
Frailty in Aging and the Search for the Optimal Biomarker: A Review

 , , ,
, , , 
Abstract
:1. Introduction
2. Methodology
3. Diagnosis of Frailty: Main Diagnostic Tools and Their Deficiencies
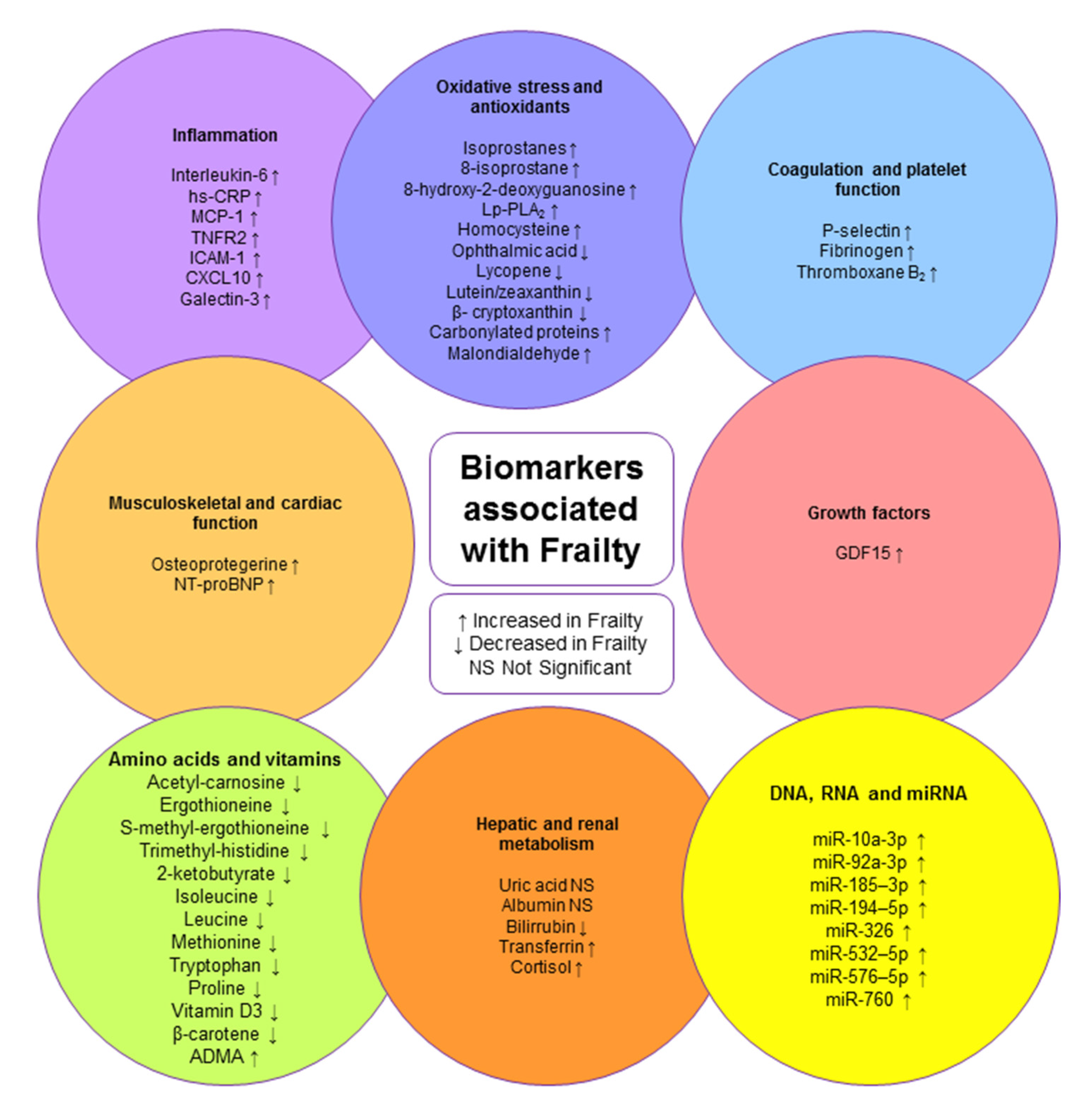
4. Blood Biomarkers Associated with Frailty
4.1. Biomarkers Associated with Inflammation
4.2. Biomarkers Associated with Oxidative Stress and Antioxidants
4.3. Biomarkers Associated with Coagulation and Platelet Function
4.4. Biomarkers Associated with Growth Factors
4.5. Biomarkers Associated with Musculoskeletal and Cardiac Function
4.6. Biomarkers Associated with Amino Acids and Vitamins
4.7. Biomarkers Associated with Hepatic and Renal Metabolism
4.8. Biomarkers Associated with DNA, RNA, and miRNA
5. Outlook and Future Directions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Patel, R.; Khan, I.; Pennington, M.; Pitts, N.B.; Robertson, C.; Gallagher, J.E. Protocol for A randomised feasibility trial comparing fluoride interventions to prevent dental decay in older people in care homes (FInCH trial). BMC Oral Health 2021, 21, 302. [Google Scholar] [CrossRef] [PubMed]
- Thumala, D.; Kennedy, B.K.; Calvo, E.; Gonzalez-Billault, C.; Zitko, P.; Lillo, P.; Villagra, R.; Ibáñez, A.; Assar, R.; Andrade, M.; et al. Aging and Health Policies in Chile: New Agendas for Research. Health Syst. Reform 2017, 3, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Michel, J.-P.; Sadana, R. “Healthy aging” concepts and measures. J. Am. Med. Dir. Assoc. 2017, 18, 460–464. [Google Scholar] [CrossRef] [PubMed]
- Veronese, N. Frailty as Cardiovascular Risk Factor (and Vice Versa). Adv. Exp. Med. Biol. 2020, 1216, 51–54. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Clinical Consortium on Healthy Ageing: Topic Focus: Frailty and Intrinsic Capacity: Report of Consortium Meeting, 1–2 December 2016 in Geneva, Switzerland; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Kojima, G. Frailty Defined by FRAIL Scale as a Predictor of Mortality: A Systematic Review and Meta-analysis. J. Am. Med. Dir. Assoc. 2018, 19, 480–483. [Google Scholar] [CrossRef]
- Kojima, G. Frailty as a Predictor of Future Falls Among Community-Dwelling Older People: A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2015, 16, 1027–1033. [Google Scholar] [CrossRef]
- Kojima, G. Frailty as a predictor of fractures among community-dwelling older people: A systematic review and meta-analysis. Bone 2016, 90, 116–122. [Google Scholar] [CrossRef]
- Kojima, G.; Taniguchi, Y.; Iliffe, S.; Walters, K. Frailty as a Predictor of Alzheimer Disease, Vascular Dementia, and All Dementia Among Community-Dwelling Older People: A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2016, 17, 881–888. [Google Scholar] [CrossRef]
- Kojima, G. Frailty as a predictor of disabilities among community-dwelling older people: A systematic review and meta-analysis. Disabil. Rehabil. 2017, 39, 1897–1908. [Google Scholar] [CrossRef]
- Kojima, G.; Iliffe, S.; Jivraj, S.; Walters, K. Association between frailty and quality of life among community-dwelling older people: A systematic review and meta-analysis. J. Epidemiol. Community Health 2016, 70, 716–721. [Google Scholar] [CrossRef]
- García-Nogueras, I.; Aranda-Reneo, I.; Peña-Longobardo, L.M.; Oliva-Moreno, J.; Abizanda, P. Use of Health Resources and Healthcare Costs associated with Frailty: The FRADEA Study. J. Nutr. Health Aging 2017, 21, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Gobbens, R.J.; Luijkx, K.G.; Wijnen-Sponselee, M.T.; Schols, J.M. Toward a conceptual definition of frail community dwelling older people. Nurs. Outlook 2010, 58, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Lee, E.; Jang, I.Y. Frailty and Comprehensive Geriatric Assessment. J. Korean Med. Sci. 2020, 35, e16. [Google Scholar] [CrossRef] [PubMed]
- Briggs, A.M.; Araujo de Carvalho, I. Actions required to implement integrated care for older people in the community using the World Health Organization’s ICOPE approach: A global Delphi consensus study. PLoS ONE 2018, 13, e0205533. [Google Scholar] [CrossRef] [PubMed]
- Won, C.W.; Ha, E.; Jeong, E.; Kim, M.; Park, J.; Baek, J.E.; Kim, S.; Kim, S.B.; Roh, J.; Choi, J.H.; et al. World Health Organization Integrated Care for Older People (ICOPE) and the Integrated Care of Older Patients with Frailty in Primary Care (ICOOP_Frail) Study in Korea. Ann. Geriatr. Med. Res. 2021, 25, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Rudnicka, E.; Napierała, P.; Podfigurna, A.; Męczekalski, B.; Smolarczyk, R.; Grymowicz, M. The World Health Organization (WHO) approach to healthy ageing. Maturitas 2020, 139, 6–11. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G. Frailty in older adults evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Mitnitski, A.B.; Mogilner, A.J.; Rockwood, K. Accumulation of deficits as a proxy measure of aging. Sci. World J. 2001, 1, 323–336. [Google Scholar] [CrossRef] [Green Version]
- Aygör, H.E.; Fadıloğlu, Ç.; Şahin, S.; Aykar, F.Ş.; Akçiçek, F. Validation of edmonton frail scale into elderly turkish population. Arch. Gerontol. Geriatr. 2018, 76, 133–137. [Google Scholar] [CrossRef]
- García-García, F.J.; Carcaillon, L.; Fernandez-Tresguerres, J.; Alfaro, A.; Larrion, J.L.; Castillo, C.; Rodriguez-Mañas, L. A New Operational Definition of Frailty: The Frailty Trait Scale. J. Am. Med. Dir. Assoc. 2014, 15, 371.e7–371.e13. [Google Scholar] [CrossRef]
- Navarro-Flores, E.; de Bengoa Vallejo, R.B.; Losa-Iglesias, M.E.; Palomo-López, P.; Calvo-Lobo, C.; López-López, D.; Martínez-Jiménez, E.M.; Romero-Morales, C. The reliability, validity, and sensitivity of the Edmonton Frail Scale (EFS) in older adults with foot disorders. Aging 2020, 12, 24623–24632. [Google Scholar] [CrossRef] [PubMed]
- Zupo, R.; Castellana, F.; Donghia, R.; Lampignano, L.; Guerra, V.; De Pergola, G.; Lozupone, M.; Bortone, I.; De Nucci, S.; Tatoli, R.; et al. Liver frailty and all-cause mortality in the older participants of the Salus in Apulia Study. GeroScience 2022, 44, 835–845. [Google Scholar] [CrossRef] [PubMed]
- Zupo, R.; Castellana, F.; Bortone, I.; Griseta, C.; Sardone, R.; Lampignano, L.; Lozupone, M.; Solfrizzi, V.; Castellana, M.; Giannelli, G.; et al. Nutritional domains in frailty tools: Working towards an operational definition of nutritional frailty. Ageing Res. Rev. 2020, 64, 101148. [Google Scholar] [CrossRef] [PubMed]
- Dibello, V.; Zupo, R.; Sardone, R.; Lozupone, M.; Castellana, F.; Dibello, A.; Daniele, A.; De Pergola, G.; Bortone, I.; Lampignano, L.; et al. Oral frailty and its determinants in older age: A systematic review. Lancet Healthy Longev. 2021, 2, e507–e520. [Google Scholar] [CrossRef]
- Vatic, M.; von Haehling, S.; Ebner, N. Inflammatory biomarkers of frailty. Exp. Gerontol. 2020, 133, 110858. [Google Scholar] [CrossRef]
- Saedi, A.A.; Feehan, J.; Phu, S.; Duque, G. Current and emerging biomarkers of frailty in the elderly. Clin. Interv. Aging 2019, 14, 389–398. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.; Liu, Z.; Wang, Y.; Wang, Z.; Shi, J.; Xie, X.; Jin, L.; Chu, X.; Wang, X. C-reactive protein, frailty and overnight hospital admission in elderly individuals: A population-based study. Arch. Gerontol. Geriatr. 2016, 64, 1–5. [Google Scholar] [CrossRef]
- Kochlik, B.; Stuetz, W.; Pérès, K.; Pilleron, S.; Féart, C.; García García, F.J.; Bandinelli, S.; Gomez-Cabrero, D.; Rodriguez-Mañas, L.; Grune, T.; et al. Associations of fat-soluble micronutrients and redox biomarkers with frailty status in the FRAILOMIC initiative. J. Cachexia Sarcopenia Muscle 2019, 10, 1339–1346. [Google Scholar] [CrossRef] [Green Version]
- Buta, B.J.; Walston, J.D.; Godino, J.G.; Park, M.; Kalyani, R.R.; Xue, Q.L.; Bandeen-Roche, K.; Varadhan, R. Frailty assessment instruments: Systematic characterization of the uses and contexts of highly-cited instruments. Ageing Res. Rev. 2016, 26, 53–61. [Google Scholar] [CrossRef] [Green Version]
- Aubertin-Leheudre, M.; Woods, A.J.; Anton, S.; Cohen, R.; Pahor, M. Frailty Clinical Phenotype: A Physical and Cognitive Point of View. Nestle Nutr. Inst. Workshop Ser. 2015, 83, 55–63. [Google Scholar] [CrossRef] [Green Version]
- Abete, P.; Basile, C.; Bulli, G.; Curcio, F.; Liguori, I.; Della-Morte, D.; Gargiulo, G.; Langellotto, A.; Testa, G.; Galizia, G.; et al. The Italian version of the “frailty index” based on deficits in health: A validation study. Aging Clin. Exp. Res. 2017, 29, 913–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afilalo, J. The Clinical Frailty Scale. Circulation 2017, 135, 2025–2027. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Ariño, M.; Torrente Jiménez, I.; Cartanyà Gutiérrez, A.; Oliva Morera, J.C.; Comet, R. Assessing the strengths and weaknesses of the Clinical Frailty Scale through correlation with a frailty index. Aging Clin. Exp. Res. 2020, 32, 2225–2232. [Google Scholar] [CrossRef] [PubMed]
- Abellan van Kan, G.; Rolland, Y.; Houles, M.; Gillette-Guyonnet, S.; Soto, M.; Vellas, B. The assessment of frailty in older adults. Clin. Geriatr. Med. 2010, 26, 275–286. [Google Scholar] [CrossRef]
- Perna, S.; Francis, M.D.A.; Bologna, C.; Moncaglieri, F.; Riva, A.; Morazzoni, P.; Allegrini, P.; Isu, A.; Vigo, B.; Guerriero, F.; et al. Performance of Edmonton Frail Scale on frailty assessment: Its association with multi-dimensional geriatric conditions assessed with specific screening tools. BMC Geriatr. 2017, 17, 2. [Google Scholar] [CrossRef] [Green Version]
- He, Y.; Li, L.W.; Hao, Y.; Sim, E.Y.; Ng, K.L.; Lee, R.; Lim, M.S.; Poopalalingam, R.; Abdullah, H.R. Assessment of predictive validity and feasibility of Edmonton Frail Scale in identifying postoperative complications among elderly patients: A prospective observational study. Sci. Rep. 2020, 10, 14682. [Google Scholar] [CrossRef]
- Rolfson, D.B.; Majumdar, S.R.; Tsuyuki, R.T.; Tahir, A.; Rockwood, K. Validity and reliability of the Edmonton Frail Scale. Age Ageing 2006, 35, 526–529. [Google Scholar] [CrossRef] [Green Version]
- Erusalimsky, J.D.; Grillari, J.; Grune, T.; Jansen-Duerr, P.; Lippi, G.; Sinclair, A.J.; Tegnér, J.; Viña, J.; Durrance-Bagale, A.; Miñambres, R.; et al. In Search of ‘Omics’-Based Biomarkers to Predict Risk of Frailty and Its Consequences in Older Individuals: The FRAILOMIC Initiative. Gerontology 2016, 62, 182–190. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J. The frailty syndrome. Clin. Med. 2011, 11, 72–75. [Google Scholar] [CrossRef]
- Strandberg, T.E.; Pitkälä, K.H. Frailty in elderly people. Lancet 2007, 369, 1328–1329. [Google Scholar] [CrossRef]
- Picca, A.; Coelho-Junior, H.J.; Calvani, R.; Marzetti, E.; Vetrano, D.L. Biomarkers shared by frailty and sarcopenia in older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2022, 73, 101530. [Google Scholar] [CrossRef] [PubMed]
- Atienza, M.; Ziontz, J.; Cantero, J.L. Low-grade inflammation in the relationship between sleep disruption, dysfunctional adiposity, and cognitive decline in aging. Sleep Med. Rev. 2018, 42, 171–183. [Google Scholar] [CrossRef] [PubMed]
- Castro-Herrera, V.M.; Lown, M.; Fisk, H.L.; Owen-Jones, E.; Lau, M.; Lowe, R.; Hood, K.; Gillespie, D.; Hobbs, F.D.R.; Little, P.; et al. Relationships Between Age, Frailty, Length of Care Home Residence and Biomarkers of Immunity and Inflammation in Older Care Home Residents in the United Kingdom. Front. Aging 2021, 2, 599084. [Google Scholar] [CrossRef]
- Calder, P.C.; Bosco, N.; Bourdet-Sicard, R.; Capuron, L.; Delzenne, N.; Doré, J.; Franceschi, C.; Lehtinen, M.J.; Recker, T.; Salvioli, S.; et al. Health relevance of the modification of low grade inflammation in ageing (inflammageing) and the role of nutrition. Ageing Res. Rev. 2017, 40, 95–119. [Google Scholar] [CrossRef] [PubMed]
- Ventura, M.T.; Casciaro, M.; Gangemi, S.; Buquicchio, R. Immunosenescence in aging: Between immune cells depletion and cytokines up-regulation. Clin. Mol. Allergy CMA 2017, 15, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, Y.; Zheng, S.G. Hall of Fame among Pro-inflammatory Cytokines: Interleukin-6 Gene and Its Transcriptional Regulation Mechanisms. Front. Immunol. 2016, 7, 604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, T.; Narazaki, M.; Kishimoto, T. IL-6 in Inflammation, Immunity, and Disease. Cold Spring Harb. Perspect. Biol. 2014, 6, a016295. [Google Scholar] [CrossRef]
- Rønning, B.; Wyller, T.B.; Seljeflot, I.; Jordhøy, M.S.; Skovlund, E.; Nesbakken, A.; Kristjansson, S.R. Frailty measures, inflammatory biomarkers and post-operative complications in older surgical patients. Age Ageing 2010, 39, 758–761. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.K.; Lyass, A.; Larson, M.G.; Massaro, J.M.; Wang, N.; D’Agostino, R.B., Sr.; Benjamin, E.J.; Murabito, J.M. Biomarkers of oxidative stress are associated with frailty: The Framingham Offspring Study. Age 2016, 38, 1. [Google Scholar] [CrossRef] [Green Version]
- Netea, M.G.; Balkwill, F.; Chonchol, M.; Cominelli, F.; Donath, M.Y.; Giamarellos-Bourboulis, E.J.; Golenbock, D.; Gresnigt, M.S.; Heneka, M.T.; Hoffman, H.M.; et al. A guiding map for inflammation. Nat. Immunol. 2017, 18, 826–831. [Google Scholar] [CrossRef] [Green Version]
- Musunuru, K.; Kral, B.G.; Blumenthal, R.S.; Fuster, V.; Campbell, C.Y.; Gluckman, T.J.; Lange, R.A.; Topol, E.J.; Willerson, J.T.; Desai, M.Y.; et al. The use of high-sensitivity assays for C-reactive protein in clinical practice. Nat. Clin. Pract. Cardiovasc. Med. 2008, 5, 621–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gale, C.R.; Baylis, D.; Cooper, C.; Sayer, A.A. Inflammatory markers and incident frailty in men and women: The English Longitudinal Study of Ageing. AGE 2013, 35, 2493–2501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puts, M.T.E.; Visser, M.; Twisk, J.W.R.; Deeg, D.J.H.; Lips, P. Endocrine and inflammatory markers as predictors of frailty. Clin. Endocrinol. 2005, 63, 403–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walston, J.; McBurnie, M.A.; Newman, A.; Tracy, R.P.; Kop, W.J.; Hirsch, C.H.; Gottdiener, J.; Fried, L.P.; Investigators, f.t.C.H.S. Frailty and Activation of the Inflammation and Coagulation Systems With and Without Clinical Comorbidities: Results From the Cardiovascular Health Study. Arch. Intern. Med. 2002, 162, 2333–2341. [Google Scholar] [CrossRef] [PubMed]
- Cranford, T.L.; Enos, R.T.; Velázquez, K.T.; McClellan, J.L.; Davis, J.M.; Singh, U.P.; Nagarkatti, M.; Nagarkatti, P.S.; Robinson, C.M.; Murphy, E.A. Role of MCP-1 on inflammatory processes and metabolic dysfunction following high-fat feedings in the FVB/N strain. Int. J. Obes. 2016, 40, 844–851. [Google Scholar] [CrossRef] [Green Version]
- Yadav, A.; Saini, V.; Arora, S. MCP-1: Chemoattractant with a role beyond immunity: A review. Clin. Chim. Acta 2010, 411, 1570–1579. [Google Scholar] [CrossRef]
- Nan, J.; Hu, H.; Sun, Y.; Zhu, L.; Wang, Y.; Zhong, Z.; Zhao, J.; Zhang, N.; Wang, Y.; Wang, Y.; et al. TNFR2 Stimulation Promotes Mitochondrial Fusion via Stat3- and NF-kB–Dependent Activation of OPA1 Expression. Circ. Res. 2017, 121, 392–410. [Google Scholar] [CrossRef]
- Kastl, L.; Sauer, S.W.; Ruppert, T.; Beissbarth, T.; Becker, M.S.; Süss, D.; Krammer, P.H.; Gülow, K. TNF-α mediates mitochondrial uncoupling and enhances ROS-dependent cell migration via NF-κB activation in liver cells. FEBS Lett. 2014, 588, 175–183. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Oppenheim, J.J. Targeting TNFR2, an immune checkpoint stimulator and oncoprotein, is a promising treatment for cancer. Sci. Signal. 2017, 10, eaal2328. [Google Scholar] [CrossRef]
- Lawson, C.; Wolf, S. ICAM-1 signaling in endothelial cells. Pharmacol. Rep. 2009, 61, 22–32. [Google Scholar] [CrossRef]
- Liu, M.; Guo, S.; Hibbert, J.M.; Jain, V.; Singh, N.; Wilson, N.O.; Stiles, J.K. CXCL10/IP-10 in infectious diseases pathogenesis and potential therapeutic implications. Cytokine Growth Factor Rev. 2011, 22, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.Y.; Lee, Z.-H.; Song, Y.W. CXCL10 and autoimmune diseases. Autoimmun. Rev. 2009, 8, 379–383. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Kim, T.; Pang, J.; Sun, W.; Yang, X.; Wang, J.; Song, Y.; Zhang, H.; Sun, H.; Rangan, V.; et al. A novel function of CXCL10 in mediating monocyte production of proinflammatory cytokines. J. Leukoc. Biol. 2017, 102, 1271–1280. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Guo, S.; Stiles, J.K. The emerging role of CXCL10 in cancer (Review). Oncol. Lett. 2011, 2, 583–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qu, T.; Yang, H.; Walston, J.D.; Fedarko, N.S.; Leng, S.X. Upregulated monocytic expression of CXC chemokine ligand 10 (CXCL-10) and its relationship with serum interleukin-6 levels in the syndrome of frailty. Cytokine 2009, 46, 319–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simovic Markovic, B.; Nikolic, A.; Gazdic, M.; Bojic, S.; Vucicevic, L.; Kosic, M.; Mitrovic, S.; Milosavljevic, M.; Besra, G.; Trajkovic, V.; et al. Galectin-3 Plays an Important Pro-inflammatory Role in the Induction Phase of Acute Colitis by Promoting Activation of NLRP3 Inflammasome and Production of IL-1β in Macrophages. J. Crohn’s Colitis 2016, 10, 593–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, R.; Zhang, M.; Hu, Q.; Zheng, S.; Soh, A.; Zheng, Y.; Yuan, H. Galectin-3 as a novel biomarker for disease diagnosis and a target for therapy (Review). Int. J. Mol. Med. 2018, 41, 599–614. [Google Scholar] [CrossRef] [Green Version]
- Lok, D.J.A.; Van Der Meer, P.; de la Porte, P.W.B.-A.; Lipsic, E.; Van Wijngaarden, J.; Hillege, H.L.; van Veldhuisen, D.J. Prognostic value of galectin-3, a novel marker of fibrosis, in patients with chronic heart failure: Data from the DEAL-HF study. Clin. Res. Cardiol. 2010, 99, 323–328. [Google Scholar] [CrossRef] [Green Version]
- Sharma, U.C.; Pokharel, S.; Brakel, T.J.v.; Berlo, J.H.v.; Cleutjens, J.P.M.; Schroen, B.; André, S.; Crijns, H.J.G.M.; Gabius, H.-J.; Maessen, J.; et al. Galectin-3 Marks Activated Macrophages in Failure-Prone Hypertrophied Hearts and Contributes to Cardiac Dysfunction. Circulation 2004, 110, 3121–3128. [Google Scholar] [CrossRef]
- Komici, K.; Gnemmi, I.; Bencivenga, L.; Vitale, D.F.; Rengo, G.; Di Stefano, A.; Eleuteri, E. Impact of Galectin-3 Circulating Levels on Frailty in Elderly Patients with Systolic Heart Failure. J. Clin. Med. 2020, 9, 2229. [Google Scholar] [CrossRef]
- Chandrasekaran, A.; Idelchik, M.; Melendez, J.A. Redox control of senescence and age-related disease. Redox Biol. 2017, 11, 91–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powers, S.K.; Ji, L.L.; Kavazis, A.N.; Jackson, M.J. Reactive oxygen species: Impact on skeletal muscle. Compr. Physiol. 2011, 1, 941–969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milne, G.L.; Yin, H.; Hardy, K.D.; Davies, S.S.; Roberts, L.J. Isoprostane Generation and Function. Chem. Rev. 2011, 111, 5973–5996. [Google Scholar] [CrossRef] [Green Version]
- Montuschi, P.; Barnes, P.J.; Roberts, L.J. Isoprostanes: Markers and mediators of oxidative stress. FASEB J. 2004, 18, 1791–1800. [Google Scholar] [CrossRef]
- Arauna, D.; García, F.; Rodríguez-Mañas, L.; Marrugat, J.; Sáez, C.; Alarcón, M.; Wehinger, S.; Espinosa-Parrilla, Y.; Palomo, I.; Fuentes, E. Older adults with frailty syndrome present an altered platelet function and an increased level of circulating oxidative stress and mitochondrial dysfunction biomarker GDF-15. Free Radic. Biol. Med. 2020, 149, 64–71. [Google Scholar] [CrossRef]
- Di Minno, A.; Turnu, L.; Porro, B.; Squellerio, I.; Cavalca, V.; Tremoli, E.; Di Minno MN, D. 8-Hydroxy-2-Deoxyguanosine Levels and Cardiovascular Disease: A Systematic Review and Meta-Analysis of the Literature. Antioxid. Redox Signal. 2016, 24, 548–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Namioka, N.; Hanyu, H.; Hirose, D.; Hatanaka, H.; Sato, T.; Shimizu, S. Oxidative stress and inflammation are associated with physical frailty in patients with Alzheimer’s disease. Geriatr. Gerontol. Int. 2017, 17, 913–918. [Google Scholar] [CrossRef]
- Dada, N.; Kim, N.W.; Wolfert, R.L. Lp-PLA2: An emerging biomarker of coronary heart disease. Expert Rev. Mol. Diagn. 2002, 2, 17–22. [Google Scholar] [CrossRef]
- De Stefano, A.; Mannucci, L.; Tamburi, F.; Cardillo, C.; Schinzari, F.; Rovella, V.; Nisticò, S.; Bennardo, L.; Di Daniele, N.; Tesauro, M. Lp-PLA(2), a new biomarker of vascular disorders in metabolic diseases. Int. J. Immunopathol. Pharmacol. 2019, 33, 2058738419827154. [Google Scholar] [CrossRef] [Green Version]
- Stafforini, D.M. Plasma PAF-AH (PLA2G7): Biochemical Properties, Association with LDLs and HDLs, and Regulation of Expression. Enzymes 2015, 38, 71–93. [Google Scholar] [CrossRef]
- Gong, M.C.; Arbogast, S.; Guo, Z.; Mathenia, J.; Su, W.; Reid, M.B. Calcium-independent phospholipase A2 modulates cytosolic oxidant activity and contractile function in murine skeletal muscle cells. J. Appl. Physiol. 2006, 100, 399–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Álvarez-Sánchez, N.; Álvarez-Ríos, A.I.; Guerrero, J.M.; García-García, F.J.; Rodríguez-Mañas, L.; Cruz-Chamorro, I.; Lardone, P.J.; Carrillo-Vico, A. Homocysteine and C-Reactive Protein Levels Are Associated With Frailty in Older Spaniards: The Toledo Study for Healthy Aging. J. Gerontology. Ser. A 2020, 75, 1488–1494. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Depeint, F.; Bruce, W.R.; Shangari, N.; Mehta, R.; O’Brien, P.J. Mitochondrial function and toxicity: Role of B vitamins on the one-carbon transfer pathways. Chem.-Biol. Interact. 2006, 163, 113–132. [Google Scholar] [CrossRef]
- Kameda, M.; Teruya, T.; Yanagida, M.; Kondoh, H. Frailty markers comprise blood metabolites involved in antioxidation, cognition, and mobility. Proc. Natl. Acad. Sci. USA 2020, 117, 9483–9489. [Google Scholar] [CrossRef] [Green Version]
- Soga, T.; Baran, R.; Suematsu, M.; Ueno, Y.; Ikeda, S.; Sakurakawa, T.; Kakazu, Y.; Ishikawa, T.; Robert, M.; Nishioka, T.; et al. Differential metabolomics reveals ophthalmic acid as an oxidative stress biomarker indicating hepatic glutathione consumption. J. Biol. Chem. 2006, 281, 16768–16776. [Google Scholar] [CrossRef] [Green Version]
- Orlowski, M.; Wilk, S. Synthesis of ophthalmic acid in liver and kidney in vivo. Biochem. J. 1978, 170, 415–419. [Google Scholar] [CrossRef] [Green Version]
- Bohn, T.; Desmarchelier, C.; El, S.N.; Keijer, J.; van Schothorst, E.; Rühl, R.; Borel, P. β-Carotene in the human body: Metabolic bioactivation pathways – from digestion to tissue distribution and excretion. Proc. Nutr. Soc. 2019, 78, 68–87. [Google Scholar] [CrossRef] [Green Version]
- Imran, M.; Ghorat, F.; Ul-Haq, I.; Ur-Rehman, H.; Aslam, F.; Heydari, M.; Shariati, M.A.; Okuskhanova, E.; Yessimbekov, Z.; Thiruvengadam, M.; et al. Lycopene as a Natural Antioxidant Used to Prevent Human Health Disorders. Antioxidants 2020, 9, 706. [Google Scholar] [CrossRef]
- Eisenhauer, B.; Natoli, S.; Liew, G.; Flood, V.M. Lutein and Zeaxanthin-Food Sources, Bioavailability and Dietary Variety in Age-Related Macular Degeneration Protection. Nutrients 2017, 9, 120. [Google Scholar] [CrossRef]
- Burri, B.J. Beta-cryptoxanthin as a source of vitamin A. J. Sci. Food Agric. 2015, 95, 1786–1794. [Google Scholar] [CrossRef] [PubMed]
- Turner, T.; Burri, B.J.; Jamil, K.M.; Jamil, M. The effects of daily consumption of β-cryptoxanthin-rich tangerines and β-carotene-rich sweet potatoes on vitamin A and carotenoid concentrations in plasma and breast milk of Bangladeshi women with low vitamin A status in a randomized controlled trial. Am. J. Clin. Nutr. 2013, 98, 1200–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alvarado, J.C.; Fuentes-Santamaría, V.; Juiz, J.M. Frailty Syndrome and Oxidative Stress as Possible Links Between Age-Related Hearing Loss and Alzheimer’s Disease. Front. Neurosci. 2022, 15, 816300. [Google Scholar] [CrossRef] [PubMed]
- Weber, D.; Davies, M.J.; Grune, T. Determination of protein carbonyls in plasma, cell extracts, tissue homogenates, isolated proteins: Focus on sample preparation and derivatization conditions. Redox Biol. 2015, 5, 367–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mas-Bargues, C.; Escrivá, C.; Dromant, M.; Borrás, C.; Viña, J. Lipid peroxidation as measured by chromatographic determination of malondialdehyde. Human plasma reference values in health and disease. Arch. Biochem. Biophys. 2021, 709, 108941. [Google Scholar] [CrossRef] [PubMed]
- Ingles, M.; Gambini, J.; Carnicero, J.A.; Garcia-Garcia, F.J.; Rodriguez-Manas, L.; Olaso-Gonzalez, G.; Dromant, M.; Borras, C.; Vina, J. Oxidative stress is related to frailty, not to age or sex, in a geriatric population: Lipid and protein oxidation as biomarkers of frailty. J. Am. Geriatr. Soc. 2014, 62, 1324–1328. [Google Scholar] [CrossRef] [PubMed]
- El-Badry, A.A.-M. Serum Malondialdehyde Levels as a Biomarker of Cellular Injury In Human Fascioliasis. J. Taibah Univ. Med. Sci. 2006, 1, 57–64. [Google Scholar] [CrossRef] [Green Version]
- Mao, C.; Yuan, J.-Q.; Lv, Y.-B.; Gao, X.; Yin, Z.-X.; Kraus, V.B.; Luo, J.-S.; Chei, C.-L.; Matchar, D.B.; Zeng, Y.; et al. Associations between superoxide dismutase, malondialdehyde and all-cause mortality in older adults: A community-based cohort study. BMC Geriatr. 2019, 19, 104. [Google Scholar] [CrossRef]
- Gil, P.; Fariñas, F.; Casado, A.; López-Fernández, E. Malondialdehyde: A Possible Marker of Ageing. Gerontology 2002, 48, 209–214. [Google Scholar] [CrossRef]
- Wu, I.C.; Shiesh, S.C.; Kuo, P.H.; Lin, X.Z. High oxidative stress is correlated with frailty in elderly chinese. J. Am. Geriatr. Soc. 2009, 57, 1666–1671. [Google Scholar] [CrossRef]
- Sang, Y.; Roest, M.; de Laat, B.; de Groot, P.G.; Huskens, D. Interplay between platelets and coagulation. Blood Rev. 2021, 46, 100733. [Google Scholar] [CrossRef] [PubMed]
- Kattula, S.; Byrnes, J.R.; Wolberg, A.S. Fibrinogen and Fibrin in Hemostasis and Thrombosis. Arterioscler. Thromb. Vasc. Biol. 2017, 37, e13–e21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hegazy, S.; Elsabaawy, M.; Eltabakh, M.; Hammad, R.; Bedair, H. CD62P (P-selectin) expression as a platelet activation marker in patients with liver cirrhosis with and without cholestasis. Clin. Exp. Hepatol. 2021, 7, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Patrono, C.; Rocca, B. Measurement of Thromboxane Biosynthesis in Health and Disease. Front. Pharmacol. 2019, 10, 1244. [Google Scholar] [CrossRef] [PubMed]
- Qi, C.; Wei, B.; Zhou, W.; Yang, Y.; Li, B.; Guo, S.; Li, J.; Ye, J.; Li, J.; Zhang, Q.; et al. P-selectin-mediated platelet adhesion promotes tumor growth. Oncotarget 2015, 6, 6584–6596. [Google Scholar] [CrossRef] [Green Version]
- Darvin, K.; Randolph, A.; Ovalles, S.; Halade, D.; Breeding, L.; Richardson, A.; Espinoza, S.E. Plasma Protein Biomarkers of the Geriatric Syndrome of Frailty. J. Gerontol. Ser. A 2013, 69A, 182–186. [Google Scholar] [CrossRef] [Green Version]
- Lowe, G.D.O.; Rumley, A.; Mackie, I.J. Plasma fibrinogen. Ann. Clin. Biochem. 2004, 41, 430–440. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Shao, H.-Y.; Hao, L.-B.; Yu, B.-Z.; Qu, P.-F.; Zhou, Y.-X.; Chen, J.-Y. Plasma Fibrinogen Exhibits Better Performance Than Plasma D-Dimer in the Diagnosis of Periprosthetic Joint Infection: A Multicenter Retrospective Study. JBJS 2019, 101, 613–619. [Google Scholar] [CrossRef]
- Hernández, B.; Fuentes, E.; Palomo, I.; Alarcón, M. Increased platelet function during frailty. Exp. Hematol. 2019, 77, 12–25.e12. [Google Scholar] [CrossRef]
- Faria, A.V.S.; Andrade, S.S.; Peppelenbosch, M.P.; Ferreira-Halder, C.V.; Fuhler, G.M. Platelets in aging and cancer—“double-edged sword”. Cancer Metastasis Rev. 2020, 39, 1205–1221. [Google Scholar] [CrossRef]
- Soysal, P.; Isik, A.T.; Carvalho, A.F.; Fernandes, B.S.; Solmi, M.; Schofield, P.; Veronese, N.; Stubbs, B. Oxidative stress and frailty: A systematic review and synthesis of the best evidence. Maturitas 2017, 99, 66–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Liu, S.; Wang, K.; Liu, H. Association of Frailty With Antiplatelet Response Among Elderly Chinese Patients With Coronary Artery Disease Undergoing Percutaneous Coronary Intervention. Clin. Appl. Thromb./Hemost. 2020, 26, 1076029620915994. [Google Scholar] [CrossRef] [PubMed]
- Unsicker, K.; Spittau, B.; Krieglstein, K. The multiple facets of the TGF-β family cytokine growth/differentiation factor-15/macrophage inhibitory cytokine-1. Cytokine Growth Factor Rev. 2013, 24, 373–384. [Google Scholar] [CrossRef] [PubMed]
- Adela, R.; Banerjee, S.K. GDF-15 as a Target and Biomarker for Diabetes and Cardiovascular Diseases: A Translational Prospective. J. Diabetes Res. 2015, 2015, 490842. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Huang, Y.; Lyu, Y.; Dai, W.; Tong, Y.; Li, Y. GDF15 as a biomarker of ageing. Exp. Gerontol. 2021, 146, 111228. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.S.; Kim, S.; Won, C.W.; Jeong, K.H. Association between Plasma Levels of Growth Differentiation Factor-15 and Renal Function in the Elderly: Korean Frailty and Aging Cohort Study. Kidney Blood Press. Res. 2019, 44, 405–414. [Google Scholar] [CrossRef]
- Valentini, A.; Cianfarani, M.A.; Tarantino, U.; Di Daniele, N.; Bertoli, A. Osteoprotegerin as a biomarker of geriatric frailty syndrome. Aging 2019, 11, 4900–4909. [Google Scholar] [CrossRef]
- Pérez de Ciriza, C.; Lawrie, A.; Varo, N. Osteoprotegerin in Cardiometabolic Disorders. Int. J. Endocrinol. 2015, 2015, 564934. [Google Scholar] [CrossRef]
- Muñoz-Torres, M.; Higuera López-Frías, M.d.l.; Fernández García, D. Avances en el conocimiento de la biología del osteoclasto: El sistema osteoprotegerina-ligando del RANK. Med. Clínica 2004, 122, 75–77. [Google Scholar] [CrossRef]
- Poulsen, M.K.; Nybo, M.; Dahl, J.; Hosbond, S.; Poulsen, T.S.; Johansen, A.; Høilund-Carlsen, P.F.; Beck-Nielsen, H.; Rasmussen, L.M.; Henriksen, J.E. Plasma osteoprotegerin is related to carotid and peripheral arterial disease, but not to myocardial ischemia in type 2 diabetes mellitus. Cardiovasc. Diabetol. 2011, 10, 76. [Google Scholar] [CrossRef] [Green Version]
- Montecucco, F.; Steffens, S.; Mach, F. The immune response is involved in atherosclerotic plaque calcification: Could the RANKL/RANK/OPG system be a marker of plaque instability? Clin. Dev. Immunol. 2007, 2007, 75805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDermott, M.M.; Liu, K.; Greenland, P.; Guralnik, J.M.; Criqui, M.H.; Chan, C.; Pearce, W.H.; Schneider, J.R.; Ferrucci, L.; Celic, L.; et al. Functional decline in peripheral arterial disease: Associations with the ankle brachial index and leg symptoms. Jama 2004, 292, 453–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maisel, A.S.; Krishnaswamy, P.; Nowak, R.M.; McCord, J.; Hollander, J.E.; Duc, P.; Omland, T.; Storrow, A.B.; Abraham, W.T.; Wu, A.H.B.; et al. Rapid Measurement of B-Type Natriuretic Peptide in the Emergency Diagnosis of Heart Failure. N. Engl. J. Med. 2002, 347, 161–167. [Google Scholar] [CrossRef]
- Milani, P.; Vincent Rajkumar, S.; Merlini, G.; Kumar, S.; Gertz, M.A.; Palladini, G.; Lacy, M.Q.; Buadi, F.K.; Hayman, S.R.; Leung, N.; et al. N-terminal fragment of the type-B natriuretic peptide (NT-proBNP) contributes to a simple new frailty score in patients with newly diagnosed multiple myeloma. Am. J. Hematol. 2016, 91, 1129–1134. [Google Scholar] [CrossRef] [Green Version]
- Sze, S.; Pellicori, P.; Zhang, J.; Weston, J.; Squire, I.; Clark, A. Effect of frailty on treatment, hospitalisation and death in patients with chronic heart failure. Clin. Res. Cardiol. 2021, 110, 1249–1258. [Google Scholar] [CrossRef] [PubMed]
- Baum, J.I.; Kim, I.-Y.; Wolfe, R.R. Protein Consumption and the Elderly: What Is the Optimal Level of Intake? Nutrients 2016, 8, 359. [Google Scholar] [CrossRef] [Green Version]
- Paddon-Jones, D.; Rasmussen, B.B. Dietary protein recommendations and the prevention of sarcopenia. Curr. Opin. Clin. Nutr. Metab. Care 2009, 12, 86–90. [Google Scholar] [CrossRef] [Green Version]
- Clegg, M.E.; Williams, E.A. Optimizing nutrition in older people. Maturitas 2018, 112, 34–38. [Google Scholar] [CrossRef]
- Richardson, N.E.; Konon, E.N.; Schuster, H.S.; Mitchell, A.T.; Boyle, C.; Rodgers, A.C.; Finke, M.; Haider, L.R.; Yu, D.; Flores, V.; et al. Lifelong restriction of dietary branched-chain amino acids has sex-specific benefits for frailty and lifespan in mice. Nat. Aging 2021, 1, 73–86. [Google Scholar] [CrossRef]
- O’Dowd, J.J.; Robins, D.J.; Miller, D.J. Detection, characterisation, and quantification of carnosine and other histidyl derivatives in cardiac and skeletal muscle. Biochim. Biophys. Acta 1988, 967, 241–249. [Google Scholar] [CrossRef]
- Babizhayev, M.A.; Deyev, A.I.; Yermakova, V.N.; Semiletov, Y.A.; Davydova, N.G.; Kurysheva, N.I.; Zhukotskii, A.V.; Goldman, I.M. N-Acetylcarnosine, a natural histidine-containing dipeptide, as a potent ophthalmic drug in treatment of human cataracts. Peptides 2001, 22, 979–994. [Google Scholar] [CrossRef]
- Ishimoto, T.; Masuo, Y.; Kato, Y.; Nakamichi, N. Ergothioneine-induced neuronal differentiation is mediated through activation of S6K1 and neurotrophin 4/5-TrkB signaling in murine neural stem cells. Cell. Signal. 2019, 53, 269–280. [Google Scholar] [CrossRef] [PubMed]
- López de Heredia, M.; Muñoz, L.; Carru, C.; Sotgia, S.; Zinellu, A.; Serra, C.; Llebaria, A.; Kato, Y.; Nunes, V. S-Methyl-L-Ergothioneine to L-Ergothioneine Ratio in Urine Is a Marker of Cystine Lithiasis in a Cystinuria Mouse Model. Antioxidants 2021, 10, 1424. [Google Scholar] [CrossRef] [PubMed]
- Borodina, I.; Kenny, L.C.; McCarthy, C.M.; Paramasivan, K.; Pretorius, E.; Roberts, T.J.; van der Hoek, S.A.; Kell, D.B. The biology of ergothioneine, an antioxidant nutraceutical. Nutr. Res. Rev. 2020, 33, 190–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheah, I.; Tang, R.; Yew, T.; Lim, K.; Halliwell, B. Administration of Pure Ergothioneine to Healthy Human Subjects: Uptake, Metabolism, and Effects on Biomarkers of Oxidative Damage and Inflammation. Antioxid. Redox Signal. 2016, 26. [Google Scholar] [CrossRef] [Green Version]
- Holeček, M. Histidine in Health and Disease: Metabolism, Physiological Importance, and Use as a Supplement. Nutrients 2020, 12, 848. [Google Scholar] [CrossRef] [Green Version]
- Nagasawa, T.; Yoshizawa, F.; Nishizawa, N. Plasma Nτ-Methylhistidine Concentration Is a Sensitive Index of Myofibrillar Protein Degradation during Starvation in Rats. Biosci. Biotechnol. Biochem. 1996, 60, 501–502. [Google Scholar] [CrossRef] [Green Version]
- Bui, D.; Ravasz, D.; Chinopoulos, C. The Effect of 2-Ketobutyrate on Mitochondrial Substrate-Level Phosphorylation. Neurochem. Res. 2019, 44, 2301–2306. [Google Scholar] [CrossRef] [Green Version]
- Ge, M.L.; Simonsick, E.M.; Dong, B.R.; Kasper, J.D.; Xue, Q.L. Frailty, With or Without Cognitive Impairment, Is a Strong Predictor of Recurrent Falls in a US Population-Representative Sample of Older Adults. J. Gerontol. Ser. A 2021, 76, e354–e360. [Google Scholar] [CrossRef]
- Pályi, G. (Ed.) Chapter 2 - Stock-list of chiral biomolecules. In Biological Chirality; Academic Press: Cambridge, MA, USA, 2020; pp. 15–83. [Google Scholar] [CrossRef]
- Mero, A. Leucine supplementation and intensive training. Sports Med. 1999, 27, 347–358. [Google Scholar] [CrossRef]
- Gorissen, S.H.M.; Phillips, S.M. Chapter 17 - Branched-Chain Amino Acids (Leucine, Isoleucine, and Valine) and Skeletal Muscle. In Nutrition and Skeletal Muscle; Walrand, S., Ed.; Academic Press: Cambridge, MA, USA, 2019; pp. 283–298. [Google Scholar] [CrossRef]
- Harper, A.E.; Miller, R.H.; Block, K.P. Branched-Chain Amino Acid Metabolism. Annu. Rev. Nutr. 1984, 4, 409–454. [Google Scholar] [CrossRef] [PubMed]
- Martínez, Y.; Li, X.; Liu, G.; Bin, P.; Yan, W.; Más, D.; Valdivié, M.; Hu, C.-A.A.; Ren, W.; Yin, Y. The role of methionine on metabolism, oxidative stress, and diseases. Amino Acids 2017, 49, 2091–2098. [Google Scholar] [CrossRef] [PubMed]
- Friedman, M. Analysis, Nutrition, and Health Benefits of Tryptophan. Int. J. Tryptophan Res. 2018, 11, 1178646918802282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz, B.; Oliveira, A.; Ventrucci, G.; Gomes-Marcondes, M.C.C. A leucine-rich diet modulates the mTOR cell signalling pathway in the gastrocnemius muscle under different Walker-256 tumour growth conditions. BMC Cancer 2019, 19, 349. [Google Scholar] [CrossRef]
- Mirza, K.A.; Pereira, S.L.; Voss, A.C.; Tisdale, M.J. Comparison of the anticatabolic effects of leucine and Ca-β-hydroxy-β-methylbutyrate in experimental models of cancer cachexia. Nutrition 2014, 30, 807–813. [Google Scholar] [CrossRef]
- Albaugh, V.L.; Mukherjee, K.; Barbul, A. Proline Precursors and Collagen Synthesis: Biochemical Challenges of Nutrient Supplementation and Wound Healing. J. Nutr. 2017, 147, 2011–2017. [Google Scholar] [CrossRef]
- Kelaiditi, E.; Guyonnet, S.; Cesari, M. Is nutrition important to postpone frailty? Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 37–42. [Google Scholar] [CrossRef] [Green Version]
- Lorenzo-López, L.; Maseda, A.; de Labra, C.; Regueiro-Folgueira, L.; Rodríguez-Villamil, J.L.; Millán-Calenti, J.C. Nutritional determinants of frailty in older adults: A systematic review. BMC Geriatr. 2017, 17, 108. [Google Scholar] [CrossRef] [Green Version]
- Bartali, B.; Frongillo, E.A.; Bandinelli, S.; Lauretani, F.; Semba, R.D.; Fried, L.P.; Ferrucci, L. Low nutrient intake is an essential component of frailty in older persons. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2006, 61, 589–593. [Google Scholar] [CrossRef]
- Nair, R.; Maseeh, A. Vitamin D: The “sunshine” vitamin. J. Pharmacol. Pharmacother. 2012, 3, 118–126. [Google Scholar] [CrossRef]
- Alonso-Bouzon, C.; Carcaillon, L.; Garcia-Garcia, F.J.; Amor-Andres, M.S.; El Assar, M.; Rodriguez-Manas, L. Association between endothelial dysfunction and frailty: The Toledo Study for Healthy Aging. Age 2014, 36, 495–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, W.; Lee, H.J.; Jang, H.B.; Kim, H.-J.; Ban, H.-J.; Kim, K.Y.; Nam, M.S.; Choi, J.S.; Lee, K.-T.; Cho, S.B.; et al. Asymmetric dimethylarginine (ADMA) is identified as a potential biomarker of insulin resistance in skeletal muscle. Sci. Rep. 2018, 8, 2133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- San Miguel, A.; San Miguel, R.; Martín Gil, F.J. Dimetilarginina asimétrica (ADMA) en diferentes enfermedades. Rev. Lab. Clín. 2008, 1, 113–121. [Google Scholar] [CrossRef]
- Sibal, L.; Agarwal, S.C.; Home, P.D.; Boger, R.H. The Role of Asymmetric Dimethylarginine (ADMA) in Endothelial Dysfunction and Cardiovascular Disease. Curr. Cardiol. Rev. 2010, 6, 82–90. [Google Scholar] [CrossRef]
- Yamamoto, M.; Adachi, H.; Enomoto, M.; Fukami, A.; Nakamura, S.; Nohara, Y.; Sakaue, A.; Morikawa, N.; Hamamura, H.; Toyomasu, K.; et al. Lower albumin levels are associated with frailty measures, trace elements, and an inflammation marker in a cross-sectional study in Tanushimaru. Environ. Health Prev. Med. 2021, 26, 25. [Google Scholar] [CrossRef]
- Vítek, L. Bilirubin and atherosclerotic diseases. Physiol. Res. 2017, 66, S11–S20. [Google Scholar] [CrossRef]
- Inoguchi, T.; Fukuhara, S.; Yamato, M.; Nakai, M.; Etoh, T.; Masakado, M.; Suehiro, S.; Umeda, F.; Yamauchi, T. Serum bilirubin level is a strong predictor for disability in activities in daily living (ADL) in Japanese elderly patients with diabetes. Sci. Rep. 2019, 9, 7069. [Google Scholar] [CrossRef]
- Kawabata, H. Transferrin and transferrin receptors update. Free Radic. Biol. Med. 2019, 133, 46–54. [Google Scholar] [CrossRef]
- Marcos-Pérez, D.; Sánchez-Flores, M.; Maseda, A.; Lorenzo-López, L.; Millán-Calenti, J.C.; Pásaro, E.; Laffon, B.; Valdiglesias, V. Serum cortisol but not oxidative stress biomarkers are related to frailty: Results of a cross-sectional study in Spanish older adults. J. Toxicol. Environ. Health Part A 2019, 82, 815–825. [Google Scholar] [CrossRef]
- Katsu, Y.; Baker, M.E. Subchapter 123D—Cortisol. In Handbook of Hormones (Second Edition); Ando, H., Ukena, K., Nagata, S., Eds.; Academic Press: San Diego, CA, USA, 2021; pp. 947–949. [Google Scholar] [CrossRef]
- Gardner, M.P.; Lightman, S.; Sayer, A.A.; Cooper, C.; Cooper, R.; Deeg, D.; Ebrahim, S.; Gallacher, J.; Kivimaki, M.; Kumari, M.; et al. Dysregulation of the hypothalamic pituitary adrenal (HPA) axis and physical performance at older ages: An individual participant meta-analysis. Psychoneuroendocrinology 2013, 38, 40–49. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Yi, X.; Tu, S.; Cheng, C.; Luo, J. Kaempferol promotes BMSC osteogenic differentiation and improves osteoporosis by downregulating miR-10a-3p and upregulating CXCL12. Mol. Cell. Endocrinol. 2021, 520, 111074. [Google Scholar] [CrossRef] [PubMed]
- Smith-Vikos, T.; Liu, Z.; Parsons, C.; Gorospe, M.; Ferrucci, L.; Gill, T.M.; Slack, F.J. A serum miRNA profile of human longevity: Findings from the Baltimore Longitudinal Study of Aging (BLSA). Aging 2016, 8, 2971–2987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ipson, B.R.; Fletcher, M.B.; Espinoza, S.E.; Fisher, A.L. Identifying Exosome-Derived MicroRNAs as Candidate Biomarkers of Frailty. J. Frailty Aging 2018, 7, 100–103. [Google Scholar] [CrossRef] [PubMed]
- Valadi, H.; Ekström, K.; Bossios, A.; Sjöstrand, M.; Lee, J.J.; Lötvall, J.O. Exosome-mediated transfer of mRNAs and microRNAs is a novel mechanism of genetic exchange between cells. Nat. Cell Biol. 2007, 9, 654–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Zhang, L.; Shi, X.; Liao, T.; Zhang, N.; Gao, Y.; Xing, R.; Wang, P. MicroRNA-10a-3p Improves Cartilage Degeneration by Regulating CH25H-CYP7B1-RORα Mediated Cholesterol Metabolism in Knee Osteoarthritis Rats. Front. Pharmacol. 2021, 12, 690181. [Google Scholar] [CrossRef]
- Mao, G.; Zhang, Z.; Huang, Z.; Chen, W.; Huang, G.; Meng, F.; Zhang, Z.; Kang, Y. MicroRNA-92a-3p regulates the expression of cartilage-specific genes by directly targeting histone deacetylase 2 in chondrogenesis and degradation. Osteoarthr. Cartil. 2017, 25, 521–532. [Google Scholar] [CrossRef] [Green Version]
- Zhou, C.; Kong, W.; Ju, T.; Xie, Q.; Zhai, L. MiR-185-3p mimic promotes the chemosensitivity of CRC cells via AQP5. Cancer Biol. Ther. 2020, 21, 790–798. [Google Scholar] [CrossRef]
- Zhu, X.; Li, D.; Yu, F.; Jia, C.; Xie, J.; Ma, Y.; Fan, S.; Cai, H.; Luo, Q.; Lv, Z.; et al. miR-194 inhibits the proliferation, invasion, migration, and enhances the chemosensitivity of non-small cell lung cancer cells by targeting forkhead box A1 protein. Oncotarget 2016, 7, 13139–13152. [Google Scholar] [CrossRef] [Green Version]
- Yang, F.; Xiao, Z.; Zhang, S. Knockdown of miR-194-5p inhibits cell proliferation, migration and invasion in breast cancer by regulating the Wnt/β-catenin signaling pathway. Int. J. Mol. Med. 2018, 42, 3355–3363. [Google Scholar] [CrossRef] [Green Version]
- Chang, H.Y.; Ye, S.P.; Pan, S.L.; Kuo, T.T.; Liu, B.C.; Chen, Y.L.; Huang, T.C. Overexpression of miR-194 Reverses HMGA2-driven Signatures in Colorectal Cancer. Theranostics 2017, 7, 3889–3900. [Google Scholar] [CrossRef]
- Shi, Y.; Mao, X.; Cai, M.; Hu, S.; Lai, X.; Chen, S.; Jia, X.; Wang, J.; Lai, S. miR-194-5p negatively regulates the proliferation and differentiation of rabbit skeletal muscle satellite cells. Mol. Cell. Biochem. 2021, 476, 425–433. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.; Li, Z.; Men, Q.; Li, Y.; Li, H.; Chong, T. miR-326 functions as a tumor suppressor in human prostatic carcinoma by targeting Mucin1. Biomed. Pharmacother. 2018, 108, 574–583. [Google Scholar] [CrossRef] [PubMed]
- Kitago, M.; Martinez, S.R.; Nakamura, T.; Sim, M.S.; Hoon, D.S. Regulation of RUNX3 tumor suppressor gene expression in cutaneous melanoma. Clin. Cancer Res. 2009, 15, 2988–2994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kordaß, T.; Weber, C.E.M.; Eisel, D.; Pane, A.A.; Osen, W.; Eichmüller, S.B. miR-193b and miR-30c-1(*) inhibit, whereas miR-576-5p enhances melanoma cell invasion in vitro. Oncotarget 2018, 9, 32507–32522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, J.; Liu, L.; Shen, J.; Zhou, N.; Feng, Y.; Zhang, N.; Sun, Q.; Zhu, Y. miR-576-5p promotes epithelial-to-mesenchymal transition in colorectal cancer by targeting the Wnt5a-mediated Wnt/β-catenin signaling pathway. Mol. Med. Rep. 2021, 23, 94. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.; Wang, J.; Zhou, S.; Zhou, J.; Jia, G.; Wang, H.; Xin, C.; Fu, G.; Zhang, J. miR-760 regulates skeletal muscle proliferation in rheumatoid arthritis by targeting Myo18b. Mol. Med. Rep. 2019, 20, 4843–4854. [Google Scholar] [CrossRef] [Green Version]
- Wou, F.; Conroy, S. The frailty syndrome. Medicine 2013, 41, 13–15. [Google Scholar] [CrossRef]
- Blodgett, J.; Theou, O.; Kirkland, S.; Andreou, P.; Rockwood, K. Frailty in NHANES: Comparing the frailty index and phenotype. Arch. Gerontol. Geriatr. 2015, 60, 464–470. [Google Scholar] [CrossRef]
- Mitnitski, A.; Collerton, J.; Martin-Ruiz, C.; Jagger, C.; von Zglinicki, T.; Rockwood, K.; Kirkwood, T.B. Age-related frailty and its association with biological markers of ageing. BMC Med. 2015, 13, 161. [Google Scholar] [CrossRef] [Green Version]
- Mailliez, A.; Guilbaud, A.; Puisieux, F.; Dauchet, L.; Boulanger, É. Circulating biomarkers characterizing physical frailty: CRP, hemoglobin, albumin, 25OHD and free testosterone as best biomarkers. Results of a meta-analysis. Exp. Gerontol. 2020, 139, 111014. [Google Scholar] [CrossRef]
- Pérez-Ros, P.; Navarro-Flores, E.; Julián-Rochina, I.; Martínez-Arnau, F.M.; Cauli, O. Changes in Salivary Amylase and Glucose in Diabetes: A Scoping Review. Diagnostics 2021, 11, 453. [Google Scholar] [CrossRef] [PubMed]
- Kouroubali, A.; Kondylakis, H.; Logothetidis, F.; Katehakis, D.G. Developing an AI-Enabled Integrated Care Platform for Frailty. Healthcare 2022, 10, 443. [Google Scholar] [CrossRef] [PubMed]
- Ambagtsheer, R.C.; Shafiabady, N.; Dent, E.; Seiboth, C.; Beilby, J. The application of artificial intelligence (AI) techniques to identify frailty within a residential aged care administrative data set. Int. J. Med. Inform. 2020, 136, 104094. [Google Scholar] [CrossRef] [PubMed]
- Contreras, I.; Vehi, J. Artificial Intelligence for Diabetes Management and Decision Support: Literature Review. J. Med. Internet Res. 2018, 20, e10775. [Google Scholar] [CrossRef]
- Mohanty, S.D.; Lekan, D.; McCoy, T.P.; Jenkins, M.; Manda, P. Machine learning for predicting readmission risk among the frail: Explainable AI for healthcare. Patterns 2022, 3, 100395. [Google Scholar] [CrossRef]
- Tarekegn, A.; Ricceri, F.; Costa, G.; Ferracin, E.; Giacobini, M. Predictive Modeling for Frailty Conditions in Elderly People: Machine Learning Approaches. JMIR Med. Inform. 2020, 8, e16678. [Google Scholar] [CrossRef]


{kind=link}
| BIOMARKER | SAMPLE | CUT VALUES (FRAIL—NOT FRAIL) | FRAILTY SCALE | COUNTRY | YEAR | GROUP DESCRIPTION | REFERENCE |
|---|---|---|---|---|---|---|---|
| Interleukin-6 (pg/L) | Serum | Median 11.08 interquartile range: 5.04–13.63 (Frail) Median 4.11 interquartile range: 2.83–5.84 (Not Frail) | Fried | Norway | 2010 | Transversal study Group of 137 patients, median age 80 years | Rønning, B. et al., 2010 [49] |
| Hs-CRP (mg/L) | Serum | 4.2 (Frail) 3.1 (Not Frail) | Fried | China | 2016 | Transversal study Group of 1478 participants, 70–84 years old | Zhu, Y. et al. (2016) [28] |
| MCP-1 (pg/mL) | Plasma | Median and interquartile range: 415 (345–501) (Frail) 384 (324–462) (Pre-frail) 364 (301–441) (Not Frail) | Fried | United States | 2016 | Group of people over 60 years of age, divided into 3 groups: n = 142 frail, n = 864 pre-frail, n = 913 not frail | Liu, C.K. et al. (2016) [50] |
| TNFR2 (pg/mL) | Plasma | Median and interquartile range: 3151 (2506–4447) (Frail) 2669 (2149–3443) (Pre-frail) 2385 (1963–2877) (Not Frail) | Fried | United States | 2016 | Group of people over 60 years of age, divided into 3 groups: n = 142 frail, n = 864 pre-frail, n = 913 not frail | Liu, C.K. et al. (2016) [50] |
| ICAM-1 (ng/mL) | Plasma | Median and interquartile range: 307 (250–381) (Frail) 293 (244–359) (Pre-frail) 270 (233–334) (Not Frail) | Fried | United States | 2016 | Group of people over 60 years of age, divided into 3 groups: n = 142 frail, n = 864 pre-frail, n = 913 not frail | Liu, C.K. et al. (2016) [50] |
| CXCL10 | Whole blood | Increased in frailty | Fried | United States | 2009 | Group of 32 people, 16 frail and 16 not frail, average age of 83 years, 87.5% women | Qu et al. (2009) [66] |
| Galectin-3 (ng/mL) | Serum | 34.4 ± 19.3 (Frail). 14.3 ± 7.6 (Not Frail). Increased in frailty | Clinical Frailty Scale (CFS) | Italy | 2020 | Group of 54 frail persons and 74 not frail persons, age frail 70.5 ± 5.4 years, age not frail 68.2 ± 4.2 years | Komici et al. (2020) [71] |
| BIOMARKER | SAMPLE | CUT VALUES (FRAIL–NOT FRAIL) | FRAILTY SCALE | COUNTRY | YEAR | GROUP DESCRIPTION | REFERENCE |
|---|---|---|---|---|---|---|---|
| Isoprostanes (mg/L) | Urine | Median and interquartile range: 11.5 (8.50–15.40) (Frail) 10.2 (7.60–14.30) (Pre-frail) 9.5 (7.1–12.8) (Not Frail) | Fried | United States | 2016 | Group of people over 60 years of age, divided into 3 groups: n = 142 frail, n = 864 pre-frail, n = 913 not frail | Liu, C.K. et al. (2016) [50] |
| 8-isoprostane (pg/mL) | Plasma | Interquartile range: 64.0–96.7 (Frail) 38.2–72.2 (Not Frail) | Fried | Chile | 2019 | Group of people over 65 years of age, divided into 2 groups: n = 29 frail, n = 29 not frail. | Arauna, D. et al. (2019) [76] |
| 8-hydroxy-2-deoxyguanosine (ng/mg Creatinine) | Urine | 5.39 ± 2.23 (Frail) 5.44 ± 2.70 (Pre-frail) 3.90 ± 1.67 (Not Frail) | Fried | Japan | 2017 | Group of 140 outpatients with probable Alzheimer’s disease, 65 years and older | Namioka, N. et al. (2017) [78] |
| Lp-PLA2 mass (ng/mL) | Plasma | Median and interquartile range: 210 (183–237) (Frail) 199 (172–229) (Pre-frail) 199 (168–228) (Not Frail) | Fried | United States | 2016 | Group of people over 60 years of age, divided into 3 groups: n = 142 frail, n = 864 pre-frail, n = 913 not frail | Liu, C.K. et al. (2016) [50] |
| Lp-PLA2 activity (nm/mL/min) | Plasma | Median and interquartile range: 139 (119–166) (Frail) 137 (115–160) (Pre-frail) 136 (114–159) (Not Frail) | Fried | United States | 2016 | Group of people over 60 years of age, divided into 3 groups: n = 142 frail, n = 864 pre-frail, n = 913 not frail | Liu, C.K. et al. (2016) [50] |
| Homocysteine (µmol/L) | Serum | Increased in frail older people | Fried | Spain | 2020 | Study group of 1211 people, of which 515 were men (42.5%) and 696 were women (57.5%), whose ages were between 65 and 98 years | Alvarez-Sanchez n, (2020) [83] |
| Ophthalmic acid | Serum | Decreased in frailty | Edmonton Frail Scale (EFS) | Japan | 2020 | Group of 19 participants, mean age 84.2 ± 6.9 years, 7 men and 12 women, of which 9 were diagnosed as frail (age 88.2 ± 6.8 years) and 10 as not frail (age 80.5 ± 4.7 years) | Kameda, M., et al. (2020) [86] |
| Lycopene (µmol/L) | Plasma | Decreased in frail older people | Fried | Germany | 2019 | Study group of 1450 people from the FRAILOMIC database, all over 65 years of age | Kochlik, B., (2019) [29] |
| Lutein/zeaxanthin (µmol/L) | Plasma | Decreased in frail older people | Fried | Germany | 2019 | Study group of 1450 people from the FRAILOMIC database, all over 65 years of age | Kochlik, B., (2019) [29] |
| β- cryptoxanthin (µmol/L) | Plasma | Decreased in frail older people | Fried | Germany | 2019 | Study group of 1450 people from the FRAILOMIC database, all over 65 years of age | Kochlik, B., (2019) [29] |
| Carbonylated proteins (nmol/mg) | Plasma | Increased in frail older people | Fried | Germany | 2019 | Study group of 1450 people from the FRAILOMIC database, all over 65 years of age | Kochlik, B., (2019) [29] |
| Malondialdehyde | Plasma | Increased in frail older people | Fried | Spain | 2014 | Group of 742 people from the Toledo Study for Healthy Aging, of which 309 were men and 433 were women | Ingles, M., (2014) [97] |
| BIOMARKER | SAMPLE | CUT VALUES (FRAIL—NOT FRAIL) | FRAILTY SCALE | COUNTRY | YEAR | GROUP DESCRIPTION | REFERENCE |
|---|---|---|---|---|---|---|---|
| P-selectin (ng/mL) | Plasma | Median and interquartile range: 41 (32–51) (Frail) 41 (33–49) (Pre-frail) 39 (32–47) (Not Frail) | Fried | United States | 2016 | Group of people over 60 years of age, divided into 3 groups: n = 142 frail, n = 864 pre-frail, n = 913 not frail | Liu, C.K. et al. (2016) [50] |
| Fibrinogen (g/L) | Plasma | 70.4 ± 17.5 (Frail) 40.6 ± 9.3 (Not Frail) | Fried | United States | 2013 | Group of 65 people over 65 years old n = 12 frail n = 22 not frail | Darvin, K. et al., 2013 [107] |
| Thromboxane B2 (ng/mL) | Plasma | Interquartile range: 64.0–96.7 (Frail) 38.1–72.2 (Not Frail) | Fried | Chile | 2019 | Group of people over 65 years of age, divided into 2 groups: n = 29 frail, n = 29 not frail | Arauna, D. et al. (2019) [76] |
| BIOMARKER | SAMPLE | CUT VALUES (FRAIL—NOT FRAIL) | FRAILTY SCALE | COUNTRY | YEAR | GROUP DESCRIPTION | REFERENCE |
|---|---|---|---|---|---|---|---|
| GDF15 | Plasma | Interquartile range: 1845–4121 (Frail) 1190–1747 (Not Frail) | Fried | Chile | 2019 | Group of people over 65 years of age, divided into 2 groups: n = 29 frail, n = 29 not frail | Arauna, D. et al. (2019) [76] |
| BIOMARKER | SAMPLE | CUT VALUES (FRAIL—NOT FRAIL) | FRAILTY SCALE | COUNTRY | YEAR | GROUP DESCRIPTION | REFERENCE |
|---|---|---|---|---|---|---|---|
| Osteoprotegerine (pm/L) | Plasma | Median and interquartile range: 5.88 (4.82–7.41) (Frail) 5.13 (4.23–6.13) (Pre-frail) 4.81 (4.01–5.59) (Not Frail) | Fried | United States | 2016 | Group of people over 60 years of age, divided into 3 groups: n = 142 frail, n = 864 pre-frail, n = 913 not frail | Liu, C.K. et al. (2016) [50] |
| NT-proBNP (pg/mL) | Serum | 11,427.9 ± 21,803.4 (Frail). 1856.4 ± 3570.1 (Not Frail). Increased in frailty | Clinical Frailty Scale (CFS) | Italy | 2020 | Group of 54 frail persons and 74 not frail persons, age frail 70.5 ± 5.4 years, age not frail 68.2 ± 4.2 years | Komici et al. (2020) [71] |
| BIOMARKER | SAMPLE | CUT VALUES (FRAIL—NOT FRAIL) | FRAILTY SCALE | COUNTRY | YEAR | GROUP DESCRIPTION | REFERENCE |
|---|---|---|---|---|---|---|---|
| Acetyl-carnosine | Serum | Decreased in frailty | Edmonton Frail Scale (EFS) | Japan | 2020 | Group of 19 participants, mean age 84.2 ± 6.9 years, 7 men and 12 women, of which 9 were diagnosed as frail (age 88.2 ± 6.8 years) and 10 as not frail (age 80.5 ± 4.7 years) | Kameda, M., et al. (2020) [86] |
| Ergothioneine | Serum | Decreased in frailty | Edmonton Frail Scale (EFS) | Japan | 2020 | Group of 19 participants, mean age 84.2 ± 6.9 years, 7 men and 12 women, of which 9 were diagnosed as frail (age 88.2 ± 6.8 years) and 10 as not frail (age 80.5 ± 4.7 years) | Kameda, M., et al. (2020) [86] |
| S-methyl-ergothioneine | Serum | Decreased in frailty | Edmonton Frail Scale (EFS) | Japan | 2020 | Group of 19 participants, mean age 84.2 ± 6.9 years, 7 men and 12 women, of which 9 were diagnosed as frail (age 88.2 ± 6.8 years) and 10 as not frail (age 80.5 ± 4.7 years) | Kameda, M., et al. (2020) [86] |
| Trimethyl-histidine | Serum | Decreased in frailty | Edmonton Frail Scale (EFS) | Japan | 2020 | Group of 19 participants, mean age 84.2 ± 6.9 years, 7 men and 12 women, of which 9 were diagnosed as frail (age 88.2 ± 6.8 years) and 10 as not frail (age 80.5 ± 4.7 years) | Kameda, M., et al. (2020) [86] |
| 2-ketobutyrate | Serum | Decreased in frailty | Edmonton Frail Scale (EFS) | Japan | 2020 | Group of 19 participants, mean age 84.2 ± 6.9 years, 7 men and 12 women, of which 9 were diagnosed as frail (age 88.2 ± 6.8 years) and 10 as not frail (age 80.5 ± 4.7 years) | Kameda, M., et al. (2020) [86] |
| Isoleucine | Serum | Decreased in frailty | Edmonton Frail Scale (EFS) | Japan | 2020 | Group of 19 participants, mean age 84.2 ± 6.9 years, 7 men and 12 women, of which 9 were diagnosed as frail (age 88.2 ± 6.8 years) and 10 as not frail (age 80.5 ± 4.7 years) | Kameda, M., et al. (2020) [86] |
| Leucine | Serum | Decreased in frailty | Edmonton Frail Scale (EFS) | Japan | 2020 | Group of 19 participants, mean age 84.2 ± 6.9 years, 7 men and 12 women, of which 9 were diagnosed as frail (age 88.2 ± 6.8 years) and 10 as not frail (age 80.5 ± 4.7 years) | Kameda, M., et al. (2020) [86] |
| Methionine | Serum | Decreased in frailty | Edmonton Frail Scale (EFS) | Japan | 2020 | Group of 19 participants, mean age 84.2 ± 6.9 years, 7 men and 12 women, of which 9 were diagnosed as frail (age 88.2 ± 6.8 years) and 10 as not frail (age 80.5 ± 4.7 years) | Kameda, M., et al. (2020) [86] |
| Tryptophan | Serum | Decreased in frailty | Edmonton Frail Scale (EFS) | Japan | 2020 | Group of 19 participants, mean age 84.2 ± 6.9 years, 7 men and 12 women, of which 9 were diagnosed as frail (age 88.2 ± 6.8 years) and 10 as not frail (age 80.5 ± 4.7 years) | Kameda, M., et al. (2020) [86] |
| Proline | Serum | Decreased in frailty | Edmonton Frail Scale (EFS) | Japan | 2020 | Group of 19 participants, mean age 84.2 ± 6.9 years, 7 men and 12 women, of which 9 were diagnosed as frail (age 88.2 ± 6.8 years) and 10 as not frail (age 80.5 ± 4.7 years) | Kameda, M., et al. (2020) [86] |
| Vitamin D3 (nmol/L) | Plasma | Decreased in frail older people | Fried | Germany | 2019 | Study group of 1450 people from the FRAILOMIC database, all over 65 years of age | Kochlik, B., (2019) [29] |
| β-carotene (µmol/L) | Plasma | Decreased in frail older people | Fried | Germany | 2019 | Study group of 1450 people from the FRAILOMIC database, all over 65 years of age | Kochlik, B., (2019) [29] |
| ADMA | Plasma | Increased in frailty | Fried | Spain | 2014 | Group of 1287 people (552 men and 735 women), mean age of 74.4 years, of which 107 were frail, 542 pre-frail, and 638 not frail. In the group of frail people, ADMA presented higher values | Alonso-Bouzón, C. et al. (2014) [154] |
| BIOMARKER | SAMPLE | CUT VALUES (FRAIL—NOT FRAIL) | FRAILTY SCALE | COUNTRY | YEAR | GROUP DESCRIPTION | REFERENCE |
|---|---|---|---|---|---|---|---|
| Uric acid (mg/dL) | Serum | 5.49 ± 1.29 (Frail) 5.00 ± 1.06 (Pre-frail) 5.25 ± 1.23 (Not Frail) | Fried | Japan | 2017 | Group of 140 outpatients with probable Alzheimer’s disease, 65 years and older | Namioka, N. et al. (2017) [78] |
| Urate | Serum | Decreased in frailty | Edmonton Frail Scale (EFS) | Japan | 2020 | Group of 19 participants, mean age 84.2 ± 6.9 years, 7 men and 12 women, of which 9 were diagnosed as frail (age 88.2 ± 6.8 years) and 10 as not frail (age 80.5 ± 4.7 years) | Kameda, M., et al. (2020) [86] |
| Albumin (g/dL) | Serum | 3.92 ± 0.31 (Frail) 3.96 ± 0.29 (Pre-frail) 4.06 ± 0.26 (Not Frail) | Fried | Japan | 2017 | Group of 140 outpatients with probable Alzheimer’s disease, 65 years and older | Namioka, N. et al. (2017) [78] |
| Bilirubin (mg/dL) | Serum | 0.54 ± 0.18 (Frail) 0.60 ± 0.21 (Pre-frail) 0.66 ± 0.22 (Not frail) | Fried | Japan | 2017 | Group of 140 outpatients with probable Alzheimer’s disease, 65 years and older | Namioka, N. et al. (2017) [78] |
| Transferrin (ng/mL) | Plasma | 58.3 ± 10.2 (Frail) 43.4 ± 11.4 (Not Frail) | Fried | United States | 2013 | Group of 65 people over 65 years old, n = 12 frail n = 22 not frail | Darvin, K. et al., 2013 [107] |
| Cortisol (µg/dL) | Serum | Increased in frail older people | Fried | Spain | 2019 | Study group of 252 elderly people (82 men and 170 women) from Spain, whose age range was 65–102 years | Marcos-Perez, D. (2019) [162] |
| BIOMARKER | SAMPLE | CUT VALUES (FRAIL—NOT FRAIL) | FRAILTY SCALE | COUNTRY | YEAR | GROUP DESCRIPTION | REFERENCE |
|---|---|---|---|---|---|---|---|
| miR-10a-3p | Plasma | Increased in frailty | Fried | United States | 2018 | Young people (ages 23–35 years) and people older than 65 years were recruited (the latter were classified as frail or not frail according to Fried’s criteria). | Ipson, B.R., et al. (2018) [167] |
| miR-92a-3p | Plasma | Increased in frailty | Fried | United States | 2018 | Young people (ages 23–35 years) and people older than 65 years were recruited (the latter were classified as frail or not frail according to Fried’s criteria) | Ipson, B.R., et al. (2018) [167] |
| miR-185–3p | Plasma | Increased in frailty | Fried | United States | 2018 | Young people (ages 23–35 years) and people older than 65 years were recruited (the latter were classified as frail or not frail according to Fried’s criteria) | Ipson, B.R., et al. (2018) [167] |
| miR-194–5p | Plasma | Increased in frailty | Fried | United States | 2018 | Young people (ages 23–35 years) and people older than 65 years were recruited (the latter were classified as frail or not frail according to Fried’s criteria) | Ipson, B.R., et al. (2018) [167] |
| miR-326 | Plasma | Increased in frailty | Fried | United States | 2018 | Young people (ages 23–35 years) and people older than 65 years were recruited (the latter were classified as frail or not frail according to Fried’s criteria) | Ipson, B.R., et al. (2018) [167] |
| miR-532–5p | Plasma | Increased in frailty | Fried | United States | 2018 | Young people (ages 23–35 years) and people older than 65 years were recruited (the latter were classified as frail or not frail according to Fried’s criteria) | Ipson, B.R., et al. (2018) [167] |
| miR-576–5p | Plasma | Increased in frailty | Fried | United States | 2018 | Young people (ages 23–35 years) and people older than 65 years were recruited (the latter were classified as frail or not frail according to Fried’s criteria) | Ipson, B.R., et al. (2018) [167] |
| miR-760 | Plasma | Increased in frailty | Fried | United States | 2018 | Young people (ages 23–35 years) and people older than 65 years were recruited (the latter were classified as frail or not frail according to Fried’s criteria) | Ipson, B.R., et al. (2018) [167] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sepúlveda, M.; Arauna, D.; García, F.; Albala, C.; Palomo, I.; Fuentes, E. Frailty in Aging and the Search for the Optimal Biomarker: A Review. Biomedicines 2022, 10, 1426. https://doi.org/10.3390/biomedicines10061426
Sepúlveda M, Arauna D, García F, Albala C, Palomo I, Fuentes E. Frailty in Aging and the Search for the Optimal Biomarker: A Review. Biomedicines. 2022; 10(6):1426. https://doi.org/10.3390/biomedicines10061426
Chicago/Turabian StyleSepúlveda, Magdalena, Diego Arauna, Francisco García, Cecilia Albala, Iván Palomo, and Eduardo Fuentes. 2022. "Frailty in Aging and the Search for the Optimal Biomarker: A Review" Biomedicines 10, no. 6: 1426. https://doi.org/10.3390/biomedicines10061426