
Increased Oxidative Stress in Asthma—Relation to Inflammatory Blood and Lung Biomarkers and Airway Remodeling Indices

 ,
,  , , , , ,
, , , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Spirometry and Lung Computed Tomography (CT)
2.3. Bronchofiberoscopy and Airway Sample Collection
2.4. Laboratory Investigations
2.4.1. Basic Laboratory Tests
2.4.2. Coumarin Boronic Acid (CBA) Assay
2.5. Statistical Analysis
3. Results
3.1. Study Participants
3.2. Clinical Characteristics and Airway Remodeling in Asthma Patients
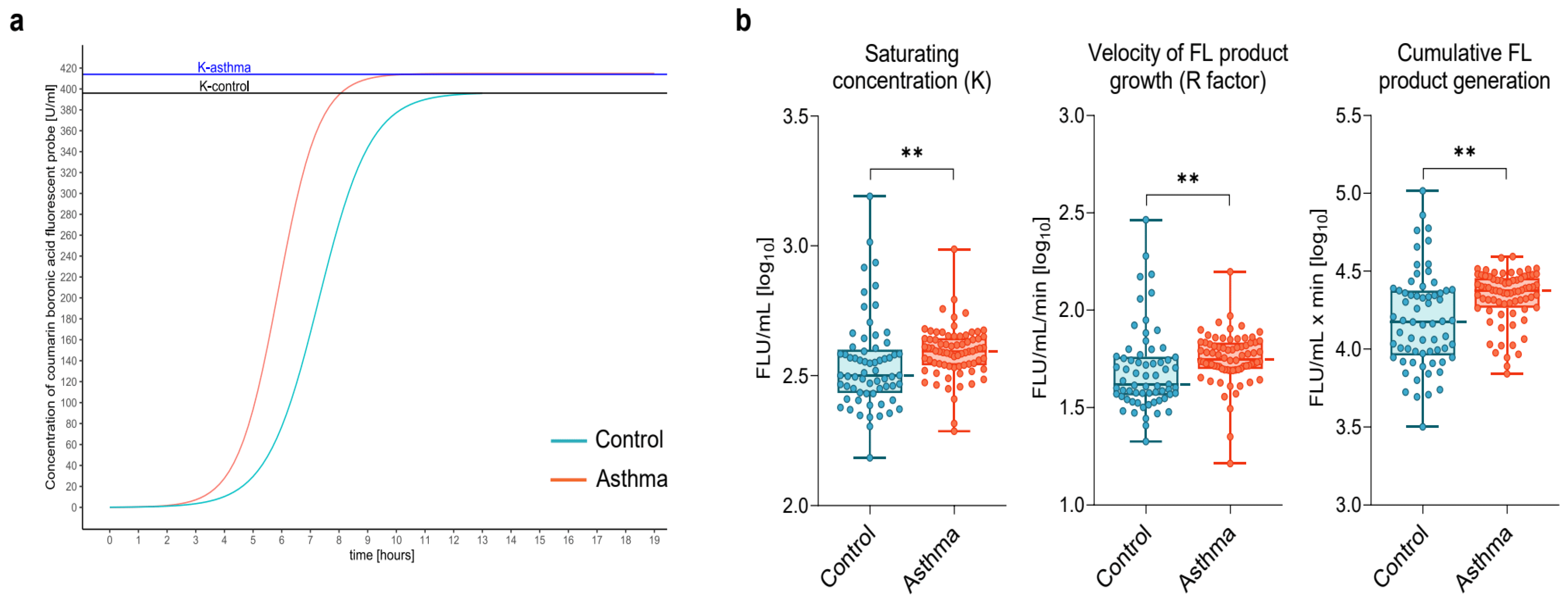
3.3. Increased Systemic Generation of Protein Hydroperoxides in Asthma
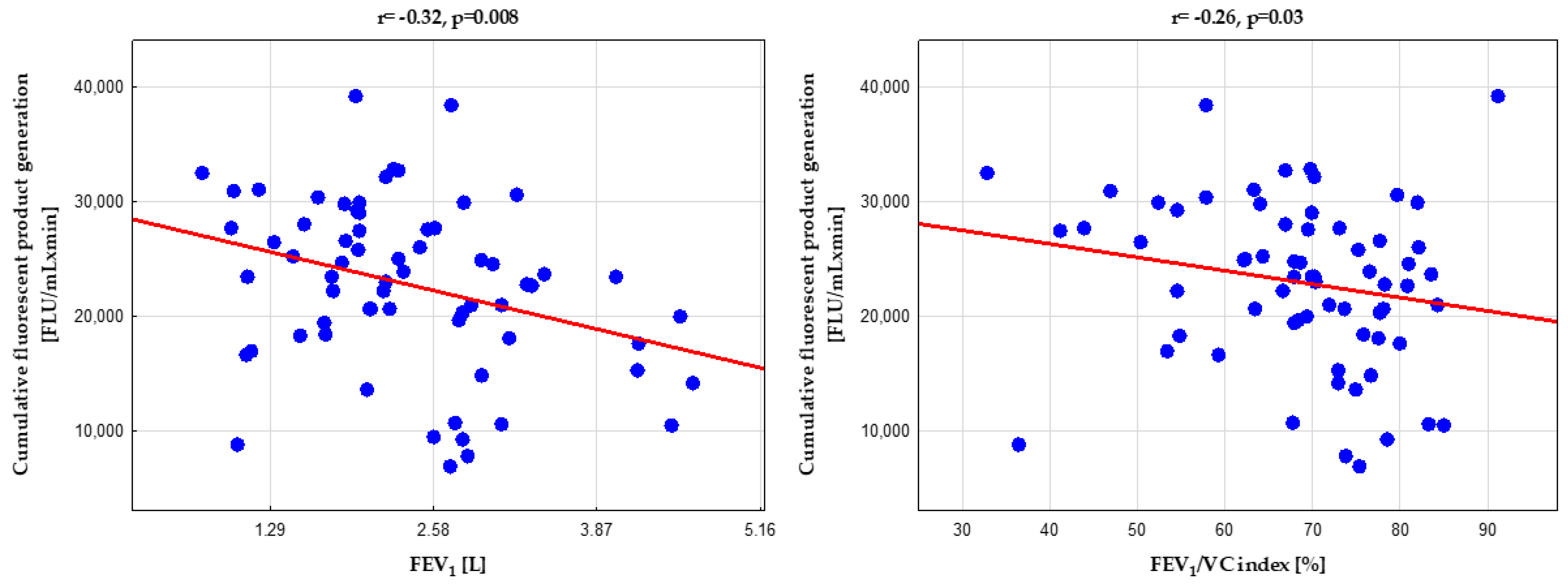
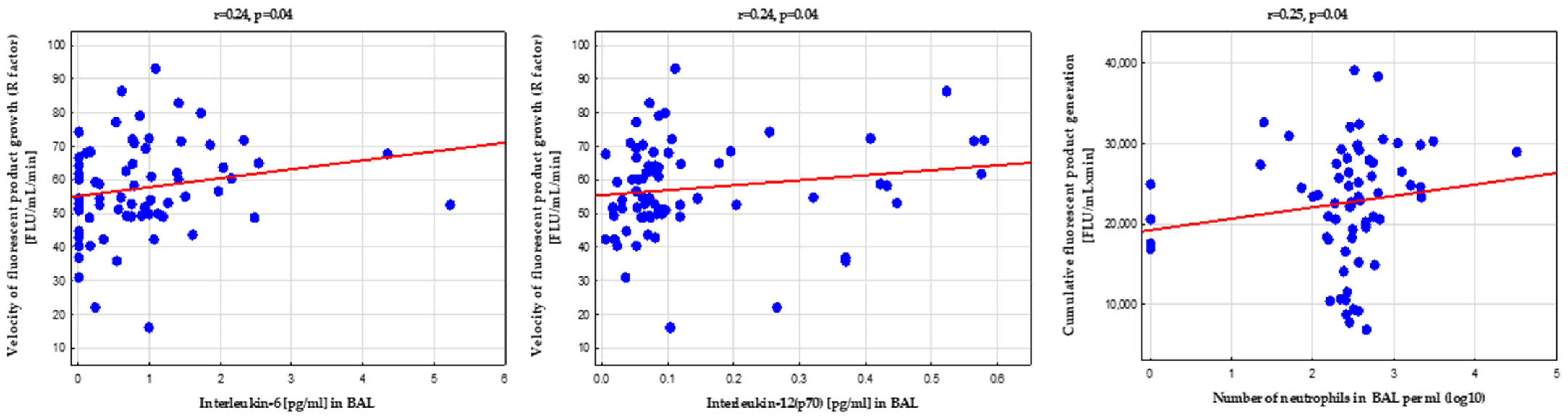
3.4. Systemic Protein Hydroperoxides Generation Was Related to Bronchial Obstruction, Airway Geometry, and Bronchoalveolar Lavage Fluid Biomarkers
3.5. Complex Regulation of Circulating Protein Hydroperoxides Generation by Peripheral Blood Biomarkers
4. Discussion
Study Limitation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global Initiative for Asthma—Global Initiative for Asthma—GINA. Available online: https://ginasthma.org/ (accessed on 26 September 2018).
- Hellings, P.W.; Steelant, B. Epithelial barriers in allergy and asthma. J. Allergy Clin. Immunol. 2020, 145, 1499–1509. [Google Scholar] [CrossRef] [PubMed]
- Nadeem, A.; Siddiqui, N.; Alharbi, N.O.; Alharbi, M.M. Airway and systemic oxidant-antioxidant dysregulation in asthma: A possible scenario of oxidants spill over from lung into blood. Pulm. Pharmacol. Ther. 2014, 29, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Yi, M.; Jin, R.; Feng, X.; Ma, L.; Wang, Y.; Shan, Y.; Yang, Z.; Zhao, B. Correlation between oxidative stress and NF-κB signaling pathway in the obesity-asthma mice. Mol. Biol. Rep. 2020, 47, 3735–3744. [Google Scholar] [CrossRef] [PubMed]
- Kleniewska, P.; Pawliczak, R. The participation of oxidative stress in the pathogenesis of bronchial asthma. Biomed. Pharmacother. 2017, 94, 100–108. [Google Scholar] [CrossRef]
- Morgan, P.E.; Pattison, D.I.; Davies, M.J. Quantification of hydroxyl radical-derived oxidation products in peptides containing glycine, alanine, valine, and proline. Free Radic. Biol. Med. 2012, 52, 328–339. [Google Scholar] [CrossRef]
- Aihua, B.; Yuqing, C.; Zhang, M.; Feng, L.; Xin, Z. Effects of ozone oxidative stress on the airway hyperresponsiveness and mucus production in mice with acute allergic airway inflammation. Zhonghua Jie He He Hu Xi Za Zhi 2015, 38, 179–184. [Google Scholar]
- Casalino-Matsuda, S.M.; Monzón, M.E.; Forteza, R.M. Epidermal Growth Factor Receptor Activation by Epidermal Growth Factor Mediates Oxidant-Induced Goblet Cell Metaplasia in Human Airway Epithelium. Am. J. Respir. Cell Mol. Biol. 2012, 34, 581–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salisbury, D.; Bronas, U. Reactive oxygen and nitrogen species: Impact on endothelial dysfunction. Nurs. Res. 2015, 64, 53–66. [Google Scholar] [CrossRef]
- Larkin, E.K.; Gao, Y.-T.; Gebretsadik, T.; Hartman, T.J.; Wu, P.; Wen, W.; Yang, G.; Bai, C.; Jin, M.; Roberts, L.J., II; et al. New Risk Factors for Adult-Onset Incident Asthma. A Nested Case–Control Study of Host Antioxidant Defense. Am. J. Respir. Crit. Care Med. 2014, 191, 45–53. [Google Scholar] [CrossRef] [Green Version]
- Kuczia, P.; Mastalerz, L.; Potaczek, D.P.; Cybulska, A.; Zareba, L.; Bazan-Socha, S.; Undas, A. Increased activity of lipoprotein-associated phospholipase A2 in non-severe asthma. Allergol. Int. 2019, 68, 450–455. [Google Scholar] [CrossRef]
- Bazan-Socha, S.; Buregwa-Czuma, S.; Jakiela, B.; Zareba, L.; Zawlik, I.; Myszka, A.; Soja, J.; Okon, K.; Zarychta, J.; Kozlik, P.; et al. Reticular Basement Membrane Thickness Is Associated with Growth- and Fibrosis-Promoting Airway Transcriptome Profile-Study in Asthma Patients. Int. J. Mol. Sci. 2021, 22, 998. [Google Scholar] [CrossRef] [PubMed]
- Abboud, M.M.; Al-Rawashde, F.A.; Al-Zayadneh, E.M. Alterations of serum and saliva oxidative markers in patients with bronchial asthma. J. Asthma 2021. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Pacholczak-Madej, R.; Kuszmiersz, P.; Iwaniec, T.; Zaręba, L.; Zarychta, J.; Walocha, J.; Dropiński, J.; Bazan-Socha, S. Endothelial dysfunction and pentraxin-3 in clinically stable adult asthma patients. J. Investig. Allergol. Clin. Immunol. 2021, 31, 417–425. [Google Scholar] [CrossRef]
- Tattersall, M.; Guo, M.; Korcarz, C. Asthma predicts cardiovascular disease events: The multi-ethnic study of atherosclerosis. Arter. Thromb Vasc Biol. 2015, 35, 1520–1525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strand, L.B.; Tsai, M.K.; Wen, C.P.; Chang, S.; Brumpton, B.M. Is having asthma associated with an increased risk of dying from cardiovascular disease? A prospective cohort study of 446 346 Taiwanese adults. BMJ Open 2018, 8, e019992. [Google Scholar] [CrossRef]
- Onufrak, S.J.; Abramson, J.L.; Austin, H.D.; Holguin, F.; McClellan, W.M.; Vaccarino, L.V. Relation of Adult-Onset Asthma to Coronary Heart Disease and Stroke. Am. J. Cardiol. 2008, 101, 1247–1252. [Google Scholar] [CrossRef] [Green Version]
- Nadeem, A.; Chhabra, S.K.; Masood, A.; Raj, H.G. Increased oxidative stress and altered levels of antioxidants in asthma. J. Allergy Clin. Immunol. 2003, 111, 72–78. [Google Scholar] [CrossRef]
- Bou, R.; Codony, R.; Tres, A.; Decker, E.A.; Guardiola, F. Determination of hydroperoxides in foods and biological samples by the ferrous oxidation–xylenol orange method: A review of the factors that influence the method’s performance. Anal. Biochem. 2008, 377, 1–15. [Google Scholar] [CrossRef]
- Gay, C.; Collins, J.; Gebicki, J.M. Hydroperoxide Assay with the Ferric–Xylenol Orange Complex. Anal. Biochem. 1999, 273, 149–155. [Google Scholar] [CrossRef]
- Michalski, R.; Zielonka, J.; Gapys, E.; Marcinek, A.; Joseph, J.; Kalyanaraman, B. Real-time measurements of amino acid and protein hydroperoxides using coumarin boronic acid. J. Biol. Chem. 2014, 289, 22536–22553. [Google Scholar] [CrossRef] [Green Version]
- Culver, B.H.; Graham, B.L.; Coates, A.L.; Wanger, J.; Berry, C.E.; Clarke, P.K.; Hallstrand, T.S.; Hankinson, J.L.; Kaminsky, D.A.; MacIntyre, N.R.; et al. Recommendations for a Standardized Pulmonary Function Report. An Official American Thoracic Society Technical Statement. Am. J. Respir. Crit. Care Med. 2017, 196, 1463–1472. [Google Scholar] [CrossRef] [PubMed]
- Kozlik, P.; Zuk, J.; Bartyzel, S.; Zarychta, J.; Okon, K.; Zareba, L.; Bazan, J.G.; Kosalka, J.; Soja, J.; Musial, J.; et al. The relationship of airway structural changes to blood and bronchoalveolar lavage biomarkers, and lung function abnormalities in asthma. Clin. Exp. Allergy 2020, 50, 15–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sokolowski, J.W.; Burgher, L.W.; Jones, F.L.; Patterson, J.R.; Selecky, P.A. Position Paper on Guidelines for Fiberoptic Bronchoscopy in Adults. Am. Rev. Respir. Dis. 1987, 136, 1066. [Google Scholar] [CrossRef] [PubMed]
- Ferrando, R.E.; Nyengaard, J.R.; Hays, S.R.; Fahy, J.V.; Woodruff, P.G. Applying stereology to measure thickness of the basement membrane zone in bronchial biopsy specimens. J. Allergy Clin. Immunol. 2003, 112, 1243–1245. [Google Scholar] [CrossRef]
- Olchawa, M.M.; Szewczyk, G.M.; Zadlo, A.C.; Krzysztynska-Kuleta, O.I.; Sarna, T.J. The effect of aging and antioxidants on photoreactivity and phototoxicity of human melanosomes: An in vitro study. Pigment. Cell Melanoma Res. 2021, 34, 670–682. [Google Scholar] [CrossRef]
- Bazan-Socha, S.; Jakiela, B.; Zuk, J.; Zarychta, J.; Soja, J.; Okon, K.; Dziedzina, S.; Zareba, L.; Dropinski, J.; Wojcik, K.; et al. Interactions via α 2 β 1 Cell Integrin May Protect against the Progression of Airway Structural Changes in Asthma. Int. J. Mol. Sci. 2021, 22, 6315. [Google Scholar] [CrossRef]
- Kuczia, P.; Zuk, J.; Iwaniec, T.; Soja, J.; Dropinski, J.; Malesa-Wlodzik, M.; Zareba, L.; Bazan, J.G.; Undas, A.; Bazan-Socha, S. Citrullinated histone H3, a marker of extracellular trap formation, is increased in blood of stable asthma patients. Clin. Transl. Allergy 2020, 10, 31. [Google Scholar] [CrossRef]
- Olchawa, M.M.; Krzysztynska-Kuleta, O.I.; Mokrzynski, K.T.; Sarna, P.M.; Sarna, T.J. Quercetin protects ARPE-19 cells against photic stress mediated by the products of rhodopsin photobleaching. Photochem. Photobiol. Sci. 2020, 19, 1022–1034. [Google Scholar] [CrossRef]
- Olchawa, M.; Krzysztynska-Kuleta, O.; Duda, M.; Pawlak, A.; Pabisz, P.; Czuba-Pelech, B.; Sarna, T. In vitro phototoxicity of rhodopsin photobleaching products in the retinal pigment epithelium (RPE). Free Radic. Res. 2019, 53, 456–471. [Google Scholar] [CrossRef]
- Bazan-Socha, S.; Mastalerz, L.; Cybulska, A.; Zareba, L.; Kremers, R.; Zabczyk, M.; Pulka, G.; Iwaniec, T.; Hemker, C.; Undas, A. Prothrombotic State in Asthma Is Related to Increased Levels of Inflammatory Cytokines, IL-6 and TNFα, in Peripheral Blood. Inflammation 2017, 40, 1225–1235. [Google Scholar] [CrossRef]
- Bazan-Socha, S.; Mastalerz, L.; Cybulska, A.; Zareba, L.; Kremers, R.; Zabczyk, M.; Pulka, G.; Iwaniec, T.; Hemker, C.; Undas, A. Asthma is associated with enhanced thrombin formation and impaired fibrinolysis. Clin. Exp. Allergy 2016, 46, 932–944. [Google Scholar] [CrossRef] [PubMed]
- Zelzer, S.; Tatzber, F.; Herrmann, M.; Wonisch, W.; Rinnerhofer, S.; Kundi, M.; Obermayer-Pietsch, B.; Niedrist, T.; Cvirn, G.; Wultsch, G.; et al. Work Intensity, Low-Grade Inflammation, and Oxidative Status: A Comparison between Office and Slaughterhouse Workers. Oxid. Med. Cell. Longev. 2018, 2018, 2737563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.M.; Truong, S.T.; Wong, N.D. Association of adult-onset asthma with specific cardiovascular conditions. Respir. Med. 2012, 106, 948–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tattersall, M.C.; Barnet, J.H.; Korcarz, C.E.; Hagen, E.W.; Peppard, P.E.; Stein, J.H. Late-Onset Asthma Predicts Cardiovascular Disease Events: The Wisconsin Sleep Cohort. J. Am. Heart Assoc. 2016, 5, e003448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricciardolo, F.L.M.; Sprio, A.E.; Baroso, A.; Gallo, F.; Riccardi, E.; Bertolini, F.; Carriero, V.; Arrigo, E.; Ciprandi, G. Characterization of t2-low and t2-high asthma phenotypes in real-life. Biomedicines 2021, 9, 1648. [Google Scholar] [CrossRef]
- Miethe, S.; Guarino, M.; Alhamdan, F.; Simon, H.U.; Renz, H.; Dufour, J.F.; Potaczek, D.P.; Garn, H. Effects of obesity on asthma: Immunometabolic links. Polish Arch. Intern. Med. 2018, 128, 469–477. [Google Scholar] [CrossRef] [Green Version]
- Payne, D.N.R.; Rogers, A.V.; Ädelroth, E.; Bandi, V.; Guntupalli, K.K.; Bush, A.; Jeffery, P.K. Early thickening of the reticular basement membrane in children with difficult asthma. Am. J. Respir. Crit. Care Med. 2003, 167, 78–82. [Google Scholar] [CrossRef]
- Mohanty, J.G.; Nagababu, E.; Rifkind, J.M. Red blood cell oxidative stress impairs oxygen delivery and induces red blood cell aging. Front. Physiol. 2014, 5, 84. [Google Scholar] [CrossRef] [Green Version]
- Dozor, A.J. The role of oxidative stress in the pathogenesis and treatment of asthma. Ann. N. Y. Acad. Sci. 2010, 1203, 133–137. [Google Scholar] [CrossRef]
- Troisi, R.J.; Willett, W.C.; Weiss, S.T.; Trichopoulos, D.; Rosner, B.; Speizer, F.E. A prospective study of diet and adult-onset asthma. Am. J. Respir. Crit. Care Med. 2012, 151, 1401–1408. [Google Scholar] [CrossRef]
- Varraso, R.; Kauffmann, F.; Leynaert, B.; Le Moual, N.; Boutron-Ruault, M.C.; Clavel-Chapelon, F.; Romieu, I. Dietary patterns and asthma in the E3N study. Eur. Respir. J. 2009, 33, 33–41. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Patients n = 74 | Controls n = 65 | p-Value |
|---|---|---|---|
| Age, years | 53.5 ± 13.1 | 51.4 ± 12.3 | 0.63 |
| Male gender, n(%) | 19 (26) | 23 (35) | 0.22 |
| Body mass index, kg/m2 | 26.9 ± 4.6 | 25.9 ± 3.4 | 0.1 |
| Past smoking, n(%) | 13 (18) | 15 (23) | 0.3 |
| Pack-years of smoking, n | 0 (0–0) | 0 (0–0) | 0.59 |
| Living primarily in inner-city environments, n(%) | 39 (53) | 38 (58) | 0.57 |
| Internal medicine comorbidities | |||
| Hypertension, n(%) | 34 (46) | 25 (38) | 0.67 |
| Diabetes mellitus, n(%) | 11 (15) | 8 (12) | 0.68 |
| Hypercholesterolemia, n(%) | 21 (28) | 15 (23) | 0.52 |
| Asthma duration, years | 10 (5–20) |
| Atopy, n(%) | 39 (53%) |
| Severe asthma, n(%) | 29 (39%) |
| Asthma severity (GINA) | |
| Mild, n(%) | 18 (24%) |
| Moderate, n(%) | 27 (36%) |
| Severe, n(%) | 29 (39%) |
| Asthma symptom control § | |
| Well-controlled asthma, n(%) | 22 (30%) |
| Not-well controlled asthma, n(%) | 33 (44%) |
| Very-poorly controlled asthma, n(%) | 19 (26%) |
| Spirometry values | |
| FEV1 before bronchodilator, % of the predicted value | 81.8 (66.6–99.4) |
| FEV1 after bronchodilator, % of the predicted value | 91.9 (73.2–104.1) |
| VC before bronchodilator, L | 3.2 (2.6–3.97) |
| VC after bronchodilator, L | 3.36 (2.7–4) |
| FEV1/VC (before bronchodilator) | 65.8 (57.4–72.6) |
| FEV1/VC (after bronchodilator) | 69.9 (63.2–77.5) |
| Computed tomography airway remodeling indices | |
| The right upper lobe apical segmental bronchus (RB1) | |
| Lumen area, mm2 | 12.5 (10–16) |
| Wall area, mm2 | 34.8 (27.9–45.4) |
| Wall thickness, mm | 1.9 (1.7–2.1) |
| Wall thickness ratio (WTR) | 24.1 ± 2.7 |
| Wall area ratio (WAR) | 73.2 ± 5.6 |
| The right lower lobe basal posterior bronchus (RB10) | |
| Lumen area, mm2 | 12.5 (9–18) |
| Wall area, mm2 | 35.1 ± 12.3 |
| Wall thickness, mm | 1.8 (1.6–2.1) |
| Wall thickness ratio (WTR) | 23.6 (22–25.9) |
| Wall area ratio (WAR) | 72.3 (68.5–76.9) |
| Bronchial biopsy histology | |
| Reticular basement membrane (RBM) thickness, μm ¥ | 6.49 (5.3–7.86) |
| Collagen I staining, % of the stroma showing reactivity | 30 (20–60) |
| Bronchoalveolar lavage fluid (BAL) cellularity # | |
| Macrophages, % | 85 (72–93) |
| Lymphocytes, % | 8 (4–15) |
| Neutrophils, % | 3 (2–5) |
| Eosinophils, % | 1 (0.1–2) |
| Eosinophils ≥2% in BAL, n(%) | 17 (37.5%) |
| Neutrophils ≥4% in BAL, n(%) | 29 (43.3%) |
| Bronchoalveolar lavage fluid biomarkers † | |
| Periostin, ng/mL | 0.85 (0.75–0.97) |
| Interleukin-6, pg/mL | 0.75 (0.1–1.19) |
| Interleukin-12(p70), pg/mL | 0.078 (0.05–0.12) |
| Asthma therapy | |
| Oral corticosteroids | 14 (19%) |
| Inhaled corticosteroids (persistent use) | 68 (92%) |
| Long-acting β2-agonists (persistent use) | 54 (73%) |
| Antileukotrienes | 10 (14%) |
| Theophylline | 8 (11%) |
| Long-acting anticholinergics (persistent use) | 5 (7%) |
| Fluorescent Product Growth Velocity (R Factor) | ||
|---|---|---|
| β (95% CI) | R2 | |
| FEV1, % | −0.18 (−0.31 to −0.04) | 0.16 |
| Wall thickness ratio (WTR), RB1 | 0.22 (0.08 to 0.36) | |
| Interleukin 6, BAL, pg/mL | 0.28 (0.14 to 0.41) | |
| Adjustment statistics | F = 2.9, p < 0.001 | |
| Patients n = 74 | Controls n = 65 | p-Value | |
|---|---|---|---|
| Basic laboratory tests | |||
| Hemoglobin, g/dL | 13.5 (13–14.4) | 13.9 ± 1.28 | 0.09 |
| Red blood cell count, 106/μL | 4.61 ± 0.43 | 4.6 ± 0.38 | 0.83 |
| White blood cell count, 103/μL | 6.68 (5.6–7.96) | 5.48 (4.82–6.64) | <0.001 ** |
| Eosinophils, 103/μL | 275 (135–470) | 15 (9–80) | <0.001 ** |
| Monocytes, 103/μL | 600 (485–815) | 480 (430–670) | <0.001 ** |
| Blood platelets, 103/μL | 218 (191–247) | 232 (203–293) | 0.01 * |
| C-reactive protein, mg/L | 2.55 (0.58–8.67) | 1 (0.9–1.7) | 0.04 * |
| Immunoglobulin E, IU/mL | 71.5 (29.4–380) | 22.6 (18.5–53.5) | 0.001 * |
| Glucose, mmol/L | 5 (4.65–5.55) | 5.17 ± 0.54 | 0.63 |
| Total cholesterol, mmol/L | 4.83 ± 0.98 | 4.8 (4.25–5.35) | 0.74 |
| Low-density lipoprotein cholesterol, mmol/L | 2.61 ± 0.76 | 3.38 ± 0.96 | <0.001 ** |
| High-density lipoprotein cholesterol, mmol/L | 1.34 (1.09–1.61) | 1.58 ± 0.41 | 0.01 * |
| Triglycerides, mmol/L | 1.4 (1–2) | 1.09 (0.82–1.42) | <0.001 ** |
| Biomarkers in serum § | |||
| Interleukin-6, pg/mL | 0.78 (0.45–2.09) | 0.73 ± 0.52 | 0.31 |
| Interleukin-10, pg/mL | 0.57 (0.25–0.97) | 0.005 (0.005–0.01) | <0.001 ** |
| Interleukin-12(p70), pg/mL | 0.005 (0.005–1.3) | 0.005 (0.005–1.69) | 0.75 |
| Interleukin-17A, pg/mL | 0.005 (0.005–0.12) | 0.005 (0.005–0.06) | 0.87 |
| Interferon-γ, pg/mL | 0.005 (0.005–0.28) | 0.11 (0.005–0.27) | 0.66 |
| Citrullinated histone H3, ng/mL | 16.3 (10.7–19.8) | 12.8 (8.2–17.6) | 0.04 * |
| Fluorescent Product Growth Velocity (R Factor) | ||
|---|---|---|
| β (95% CI) | R2 | |
| Monocyte count, 103/μL | 0.14 (0.02 to 0.28) | 0.33 |
| Red blood cell count, 106/μL | −0.58 (−0.73 to −0.43) | |
| Blood eosinophilia, 103/μL | −0.23 (−0.41 to −0.06) | |
| Citrulinated histone 3, ng/mL | 0.22 (0.07 to 0.37) | |
| Interleukin 17A, pg/mL | 0.26 (0.13 to 0.4) | |
| Total cholesterol, mmol/L | 0.22 (0.08 to 0.37) | |
| Adjustment statistics | F = 3.3, p = 0.01 | |
| Fluorescent Product Growth Velocity (R Factor) | ||
|---|---|---|
| β (95% CI) | R2 | |
| FEV1, % | −0.21 (−0.34 to −0.07) | 0.26 |
| Red blood cell count, 106/μL | −0.26 (−0.39 to −0.12) | |
| Citrulinated histone 3, ng/mL | 0.35 (0.23 to 0.47) | |
| Interleukin 6, BAL, pg/mL | 0.19 (0.08 to 0.31) | |
| Adjustment statistics | F = 5.04, p = 0.002 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bazan-Socha, S.; Wójcik, K.; Olchawa, M.; Sarna, T.; Pięta, J.; Jakieła, B.; Soja, J.; Okoń, K.; Zarychta, J.; Zaręba, L.; et al. Increased Oxidative Stress in Asthma—Relation to Inflammatory Blood and Lung Biomarkers and Airway Remodeling Indices. Biomedicines 2022, 10, 1499. https://doi.org/10.3390/biomedicines10071499
Bazan-Socha S, Wójcik K, Olchawa M, Sarna T, Pięta J, Jakieła B, Soja J, Okoń K, Zarychta J, Zaręba L, et al. Increased Oxidative Stress in Asthma—Relation to Inflammatory Blood and Lung Biomarkers and Airway Remodeling Indices. Biomedicines. 2022; 10(7):1499. https://doi.org/10.3390/biomedicines10071499
Chicago/Turabian StyleBazan-Socha, Stanisława, Krzysztof Wójcik, Magdalena Olchawa, Tadeusz Sarna, Jakub Pięta, Bogdan Jakieła, Jerzy Soja, Krzysztof Okoń, Jacek Zarychta, Lech Zaręba, and et al. 2022. "Increased Oxidative Stress in Asthma—Relation to Inflammatory Blood and Lung Biomarkers and Airway Remodeling Indices" Biomedicines 10, no. 7: 1499. https://doi.org/10.3390/biomedicines10071499