.; Chang, J.-K.; Ho, M.-L. The effect of the local delivery of alendronate on human adipose-derived stem cell-based bone regeneration. Biomaterials 2010, 31, 8674–8683. [Google Scholar] [CrossRef] [PubMed]
- Mundy, G.; Garrett, R.; Halrris, S.; Chan, J.; Chen, D.; Rossini, G.; Boyce, B.; Zhao, M.; Gutierrez, G. Stimulation of bone formation in vitro and in rodents by statins. Science 1999, 286, 1946–1949. [Google Scholar] [CrossRef] [PubMed]
- Staal, A.; Frith, J.C.; French, M.H.; Swartz, J.; Güngör, T.; Halrrity, T.W.; Tamasi, J.; Rogers, M.J.; Feyen, J.H. The ability of statins to inhibit bone resorption is directly related to their inhibitory effect on HMG-CoA reductase activity. J. Bone Miner. Res. 2003, 18, 88–96. [Google Scholar] [CrossRef]
- Maeda, T.; Matsunuma, A.; Kurahashi, I.; Yanagawa, T.; Yoshida, H.; Horiuchi, N. Induction of osteoblast differentiation indices by statins in MC3T3-E1 cells. J. Cell. Biochem. 2004, 92, 458–471. [Google Scholar] [CrossRef]
- Weivoda, M.M.; Hohl, R.J. Effects of farnesyl pyrophosphate accumulation on calvarial osteoblast differentiation. Endocrinology 2011, 152, 3113–3122. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Song, Q.-S.; Wang, J.-Y.; Leng, H.-J.; Chen, Z.-Q.; Liu, Z.-J.; Dang, G.-T.; Song, C.-L. Simvastatin induces estrogen receptor-alpha expression in bone, restores bone loss, and decreases ERα expression and uterine wet weight in ovariectomized rats. J. Bone Miner. Metab. 2011, 29, 396–403. [Google Scholar] [CrossRef]
- Chuang, S.-C.; Chen, C.-H.; Fu, Y.-C.; Tai, I.-C.; Li, C.-J.; Chang, L.-F.; Ho, M.-L.; Chang, J.-K. Estrogen receptor mediates simvastatin-stimulated osteogenic effects in bone marrow mesenchymal stem cells. Biochem. Pharmacol. 2015, 98, 453–464. [Google Scholar] [CrossRef]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, T.-C.; Chen, H.-T.; Tai, I.-C.; Kao, L.-T.; Hung, M.-H.; Chen, C.-H.; Fu, Y.-C.; Wang, Y.-H.; Kao, C.-M.; Chang, J.-K.; et al. Anabolic Effects of a Novel Simvastatin Derivative on Treating Rat Bone Defects. Biomedicines 2022, 10, 1915. https://doi.org/10.3390/biomedicines10081915
Lee T-C, Chen H-T, Tai I-C, Kao L-T, Hung M-H, Chen C-H, Fu Y-C, Wang Y-H, Kao C-M, Chang J-K, et al. Anabolic Effects of a Novel Simvastatin Derivative on Treating Rat Bone Defects. Biomedicines. 2022; 10(8):1915. https://doi.org/10.3390/biomedicines10081915
Chicago/Turabian StyleLee, Tien-Ching, Hui-Ting Chen, I-Chun Tai, Li-Ting Kao, Ming-Hsin Hung, Chung-Hwan Chen, Yin-Chih Fu, Yan-Hsiung Wang, Chih-Ming Kao, Je-Ken Chang, and et al. 2022. "Anabolic Effects of a Novel Simvastatin Derivative on Treating Rat Bone Defects" Biomedicines 10, no. 8: 1915. https://doi.org/10.3390/biomedicines10081915