
Altered Ocular Surface Health Status and Tear Film Immune Profile Due to Prolonged Daily Mask Wear in Health Care Workers


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Tear Fluid Collection
2.3. Tear Soluble Factor Measurements
2.4. Ocular Surface Immune Cell Collection
2.5. Ocular Surface Immune Cell Phenotyping by Flow Cytometry
2.6. Cell Culture and Explant Culture
2.7. Osmolarity and pH Measurements
2.8. Quantitative PCR
2.9. Mucin Measurement
2.10. Statistical Analysis
3. Results
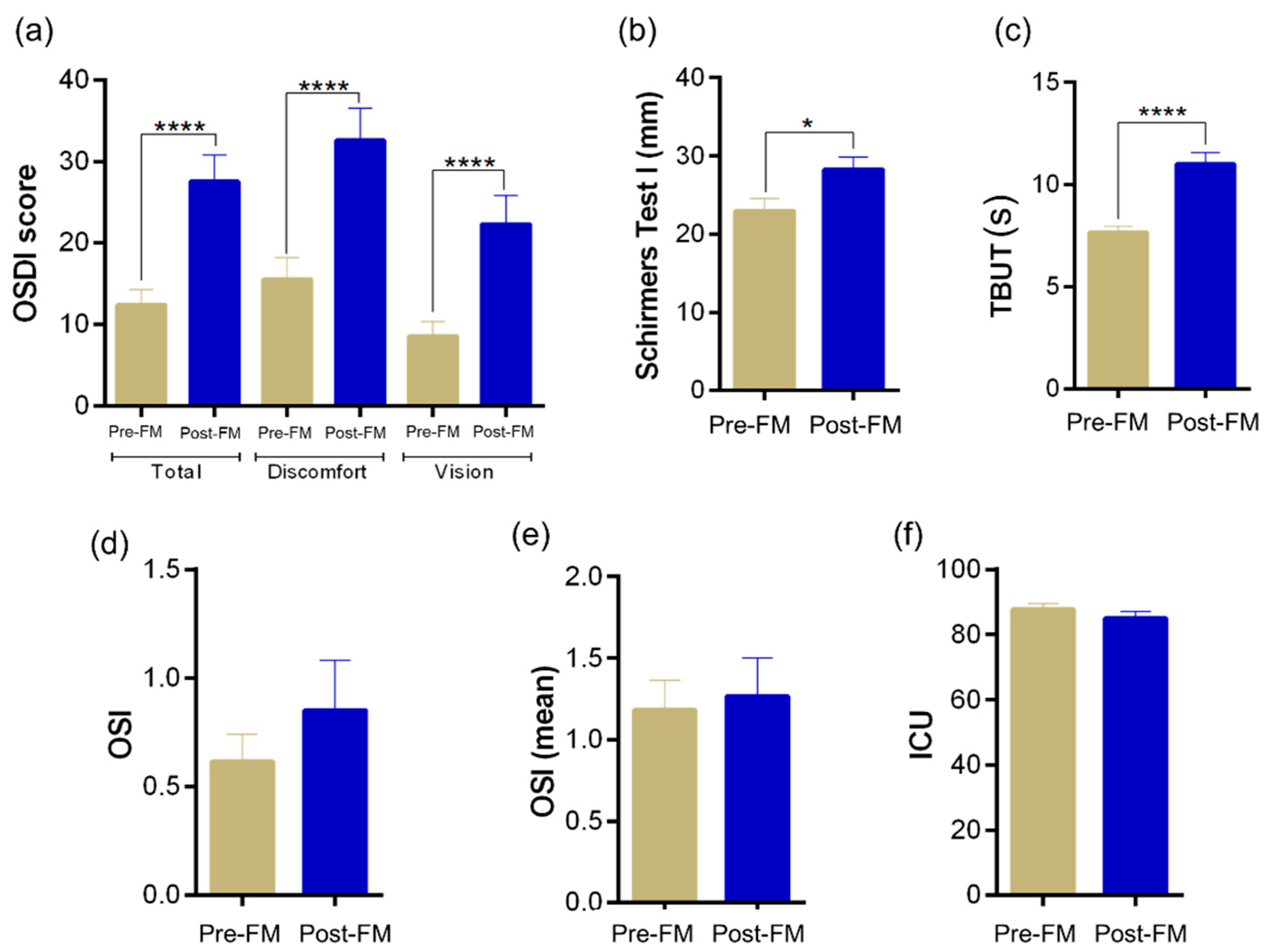
3.1. Ocular Surface Clinical Indices
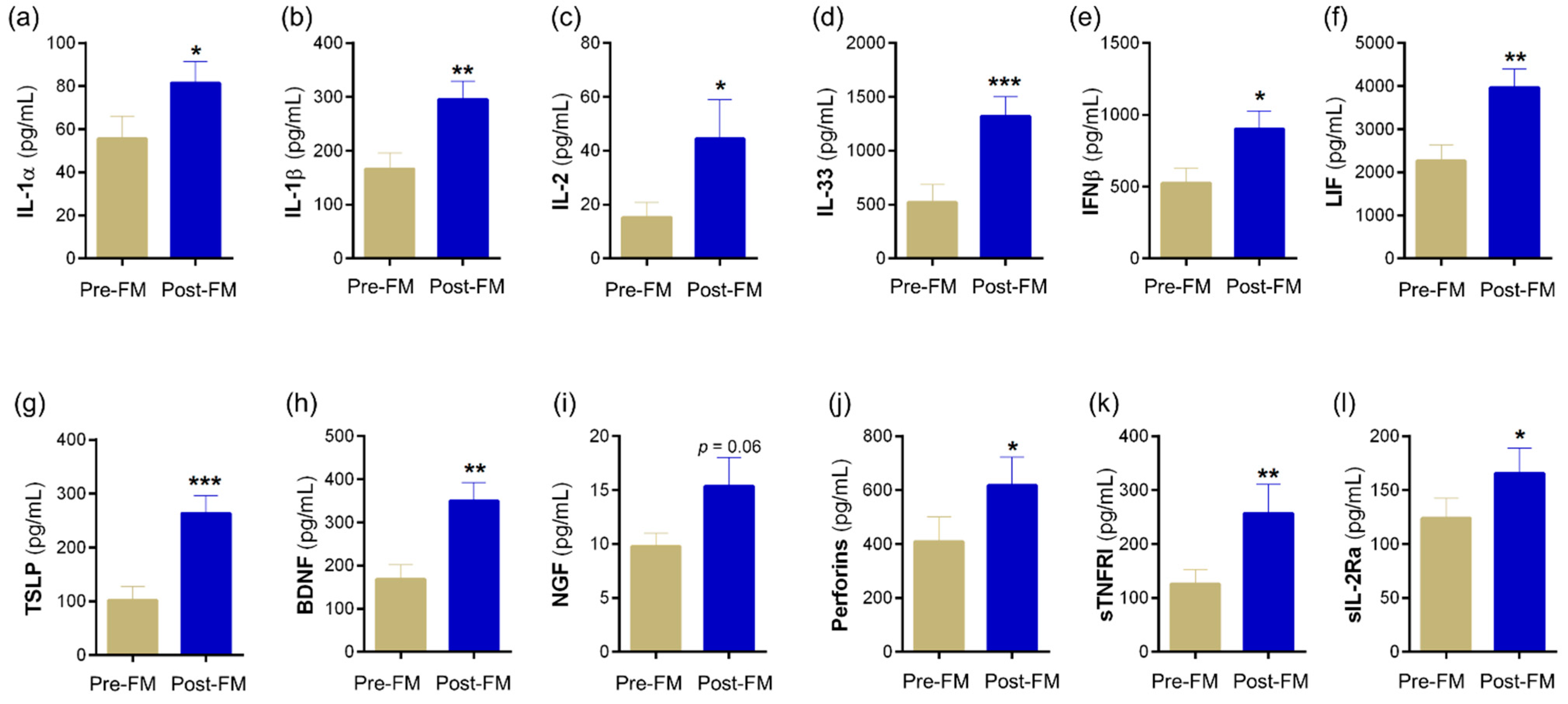
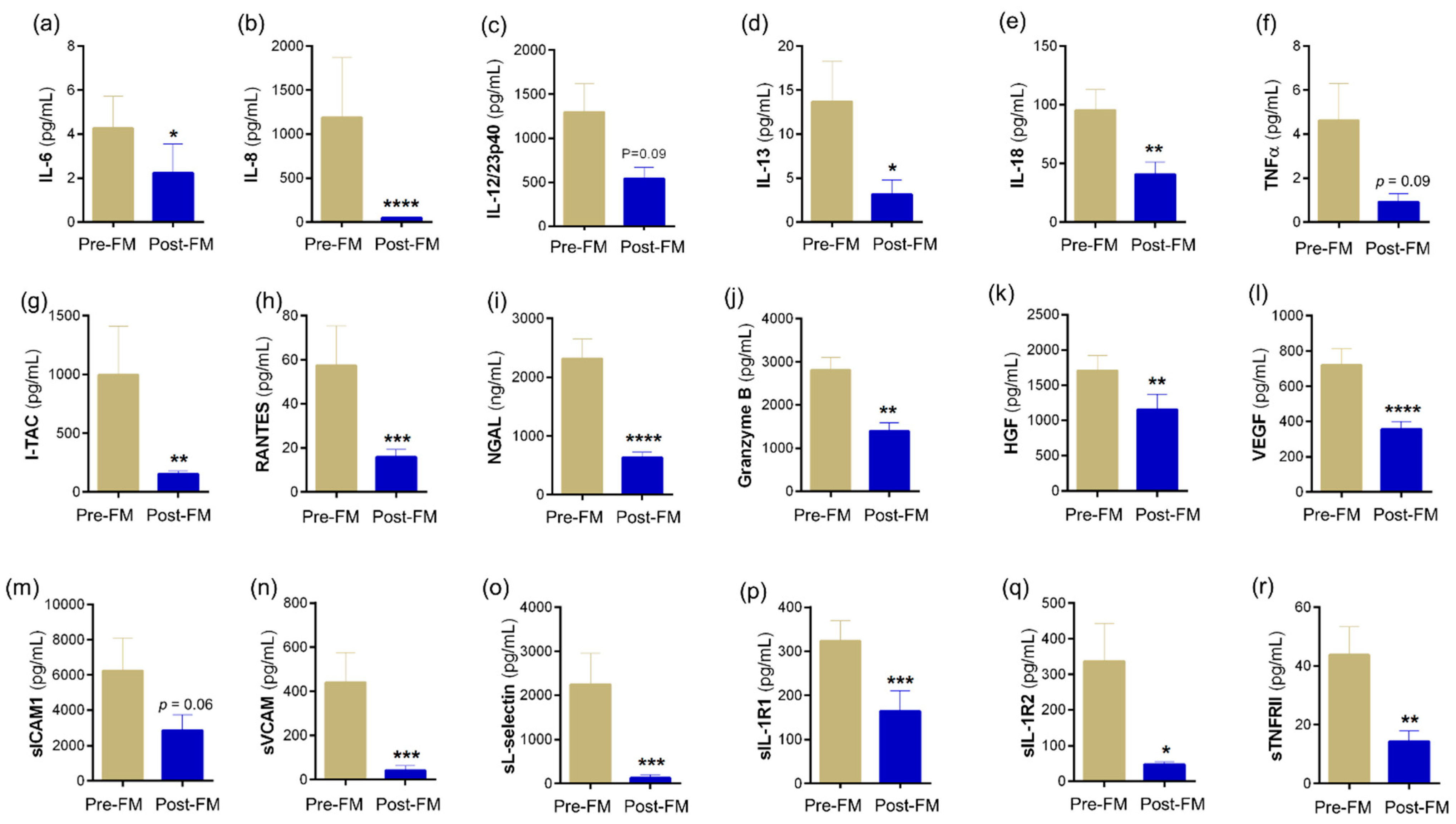
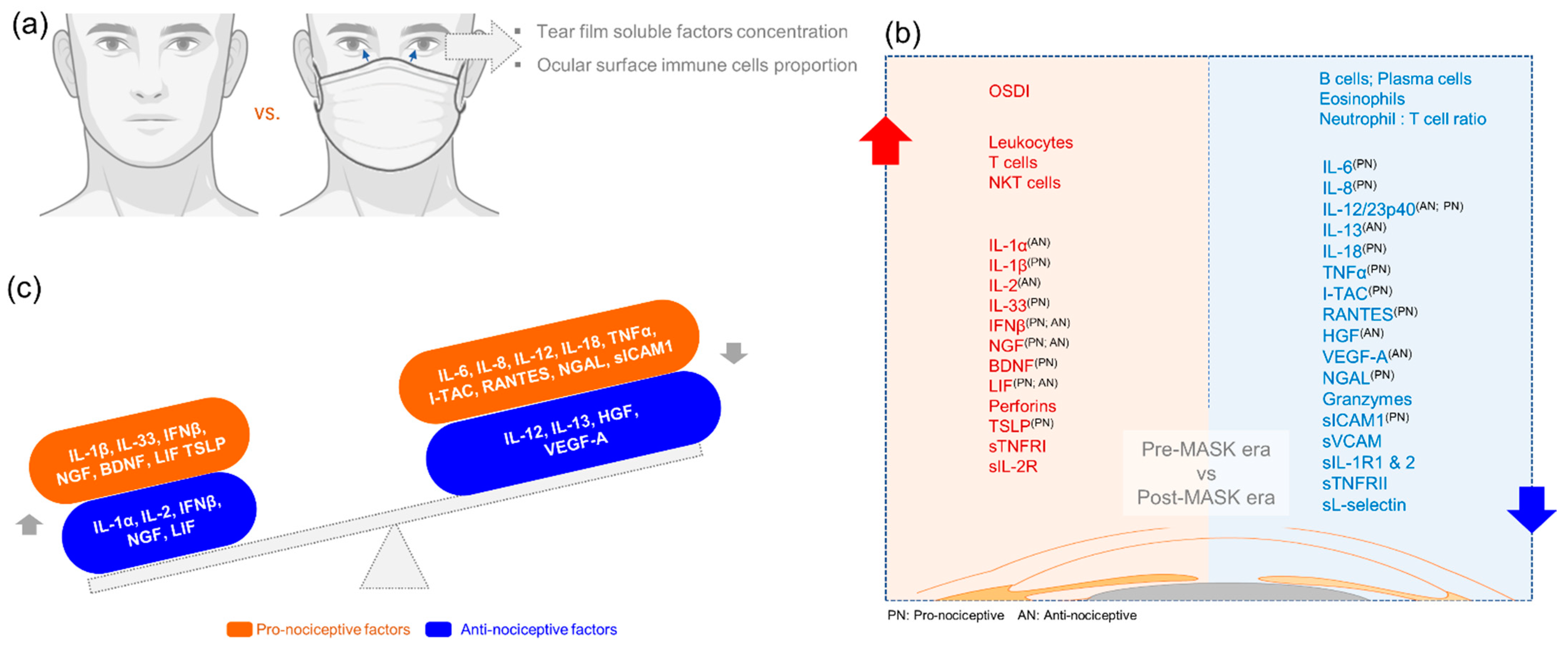
3.2. Tear Soluble Factors Indicate a Skewed Inflammatory Profile Post Mask Wear
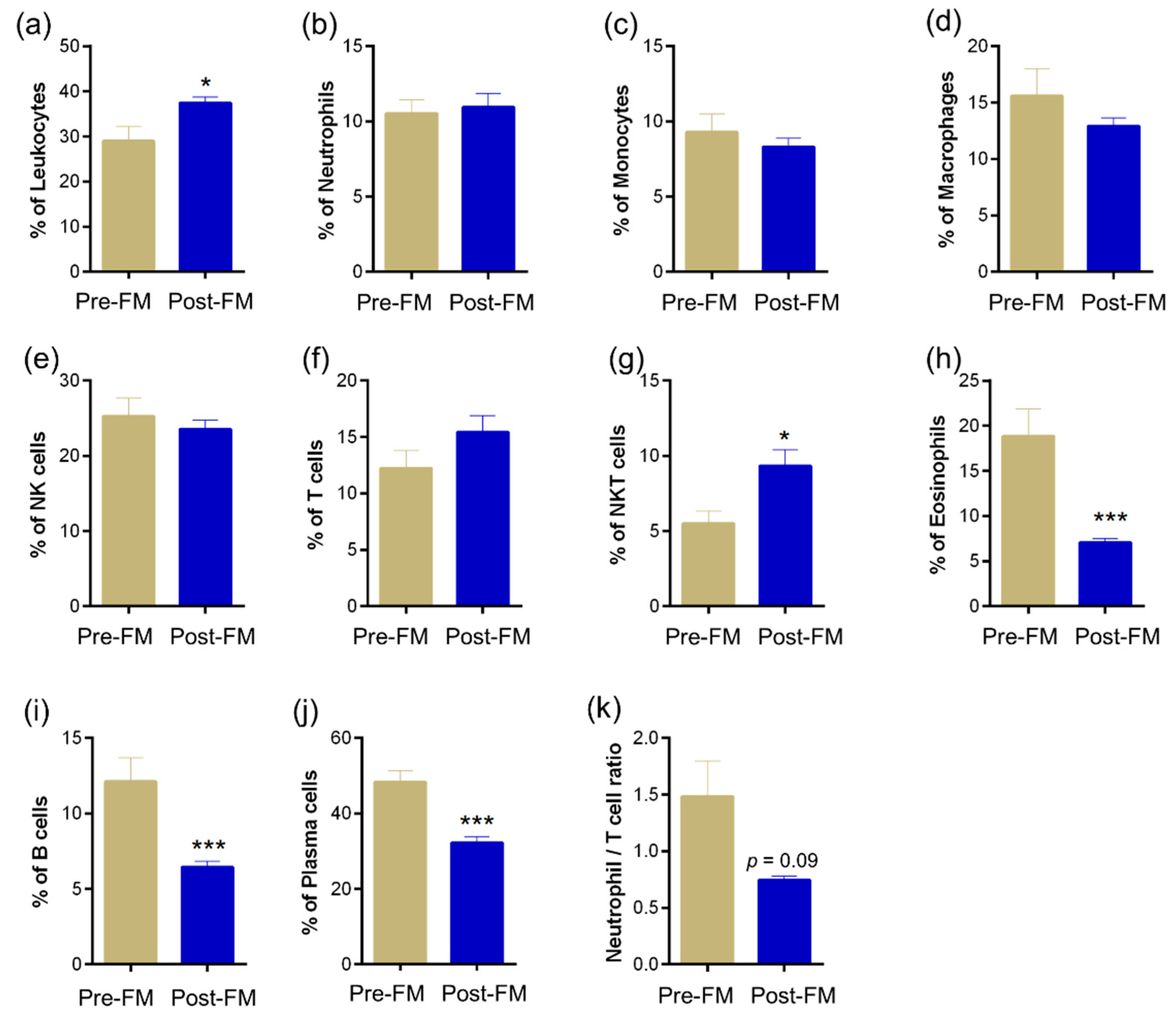
3.3. Ocular Surface Immune Cell Profile Reveals Significant Changes Due to Mask Wear
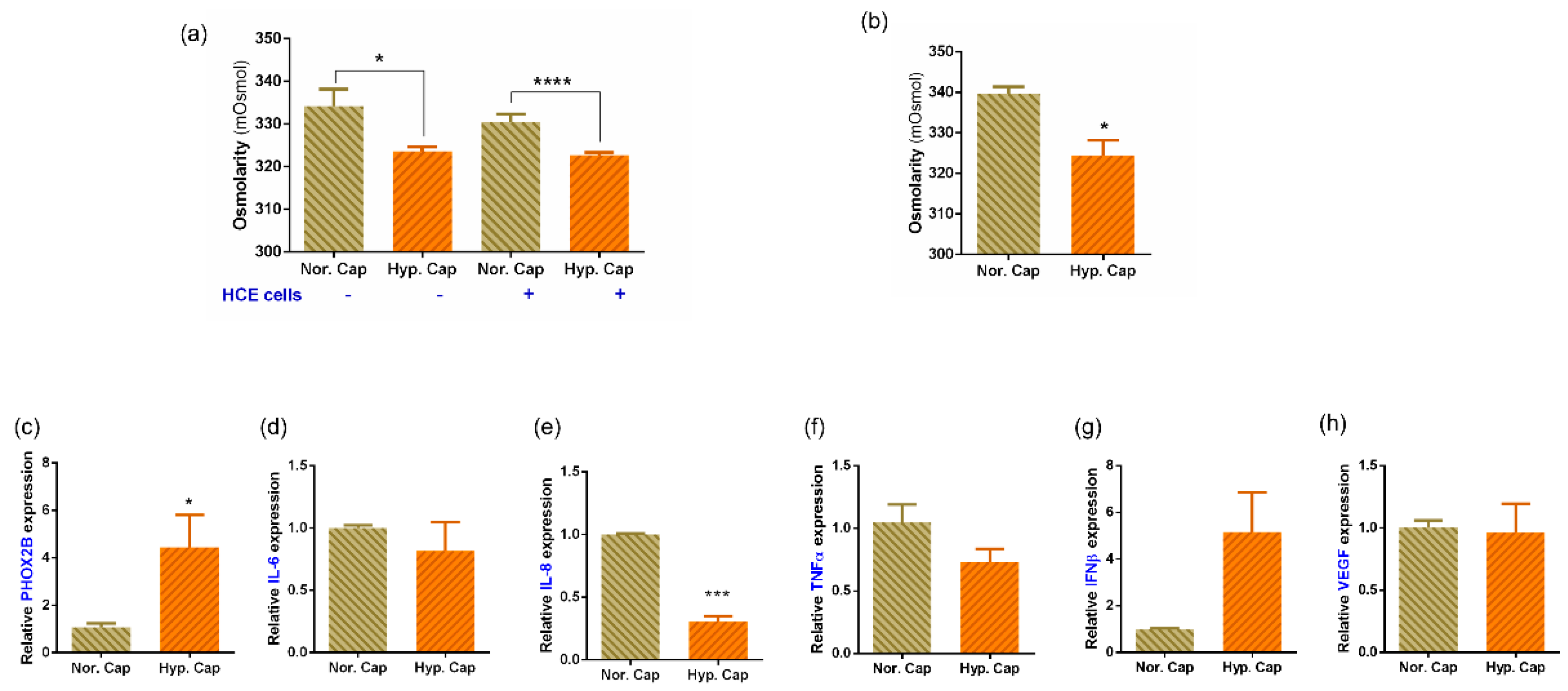
3.4. Exposure to 20% CO2 Induces a Hypercapnic Response and Reduces Osmolarity in In Vitro and Ex Vivo Cultures
3.5. Hypercapnia Altered Inflammatory Profile from Human Primary Ex Vivo Cultures
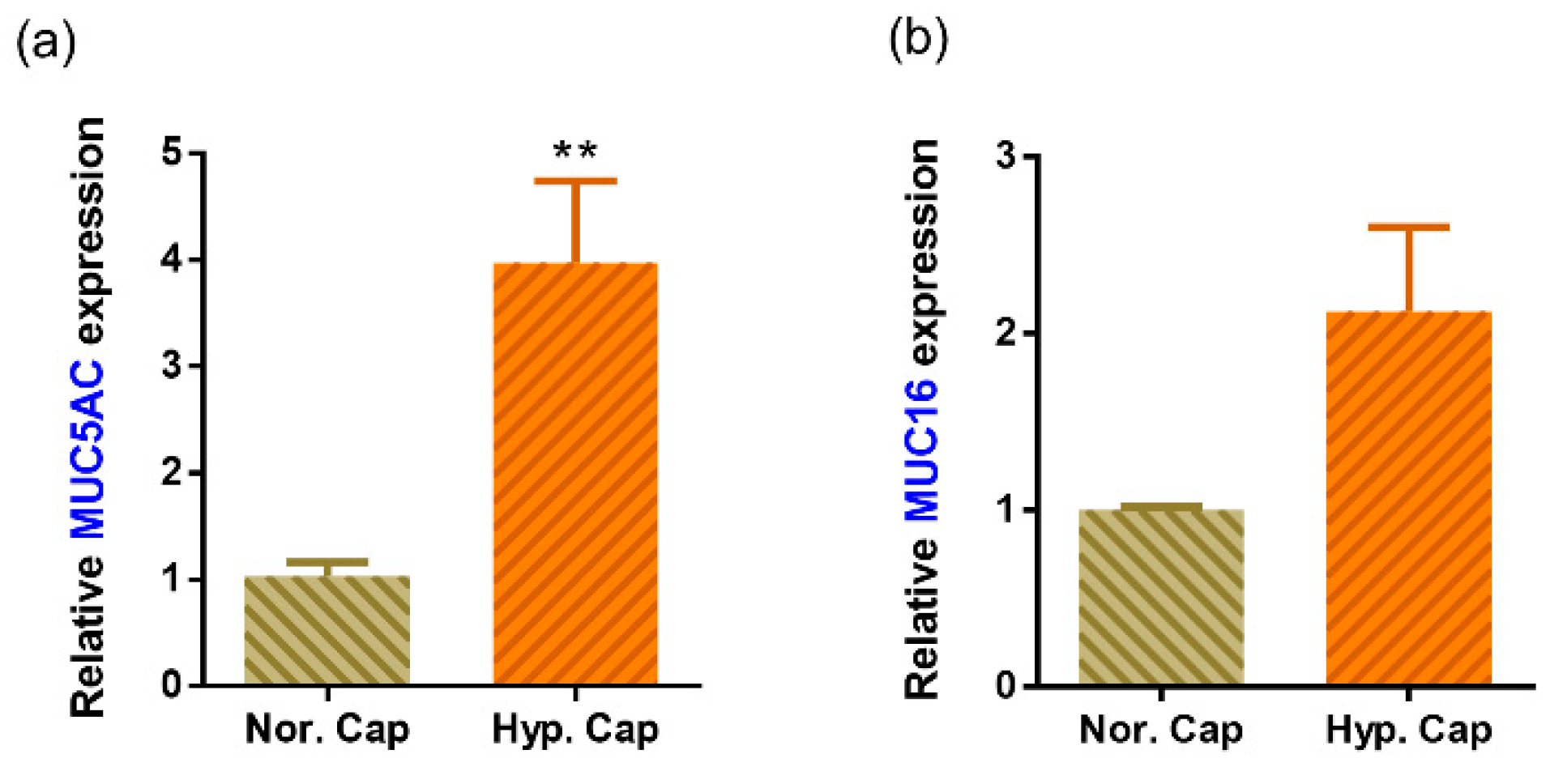
3.6. Hypercapnia Is Associated with Increased Mucin Production
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.U.; Kumar, D.T.; Christopher, B.P.; Doss, C.G.P. The Rise and Impact of COVID-19 in India. Front. Med. 2020, 7, 250. [Google Scholar] [CrossRef] [PubMed]
- Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). COVID-19 Dashboard. 2021. Available online: https://coronavirus.jhu.edu/map.html (accessed on 8 March 2022).
- Shetty, R.; Lalgudi, V.G.; Khamar, P.; Gupta, K.; Sethu, S.; Nair, A.; Honavar, S.G.; Ghosh, A.; D’Souza, S. Potential ocular and systemic COVID-19 prophylaxis approaches for healthcare professionals. Indian J. Ophthalmol. 2020, 68, 1349–1356. [Google Scholar] [CrossRef] [PubMed]
- Desai, A.N.; Aronoff, D.M. Masks and Coronavirus Disease 2019 (COVID-19). JAMA 2020, 323, 2103. [Google Scholar] [CrossRef] [PubMed]
- Sengupta, S.; Honavar, S.G.; Sachdev, M.S.; Sharma, N.; Kumar, A.; Ram, J.; Shetty, R.; Rao, G.S.; Ramasamy, K.; Khanna, R.; et al. All India Ophthalmological Society-Indian Journal of Ophthalmology consensus statement on preferred practices during the COVID-19 pandemic. Indian J. Ophthalmol. 2020, 68, 711–724. [Google Scholar] [CrossRef]
- Chodosh, J. Important Coronavirus Updates for Ophthalmologists. Available online: https://www.aao.org/headline/alert-important-coronavirus-context (accessed on 11 March 2021).
- Gandhi, M.; Yokoe, D.S.; Havlir, D.V. Asymptomatic Transmission, the Achilles’ Heel of Current Strategies to Control COVID-19. N. Engl. J. Med. 2020, 382, 2158–2160. [Google Scholar] [CrossRef]
- CDC. Interim Operational Considerations for Public Health Management of Healthcare Workers Exposed to or with Suspected or Confirmed COVID-19: Non-U.S. Healthcare Settings. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/non-us-settings/public-health-management-hcw-exposed.html (accessed on 11 March 2021).
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Qaseem, A.; Etxeandia-Ikobaltzeta, I.; Yost, J.; Miller, M.C.; Abraham, G.M.; Obley, A.J.; Forciea, M.A.; Jokela, J.A.; Humphrey, L.L. Use of N95, Surgical, and Cloth Masks to Prevent COVID-19 in Health Care and Community Settings: Living Practice Points from the American College of Physicians (Version 1). Ann. Intern. Med. 2020, 173, 642–649. [Google Scholar] [CrossRef]
- Boccardo, L. Self-reported symptoms of mask-associated dry eye: A survey study of 3,605 people. Contact Lens Anterior Eye 2021, 45, 101408. [Google Scholar] [CrossRef]
- Moshirfar, M.; West, W.B.; Marx, D.P. Face Mask-Associated Ocular Irritation and Dryness. Ophthalmol. Ther. 2020, 9, 397–400. [Google Scholar] [CrossRef]
- Smith, D.; Pysanenko, A.; Spanel, P. The quantification of carbon dioxide in humid air and exhaled breath by selected ion flow tube mass spectrometry. Rapid Commun. Mass Spectrom. 2009, 23, 1419–1425. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Chacko, B.K.; Ricksecker, A.; Shingarev, R.; Andrews, E.; Patel, R.P.; Lang, J.D. Modulatory effects of hypercapnia on in vitro and in vivo pulmonary endothelial-neutrophil adhesive responses during inflammation. Cytokine 2008, 44, 108–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pandey, S.K.; Sharma, V. Mask-associated dry eye disease and dry eye due to prolonged screen time: Are we heading towards a new dry eye epidemic during the COVID-19 era? Indian J. Ophthalmol. 2021, 69, 448–449. [Google Scholar] [CrossRef] [PubMed]
- Schiffman, R.M.; Christianson, M.D.; Jacobsen, G.; Hirsch, J.D.; Reis, B.L. Reliability and validity of the Ocular Surface Disease Index. Arch. Ophthalmol. 2000, 118, 615–621. [Google Scholar] [CrossRef]
- Fernandez, J.; Rodriguez-Vallejo, M.; Martinez, J.; Tauste, A.; Garcia-Montesinos, J.; Pinero, D.P. Agreement and repeatability of objective systems for assessment of the tear film. Graefe’s Arch. Clin. Exp. Ophthalmol. 2018, 256, 1535–1541. [Google Scholar] [CrossRef] [Green Version]
- Khamar, P.; Nair, A.P.; Shetty, R.; Vaidya, T.; Subramani, M.; Ponnalagu, M.; Dhamodaran, K.; D’Souza, S.; Ghosh, A.; Pahuja, N.; et al. Dysregulated Tear Fluid Nociception-Associated Factors, Corneal Dendritic Cell Density, and Vitamin D Levels in Evaporative Dry Eye. Investig. Ophthalmol. Vis. Sci. 2019, 60, 2532–2542. [Google Scholar] [CrossRef] [Green Version]
- Nair, A.P.; D’Souza, S.; Shetty, R.; Ahuja, P.; Kundu, G.; Khamar, P.; Dadachanji, Z.; Paritekar, P.; Patel, P.; Dickman, M.M.; et al. Altered ocular surface immune cell profile in patients with dry eye disease. Ocul. Surf. 2021, 21, 96–106. [Google Scholar] [CrossRef]
- Willcox, M.D.P.; Argueso, P.; Georgiev, G.A.; Holopainen, J.M.; Laurie, G.W.; Millar, T.J.; Papas, E.B.; Rolland, J.P.; Schmidt, T.A.; Stahl, U.; et al. TFOS DEWS II Tear Film Report. Ocul. Surf. 2017, 15, 366–403. [Google Scholar] [CrossRef] [Green Version]
- Georgiev, G.A.; Eftimov, P.; Yokoi, N. Contribution of Mucins towards the Physical Properties of the Tear Film: A Modern Update. Int. J. Mol. Sci. 2019, 20, 6132. [Google Scholar] [CrossRef] [Green Version]
- Kojima, T.; Dogru, M.; Kawashima, M.; Nakamura, S.; Tsubota, K. Advances in the diagnosis and treatment of dry eye. Prog. Retin. Eye Res. 2020, 78, 100842. [Google Scholar] [CrossRef]
- Wang, N.; Nlend, M.C.; Nair, A.; Sznajder, J.I.; Sporn, P.H.S. 46 Hypercapnia Induces Mucin Gene Expression in Human Airway Epithelial Cells. J. Investig. Med. 2006, 54, S351. [Google Scholar] [CrossRef]
- Abolhassani, M.; Guais, A.; Chaumet-Riffaud, P.; Sasco, A.J.; Schwartz, L. Carbon dioxide inhalation causes pulmonary inflammation. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2009, 296, L657–L665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chadwick, O.; Lockington, D. Addressing post-operative Mask-Associated Dry Eye (MADE). Eye 2021, 35, 1543–1544. [Google Scholar] [CrossRef] [PubMed]
- Powell, J.B.; Kim, J.H.; Roberge, R.J. Powered air-purifying respirator use in healthcare: Effects on thermal sensations and comfort. J. Occup. Environ. Hyg. 2017, 14, 947–954. [Google Scholar] [CrossRef]
- Singh, N.P.; Walker, R.J.; Cowan, F.; Davidson, A.C.; Roberts, D.N. Retrograde air escape via the nasolacrimal system: A previously unrecognized complication of continuous positive airway pressure in the management of obstructive sleep apnea. Ann. Otol. Rhinol. Laryngol. 2014, 123, 321–324. [Google Scholar] [CrossRef]
- Wolffsohn, J.S.; Arita, R.; Chalmers, R.; Djalilian, A.; Dogru, M.; Dumbleton, K.; Gupta, P.K.; Karpecki, P.; Lazreg, S.; Pult, H.; et al. TFOS DEWS II Diagnostic Methodology report. Ocul. Surf. 2017, 15, 539–574. [Google Scholar] [CrossRef]
- Mainville, N.; Jordan, D.R. Etiology of tearing: A retrospective analysis of referrals to a tertiary care oculoplastics practice. Ophthalmic Plast. Reconstr. Surg. 2011, 27, 155–157. [Google Scholar] [CrossRef]
- Li, J.; Ma, J.; Hu, M.; Yu, J.; Zhao, Y. Assessment of tear film lipid layer thickness in patients with Meibomian gland dysfunction at different ages. BMC Ophthalmol. 2020, 20, 394. [Google Scholar] [CrossRef]
- D’Souza, S.; Annavajjhala, S.; Thakur, P.; Mullick, R.; Tejal, S.J.; Shetty, N. Study of tear film optics and its impact on quality of vision. Indian J. Ophthalmol. 2020, 68, 2899–2902. [Google Scholar] [CrossRef]
- Bron, A.J.; de Paiva, C.S.; Chauhan, S.K.; Bonini, S.; Gabison, E.E.; Jain, S.; Knop, E.; Markoulli, M.; Ogawa, Y.; Perez, V.; et al. TFOS DEWS II pathophysiology report. Ocul. Surf. 2017, 15, 438–510. [Google Scholar] [CrossRef]
- Yamaguchi, T. Inflammatory Response in Dry Eye. Investig. Ophthalmol. Vis. Sci. 2018, 59, DES192–DES199. [Google Scholar] [CrossRef] [Green Version]
- Perez, V.L.; Stern, M.E.; Pflugfelder, S.C. Inflammatory basis for dry eye disease flares. Exp. Eye Res. 2020, 201, 108294. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, I.; Lopez-Miguel, A.; Enriquez-de-Salamanca, A.; Teson, M.; Stern, M.E.; Gonzalez-Garcia, M.J.; Calonge, M. Response profiles to a controlled adverse desiccating environment based on clinical and tear molecule changes. Ocul. Surf. 2019, 17, 502–515. [Google Scholar] [CrossRef] [PubMed]
- Shetty, R.; Sethu, S.; Chevour, P.; Deshpande, K.; Pahuja, N.; Nagaraja, H.; Pindipapanahalli, N.; Ghosh, A. Lower Vitamin D Level and Distinct Tear Cytokine Profile Were Observed in Patients with Mild Dry Eye Signs but Exaggerated Symptoms. Transl. Vis. Sci. Technol. 2016, 5, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhee, M.S.M.; Lindquist, C.D.; Silvestrini, M.T.; Chan, A.C.; Ong, J.J.Y.; Sharma, V.K. Carbon dioxide increases with face masks but remains below short-term NIOSH limits. BMC Infect. Dis. 2021, 21, 354. [Google Scholar] [CrossRef] [PubMed]
- Gaultier, C.; Trang, H.; Dauger, S.; Gallego, J. Pediatric disorders with autonomic dysfunction: What role for PHOX2B? Pediatr. Res. 2005, 58, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, L.; Li, D.Q.; Corrales, R.M.; Pflugfelder, S.C. Hyperosmolar saline is a proinflammatory stress on the mouse ocular surface. Eye Contact Lens 2005, 31, 186–193. [Google Scholar] [CrossRef]
- Aragona, P.; Di Stefano, G.; Ferreri, F.; Spinella, R.; Stilo, A. Sodium hyaluronate eye drops of different osmolarity for the treatment of dry eye in Sjogren’s syndrome patients. Br. J. Ophthalmol. 2002, 86, 879–884. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| OSDI-Total | OSDI-Discomfort Scale | OSDI-Vision Scale | ||||
|---|---|---|---|---|---|---|
| r | p-Value | r | p-Value | r | p-Value | |
| Analytes | ||||||
| IL-1β | 0.310 | 0.010 | 0.279 | 0.021 | 0.191 | 0.119 |
| IL-6 | −0.279 | 0.021 | −0.313 | 0.010 | −0.175 | 0.154 |
| IL-8 | −0.297 | 0.014 | −0.315 | 0.009 | −0.157 | 0.202 |
| IL-12p70 | −0.378 | 0.002 | −0.442 | 0.000 | −0.157 | 0.200 |
| IL-12/23p40 | −0.198 | 0.105 | −0.303 | 0.012 | −0.072 | 0.561 |
| IL-13 | −0.279 | 0.021 | −0.295 | 0.015 | −0.194 | 0.113 |
| IL-33 | 0.375 | 0.002 | 0.334 | 0.005 | 0.212 | 0.083 |
| IFNα | −0.155 | 0.207 | −0.231 | 0.058 | −0.133 | 0.278 |
| IFNβ | 0.242 | 0.047 | 0.213 | 0.081 | 0.101 | 0.411 |
| BDNF | 0.384 | 0.001 | 0.359 | 0.003 | 0.216 | 0.077 |
| Eotaxin | −0.158 | 0.199 | −0.269 | 0.026 | −0.043 | 0.730 |
| Granzymes | −0.280 | 0.021 | −0.281 | 0.021 | −0.193 | 0.115 |
| TSLP | 0.307 | 0.011 | 0.278 | 0.022 | 0.181 | 0.140 |
| VEGF | −0.275 | 0.023 | −0.218 | 0.075 | −0.171 | 0.164 |
| sTNFRI | 0.253 | 0.038 | 0.218 | 0.075 | 0.228 | 0.062 |
| sFasL | −0.218 | 0.074 | −0.285 | 0.019 | −0.079 | 0.523 |
| Immune cells | ||||||
| Leukocytes | 0.262 | 0.086 | 0.421 | 0.004 | −0.059 | 0.704 |
| Macrophage | 0.376 | 0.012 | 0.327 | 0.030 | 0.366 | 0.015 |
| NK cells | 0.306 | 0.043 | 0.370 | 0.014 | 0.000 | 0.998 |
| NKT cells | 0.207 | 0.178 | 0.275 | 0.071 | 0.017 | 0.913 |
| Analytes (pg/mL) | Normocapnia (5% CO2) | Hypercapnia (20% CO2) | Fold Diff. | ||||
|---|---|---|---|---|---|---|---|
| Mean | Stdev | SEM | Mean | Stdev | SEM | ||
| IL-1α | 8.9 | 18.3 | 10.6 | 15.4 | 1.2 | 0.7 | 1.7 |
| IL-6 | 4654.9 | 157.7 | 91.0 | 184.1 | 0.1 | 0.1 | 0.0 |
| IL-8 | 328.8 | 28.9 | 16.7 | 163.8 | 0.4 | 0.2 | 0.5 |
| IL-13 | 1.6 | 0.1 | 0.1 | 1.3 | 0.1 | 0.0 | 0.8 |
| IFNβ | 17.3 | 35.1 | 20.3 | 43.6 | 2.2 | 1.3 | 2.5 |
| TNFα | 2.1 | 0.1 | 0.0 | 0.5 | 2.4 | 1.4 | 0.2 |
| HGF | 9573.9 | 4395.3 | 2537.6 | 5961.2 | 1.0 | 0.6 | 0.6 |
| VEGF | 422.0 | 67.7 | 39.1 | 267.6 | 0.6 | 0.4 | 0.6 |
| LIF | 448.5 | 191.6 | 110.6 | 518.6 | 0.3 | 0.2 | 1.2 |
| Perforins | 5.9 | 2.4 | 1.4 | 8.4 | 0.8 | 0.4 | 1.4 |
| (a) | ||
| Tear Fluid | MUC5AC | MUC16 |
| Fold Diff. (Post-ME/Pre-ME) | Fold Diff. (Post-ME/Pre-ME) | |
| Subject 1 | 1.6 | 1.3 |
| Subject 2 | 4.9 | 0.8 |
| Subject 3 | 0.5 | 7.5 |
| Subject 4 | 0.5 | 0.7 |
| Subject 5 | 0.1 | 0.9 |
| Subject 6 | 1.8 | 1.4 |
| Mean ± SEM | 1.6 ± 0.7 | 2.1 ± 1.1 |
| (b) | ||
|---|---|---|
| Corneoscleral Rim Explant Culture | MUC5AC | MUC16 |
| Fold Diff. (Hypercapnia/Normocapnia) | Fold Diff. (Hypercapnia/Normocapnia) | |
| Donor 1 | 5.2 | 0.8 |
| Donor 2 | 4.4 | 3.4 |
| Donor 3 | 1.8 | 2.1 |
| Mean ± SEM | 3.8 ± 1.0 | 2.1 ± 1.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Souza, S.; Vaidya, T.; Nair, A.P.; Shetty, R.; Kumar, N.R.; Bisht, A.; Panigrahi, T.; J, T.S.; Khamar, P.; Dickman, M.M.; et al. Altered Ocular Surface Health Status and Tear Film Immune Profile Due to Prolonged Daily Mask Wear in Health Care Workers. Biomedicines 2022, 10, 1160. https://doi.org/10.3390/biomedicines10051160
D’Souza S, Vaidya T, Nair AP, Shetty R, Kumar NR, Bisht A, Panigrahi T, J TS, Khamar P, Dickman MM, et al. Altered Ocular Surface Health Status and Tear Film Immune Profile Due to Prolonged Daily Mask Wear in Health Care Workers. Biomedicines. 2022; 10(5):1160. https://doi.org/10.3390/biomedicines10051160
Chicago/Turabian StyleD’Souza, Sharon, Tanuja Vaidya, Archana Padmanabhan Nair, Rohit Shetty, Nimisha Rajiv Kumar, Anadi Bisht, Trailokyanath Panigrahi, Tejal S. J, Pooja Khamar, Mor M. Dickman, and et al. 2022. "Altered Ocular Surface Health Status and Tear Film Immune Profile Due to Prolonged Daily Mask Wear in Health Care Workers" Biomedicines 10, no. 5: 1160. https://doi.org/10.3390/biomedicines10051160