
Immediate Effects of Extracorporeal Shock Wave Therapy in Fascial Fibroblasts: An In Vitro Study

 , , ,
, , ,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cell Isolation and Culture
2.2. Cell Treatment with ESW
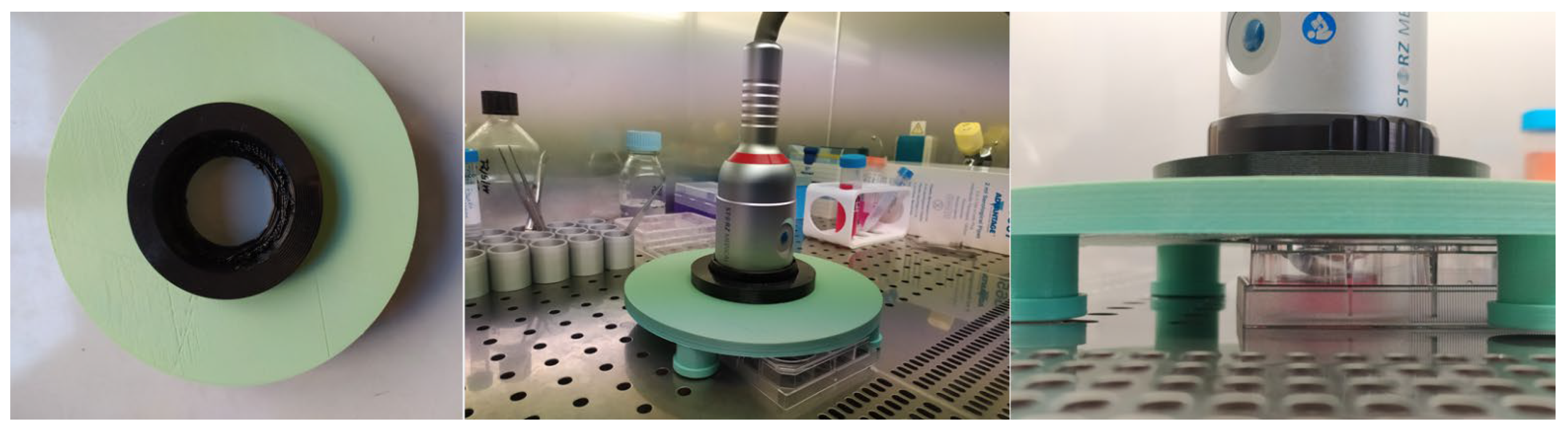
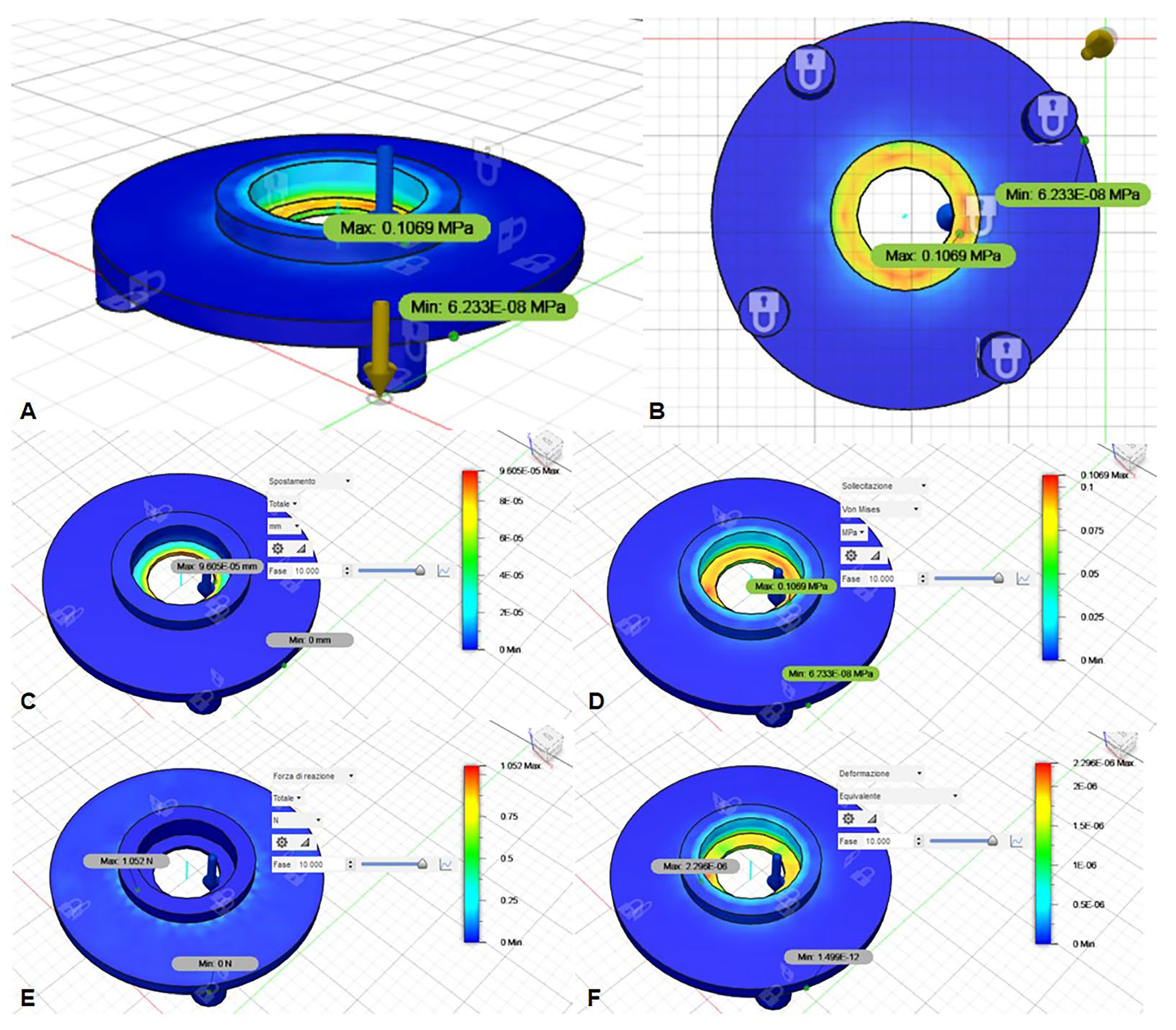
2.3. ESW Cylindrical Coil Source Support Design and Fabrication
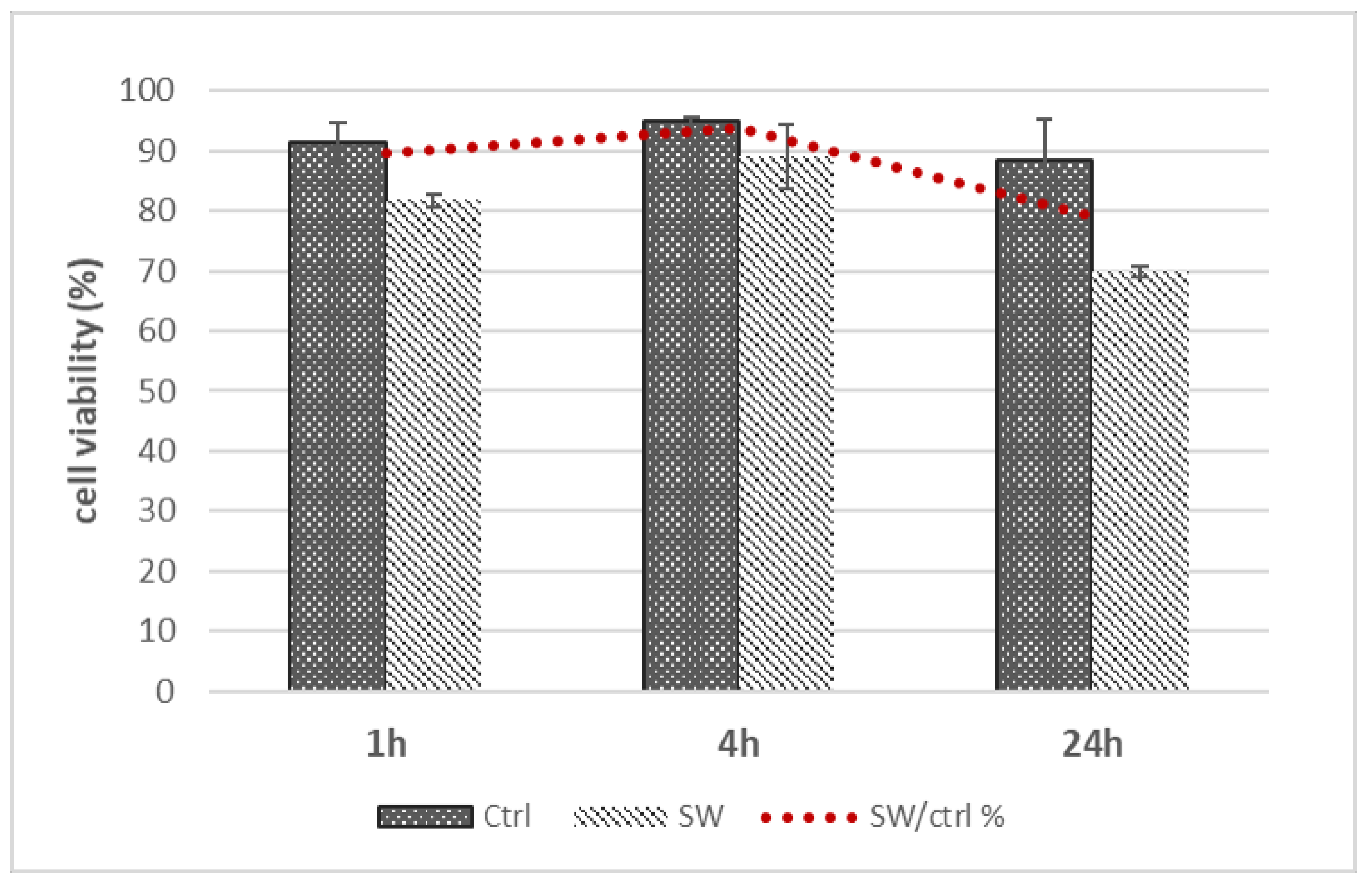
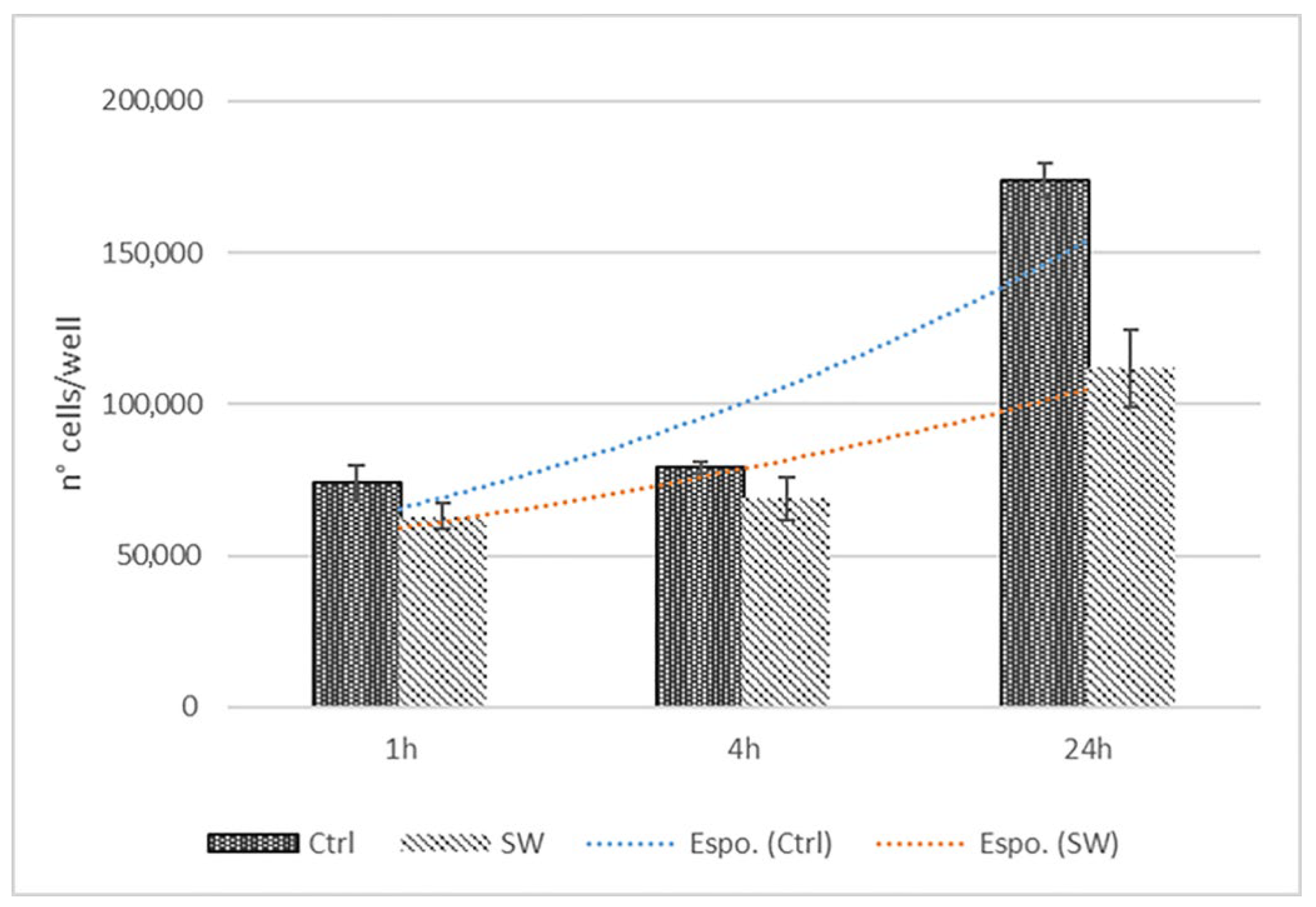
2.4. Dose–Response and Time-Course Analysis
2.5. Statistical Analysis
2.6. Preparation of Samples for Stainings
2.7. Staining Protocols
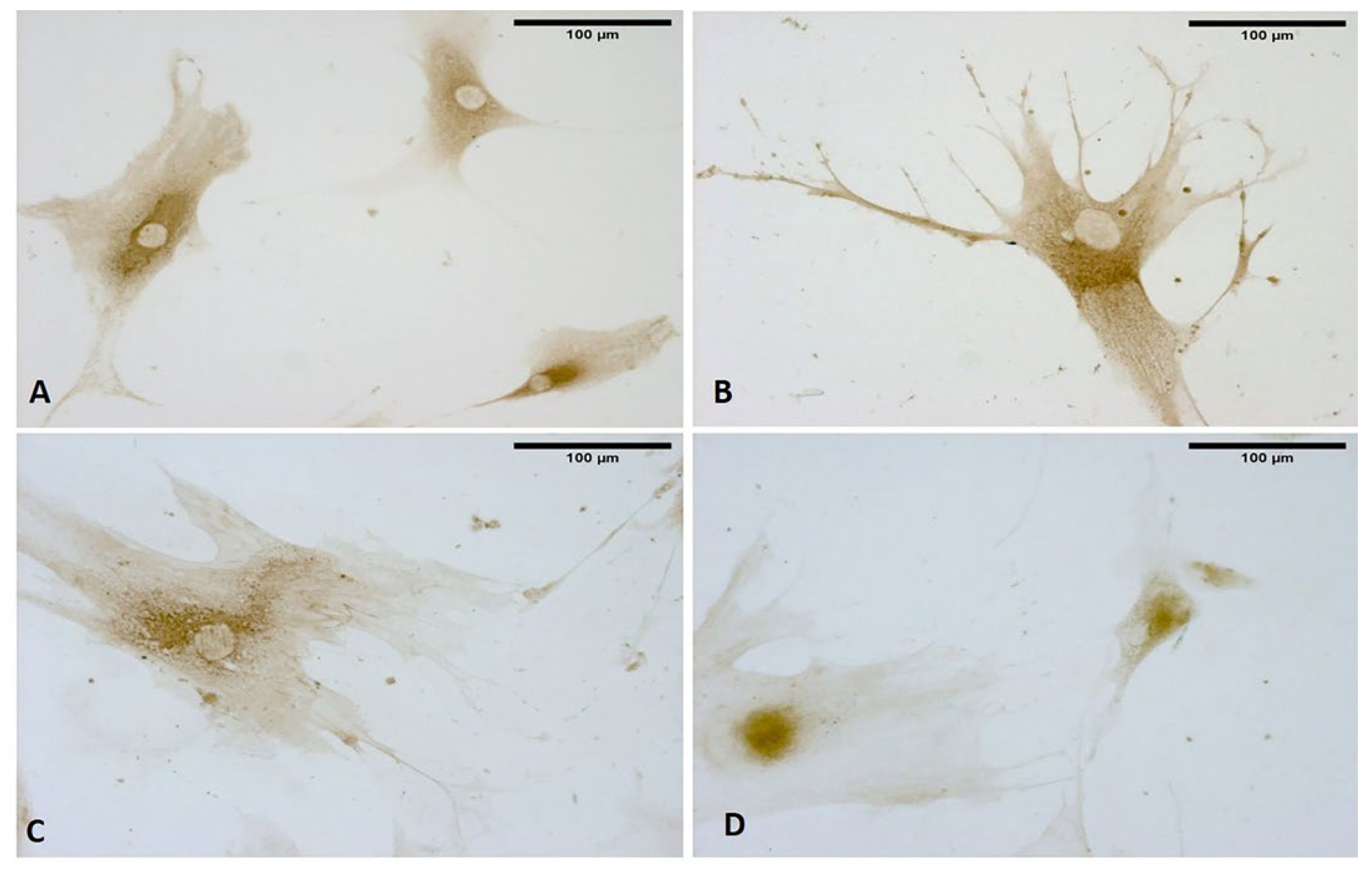
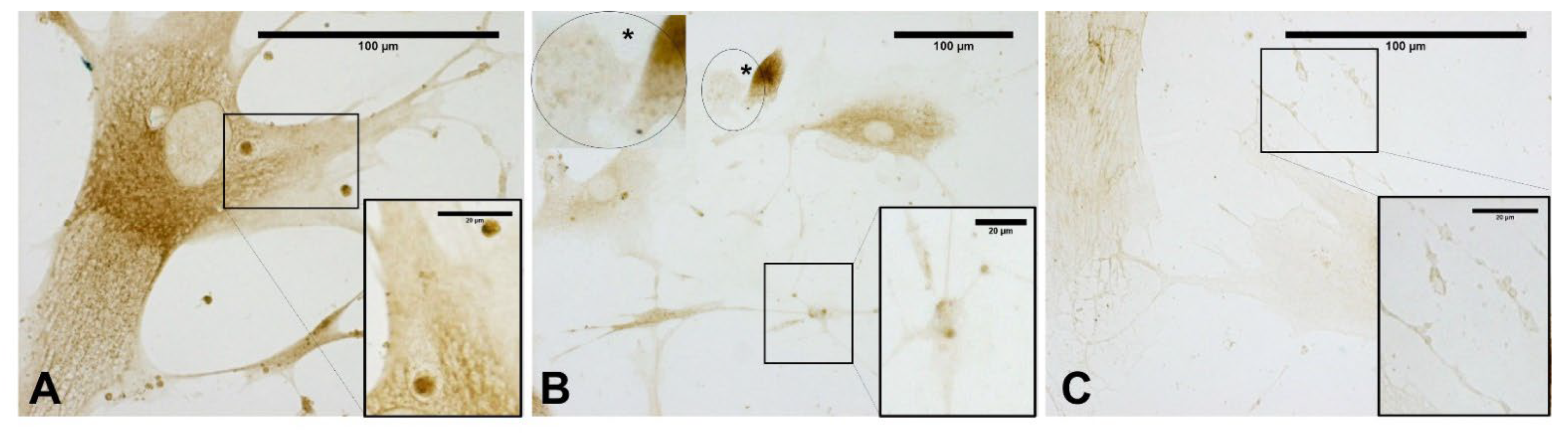
2.8. Immunocytochemistry to Detect HABP (Hyaluronic Acid Binding Protein)
2.9. Immunocytochemistry to Detect Collagen Type I and III
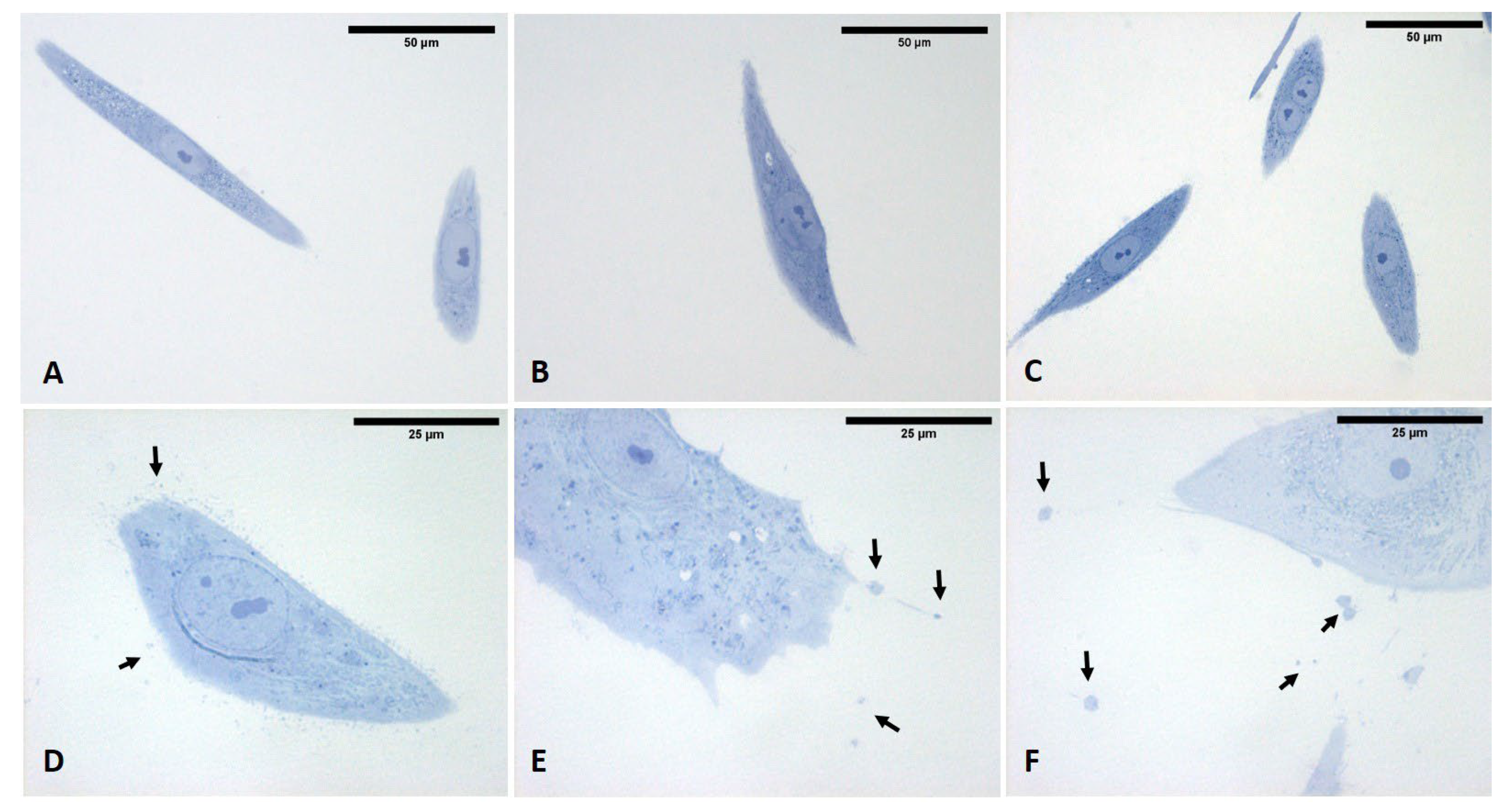
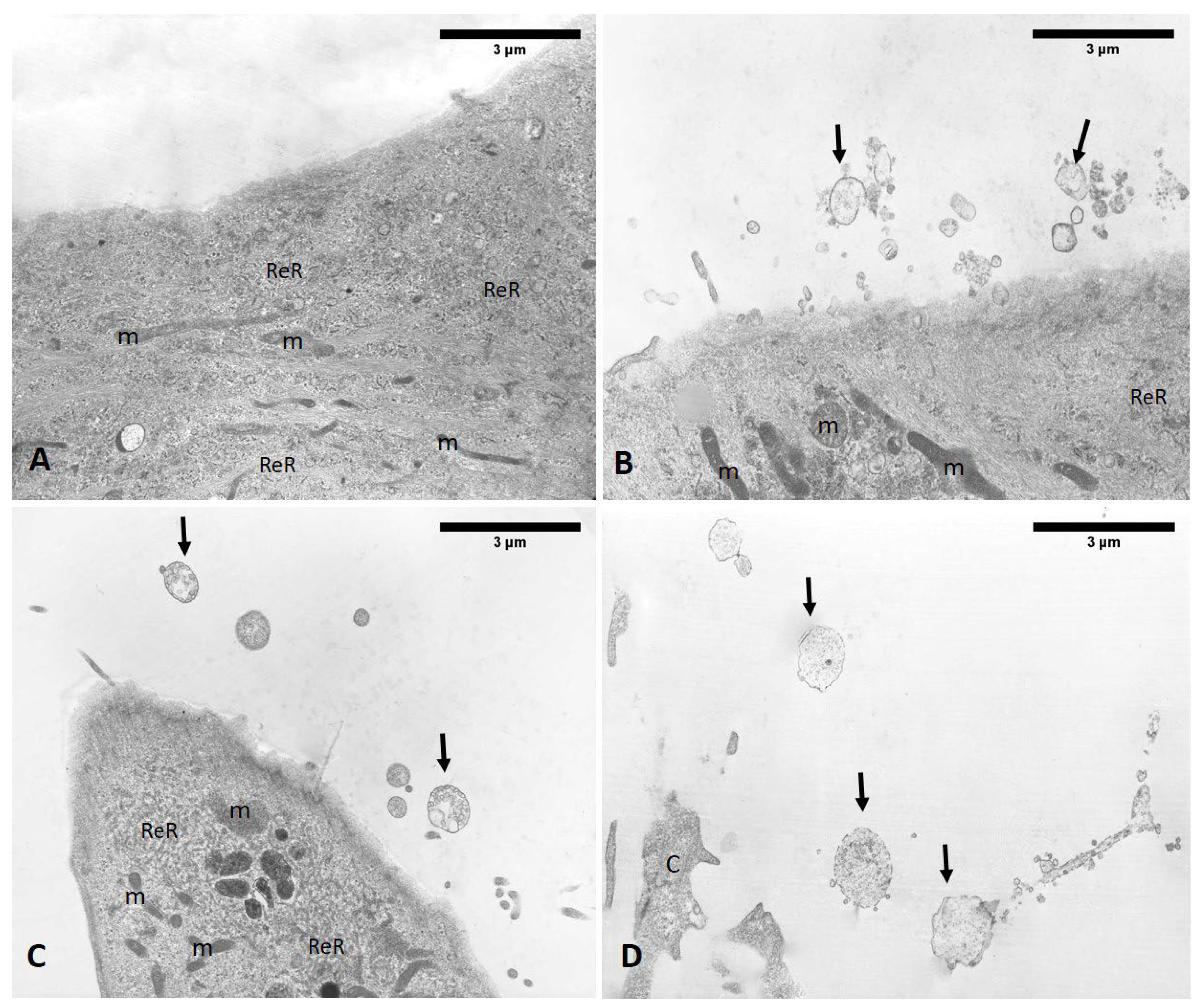
2.10. Semithin Sections and Transmission Electron Microscopy (TEM) Analysis
2.11. Image Acquisition and Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Martini, L.; Fini, M.; Giavaresi, G.; Torricelli, P.; de Pretto, M.; Rimondini, L.; Giardino, R. Primary osteoblasts response to shock wave therapy using different parameters. Artif. Cells Blood Substit. Biotechnol. 2003, 31, 449–466. [Google Scholar] [CrossRef] [PubMed]
- Furia, J.P. High-energy extracorporeal shock wave therapy as a treatment for insertional Achilles tendinopathy. Am. J. Sports Med. 2006, 34, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Rompe, J.D. Shock wave therapy for chronic Achilles tendon pain: A randomized placebo-controlled trial. Clin. Orthop. Relat. Res. 2006, 445, 276–277. [Google Scholar] [CrossRef] [PubMed]
- Rompe, J.D.; Decking, J.; Schoellner, C.; Theis, C. Repetitive low-energy shock wave treatment for chronic lateral epicondylitis in tennis players. Am. J. Sports Med. 2004, 32, 734–743. [Google Scholar] [CrossRef]
- Wuerfel, T.; Schmitz, C.; Jokinen, L.L.J. The Effects of the Exposure of Musculoskeletal Tissue to Extracorporeal Shock Waves. Biomedicines 2022, 10, 1084. [Google Scholar] [CrossRef]
- Li, B.; Wang, R.; Huang, X.; Ou, Y.; Jia, Z.; Lin, S.; Zhang, Y.; Xia, H.; Chen, B. Extracorporeal shock wave therapy promotes osteogenic differentiation in a rabbit osteoporosis model. Front. Endocrinol. 2021, 12, 627718. [Google Scholar] [CrossRef]
- Inoue, S.; Hatakeyama, J.; Aoki, H.; Kuroki, H.; Niikura, T.; Oe, K.; Fukui, T.; Kuroda, R.; Akisue, T.; Moriyama, H. Utilization of mechanical stress to treat osteoporosis: The effects of electrical stimulation, radial extracorporeal shock wave, and ultrasound on experimental osteoporosis in ovariectomized rats. Calcif. Tissue Int. 2021, 109, 215–229. [Google Scholar] [CrossRef]
- Zhao, Z.; Wang, Y.; Wang, Q.; Liang, J.; Hu, W.; Zhao, S.; Li, P.; Zhu, H.; Li, Z. Radial extracorporeal shockwave promotes subchondral bone stem/progenitor cell self-renewal by activating YAP/TAZ and facilitates cartilage repair in vivo. Stem Cell Res. Ther. 2021, 12, 19. [Google Scholar] [CrossRef]
- Waugh, C.M.; Morrissey, D.; Jones, E.; Riley, G.P.; Langberg, H.; Screen, H.R. In vivo biological response to extracorporeal shockwave therapy in human tendinopathy. Eur. Cell Mater. 2015, 29, 268–280. [Google Scholar] [CrossRef]
- Vulpiani, M.C.; Trischitta, D.; Trovato, P.; Vetrano, M.; Ferretti, A. Extracorporeal shockwave therapy (ESWT) in Achilles tendinopathy. A long-term follow-up observational study. J. Sports Med. Phys. Fit. 2009, 49, 171–176. [Google Scholar]
- Cinar, B.M.; Circi, E.; Balcik, C.; Guven, G.; Akpinar, S.; Derincek, A. The effects of extracorporeal shock waves on carrageenaninduced achilles tendinitis in rats: A biomechanical and histological analysis. Acta Orthop. Traumatol. Turc. 2013, 47, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Hong, J.; Piao, Y.; Shin, H.J.; Lee, S.J.; Rhyu, I.J.; Yi, M.H.; Kim, J.; Kim, D.W.; Beom, J. Extracorporeal shockwave therapy enhances peripheral nerve remyelination and gait function in a crush model. Adv. Clin. Exp. Med. 2020, 29, 819–824. [Google Scholar] [CrossRef] [PubMed]
- Sagir, D.; Bereket, C.; Onger, M.E.; Bakhit, N.; Keskin, M.; Ozkan, E. Efficacy of extracorporeal shockwaves therapy on peripheral nerve regeneration. J. Craniofacial Surg. 2019, 30, 2635–2639. [Google Scholar] [CrossRef]
- Yin, T.C.; Wu, R.W.; Sheu, J.J.; Sung, P.H.; Chen, K.H.; Chiang, J.Y.; Hsueh, S.K.; Chung, W.J.; Lin, P.Y.; Hsu, S.L.; et al. Combined therapy with extracorporeal shock wave and adipose-derived mesenchymal stem cells remarkably improved acute ischemia-reperfusion injury of quadriceps muscle. Oxid. Med. Cell. Longev. 2018, 2018, 6012636. [Google Scholar] [CrossRef] [PubMed]
- Tognolo, L.; Giordani, F.; Biz, C.; Bernini, A.; Ruggieri, P.; Stecco, C.; Frigo, A.C.; Masiero, S. Myofascial points treatment with focused extracorporeal shock wave therapy (f-ESWT) for plantar fasciitis: An open label randomized clinical trial. Eur. J. Phys. Rehabil. Med. 2022, 58, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Stecco, A.; Gesi, M.; Stecco, C.; Stern, R. Fascial Components of the Myofascial Pain Syndrome. Curr. Pain Headache Rep. 2013, 17, 352. [Google Scholar] [CrossRef]
- Langevin, H.M. Fascia Mobility, Proprioception, and Myofascial Pain. Life 2021, 11, 668. [Google Scholar] [CrossRef]
- Wang, C.; Wang, F.; Yang, K. Shock wave therapy induces neovascularization at the tendon-bone junction. A study in rabbits. J. Orthop. Res. 2003, 21, 984–989. [Google Scholar] [CrossRef]
- Mariotto, S.; Cavalieri, E.; Amelio, E.; Ciampa, A.R.; de Prati, A.C.; Marlinghaus, E.; Russo, S.; Suzuki, H. Extracorporeal shock waves: From lithotripsy to anti-inflammatory action by NO production. Nitric Oxide 2005, 12, 89–96. [Google Scholar] [CrossRef]
- Frairia, R.; Berta, L. Biological effects of extracorporeal shock waves on fibroblasts: A review. Muscles Ligaments Tendons J. 2012, 1, 138–147. [Google Scholar]
- D’Agostino, M.C.; Craig, K.; Tibalt, E.; Respizzi, S. Shock wave as biological therapeutic tool: From mechanical stimulation to recovery and healing, through mechanotransduction. Int. J. Surg. 2015, 24, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Basoli, V.; Chaudary, S.; Cruciani, S.; Santaniello, S.; Balzano, F.; Ventura, C.; Redl, H.; Dungel, P.; Maioli, M. Mechanical Stimulation of Fibroblasts by Extracorporeal Shock Waves: Modulation of Cell Activation and Proliferation through a Transient Proinflammatory Milieu. Cell Transplant. 2020, 29, 0963689720916175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stecco, C.; Stern, R.; Porzionato, A.; Macchi, V.; Masiero, S.; Stecco, A.; De Caro, R. Hyaluronan within fascia in the etiology of myofascial pain. Surg. Radiol. Anat. 2011, 33, 891–896. [Google Scholar] [CrossRef]
- Birk, D.E.; Mayne, R. Localization of collagen type I, III and V during tendon development. Changes in collagen type I and III are correlated with changes in fibril diameter. Eur. J. Cell Biol. 1997, 72, 352–361. [Google Scholar]
- Fede, C.; Pirri, C.; Fan, C.; Albertin, G.; Porzionato, A.; Macchi, V.; De Caro, R.; Stecco, C. Sensitivity of the fasciae to sex hormone levels: Modulation of collagen-I, collagen-III and fibrillin production. PLoS ONE 2019, 14, e0223195. [Google Scholar] [CrossRef] [PubMed]
- Fede, C.; Pirri, C.; Petrelli, L.; Guidolin, D.; Fan, C.; De Caro, R.; Stecco, C. Sensitivity of the Fasciae to the Endocannabinoid System: Production of Hyaluronan-Rich Vesicles and Potential Peripheral Effects of Cannabinoids in Fascial Tissue. Int. J. Mol. Sci. 2020, 21, 2936. [Google Scholar] [CrossRef]
- Iqbal, J.; Zaidi, M. Molecular regulation of mechanotransduction. Biochem. Biophys. Res. Commun. 2005, 328, 751–755. [Google Scholar] [CrossRef] [PubMed]
- Vogel, V. Mechanotrasduction involving multimodular proteins: Converting force into biochemical signals. Annu. Rev. Biophys. Biomol. Struct. 2006, 35, 459–488. [Google Scholar] [CrossRef]
- Hsu, C.; Chang, J. Clinical implications of growth factors in flexor tendon wound healing. J. Hand Surg. 2004, 29, 551–563. [Google Scholar] [CrossRef]
- Ryskalin, L.; Morucci, G.; Natale, G.; Soldani, P.; Gesi, M. Molecular Mechanisms Underlying the Pain-Relieving Effects of Extracorporeal Shock Wave Therapy: A Focus on Fascia Nociceptors. Life 2022, 12, 743. [Google Scholar] [CrossRef]
- Pavan, P.G.; Stecco, A.; Stern, R.; Stecco, C. Painful connections: Densification versus fibrosis of fascia. Curr. Pain Headache Rep. 2014, 18, 441. [Google Scholar] [CrossRef] [PubMed]
- Fede, C.; Albertin, G.; Petrelli, L.; Sfriso, M.M.; Biz, C.; De Caro, R.; Stecco, C. Expression of the endocannabinoid receptors in human fascial tissue. Eur. J. Histochem. 2016, 60, 2643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spinazzi, R.; Petrelli, L.; Guidolin, D.; Carraro, G.; Casale, V.; Tortorella, C.; Neri, G.; Albertin, G.; Andreis, P.G.; Nussdorfer, G.G. In vitro culture on Matrigel favors the long-term maintenance of rat zona glomerulosa-cell differentiated phenotype. Int. J. Mol. Med. 2006, 17, 1101–1110. [Google Scholar] [CrossRef] [PubMed]
- Chao, Y.H.; Tsuang, Y.H.; Sun, J.S.; Chen, L.T.; Chiang, Y.F.; Wang, C.C.; Chen, M.H. Effect of shock waves on tenocyte proliferation and extracellular matrix metabolism. Ultrasound Med. Biol. 2008, 34, 841–852. [Google Scholar] [CrossRef]
- Venturini, A.; Passalacqua, M.; Pelassa, S.; Pastorino, F.; Tedesco, M.; Cortese, K.; Gagliani, M.C.; Leo, G.; Maura, G.; Guidolin, D.; et al. Exosomes from Astrocyte Processes: Signaling to Neurons. Front. Pharmacol. 2019, 10, 1452. [Google Scholar] [CrossRef] [Green Version]
- Litwiniuk, M.; Krejner, A.; Speyrer, M.S.; Gauto, A.R.; Grzela, T. Hyaluronic Acid in Inflammation and Tissue Regeneration. Wounds 2016, 28, 78–88. [Google Scholar]
- Arasu, U.T.; Kärnä, R.; Härkönen, K.; Oikari, S.; Koistinen, A.; Kröger, H.; Qu, C.; Lammi, M.J.; Rilla, K. Human Mesenchymal Stem Cells Secrete Hyaluronan-Coated Extracellular Vesicles. Matrix Biol. 2017, 64, 54–68. [Google Scholar] [CrossRef]
- Camussi, G.; Deregibus, M.C.; Bruno, S.; Grange, C.; Fonsato, V.; Tetta, C. Exosome/microvesicle-mediated epigenetic reprogramming of cells. Am. J. Cancer Res. 2011, 1, 98–110. [Google Scholar]
- Cowman, M.K.; Schmidt, T.A.; Raghavan, P.; Stecco, A. Viscoelastic properties of hyaluronan in physiological conditions. F1000Research 2015, 4, 622. [Google Scholar] [CrossRef] [Green Version]
- Wang, F.S.; Yang, K.D.; Chen, R.F.; Wang, C.J.; Sheen-Chen, S.M. Extracorporeal shock wave promotes growth and differentiation of bone-marrow stromal cells towards osteoprogenitors associated with induction of TGF-β1. J. Bone Jt. Surg. 2002, 84, 457–461. [Google Scholar] [CrossRef]
- Wang, L.; Qin, L.; Cheung, W.H.; Yang, H.; Wong, W.N.; Chan, K.M.; Leung, K.S. Extracorporeal shock wave therapy in treatment of delayed bone-tendon healing. Am. J. Sports Med. 2008, 36, 340–347. [Google Scholar] [CrossRef] [PubMed]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
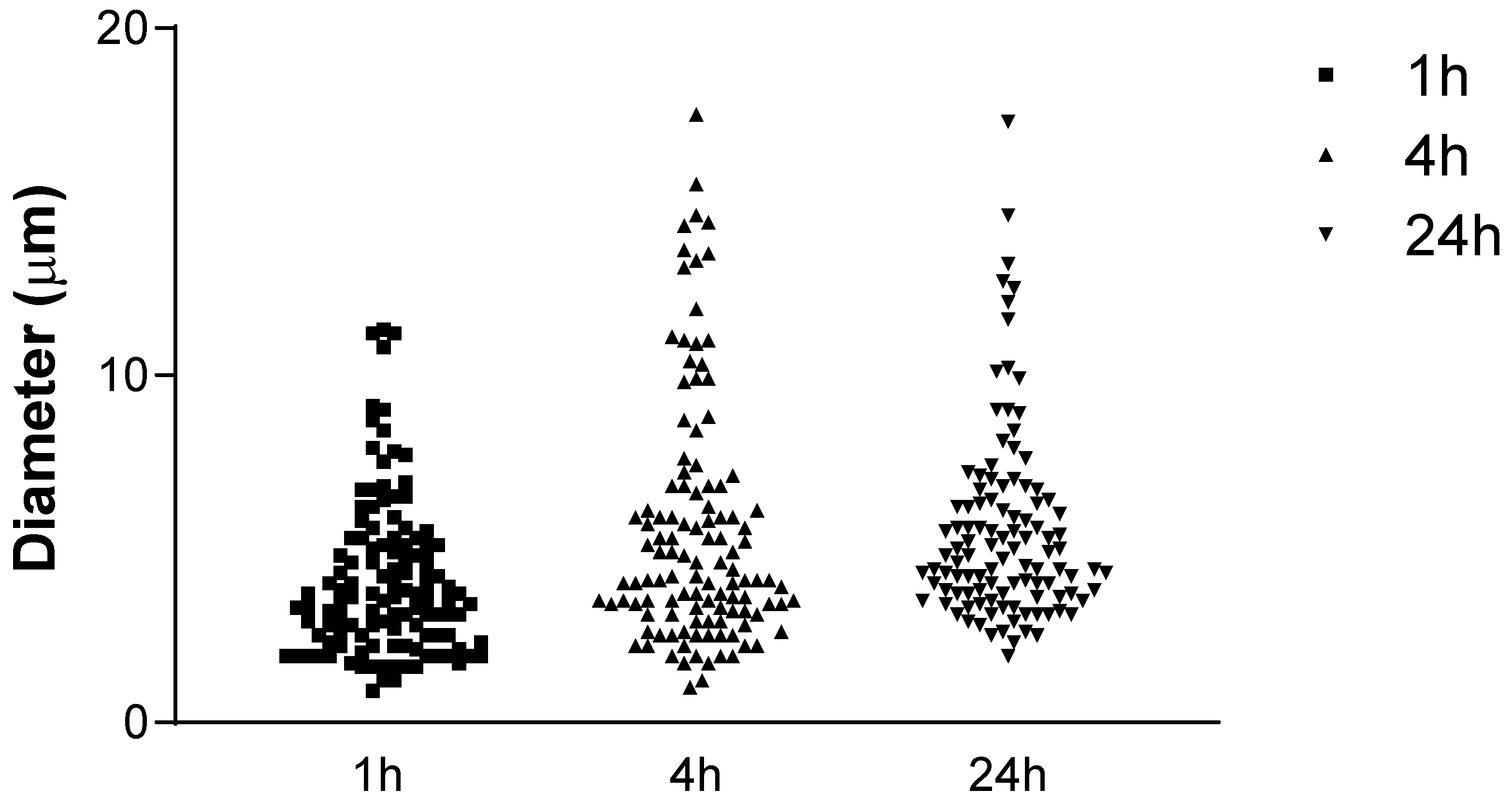
| Type of Comparison | Mean Rank Diff. | Significant | Summary | p-Value |
|---|---|---|---|---|
| 1 h vs. 4 h | −43.02 | Yes | ** | <0.01 |
| 1 h vs. 24 h | −61.33 | Yes | **** | <0.0001 |
| 4 h vs. 24 h | −18.31 | No | n.s. | >0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pirri, C.; Fede, C.; Petrelli, L.; De Rose, E.; Biz, C.; Guidolin, D.; De Caro, R.; Stecco, C. Immediate Effects of Extracorporeal Shock Wave Therapy in Fascial Fibroblasts: An In Vitro Study. Biomedicines 2022, 10, 1732. https://doi.org/10.3390/biomedicines10071732
Pirri C, Fede C, Petrelli L, De Rose E, Biz C, Guidolin D, De Caro R, Stecco C. Immediate Effects of Extracorporeal Shock Wave Therapy in Fascial Fibroblasts: An In Vitro Study. Biomedicines. 2022; 10(7):1732. https://doi.org/10.3390/biomedicines10071732
Chicago/Turabian StylePirri, Carmelo, Caterina Fede, Lucia Petrelli, Enrico De Rose, Carlo Biz, Diego Guidolin, Raffaele De Caro, and Carla Stecco. 2022. "Immediate Effects of Extracorporeal Shock Wave Therapy in Fascial Fibroblasts: An In Vitro Study" Biomedicines 10, no. 7: 1732. https://doi.org/10.3390/biomedicines10071732