
Association of Metabolomic Change and Treatment Response in Patients with Non-Alcoholic Fatty Liver Disease

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Study Design
2.3. Laboratory and Image Testing
2.4. Metabolite Measurements
2.5. Main Outcome
2.6. Statistical Analysis
2.7. Ethics
3. Results
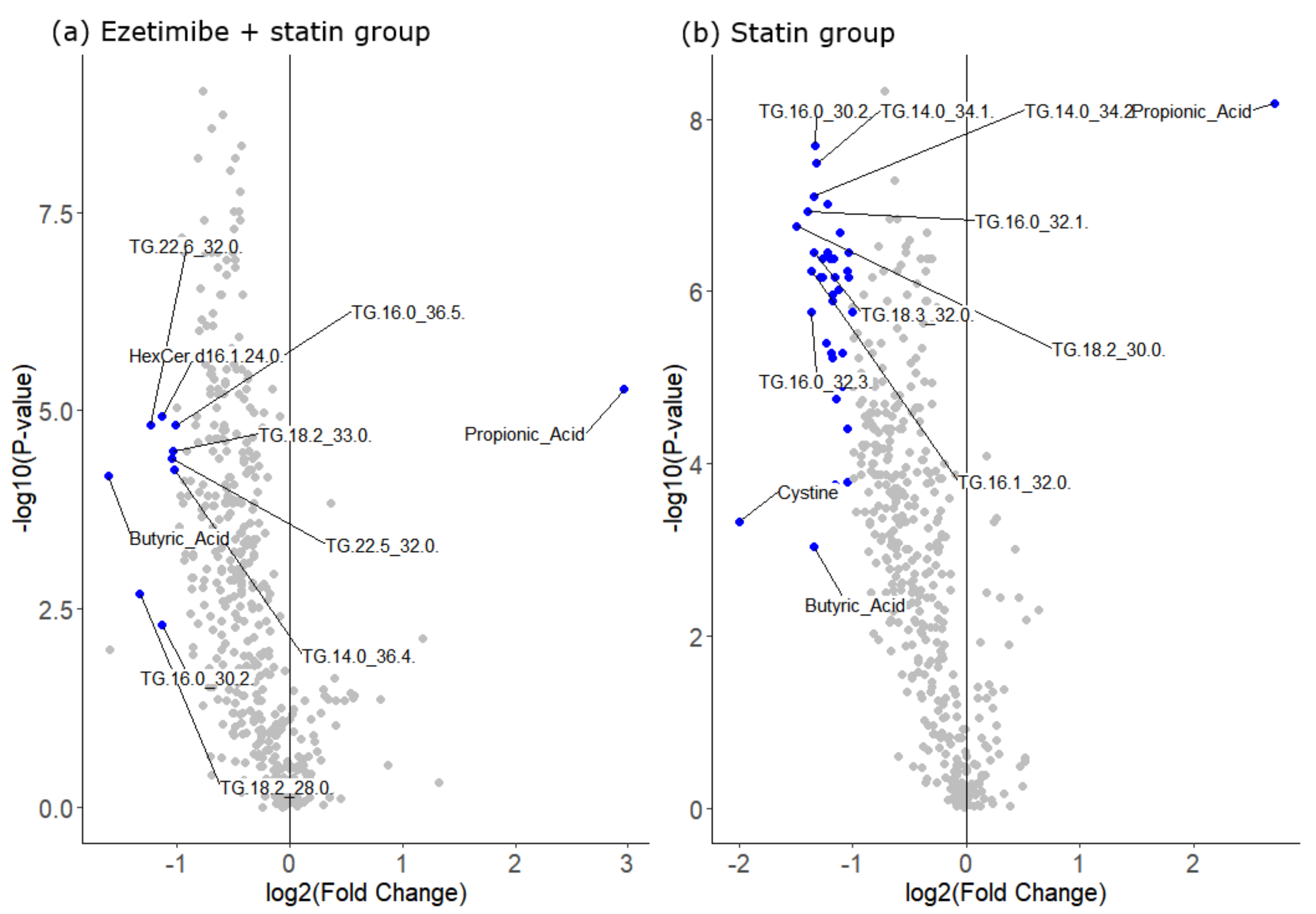
3.1. Response in Clinical Parameters and Metabolites
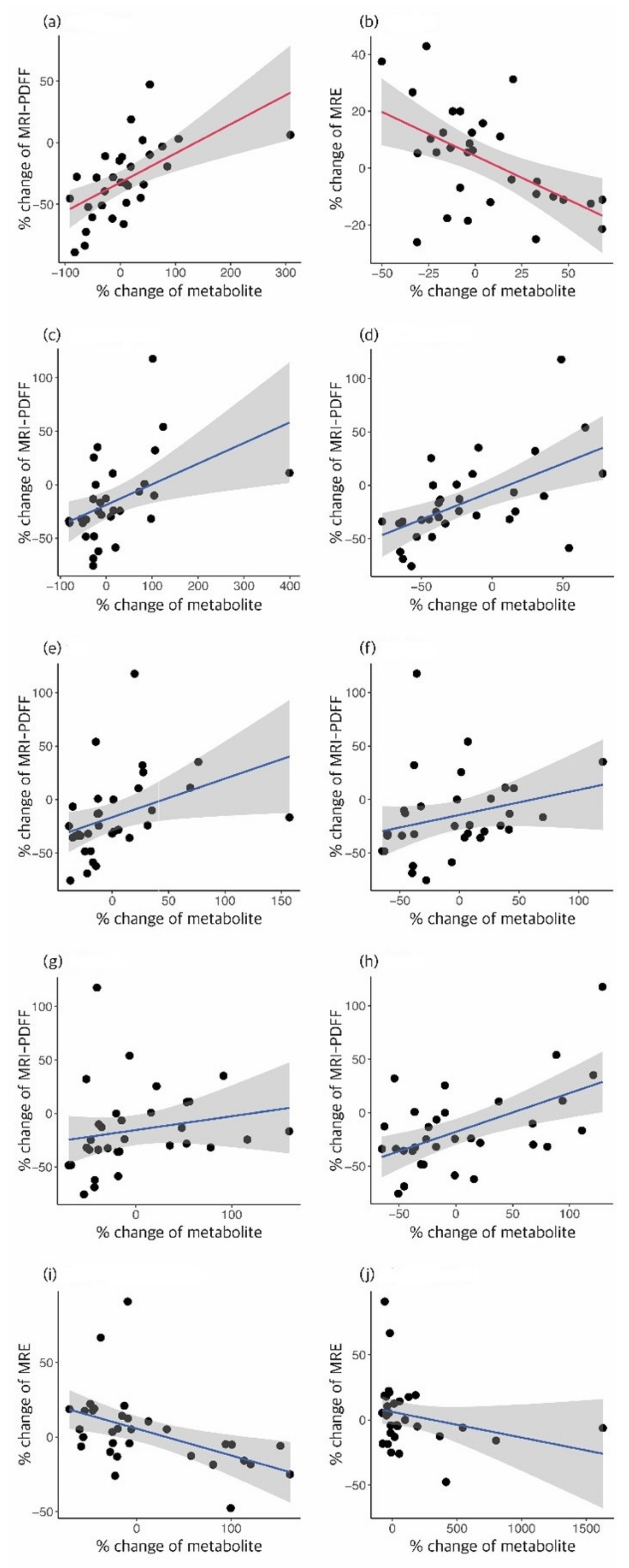
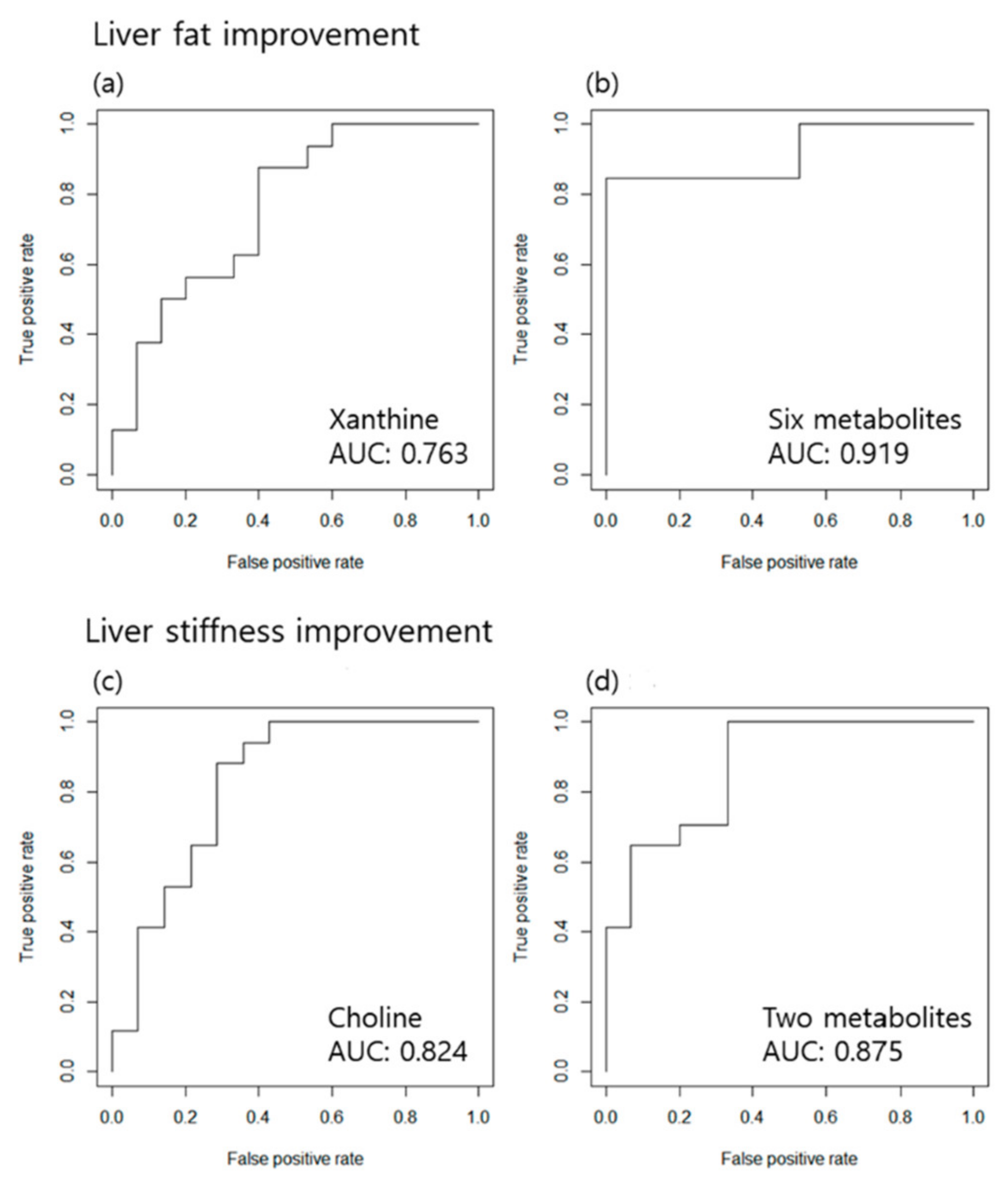
3.2. Association of the Treatment Response Defined by MRI-PDFF or MRE Results and Metabolomic Changes
3.3. Association of the Treatment Response Defined by TE and Metabolomic Changes
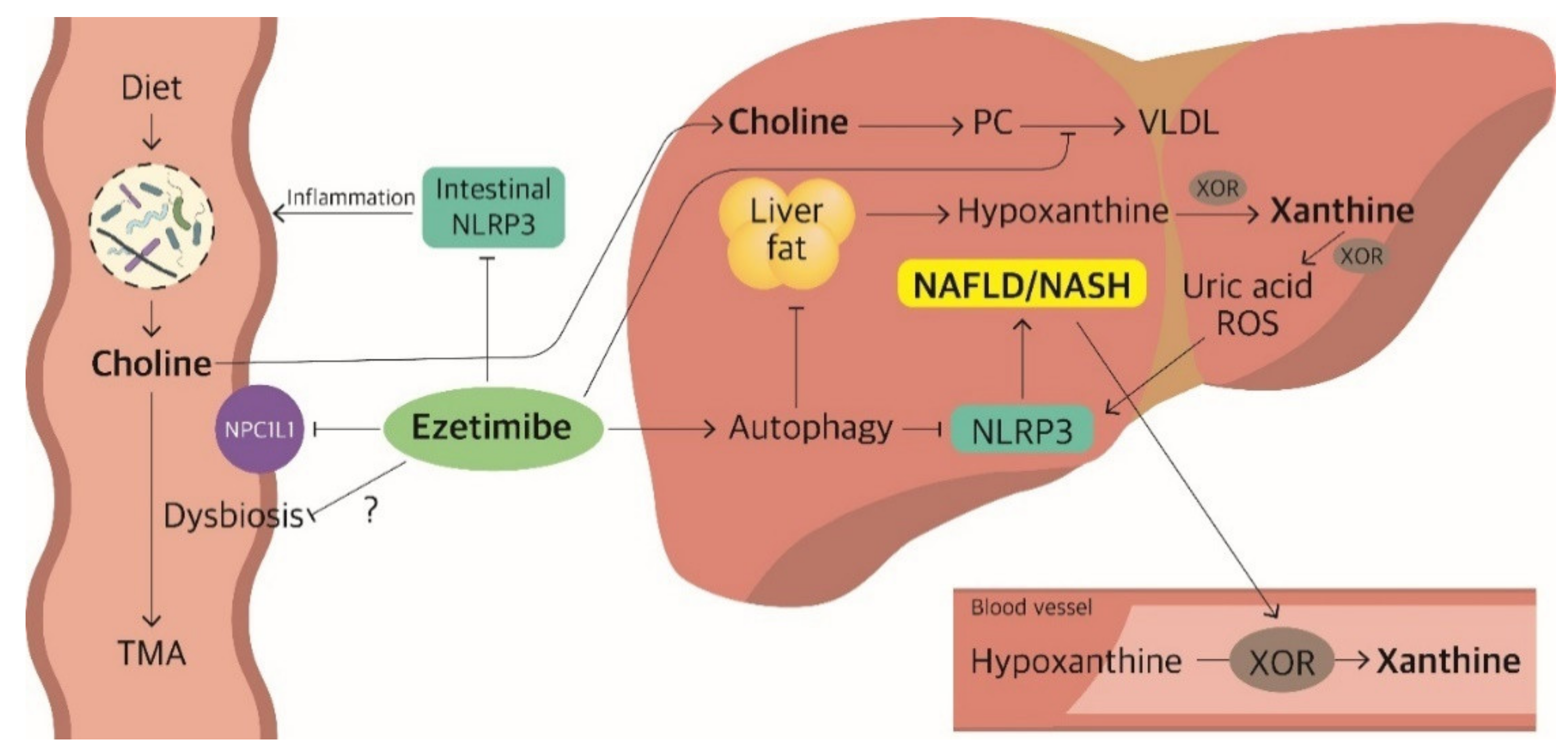
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, J.; Zou, B.; Yeo, Y.H.; Feng, Y.; Xie, X.; Lee, D.H.; Fujii, H.; Wu, Y.; Kam, L.Y.; Ji, F.; et al. Prevalence, incidence, and outcome of non-alcoholic fatty liver disease in Asia, 1999–2019: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2019, 4, 389–398. [Google Scholar] [CrossRef]
- Le, M.H.; Yeo, Y.H.; Li, X.; Li, J.; Zou, B.; Wu, Y.; Ye, Q.; Huang, D.Q.; Zhao, C.; Zhang, J.; et al. 2019 Global NAFLD Prevalence: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Adams, L.A.; Lymp, J.F.; St Sauver, J.; Sanderson, S.O.; Lindor, K.D.; Feldstein, A.; Angulo, P. The natural history of nonalcoholic fatty liver disease: A population-based cohort study. Gastroenterology 2005, 129, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Rinella, M.E.; Sanyal, A.J. Management of NAFLD: A stage-based approach. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Matteoni, C.A.; Younossi, Z.M.; Gramlich, T.; Boparai, N.; Liu, Y.C.; McCullough, A.J. Nonalcoholic fatty liver disease: A spectrum of clinical and pathological severity. Gastroenterology 1999, 116, 1413–1419. [Google Scholar] [CrossRef]
- Loomba, R.; Sanyal, A.J. The global NAFLD epidemic. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 686–690. [Google Scholar] [CrossRef]
- Jarvis, H.; Craig, D.; Barker, R.; Spiers, G.; Stow, D.; Anstee, Q.M.; Hanratty, B. Metabolic risk factors and incident advanced liver disease in non-alcoholic fatty liver disease (NAFLD): A systematic review and meta-analysis of population-based observational studies. PLoS Med. 2020, 17, e1003100. [Google Scholar] [CrossRef]
- Ekstedt, M.; Franzén, L.E.; Mathiesen, U.L.; Thorelius, L.; Holmqvist, M.; Bodemar, G.; Kechagias, S. Long-term follow-up of patients with NAFLD and elevated liver enzymes. Hepatology 2006, 44, 865–873. [Google Scholar] [CrossRef]
- Kang, S.H.; Lee, H.W.; Yoo, J.J.; Cho, Y.; Kim, S.U.; Lee, T.H.; Jang, B.K.; Kim, S.G.; Ahn, S.B.; Kim, H.; et al. KASL clinical practice guidelines: Management of nonalcoholic fatty liver disease. Clin. Mol. Hepatol. 2021, 27, 363–401. [Google Scholar] [CrossRef]
- Bacon, B.R.; Farahvash, M.J.; Janney, C.G.; Neuschwander-Tetri, B.A. Nonalcoholic steatohepatitis: An expanded clinical entity. Gastroenterology 1994, 107, 1103–1109. [Google Scholar] [CrossRef]
- Castera, L.; Friedrich-Rust, M.; Loomba, R. Noninvasive Assessment of Liver Disease in Patients with Nonalcoholic Fatty Liver Disease. Gastroenterology 2019, 156, 1264–1281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: A simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006, 6, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.H.; Kim, D.; Kim, H.J.; Lee, C.H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.H.; Cho, S.H.; Sung, M.W.; et al. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Vallet-Pichard, A.; Mallet, V.; Nalpas, B.; Verkarre, V.; Nalpas, A.; Dhalluin-Venier, V.; Fontaine, H.; Pol, S. FIB-4: An inexpensive and accurate marker of fibrosis in HCV infection. comparison with liver biopsy and fibrotest. Hepatology 2007, 46, 32–36. [Google Scholar] [CrossRef]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The NAFLD fibrosis score: A noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef]
- Park, C.C.; Nguyen, P.; Hernandez, C.; Bettencourt, R.; Ramirez, K.; Fortney, L.; Hooker, J.; Sy, E.; Savides, M.T.; Alquiraish, M.H.; et al. Magnetic Resonance Elastography vs Transient Elastography in Detection of Fibrosis and Noninvasive Measurement of Steatosis in Patients With Biopsy-Proven Nonalcoholic Fatty Liver Disease. Gastroenterology 2017, 152, 598–607. [Google Scholar] [CrossRef] [Green Version]
- Idilman, I.S.; Aniktar, H.; Idilman, R.; Kabacam, G.; Savas, B.; Elhan, A.; Celik, A.; Bahar, K.; Karcaaltincaba, M. Hepatic steatosis: Quantification by proton density fat fraction with MR imaging versus liver biopsy. Radiology 2013, 267, 767–775. [Google Scholar] [CrossRef]
- Lake, A.D.; Novak, P.; Shipkova, P.; Aranibar, N.; Robertson, D.G.; Reily, M.D.; Lehman-McKeeman, L.D.; Vaillancourt, R.R.; Cherrington, N.J. Branched chain amino acid metabolism profiles in progressive human nonalcoholic fatty liver disease. Amino Acids 2015, 47, 603–615. [Google Scholar] [CrossRef]
- Kawanaka, M.; Nishino, K.; Oka, T.; Urata, N.; Nakamura, J.; Suehiro, M.; Kawamoto, H.; Chiba, Y.; Yamada, G. Tyrosine levels are associated with insulin resistance in patients with nonalcoholic fatty liver disease. Hepat. Med. 2015, 7, 29–35. [Google Scholar] [CrossRef] [Green Version]
- Puri, P.; Wiest, M.M.; Cheung, O.; Mirshahi, F.; Sargeant, C.; Min, H.K.; Contos, M.J.; Sterling, R.K.; Fuchs, M.; Zhou, H.; et al. The plasma lipidomic signature of nonalcoholic steatohepatitis. Hepatology 2009, 50, 1827–1838. [Google Scholar] [CrossRef] [Green Version]
- Orešič, M.; Hyötyläinen, T.; Kotronen, A.; Gopalacharyulu, P.; Nygren, H.; Arola, J.; Castillo, S.; Mattila, I.; Hakkarainen, A.; Borra, R.J.; et al. Prediction of non-alcoholic fatty-liver disease and liver fat content by serum molecular lipids. Diabetologia 2013, 56, 2266–2274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, Y.; Rhee, H.; Kim, Y.; Lee, M.; Lee, B.W.; Kang, E.S.; Cha, B.S.; Choi, J.Y.; Lee, Y. Ezetimibe combination therapy with statin for non-alcoholic fatty liver disease: A randomized controlled trial (ESSENTIAL study). BMC Med. 2022, 20, 93. [Google Scholar] [CrossRef] [PubMed]
- Sasso, M.; Beaugrand, M.; de Ledinghen, V.; Douvin, C.; Marcellin, P.; Poupon, R.; Sandrin, L.; Miette, V. Controlled attenuation parameter (CAP): A novel VCTE™ guided ultrasonic attenuation measurement for the evaluation of hepatic steatosis: Preliminary study and validation in a cohort of patients with chronic liver disease from various causes. Ultrasound Med. Biol. 2010, 36, 1825–1835. [Google Scholar] [CrossRef]
- Fabbrini, E.; Mohammed, B.S.; Magkos, F.; Korenblat, K.M.; Patterson, B.W.; Klein, S. Alterations in adipose tissue and hepatic lipid kinetics in obese men and women with nonalcoholic fatty liver disease. Gastroenterology 2008, 134, 424–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ipsen, D.H.; Lykkesfeldt, J.; Tveden-Nyborg, P. Molecular mechanisms of hepatic lipid accumulation in non-alcoholic fatty liver disease. Cell Mol. Life Sci. 2018, 75, 3313–3327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Coker, O.O.; Chu, E.S.H.; Fu, K.; Lau, H.C.H.; Wang, Y.-X.; Chan, A.W.H.; Wei, H.; Yang, X.; Sung, J.J.Y.; et al. Dietary cholesterol drives fatty liver-associated liver cancer by modulating gut microbiota and metabolites. Gut 2021, 70, 761. [Google Scholar] [CrossRef]
- Garcia-Calvo, M.; Lisnock, J.; Bull, H.G.; Hawes, B.E.; Burnett, D.A.; Braun, M.P.; Crona, J.H.; Davis, H.R., Jr.; Dean, D.C.; Detmers, P.A.; et al. The target of ezetimibe is Niemann-Pick C1-Like 1 (NPC1L1). Proc. Natl. Acad. Sci. USA 2005, 102, 8132–8137. [Google Scholar] [CrossRef] [Green Version]
- Nakade, Y.; Murotani, K.; Inoue, T.; Kobayashi, Y.; Yamamoto, T.; Ishii, N.; Ohashi, T.; Ito, K.; Fukuzawa, Y.; Yoneda, M. Ezetimibe for the treatment of non-alcoholic fatty liver disease: A meta-analysis. Hepatol. Res. 2017, 47, 1417–1428. [Google Scholar] [CrossRef]
- Simon, T.G.; Corey, K.E.; Cannon, C.P.; Blazing, M.; Park, J.G.; O’Donoghue, M.L.; Chung, R.T.; Giugliano, R.P. The nonalcoholic fatty liver disease (NAFLD) fibrosis score, cardiovascular risk stratification and a strategy for secondary prevention with ezetimibe. Int. J. Cardiol. 2018, 270, 245–252. [Google Scholar] [CrossRef]
- Caparrós-Martín, J.A.; Lareu, R.R.; Ramsay, J.P.; Peplies, J.; Reen, F.J.; Headlam, H.A.; Ward, N.C.; Croft, K.D.; Newsholme, P.; Hughes, J.D.; et al. Statin therapy causes gut dysbiosis in mice through a PXR-dependent mechanism. Microbiome 2017, 5, 95. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.; Vonk, R.J.; Slooff, M.J.; Kuipers, F.; Smit, M.J. Differences in propionate-induced inhibition of cholesterol and triacylglycerol synthesis between human and rat hepatocytes in primary culture. Br. J. Nutr. 1995, 74, 197–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haghikia, A.; Zimmermann, F.; Schumann, P.; Jasina, A.; Roessler, J.; Schmidt, D.; Heinze, P.; Kaisler, J.; Nageswaran, V.; Aigner, A.; et al. Propionate attenuates atherosclerosis by immune-dependent regulation of intestinal cholesterol metabolism. Eur. Heart J. 2021, 43, 518–533. [Google Scholar] [CrossRef] [PubMed]
- Bartolomaeus, H.; Balogh, A.; Yakoub, M.; Homann, S.; Markó, L.; Höges, S.; Tsvetkov, D.; Krannich, A.; Wundersitz, S.; Avery, E.G.; et al. Short-Chain Fatty Acid Propionate Protects From Hypertensive Cardiovascular Damage. Circulation 2019, 139, 1407–1421. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Song, X.; Zhou, H.; Zhou, X.; Xia, Y.; Dong, X.; Zhong, W.; Tang, S.; Wang, L.; Wen, S.; et al. Gut Microbiome Associates with Lipid-Lowering Effect of Rosuvastatin in Vivo. Front. Microbiol. 2018, 9, 530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Lee, H.; An, J.; Song, Y.; Lee, C.-K.; Kim, K.; Kong, H. Alterations in Gut Microbiota by Statin Therapy and Possible Intermediate Effects on Hyperglycemia and Hyperlipidemia. Front. Microbiol. 2019, 10, 1947. [Google Scholar] [CrossRef] [Green Version]
- Rebalka, I.A.; Cao, A.W.; May, L.L.; Tarnopolsky, M.A.; Hawke, T.J. Statin administration activates system xC− in skeletal muscle: A potential mechanism explaining statin-induced muscle pain. Am. J. Physiol. Cell Physiol. 2019, 317, C894–C899. [Google Scholar] [CrossRef]
- Xu, C.; Wan, X.; Xu, L.; Weng, H.; Yan, M.; Miao, M.; Sun, Y.; Xu, G.; Dooley, S.; Li, Y.; et al. Xanthine oxidase in non-alcoholic fatty liver disease and hyperuricemia: One stone hits two birds. J. Hepatol. 2015, 62, 1412–1419. [Google Scholar] [CrossRef]
- Furuhashi, M.; Koyama, M.; Higashiura, Y.; Murase, T.; Nakamura, T.; Matsumoto, M.; Sakai, A.; Ohnishi, H.; Tanaka, M.; Saitoh, S.; et al. Differential regulation of hypoxanthine and xanthine by obesity in a general population. J. Diabetes Investig. 2020, 11, 878–887. [Google Scholar] [CrossRef] [Green Version]
- Nagao, H.; Nishizawa, H.; Tanaka, Y.; Fukata, T.; Mizushima, T.; Furuno, M.; Bamba, T.; Tsushima, Y.; Fujishima, Y.; Kita, S.; et al. Hypoxanthine Secretion from Human Adipose Tissue and its Increase in Hypoxia. Obesity 2018, 26, 1168–1178. [Google Scholar] [CrossRef] [Green Version]
- Kawachi, Y.; Fujishima, Y.; Nishizawa, H.; Nakamura, T.; Akari, S.; Murase, T.; Saito, T.; Miyazaki, Y.; Nagao, H.; Fukuda, S.; et al. Increased plasma XOR activity induced by NAFLD/NASH and its possible involvement in vascular neointimal proliferation. JCI Insight 2021, 6, e144762. [Google Scholar] [CrossRef]
- Kim, S.H.; Kim, G.; Han, D.H.; Lee, M.; Kim, I.; Kim, B.; Kim, K.H.; Song, Y.M.; Yoo, J.E.; Wang, H.J.; et al. Ezetimibe ameliorates steatohepatitis via AMP activated protein kinase-TFEB-mediated activation of autophagy and NLRP3 inflammasome inhibition. Autophagy 2017, 13, 1767–1781. [Google Scholar] [CrossRef] [PubMed]
- Anstee, Q.M.; Goldin, R.D. Mouse models in non-alcoholic fatty liver disease and steatohepatitis research. Int. J. Exp. Pathol. 2006, 87, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Vance, D.E. Phosphatidylcholine and choline homeostasis. J. Lipid Res. 2008, 49, 1187–1194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, D.; Wei, C.; Chen, L.; Huang, J.; Yang, S.; Diehl, A.M. Oxidative DNA damage and DNA repair enzyme expression are inversely related in murine models of fatty liver disease. Am. J. Physiol. Gastrointest. Liver Physiol. 2004, 287, G1070–G1077. [Google Scholar] [CrossRef]
- Kolodziejczyk, A.A.; Zheng, D.; Shibolet, O.; Elinav, E. The role of the microbiome in NAFLD and NASH. EMBO Mol. Med. 2019, 11, e9302. [Google Scholar] [CrossRef]
- Leung, C.; Rivera, L.; Furness, J.B.; Angus, P.W. The role of the gut microbiota in NAFLD. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 412–425. [Google Scholar] [CrossRef]
- Mao, L.; Kitani, A.; Strober, W.; Fuss, I.J. The Role of NLRP3 and IL-1β in the Pathogenesis of Inflammatory Bowel Disease. Front. Immunol. 2018, 9, 2566. [Google Scholar] [CrossRef] [Green Version]
- Abratte, C.M.; Wang, W.; Li, R.; Axume, J.; Moriarty, D.J.; Caudill, M.A. Choline status is not a reliable indicator of moderate changes in dietary choline consumption in premenopausal women. J. Nutr. Biochem. 2009, 20, 62–69. [Google Scholar] [CrossRef]
- Zuo, H.; Svingen, G.F.T.; Tell, G.S.; Ueland, P.M.; Vollset, S.E.; Pedersen, E.R.; Ulvik, A.; Meyer, K.; Nordrehaug, J.E.; Nilsen, D.W.T.; et al. Plasma Concentrations and Dietary Intakes of Choline and Betaine in Association with Atrial Fibrillation Risk: Results From 3 Prospective Cohorts with Different Health Profiles. J. Am. Heart Assoc. 2018, 7, e008190. [Google Scholar] [CrossRef]
- Naples, M.; Baker, C.; Lino, M.; Iqbal, J.; Hussain, M.M.; Adeli, K. Ezetimibe ameliorates intestinal chylomicron overproduction and improves glucose tolerance in a diet-induced hamster model of insulin resistance. Am. J. Physiol. Gastrointest. Liver Physiol. 2012, 302, G1043–G1052. [Google Scholar] [CrossRef] [Green Version]
- Bozzetto, L.; Annuzzi, G.; Corte, G.D.; Patti, L.; Cipriano, P.; Mangione, A.; Riccardi, G.; Rivellese, A.A. Ezetimibe beneficially influences fasting and postprandial triglyceride-rich lipoproteins in type 2 diabetes. Atherosclerosis 2011, 217, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Telford, D.E.; Sutherland, B.G.; Edwards, J.Y.; Andrews, J.D.; Barrett, P.H.; Huff, M.W. The molecular mechanisms underlying the reduction of LDL apoB-100 by ezetimibe plus simvastatin. J. Lipid Res. 2007, 48, 699–708. [Google Scholar] [CrossRef] [Green Version]
- Sherriff, J.L.; O’Sullivan, T.A.; Properzi, C.; Oddo, J.L.; Adams, L.A. Choline, Its Potential Role in Nonalcoholic Fatty Liver Disease, and the Case for Human and Bacterial Genes. Adv. Nutr. 2016, 7, 5–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciucanu, C.I.; Olariu, S.; Vlad, D.C.; Dumitraşcu, V. Effect of rosuvastatin on the concentration of each fatty acid in the fraction of free fatty acids and total lipids in human plasma: The role of cholesterol homeostasis. Biochem. Biophys. Rep. 2020, 24, 100822. [Google Scholar] [CrossRef] [PubMed]
- Nozue, T.; Michishita, I. Statin treatment alters serum n-3 to n-6 polyunsaturated fatty acids ratio in patients with dyslipidemia. Lipids Health Dis. 2015, 14, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krähenbühl, L.; Reichen, J.; Talos, C.; Krähenbühl, S. Benzoic acid metabolism reflects hepatic mitochondrial function in rats with long-term extrahepatic cholestasis. Hepatology 1997, 25, 278–283. [Google Scholar] [CrossRef]
- Hemming, A.W.; Gallinger, S.; Greig, P.D.; Cattral, M.S.; Langer, B.; Taylor, B.R.; Verjee, Z.; Giesbrecht, E.; Nakamachi, Y.; Furuya, K.N. The hippurate ratio as an indicator of functional hepatic reserve for resection of hepatocellular carcinoma in cirrhotic patients. J. Gastrointest. Surg. 2001, 5, 316–321. [Google Scholar] [CrossRef]
- Brial, F.; Chilloux, J.; Nielsen, T.; Vieira-Silva, S.; Falony, G.; Andrikopoulos, P.; Olanipekun, M.; Hoyles, L.; Djouadi, F.; Neves, A.L.; et al. Human and preclinical studies of the host–gut microbiome co-metabolite hippurate as a marker and mediator of metabolic health. Gut 2021, 70, 2105–2114. [Google Scholar] [CrossRef]
- Pallister, T.; Jackson, M.A.; Martin, T.C.; Zierer, J.; Jennings, A.; Mohney, R.P.; MacGregor, A.; Steves, C.J.; Cassidy, A.; Spector, T.D.; et al. Hippurate as a metabolomic marker of gut microbiome diversity: Modulation by diet and relationship to metabolic syndrome. Sci. Rep. 2017, 7, 13670. [Google Scholar] [CrossRef] [Green Version]
- Hoyles, L.; Fernández-Real, J.M.; Federici, M.; Serino, M.; Abbott, J.; Charpentier, J.; Heymes, C.; Luque, J.L.; Anthony, E.; Barton, R.H.; et al. Molecular phenomics and metagenomics of hepatic steatosis in non-diabetic obese women. Nat. Med. 2018, 24, 1070–1080. [Google Scholar] [CrossRef]
- Dias, A.M.; Cordeiro, G.; Estevinho, M.M.; Veiga, R.; Figueira, L.; Reina-Couto, M.; Magro, F. Gut bacterial microbiome composition and statin intake—A systematic review. Pharmacol. Res. Perspect. 2020, 8, e00601. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment | Ezetimibe + Statin Group (n = 31) | Statin Group (n = 32) | ||||
|---|---|---|---|---|---|---|
| Response in liver fat * | Good response (n = 16) | Non-response (n = 15) | p value | Good response (n = 14) | Non-response (n = 18) | p value |
| Age, years | 46.7 [43.5–55.0] | 49.4 [43.8–55.6] | 0.68 | 52.5 [45.3–56.8] | 59.4 [42.2–68.2] | 0.16 |
| Sex | 0.30 | >0.99 | ||||
| Male (%) | 9 (56%) | 12 (80%) | 7 (50%) | 10 (56%) | ||
| Female (%) | 7 (44%) | 3 (20%) | 7 (50%) | 8 (44%) | ||
| BMI, kg/m2 | 28.9 [25.0–31.7] | 29.5 [24.9–30.8] | 0.98 | 27.6 [26.7–28.7] | 28.4 [27.8–31.0] | 0.11 |
| HTN | 0.36 | >0.99 | ||||
| No (%) | 7 (44%) | 10 (67%) | 9 (64%) | 12 (67%) | ||
| Yes (%) | 9 (56%) | 5 (33%) | 5 (36%) | 6 (33%) | ||
| History of DM | 0.18 | >0.99 | ||||
| No (%) | 2 (13%) | 6 (40%) | 4 (29%) | 5 (28%) | ||
| Yes (%) | 14 (88%) | 9 (60%) | 10 (71%) | 13 (72%) | ||
| Image findings | ||||||
| MRI-PDFF, % | 17.9 [12.5–23.6] | 15.4 [12.9–20.1] | 0.45 | 13.1 [11.2–16.0] | 12.4 [10.4–17.9] | >0.99 |
| CAP, dB/m | 327.5 [315.5–335.0] | 327.0 [287.0–333.0] | 0.31 | 305.0 [284.0–325.0] | 324.5 [299.0–333.0] | 0.14 |
| MR elastography, kPa | 2.1 [1.8–2.5] | 1.8 [1.6–2.4] | 0.14 | 1.9 [1.7–2.7] | 2.2 [1.9–2.4] | 0.28 |
| LSM, kPa | 6.3 [5.4–7.4] | 5.7 [4.4–8.4] | 0.62 | 6.2 [5.1–6.8] | 6.8 [4.9–8.7] | 0.23 |
| Lipid profile | ||||||
| Free fatty acid, mmol/L | 472.0 [397.5–569.0] | 575.0 [429.5–724.5] | 0.29 | 620.0 [550.0–750.0] | 426.0 [334.0–515.0] | 0.004 |
| Acetic acid, μM | 69.0 [51.4–91.9] | 93.4 [66.7–159.2] | 0.03 | 97.6 [67.8–162.7] | 68.2 [61.0–101.9] | 0.20 |
| Butyric acid, μM | 2.7 [2.2–3.9] | 2.8 [0.8–3.5] | 0.84 | 2.5 [1.0–3.4] | 2.8 [0.8–3.6] | 0.99 |
| Propionic acid, μM | 0.6 [0.6–2.4] | 0.9 [0.6–2.8] | 0.62 | 0.8 [0.6–2.2] | 1.8 [0.7–3.8] | 0.27 |
| Total cholesterol, mg/dL | 189.5 [162.0–204.5] | 218.0 [187.0–244.5] | 0.06 | 209.0 [186.0–254.0] | 196.5 [188.0–214.0] | 0.46 |
| HDL cholesterol, mg/dL | 42.5 [36.0–47.5] | 49.0 [40.5–54.5] | 0.10 | 43.5 [40.0–49.0] | 42.0 [39.0–46.0] | 0.61 |
| LDL cholesterol, mg/dL | 104.8 [81.1–121.2] | 126.4 [102.0–162.0] | 0.14 | 114.3 [86.4–160.2] | 108.5 [101.4–139.6] | 0.99 |
| Triglycerides, mg/dL | 175.0 [128.5–257.5] | 158.0 [125.0–183.0] | 0.49 | 272.5 [218.0–309.0] | 210.5 [146.0–273.0] | 0.10 |
| (a) Steatosis | Metabolite | % Change from the Baseline [Q1-Q3] | p Value | FDR p Value | |
|---|---|---|---|---|---|
| Good Responder | Non-Responder | ||||
| Ezetimibe + statin | Xanthine | −21.4 [−59.1 to +10.4] | +19.5 [−7.3 to +64.9] | 0.01 | 0.02 |
| Statin | TG 20:5_36:2 | −43.5 [−51.1 to −26.5] | +14.2 [−15.0 to +92.3] | <0.001 | 0.04 |
| TG 18:1_38:6 | −53.2 [−63.2 to −42.4] | −13.8 [−37.2 to +23.3] | <0.001 | 0.04 | |
| C2 | −22.2 [−30.0 to −17.1] | +5.4 [−12.3 to +29.5] | <0.001 | 0.007 | |
| FA 18:2 | −39.0 [−60.3 to −6.3] | +8.6 [−18.1 to +40.0] | 0.001 | 0.009 | |
| FA 18:1 | −42.9 [−51.4 to −19.1] | +15.8 [−28.1 to +52.3] | 0.003 | 0.009 | |
| DHA | −36.1 [−46.0 to −17.4] | +13.3 [−20.5 to +78.2] | 0.009 | 0.02 | |
| (b) Stiffness | Metabolite | % Change from the Baseline [Q1-Q3] | p Value | FDR p Value | |
| Good Responder | Non-Responder | ||||
| Ezetimibe + statin | Xanthine | −21.4 [−59.1 to +10.4] | +19.5 [−7.3 to +64.9] | 0.01 | 0.02 |
| Statin | HexCer(d18:2/16:0) | +81.0 [−21.7 to +107.4] | −25.6 [−49.1 to −9.3] | 0.003 | 0.07 |
| Hippuric acid | +40.2 [−11.0 to +391.1] | −28.0 [−48.0 to +12.5] | 0.006 | 0.02 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.S.; Cho, Y.; Kim, H.; Hwang, H.; Cho, J.W.; Lee, Y.-h.; Lee, S.-G. Association of Metabolomic Change and Treatment Response in Patients with Non-Alcoholic Fatty Liver Disease. Biomedicines 2022, 10, 1216. https://doi.org/10.3390/biomedicines10061216
Lee KS, Cho Y, Kim H, Hwang H, Cho JW, Lee Y-h, Lee S-G. Association of Metabolomic Change and Treatment Response in Patients with Non-Alcoholic Fatty Liver Disease. Biomedicines. 2022; 10(6):1216. https://doi.org/10.3390/biomedicines10061216
Chicago/Turabian StyleLee, Kwang Seob, Yongin Cho, Hongkyung Kim, Hyunkyeong Hwang, Jin Won Cho, Yong-ho Lee, and Sang-Guk Lee. 2022. "Association of Metabolomic Change and Treatment Response in Patients with Non-Alcoholic Fatty Liver Disease" Biomedicines 10, no. 6: 1216. https://doi.org/10.3390/biomedicines10061216