
Androstenedione and Follicle-Stimulating Hormone Concentration Predict the Progression of Frailty Syndrome at One Year Follow-Up in Patients with Localized Breast Cancer Treated with Aromatase Inhibitors



Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Study Variables
2.3. Measurement of Frailty Syndrome
2.4. Statistical Analysis
3. Results
3.1. Sociodemographic and Clinical Data
3.2. Changes in Frailty Syndrome over Time under Treatment with Aromatase Inhibitors
3.3. Relationship between Clinical Characteristics and the Progression of Frailty Syndrome
3.4. Changes in Gonadotropins, Androgens and Estrogens under AROi Treatment
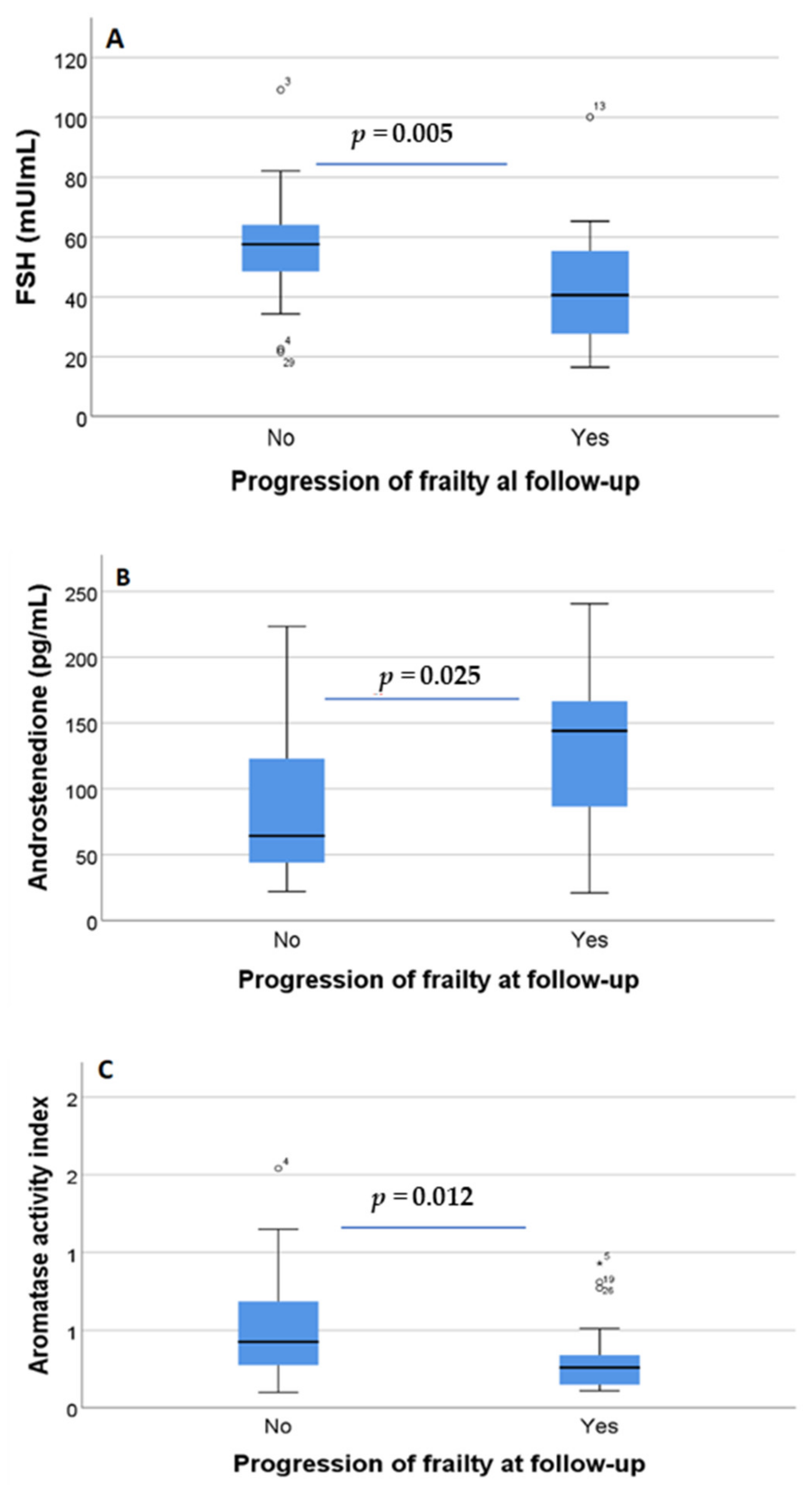
3.5. Relationship between Androgen and Estrogen Concentrations in Blood and the Progression of Frailty Syndrome
3.6. Diagnostic Sensitivity and Specificity of the Selected Biomarkers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maxwell Parkin, D.; Bray, F.; Ferlay, J.; Pisani, P. Estimating the world cancer burden: Globocan 2000. Int. J. Cancer 2001, 94, 153–156. [Google Scholar] [CrossRef] [PubMed]
- Estadísticas de Cáncer de Mama de EE UU. Available online: www.breastcancer.org (accessed on 1 February 2022).
- Sledge, G.W.; Mamounas, E.P.; Hortobagyi, G.N.; Burstein, H.J.; Goodwin, P.J.; Wolff, A.C. Past, Present, and Future Challenges in Breast Cancer Treatment. J. Clin. Oncol. 2014, 32, 1979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hershman, D.L.; Loprinzi, C.; Schneider, B.P.; Hershman, D.L.; Loprinzi, C.; Schneider, B.P. Symptoms: Aromatase Inhibitor Induced Arthralgias. Adv. Exp. Med. Biol. 2015, 862, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Goss, P.E.; Ingle, J.N.; Martino, S.; Robert, N.J.; Muss, H.B.; Piccart, M.J.; Castiglione, M.; Tu, D.; Shepherd, L.E.; Pritchard, K.I.; et al. A Randomized Trial of Letrozole in Postmenopausal Women after Five Years of Tamoxifen Therapy for Early-Stage Breast Cancer. N. Engl. J. Med. 2009, 349, 1793–1802. [Google Scholar] [CrossRef]
- Finch, C.E. The menopause and aging, a comparative perspective. J. Steroid Biochem. Mol. Biol. 2014, 142, 132–141. [Google Scholar] [CrossRef] [Green Version]
- Nelson, H.D. Menopause. Lancet 2008, 371, 760–770. [Google Scholar] [CrossRef]
- McNeil, M.A.; Merriam, S.B. Menopause. Ann. Intern. Med. 2021, 174, ITC97–ITC112. [Google Scholar] [CrossRef]
- Roberts, H.; Hickey, M. Managing the menopause: An update. Maturitas 2016, 86, 53–58. [Google Scholar] [CrossRef]
- Collard, R.M.; Boter, H.; Schoevers, R.A.; Oude Voshaar, R.C. Prevalence of frailty in community-dwelling older persons: A systematic review. J. Am. Geriatr. Soc. 2012, 60, 1487–1492. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Verschoor, C.P.; Tamim, H. Frailty is inversely related to age at menopause and elevated in women who have had a hysterectomy: An analysis of the Canadian longitudinal study on aging. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2019, 74, 675–682. [Google Scholar] [CrossRef]
- Fried, L.P.; Ferrucci, L.; Darer, J.; Williamson, J.D.; Anderson, G. Untangling the Concepts of Disability, Frailty, and Comorbidity: Implications for Improved Targeting and Care. J. Gerontol. Ser. A 2004, 59, M255–M263. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Garrido, J.; Ruiz-Ros, V.; Buigues, C.; Navarro-Martinez, R.; Cauli, O. Clinical features of prefrail older individuals and emerging peripheral biomarkers: A systematic review. Arch. Gerontol. Geriatr. 2014, 59, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef] [PubMed]
- Ethun, C.G.; Bilen, M.A.; Jani, A.B.; Maithel, S.K.; Ogan, K.; Master, V.A. Frailty and cancer: Implications for oncology surgery, medical oncology, and radiation oncology. CA Cancer J. Clin. 2017, 67, 362–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burger, H.G. The endocrinology of the menopause. Maturitas 1996, 23, 129–136. [Google Scholar] [CrossRef]
- Vagenakis, A.G. Endocrine aspects of menopause. Clin. Rheumatol. 1989, 8, 48–51. [Google Scholar] [CrossRef]
- Cai, T.; Morgia, G.; Carrieri, G.; Terrone, C.; Imbimbo, C.; Verze, P.; Mirone, V.; La Rocca, R. An improvement in sexual function is related to better quality of life, regardless of urinary function improvement: Results from the IDIProst® Gold Study. Arch. Ital. Urol. Androl. 2013, 85, 184–189. [Google Scholar] [CrossRef]
- Gonsalves, L.; Hindin, M.J.; Bayer, A.; Carcamo, C.P.; Gichangi, P.; Habib, N.; Mwaisaka, J.; Say, L. Protocol of an open, three-arm, individually randomized trial assessing the effect of delivering sexual and reproductive health information to young people (aged 13-24) in Kenya and Peru via mobile phones: Adolescent/youth reproductive mobile access and delivery initiative for love and life outcomes (ARMADILLO) study stage 2. Reprod. Health 2018, 15, 126. [Google Scholar] [CrossRef]
- Arlt, W.; Callies, F.; Allolio, B. Dhea replacement in women with adrenal insufficiency—Pharmacokinetics, bioconversion and clinical effects on well-being, sexuality and cognition. Endocr. Res. 2000, 26, 505–511. [Google Scholar] [CrossRef]
- Carcaillon, L.; García-García, F.J.; Tresguerres, J.A.F.; Gutiérrez Avila, G.; Kireev, R.; Rodríguez-Mãnas, L. Higher levels of endogenous estradiol are associated with frailty in postmenopausal women from the toledo study for healthy aging. J. Clin. Endocrinol. Metab. 2012, 97, 2898–2906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Sánchez, J.; Mafla-España, M.A.; Tejedor-Cabrera, C.; Avellán-Castillo, O.; Torregrosa, M.D.; Cauli, O. Plasma Aromatase Activity Index, Gonadotropins and Estrone Are Associated with Frailty Syndrome in Post-Menopausal Women with Breast Cancer. Curr. Oncol. 2022, 29, 1744–1760. [Google Scholar] [CrossRef] [PubMed]
- Varadhan, R.; Walston, J.; Cappola, A.R.; Carlson, M.C.; Wand, G.S.; Fried, L.P. Higher levels and blunted diurnal variation of cortisol in frail older women. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 190–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jerzak, K.J.; Desautels, D.N.; Pritchard, K.I. An update on adjuvant systemic therapy for elderly patients with early breast cancer. Expert Opin. Pharmacother. 2016, 17, 1881–1888. [Google Scholar] [CrossRef] [PubMed]
- Rani, A.; Stebbing, J.; Giamas, G.; Murphy, J. Endocrine resistance in hormone receptor positive breast cancer—From mechanism to therapy. Front. Endocrinol. 2019, 10, 245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Caoimh, R.; Galluzzo, L.; Rodríguez-Laso, Á.; Van Der Heyden, J.; Ranhoff, A.H.; Carcaillon-Bentata, L.; Beltzer, N.; Kennelly, S.; Liew, A. Transitions and trajectories in frailty states over time: A systematic review of the European Joint Action ADVANTAGE. Ann. Ist. Super. Sanita 2018, 54, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Travers, J.; Romero-Ortuno, R.; Bailey, J.; Cooney, M.T. Delaying and reversing frailty: A systematic review of primary care interventions. Br. J. Gen. Pract. 2019, 69, e61–e69. [Google Scholar] [CrossRef]
- Lorenzo-López, L.; López-López, R.; Maseda, A.; Buján, A.; Rodríguez-Villamil, J.L.; Millán-Calenti, J.C. Changes in frailty status in a community-dwelling cohort of older adults: The VERISAÚDE study. Maturitas 2019, 119, 54–60. [Google Scholar] [CrossRef]
- Leng, S.; Chen, X.; Mao, G. Frailty syndrome: An overview. Clin. Interv. Aging 2014, 9, 433. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Maxwell, C.A.; Yu, F. Biological Processes and Biomarkers Related to Frailty in Older Adults: A State-of-the-Science Literature Review. Biol. Res. Nurs. 2019, 21, 80–106. [Google Scholar] [CrossRef]
- Inglés, M.; Mas-Bargues, C.; Gimeno-Mallench, L.; Cruz-Guerrero, R.; García-García, F.J.; Gambini, J.; Borrás, C.; Rodríguez-Mañas, L.; Viña, J. Relation Between Genetic Factors and Frailty in Older Adults. J. Am. Med. Dir. Assoc. 2019, 20, 1451–1457. [Google Scholar] [CrossRef] [PubMed]
- Yan, C.H.; Coleman, C.; Nabulsi, N.A.; Chiu, B.C.H.; Ko, N.Y.; Hoskins, K.; Calip, G.S. Associations between frailty and cancer-specific mortality among older women with breast cancer. Breast Cancer Res. Treat. 2021, 189, 769–779. [Google Scholar] [CrossRef] [PubMed]
- Haghighat, S.; Akbari, M.E.; Holakouei, K.; Rahimi, A.; Montazeri, A. Factors predicting fatigue in breast cancer patients. Support. Care Cancer 2003, 11, 533–538. [Google Scholar] [CrossRef]
- Schmidt, M.E.; Chang-Claude, J.; Seibold, P.; Vrieling, A.; Heinz, J.; Flesch-Janys, D.; Steindorf, K. Determinants of long-term fatigue in breast cancer survivors: Results of a prospective patient cohort study. Psychooncology 2015, 24, 40–46. [Google Scholar] [CrossRef]
- Dias, J.P.; Melvin, D.; Simonsick, E.M.; Carlson, O.; Shardell, M.D.; Ferrucci, L.; Chia, C.W.; Basaria, S.; Egan, J.M. Effects of aromatase inhibition vs. testosterone in older men with low testosterone: Randomized-controlled trial. Andrology 2016, 4, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forrest, K.Y.Z.; Zmuda, J.M.; Cauley, J.A. Correlates of decline in lower extremity performance in older women: A 10-year follow-up study. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 1194–1200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laakkonen, E.K.; Soliymani, R.; Karvinen, S.; Kaprio, J.; Kujala, U.M.; Baumann, M.; Sipilä, S.; Kovanen, V.; Lalowski, M. Estrogenic regulation of skeletal muscle proteome: A study of premenopausal women and postmenopausal MZ cotwins discordant for hormonal therapy. Aging Cell 2017, 16, 1276–1287. [Google Scholar] [CrossRef]
- Garcia-Martinez, L.; Zhang, Y.; Nakata, Y.; Chan, H.L.; Morey, L. Epigenetic mechanisms in breast cancer therapy and resistance. Nat. Commun. 2021, 12, 1786. [Google Scholar] [CrossRef]
- Wu, I.C.; Lin, X.Z.; Liu, P.F.; Tsai, W.L.; Shiesh, S.C. Low serum testosterone and frailty in older men and women. Maturitas 2010, 67, 348–352. [Google Scholar] [CrossRef]
- Peng, X.; Hou, L.; Zhao, Y.; Lin, T.; Wang, H.; Gao, L.; Yue, J. Frailty and testosterone level in older adults: A systematic review and meta-analysis. Eur. Geriatr. Med. 2022, 13, 663–673. [Google Scholar] [CrossRef]
- Ruan, H.; Hu, J.; Zhao, J.; Tao, H.; Chi, J.; Niu, X.; Zhang, J.; Wang, Y. Menopause and frailty: A scoping review. Menopause 2020, 27, 1185–1195. [Google Scholar] [CrossRef] [PubMed]
- Nedergaard, A.; Henriksen, K.; Karsdal, M.A.; Christiansen, C. Menopause, estrogens and frailty. Gynecol. Endocrinol. 2013, 29, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Evans, W.J.; Paolisso, G.; Abbatecola, A.M.; Corsonello, A.; Bustacchini, S.; Strollo, F.; Lattanzio, F. Frailty and muscle metabolism dysregulation in the elderly. Biogerontology 2010, 11, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Fougère, B.; Boulanger, E.; Nourhashémi, F.; Guyonnet, S.; Cesari, M. Chronic inflammation: Accelerator of biological aging. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2017, 72, 1218–1225. [Google Scholar] [CrossRef] [Green Version]
- Leng, S.X.; Yang, H.; Walston, J.D. Decreased cell proliferation and altered cytokine production in frail older adults. Aging Clin. Exp. Res. 2004, 16, 249–252. [Google Scholar] [CrossRef]
- Walston, J.; Bandeen-Roche, K.; Buta, B.; Bergman, H.; Gill, T.M.; Morley, J.E.; Fried, L.P.; Robinson, T.N.; Afilalo, J.; Newman, A.B.; et al. Moving Frailty Towards Clinical Practice: NIA Intramural Frailty Science Symposium Summary. J. Am. Geriatr. Soc. 2019, 67, 1559. [Google Scholar] [CrossRef]
- Boreskie, K.F.; Hay, J.L.; Boreskie, P.E.; Arora, R.C.; Duhamel, T.A. Frailty-aware care: Giving value to frailty assessment across different healthcare settings. BMC Geriatr. 2022, 22, 13. [Google Scholar] [CrossRef]
- Korc-Grodzicki, B.; Holmes, H.M.; Shahrokni, A. Geriatric assessment for oncologists. Cancer Biol. Med. 2015, 12, 261. [Google Scholar] [CrossRef]
- Hadji, P.; Body, J.J.; Aapro, M.S.; Brufsky, A.; Coleman, R.E.; Guise, T.; Lipton, A.; Tubiana-Hulin, M. Practical guidance for the management of aromatase inhibitor-associated bone loss. Ann. Oncol. 2008, 19, 1407–1416. [Google Scholar] [CrossRef]
- Avvaru, S.P.; Noolvi, M.N.; Aminbhavi, T.M.; Chkraborty, S.; Dash, A.; Shukla, S.S. Aromatase Inhibitors Evolution as Potential Class of Drugs in the Treatment of Postmenopausal Breast Cancer Women. Mini Rev. Med. Chem. 2018, 18, 609–621. [Google Scholar] [CrossRef]
- Samavat, H.; Kurzer, M.S. Estrogen metabolism and breast cancer. Cancer Lett. 2015, 356, 231–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valko-Rokytovská, M.; Očenáš, P.; Salayová, A.; Kostecká, Z. Breast Cancer: Targeting of Steroid Hormones in Cancerogenesis and Diagnostics. Int. J. Mol. Sci. 2021, 22, 5878. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.J. Molecular Action and Clinical Relevance of Aromatase Inhibitors. Oncologist 1998, 3, 129–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casper, R.F. Aromatase inhibitors in ovarian stimulation. J. Steroid Biochem. Mol. Biol. 2007, 106, 71–75. [Google Scholar] [CrossRef]
- Pfeiler, G.; Königsberg, R.; Hadji, P.; Fitzal, F.; Maroske, M.; Dressel-Ban, G.; Zellinger, J.; Exner, R.; Seifert, M.; Singer, C.; et al. Impact of body mass index on estradiol depletion by aromatase inhibitors in postmenopausal women with early breast cancer. Br. J. Cancer 2013, 109, 1522–1527. [Google Scholar] [CrossRef] [Green Version]
- Santen, R.J.; Harvey, H.A. Use of aromatase inhibitors in breast carcinoma. Endocr. Relat. Cancer 1999, 6, 75–92. [Google Scholar] [CrossRef] [Green Version]
- Sluijmer, A.V.; Heineman, M.J.; De Jong, F.H.; Evers, J.L.H. Endocrine activity of the postmenopausal ovary: The effects of pituitary down-regulation and oophorectomy. J. Clin. Endocrinol. Metab. 1995, 80, 2163–2167. [Google Scholar] [CrossRef]
- Bancroft, J.; Cawood, E.H.H. Androgens and the menopause; a study of 40-60-year-old women. Clin. Endocrinol. 1996, 45, 577–587. [Google Scholar] [CrossRef]
- Zaidi, M.; New, M.I.; Blair, H.C.; Zallone, A.; Baliram, R.; Davies, T.F.; Cardozo, C.; Iqbal, J.; Sun, L.; Rosen, C.J.; et al. Actions of pituitary hormones beyond traditional targets. J. Endocrinol. 2018, 237, R83–R98. [Google Scholar] [CrossRef]
- Das, N.; Kumar, T.R. Molecular regulation of follicle-stimulating hormone synthesis, secretion and action. J. Mol. Endocrinol. 2018, 60, R131–R155. [Google Scholar] [CrossRef] [Green Version]
- Zaidi, M.; Lizneva, D.; Kim, S.M.; Sun, L.; Iqbal, J.; New, M.I.; Rosen, C.J.; Yuen, T. FSH, Bone Mass, Body Fat, and Biological Aging. Endocrinology 2018, 159, 3503–3514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guligowska, A.; Chrzastek, Z.; Pawlikowski, M.; Pigłowska, M.; Pisarek, H.; Winczyk, K.; Kostka, T. Gonadotropins at Advanced Age—Perhaps They Are Not So Bad? Correlations Between Gonadotropins and Sarcopenia Indicators in Older Adults. Front. Endocrinol. 2021, 12, 797243. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Ji, Y.; Yuen, T.; Rendina-Ruedy, E.; Demambro, V.E.; Dhawan, S.; Abu-Amer, W.; Izadmehr, S.; Zhou, B.; Shin, A.C.; et al. Blocking FSH induces thermogenic adipose tissue and reduces body fat. Nature 2017, 546, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Veldhuis-Vlug, A.G.; Woods, G.N.; Sigurdsson, S.; Ewing, S.K.; Le, P.T.; Hue, T.F.; Vittinghoff, E.; Xu, K.; Gudnason, V.; Sigurdsson, G.; et al. Serum FSH Is Associated With BMD, Bone Marrow Adiposity, and Body Composition in the AGES-Reykjavik Study of Older Adults. J. Clin. Endocrinol. Metab. 2021, 106, E1156–E1169. [Google Scholar] [CrossRef] [PubMed]
- Bulun, S.E.; Zeitoun, K.; Sasano, H.; Simpson, E.R. Aromatase in aging women. Semin. Reprod. Endocrinol. 1999, 17, 349–358. [Google Scholar] [CrossRef]
- Burger, H.G. Androgen production in women. Fertil. Steril. 2002, 77, 3–5. [Google Scholar] [CrossRef]
- Masamura, S.; Adlercreutz, H.; Harvey, H.; Lipton, A.; Demers, L.M.; Santen, R.J.; Santner, S.J. Aromatase inhibitor development for treatment of breast cancer. Breast Cancer Res. Treat. 1995, 33, 19–26. [Google Scholar] [CrossRef]
- Miller, W.L.; Auchus, R.J. The Molecular Biology, Biochemistry, and Physiology of Human Steroidogenesis and Its Disorders. Endocr. Rev. 2011, 32, 81. [Google Scholar] [CrossRef] [Green Version]
- Labrie, F.; Luu-The, V.; Labrie, C.; Simard, J. DHEA and its transformation into androgens and estrogens in peripheral target tissues: Intracrinology. Front. Neuroendocrinol. 2001, 22, 185–212. [Google Scholar] [CrossRef]
- Rivero-Segura, N.A.; Bello-Chavolla, O.Y.; Barrera-Vázquez, O.S.; Gutierrez-Robledo, L.M.; Gomez-Verjan, J.C. Promising biomarkers of human aging: In search of a multi-omics panel to understand the aging process from a multidimensional perspective. Ageing Res. Rev. 2020, 64, 101164. [Google Scholar] [CrossRef]
- Zhou, L.; Rueda, M.; Alkhateeb, A. Classification of Breast Cancer Nottingham Prognostic Index Using High-Dimensional Embedding and Residual Neural Network. Cancers 2022, 14, 934. [Google Scholar] [CrossRef] [PubMed]
- Walston, J.; Hadley, E.C.; Ferrucci, L.; Guralnik, J.M.; Newman, A.B.; Studenski, S.A.; Ershler, W.B.; Harris, T.; Fried, L.P. Research agenda for frailty in older adults: Toward a better understanding of physiology and etiology: Summary from the American Geriatrics Society/National Institute on Aging Research Conference on Frailty in Older Adults. J. Am. Geriatr. Soc. 2006, 54, 991–1001. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Frequency% (Categorical Variables) or Mean and Standard Error of the Mean (Range Min-Max) (Discrete Variables) |
|---|---|
| Age (years) | 66.8 ± 1.3 (52–83) |
| Marital status: | |
| Married | 23 (48.9%) |
| Divorced | 7 (14.9%) |
| Separated | 2 (4.3%) |
| Single | 4 (8.5%) |
| Widow | 11 (24.4%) |
| Histology of tumor: | |
| Ductal carcinoma | 46 (97.9%) |
| Lobular carcinoma | 1 (2.1%) |
| Estrogen receptor staining (%) | 93.1 ± 1.6 (40–100) |
| Progesterone receptor staining (%) | 61.3 ± 0.09 (1–3) |
| HER2-positive staining (patients with 3 + staining in HER2: 4 patients) | 2.5 ± 5.2 (0–10) |
| Ki67 mean values (%) | 15.4 ± 2.03 (1–60) |
| Previous chemotherapy | |
| Yes | 8 (17.0%) |
| No | 39 (83.0%) |
| Previous radiotherapy | |
| Yes | 44 (93.6%) |
| No | 3 (6.4%) |
| Charlson comorbidity index | 2.5 ± 0.1 (2–5) |
| Body mass index | 28.9 ± 0.8 (18.7–45) |
| Baseline | 6 Months | 12 Months | p-Value | |
|---|---|---|---|---|
| Weight loss | Yes 11 (23.4% | Yes 9 (19.2%) | Yes 9 (19.1%) | p = 0.9 |
| No 36 (76.6%) | No 38 (80.8%) | No 38 (80.9%) | ||
| Fatigue | Yes 5 (10.7%) | Yes 14 (29.7%) | Yes 13 (27.6%) | p = 0.04 |
| No 42 (89.3%) | No 33 (70.3%) | No 34 (72.3%) | ||
| Physical activity | Yes 18 (35.3%) | Yes 23 (45.1%) | Yes 21 (41.2%) | p = 0.438 |
| No 29 (56.9%) | No 24 (47.1%) | No 26 (51.0%) | ||
| Gait speed | Yes 4 (8.5%) | Yes 13 (27.6%) | Yes 17 (36.2%) | p = 0.001 |
| No 43 (78.7%) | No 34 (72.3%) | No 30 (63.8%) | ||
| Muscle strength | Yes 10 (21.3%) | Yes 14 (29.8%) | Yes 12 (25.5%) | p = 0.7 |
| No 37 (78.7%) | No 33 (70.2%) | No 35 (74.5%) |
| Variables | p-Value | OR | 95% CI |
|---|---|---|---|
| Age | 0.257 | 1.048 | 0.967–1.135 |
| Chemotherapy | 0.728 | 1.354 | 0.246–7.458 |
| Number of daily drugs | 0.934 | 0.986 | 0.703–1.383 |
| Charlson comorbidity index | 0.181 | 2.140 | 0.702–6.520 |
| Body mass index | 0.337 | 1.067 | 0.934–1.219 |
| Hormone Concentration in Plasma | Baseline | 6 Months of AROi Treatment | 12 Months of AROi Treatment | p-Value |
|---|---|---|---|---|
| FSH (mIU/mL) | 49.4 ± 2.93 | 52.31 ± 3.46 | 52.33 ± 3.54 | 0.01 |
| LH (mIU/mL) | 20.27 ± 1.25 | 20.5 ± 1.31 | 19.9 ± 1.59 | 0.92 |
| Progesterone (ng/mL) | 0.07 ± 0.03 | 0.08 ± 0.05 | 0.10 ± 0.08 | 0.62 |
| Estrone (pg/mL) | 31.3 ± 1.97 | 24.3 ± 1.4 | 24.1 ± 1.3 | 0.001 |
| Estradiol (pg/mL) | 7.57 ± 0.80 | 5.30 ± 0.21 | 5.9 ± 0.39 | 0.007 |
| Testosterone (ng/mL) | 0.27 ± 0.02 | 0.26 ± 0.02 | 0.27 ± 0.03 | 0.19 |
| Dehydroepiandrosterone (µg/dL) | 92.3 ± 8.16 | 83.3 ± 7.54 | 83.9 ± 7.71 | 0.57 |
| Androstenedione (pg/mL) | 108.4 ± 9.0 | 111.8 ± 7.8 | 117.9 ± 8.3 | 0.01 |
| Dihydrotestosterone (ng/mL) | 0.14 ± 0.009 | 0.15 ± 0.12 | 0.13 ± 0.10 | 0.36 |
| Aromatase activity index | 0.41 ± 0.05 | 0.26 ± 0.02 | 0.25 ± 0.02 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Sánchez, J.; Mafla-España, M.A.; Torregrosa, M.D.; Cauli, O. Androstenedione and Follicle-Stimulating Hormone Concentration Predict the Progression of Frailty Syndrome at One Year Follow-Up in Patients with Localized Breast Cancer Treated with Aromatase Inhibitors. Biomedicines 2022, 10, 1634. https://doi.org/10.3390/biomedicines10071634
García-Sánchez J, Mafla-España MA, Torregrosa MD, Cauli O. Androstenedione and Follicle-Stimulating Hormone Concentration Predict the Progression of Frailty Syndrome at One Year Follow-Up in Patients with Localized Breast Cancer Treated with Aromatase Inhibitors. Biomedicines. 2022; 10(7):1634. https://doi.org/10.3390/biomedicines10071634
Chicago/Turabian StyleGarcía-Sánchez, Javier, Mayra Alejandra Mafla-España, María Dolores Torregrosa, and Omar Cauli. 2022. "Androstenedione and Follicle-Stimulating Hormone Concentration Predict the Progression of Frailty Syndrome at One Year Follow-Up in Patients with Localized Breast Cancer Treated with Aromatase Inhibitors" Biomedicines 10, no. 7: 1634. https://doi.org/10.3390/biomedicines10071634