
Antitumor Effect and Induced Immune Response Following Exposure of Hexaminolevulinate and Blue Light in Combination with Checkpoint Inhibitor in an Orthotopic Model of Rat Bladder Cancer

Abstract
:1. Introduction
2. Materials and Methods
2.1. Tumor Cells Culture
2.2. Orthotopic Tumor Model
2.3. Hexylaminolevulinate Preparation and Administration
2.4. Illumination of Rat Bladders
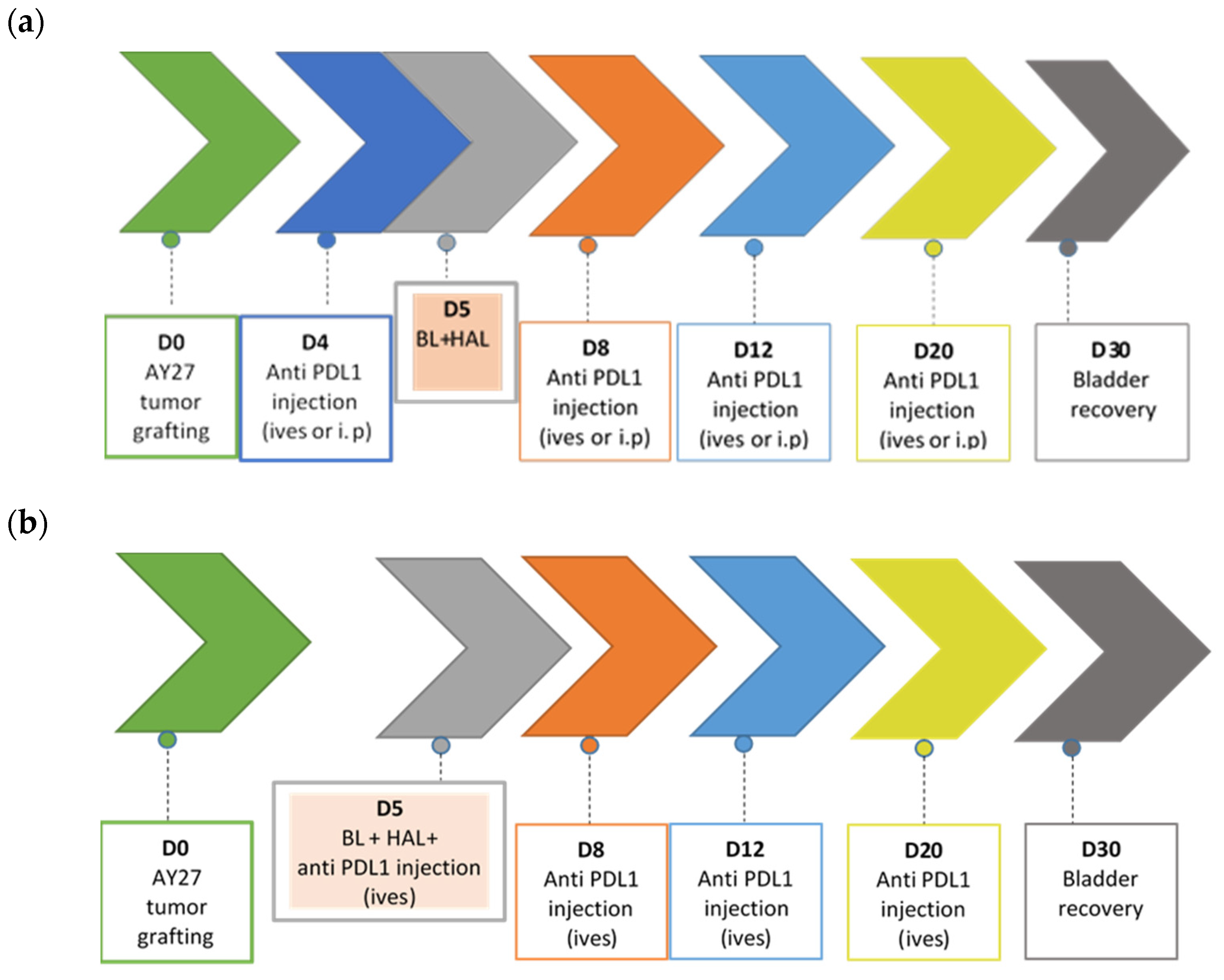
2.5. Combination Therapy
2.5.1. Intraperitoneal Injections (i.p.)
2.5.2. Intravesical Instillations (ives)
2.6. Pathological and Immunological Analysis
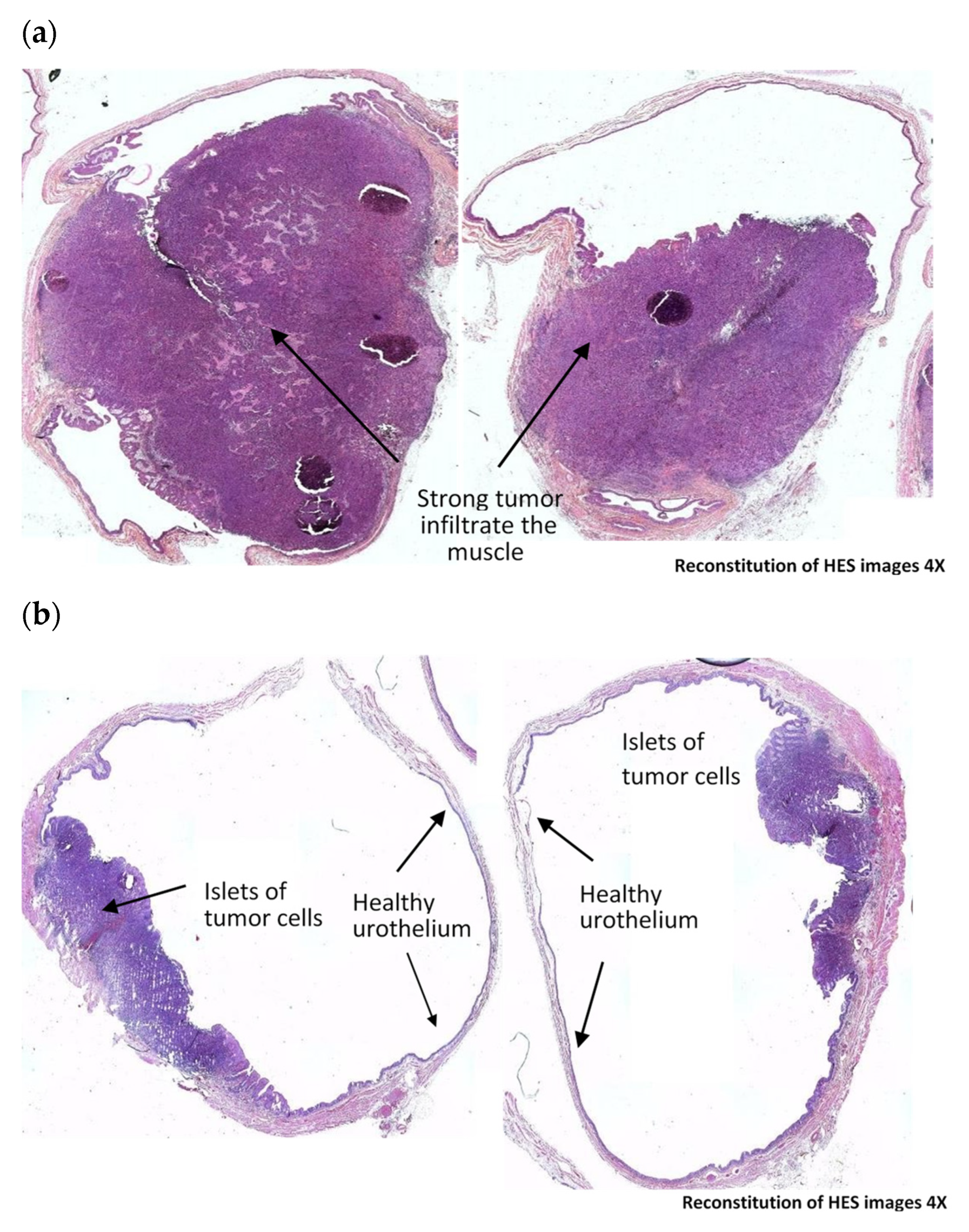
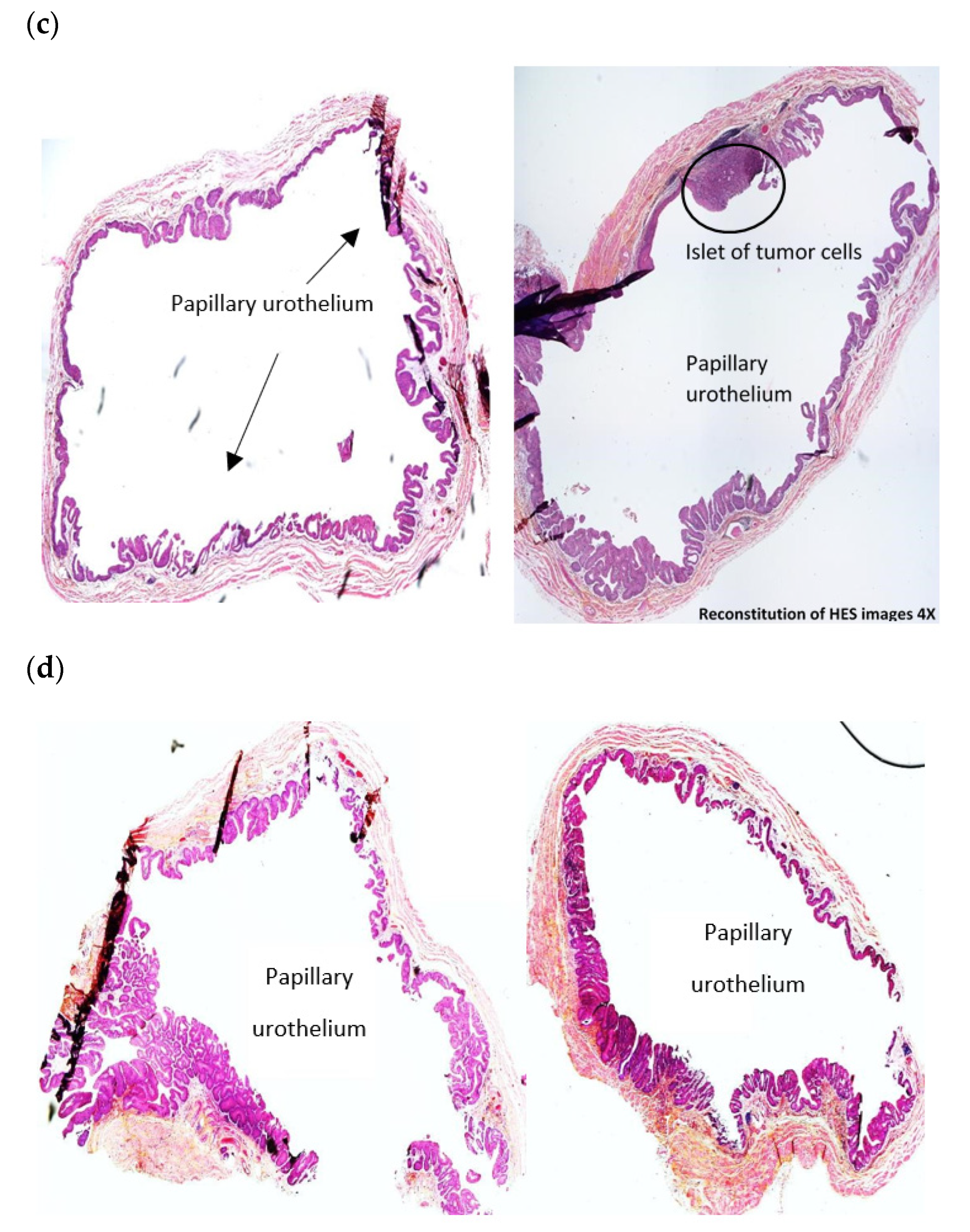
2.6.1. Hematoxylin-Eosin-Safran (HES) Analysis
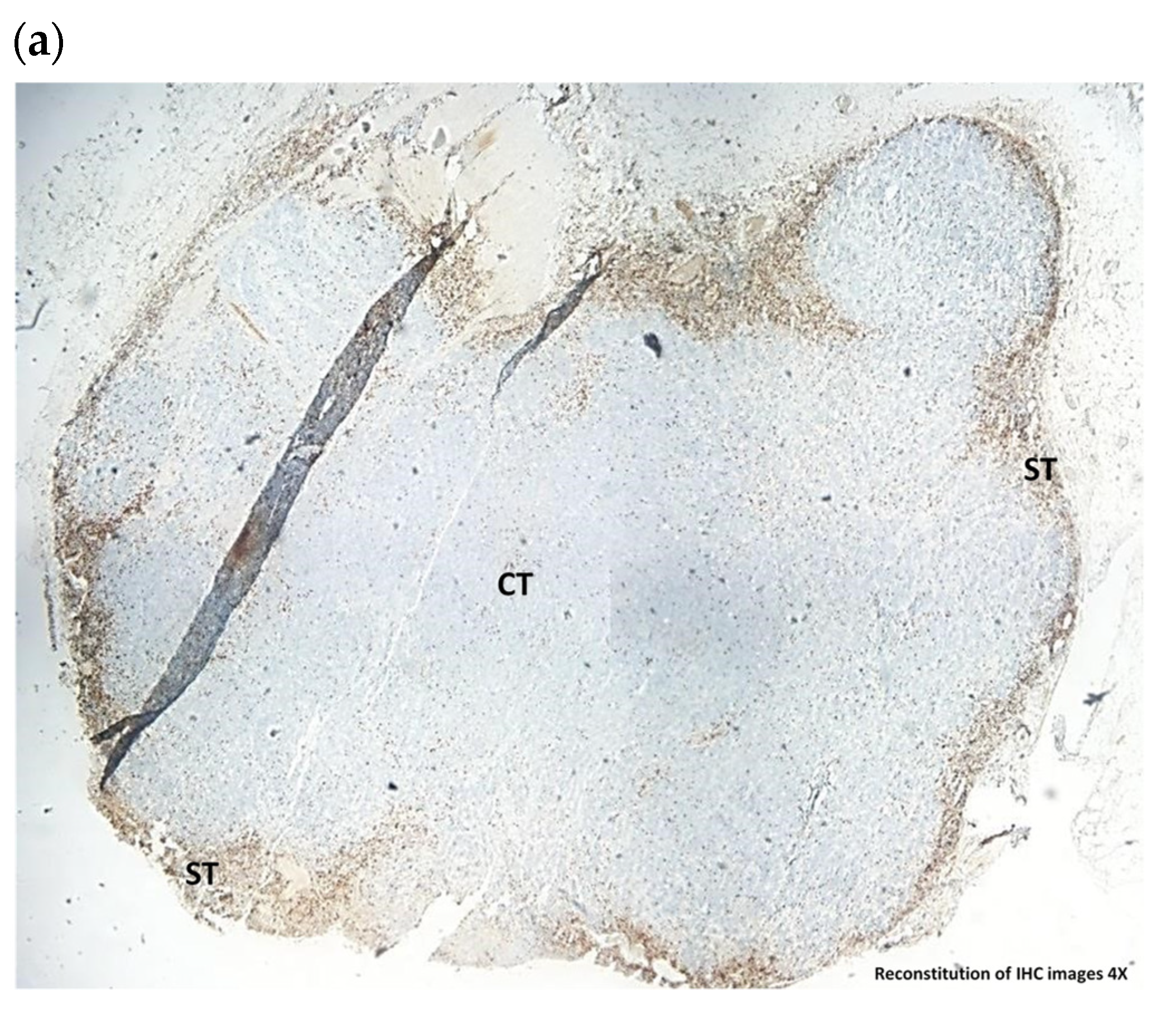
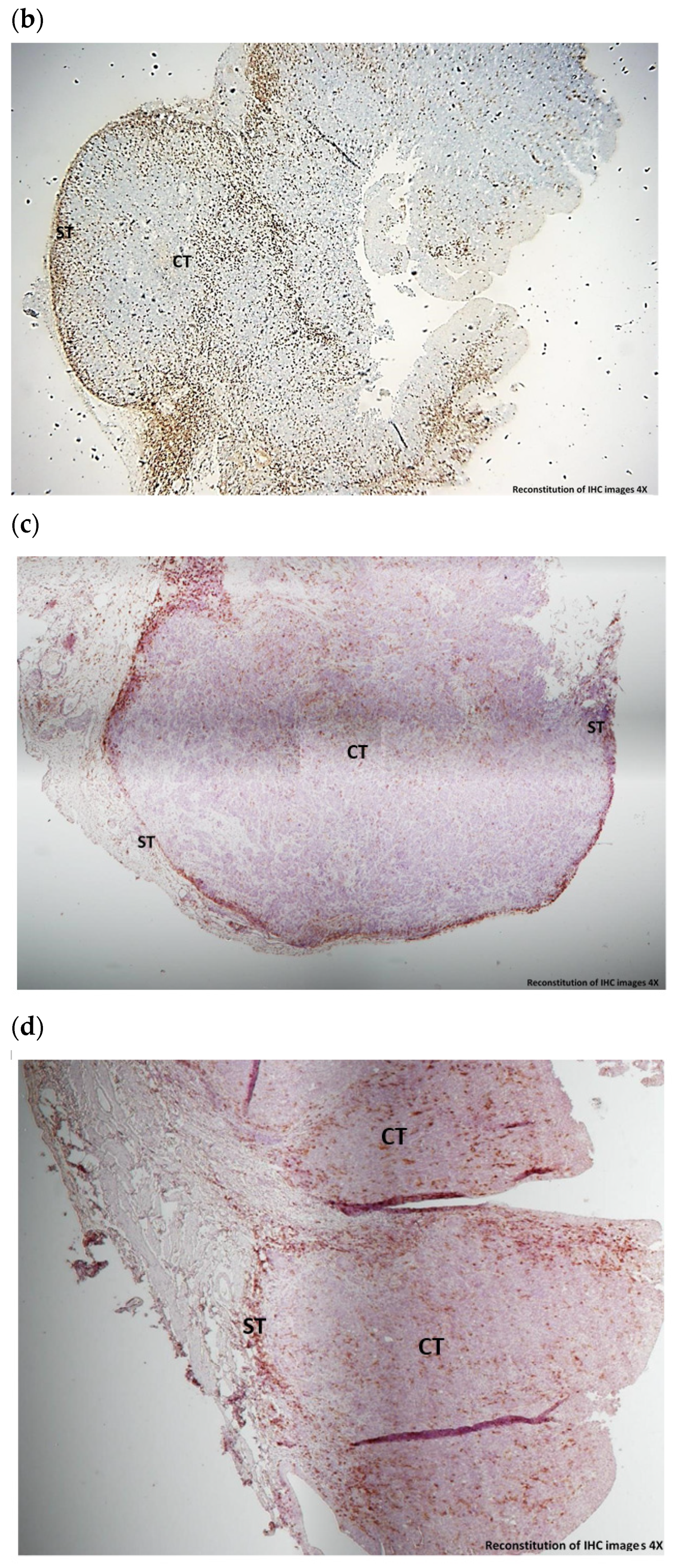
2.6.2. Assessment of Immune Cells in Tissues
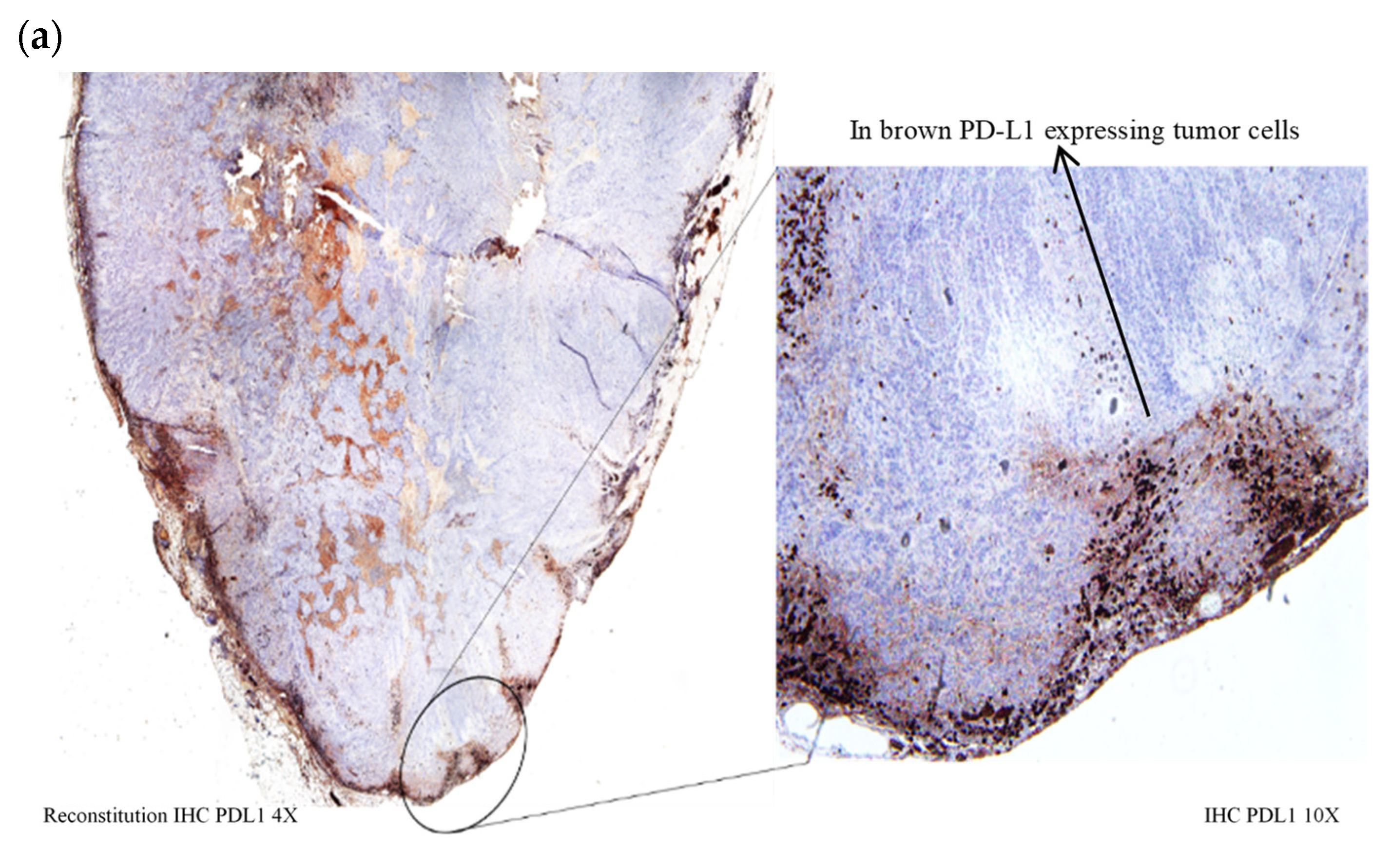
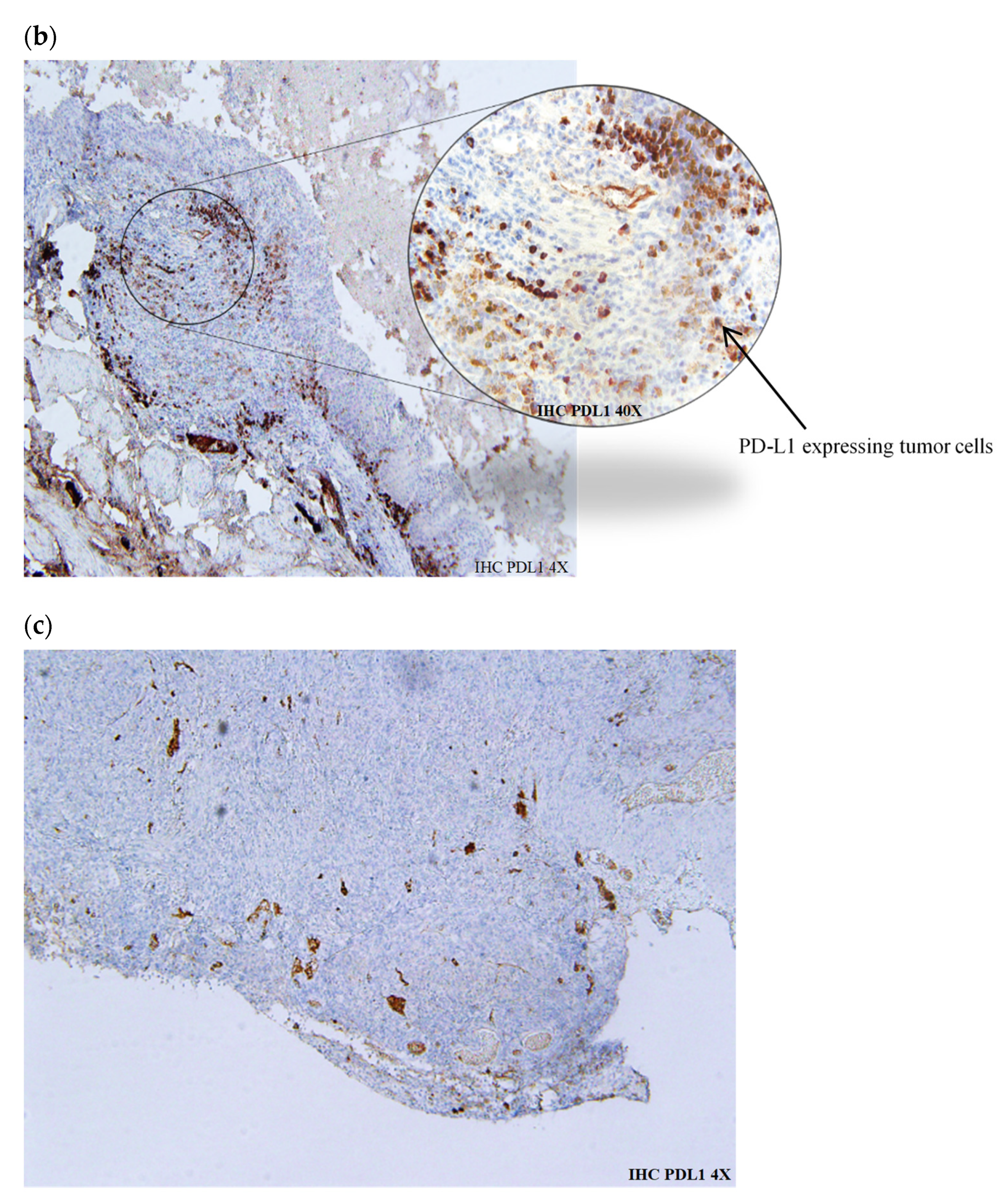
2.6.3. PD-L1 Expression in Tumor Cells
2.7. Statistical Analysis
3. Results
3.1. HAL-PDD-Mediated Therapeutic Effect in AY27 Orthotopic Bladder Tumors
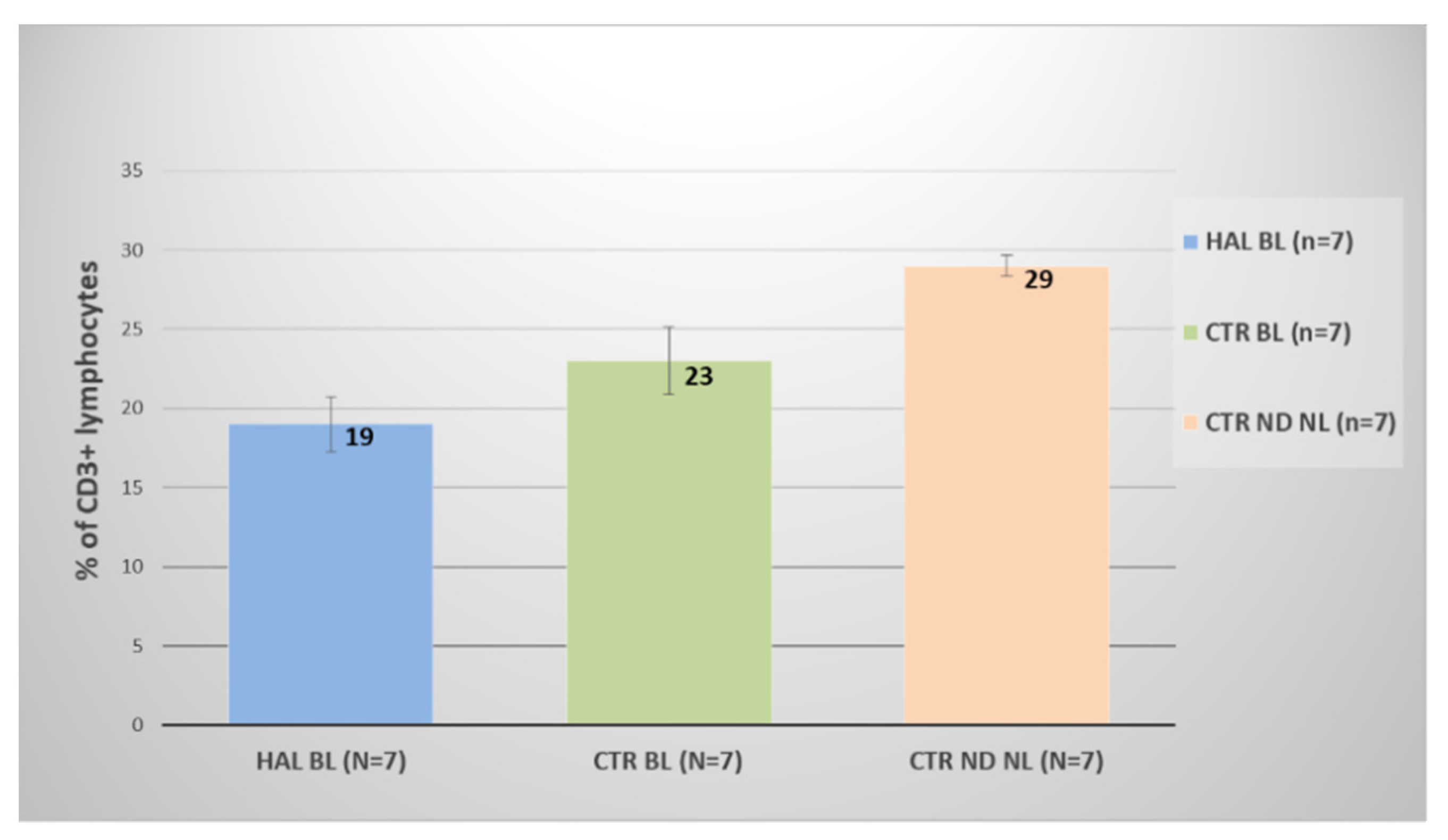
3.2. Assessment of Immunological Markers
3.3. IHC-Assessed PD-L1 Expression in Bladder Tumor Cells
3.4. Therapeutic Effect of Immune Checkpoint Therapy in AY27 Orthotopic Bladder Tumors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Miranda-Filho, A.; Bray, F.; Charvat, H.; Rajaraman, S.; Soerjomataram, I. The world cancer patient population (WCPP): An updated standard for international comparisons of population-based survival. Cancer Epidemiol. 2020, 69, 101802. [Google Scholar] [CrossRef] [PubMed]
- Matulewicz, R.S.; Steinberg, G.D. Non-muscle-invasive bladder cancer: Overview and contemporary treatment landscape of neoadjuvant chemoablative therapies. Rev. Urol. 2020, 22, 43–51. [Google Scholar] [PubMed]
- Di Stasi, S.M.; De Carlo, F.; Pagliarulo, V.; Masedu, F.; Verri, C.; Celestino, F.; Riedl, C. Hexaminolevulinate hydrochloride in the detection of nonmuscle invasive cancer of the bladder. Ther. Adv. Urol. 2015, 7, 339–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stenzl, A.; Burger, M.; Fradet, Y.; Mynderse, L.A.; Soloway, M.S.; Witjes, J.A.; Kriegmair, M.; Karl, A.; Shen, Y.; Grossman, H.B. Hexaminolevulinate guided fluorescence cystoscopy reduces recurrence in patients with nonmuscle invasive bladder cancer. J. Urol. 2010, 184, 1907–1914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grossman, H.B.; Stenzl, A.; Fradet, Y.; Mynderse, L.A.; Kriegmair, M.; Witjes, J.A.; Soloway, M.S.; Karl, A.; Burger, M. Long-term decrease in bladder cancer recurrence with hexaminolevulinate enabled fluorescence cystoscopy. J. Urol. 2012, 188, 58–62. [Google Scholar] [CrossRef]
- Chang, S.S.; Boorjian, S.A.; Chou, R.; Clark, P.E.; Daneshmand, S.; Konety, B.R.; Pruthi, R.; Quale, D.Z.; Ritch, C.R.; Seigne, J.D.; et al. Diagnosis and treatment of non-muscle invasive bladder cancer: AUA/SUO guideline. J. Urol. 2016, 196, 1021–1029. [Google Scholar] [CrossRef]
- EAU Guidelines: Non-Muscle-Invasive Bladder Cancer. Available online: https://uroweb.org/guideline/non-muscle-invasive-bladder-cancer/ (accessed on 5 January 2022).
- Garg, A.D.; Nowis, D.; Golab, J.; Agostinis, P. Photodynamic therapy: Illuminating the road from cell death towards anti-tumour immunity. Apoptosis 2010, 15, 1050–1071. [Google Scholar] [CrossRef]
- Mroz, P.; Hashmi, J.T.; Huang, Y.; Lange, N.; Hamblin, M.R. Stimulation of anti-tumor immunity by photodynamic therapy. Expert Rev. Clin. Immunol. 2011, 7, 75–91. [Google Scholar] [CrossRef] [Green Version]
- Reginato, E.; Wolf, P.; Hamblin, M.R. Immune response after photodynamic therapy increases anti-cancer and anti-bacterial effects. World J. Immunol. 2014, 4, 1–11. [Google Scholar] [CrossRef]
- Anzengruber, F.; Avci, P.; de Freitas, L.F.; Hamblin, M.R. T-cell mediated anti-tumor immunity after photodynamic therapy: Why does it not always work and how can we improve it? Photochem. Photobiol. Sci. 2015, 14, 1492–1509. [Google Scholar] [CrossRef] [Green Version]
- Hwang, H.S.; Shin, H.; Han, J.; Na, K. Combination of photodynamic therapy (PDT) and anti-tumor immunity in cancer therapy. J. Pharm. Investig. 2018, 48, 143–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bader, M.J.; Stepp, H.; Beyer, W.; Pongratz, T.; Sroka, R.; Kriegmair, M.; Dirk, Z.; Mona, W.; Derya, T.; Christian, G.S.; et al. Photodynamic therapy of bladder cancer—A phase I study using hexaminolevulinate (HAL). Urol. Oncol. Semin. Orig. Investig. 2013, 31, 1178–1183. [Google Scholar] [CrossRef] [PubMed]
- Gakis, G.; Ngamsri, T.; Rausch, S.; Mischinger, J.; Todenhöfer, T.; Schwentner, C.; Schmid, M.A.; Hassan, F.A.-S.; Renninger, M.; Stenzl, A. Fluorescence-guided bladder tumour resection: Impact on survival after radical cystectomy. World J. Urol. 2015, 33, 1429–1437. [Google Scholar] [CrossRef] [PubMed]
- Renninger, M.; Fahmy, O.; Schubert, T.; Schmid, M.A.; Hassan, F.; Stenzl, A.; Gakis, G. The prognostic impact of hexaminolevulinate-based bladder tumor resection in patients with primary non-muscle invasive bladder cancer treated with radical cystectomy. World J. Urol. 2019, 38, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Pardoll, D.M. The blockade of immune checkpoints in cancer immunotherapy. Nat. Rev. Cancer 2012, 12, 252–264. [Google Scholar] [CrossRef] [Green Version]
- Song, D.; Powles, T.; Shi, L.; Zhang, L.; Ingersoll, M.A.; Lu, Y. Bladder cancer, a unique model to understand cancer immunity and develop immunotherapy approaches. J. Pathol. 2019, 249, 151–165. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.S.; Seo, H.K. Emerging treatments for bacillus Calmette–Guérin-unresponsive non-muscle-invasive bladder cancer. Investig. Clin. Urol. 2021, 62, 361–377. [Google Scholar] [CrossRef]
- Lopez-Beltran, A.; Cimadamore, A.; Blanca, A.; Massari, F.; Vau, N.; Scarpelli, M.; Cheng, L.; Montironi, R. Immune checkpoint inhibitors for the treatment of bladder cancer. Cancers 2021, 13, 131. [Google Scholar] [CrossRef]
- Hahn, N.M.; Necchi, A.; Loriot, Y.; Powles, T.; Plimack, E.R.; Sonpavde, G.; Roupret, M.; Kamat, A.M. Role of checkpoint inhibition in localized bladder cancer. Eur. Urol. Oncol. 2018, 1, 190–198. [Google Scholar] [CrossRef]
- Anand, S.; Chan, T.; Hasan, T.; Maytin, E. Current prospects for treatment of solid tumors via photodynamic, photothermal, or ionizing radiation therapies combined with immune checkpoint inhibition (a review). Pharmaceuticals 2021, 14, 447. [Google Scholar] [CrossRef]
- O’Shaughnessy, M.J.; Murray, K.S.; La Rosa, S.P.; Budhu, S.; Merghoub, T.; Somma, A.; Monette, S.; Kim, K.; Corradi, R.B.; Scherz, A.; et al. Systemic antitumor immunity by PD-1/PD-L1 inhibition is potentiated by vascular-targeted photodynamic therapy of primary tumors. Clin. Cancer Res. 2017, 24, 592–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, L.; Zhang, C.; Gao, D.; Liu, H.; Yu, X.; Lai, J.; Wang, F.; Lin, J.; Liu, Z. Enhanced anti-tumor efficacy through a combination of integrin αvβ6-targeted photodynamic therapy and immune checkpoint inhibition. Theranostics 2016, 6, 627–637. [Google Scholar] [CrossRef] [PubMed]
- Kleinovink, J.W.; Fransen, M.F.; Löwik, C.W.; Ossendorp, F. Photodynamic-Immune checkpoint therapy eradicates local and distant tumors by CD8+ T cells. Cancer Immunol. Res. 2017, 5, 832–838. [Google Scholar] [CrossRef] [Green Version]
- Liu, Q.; Tian, J.; Tian, Y.; Sun, Q.; Sun, D.; Wang, F.; Xu, H.; Ying, G.; Wang, J.; Yetisen, A.K.; et al. Near-infrared-ii nanoparticles for cancer imaging of immune checkpoint programmed death-ligand 1 and photodynamic/immune therapy. ACS Nano 2021, 15, 515–525. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Z.; McCallum, T.J.; Brown, K.M.; Miller, G.G.; Halls, S.B.; Parney, I.; Moore, R. Characterization of a novel transplantable orthotopic rat bladder transitional cell tumour model. Br. J. Cancer 1999, 81, 638–646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Summary of Safety and Effectiveness (SSED). Karl Storz D-Light C Photodynamic Diagnosis (PDD) System. PMA Number P050027. Available online: https://fda.report/PMA/P050027/5/P050027B.pdf (accessed on 9 February 2022).
- Wu, C.-T.; Chen, W.-C.; Chang, Y.-H.; Lin, W.-Y.; Chen, M.-F. The role of PD-L1 in the radiation response and clinical outcome for bladder cancer. Sci. Rep. 2016, 6, 19740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Efficacy of Durvalumab in Non-Muscle-Invasive Bladder Cancer. Available online: https://www.clinicaltrials.gov/ct2/show/NCT03759496?term=PD-L1&cond=NMIBC&rank=1 (accessed on 7 February 2022).
- Kim, S.H.; Chan, P.S.; Kim, D.Y.; Park, J.W.; Baek, J.Y.; Kim, S.Y.; Park, S.C.; Oh, J.H.; Byung-Ho, N.; Nam, B.-H. What is the ideal tumor regression grading system in rectal cancer patients after preoperative chemoradiotherapy? Cancer Res. Treat. 2016, 48, 998–1009. [Google Scholar] [CrossRef] [Green Version]
- Bressenot, A.; Marchal, S.; Bezdetnaya, L.; Garrier, J.; Guillemin, F.; Plénat, F. Assessment of apoptosis by immunohistochemistry to active caspase-3, active caspase-7, or cleaved PARP in monolayer cells and spheroid and subcutaneous xenografts of human carcinoma. J. Histochem. Cytochem. 2009, 57, 289–300. [Google Scholar] [CrossRef]
- Arum, C.-J.; Gederaas, O.A.; Larsen, E.L.P.; Randeberg, L.L.; Hjelde, A.; Krokan, H.E.; Svaasand, L.O.; Chen, D.; Zhao, C.-M. Tissue responses to hexyl 5-aminolevulinate-induced photodynamic treatment in syngeneic orthotopic rat bladder cancer model: Possible pathways of action. J. Biomed. Opt. 2011, 16, 028001. [Google Scholar] [CrossRef]
- Lilge, L.; Roufaiel, M.; Lazic, S.; Kaspler, P.; Munegowda, M.A.; Nitz, M.; Bassan, J.; Mandel, A. Evaluation of a Ruthenium coordination complex as photosensitizer for PDT of bladder cancer: Cellular response, tissue selectivity and in vivo response. Transl. Biophotonics 2020, 2, 2. [Google Scholar] [CrossRef]
- Larsen, E.L.P.; Randeberg, L.L.; Gederaas, O.A.; Arum, C.-J.; Hjelde, A.; Zhao, C.-M.; Chen, D.; Krokan, H.E.; Svaasand, L.O. Monitoring of hexyl 5-aminolevulinate-induced photodynamic therapy in rat bladder cancer by optical spectroscopy. J. Biomed. Opt. 2008, 13, 044031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- François, A.; Salvadori, A.; Bressenot, A.; Bezdetnaya, L.; Guillemin, F.; D’Hallewin, M.A. How to avoid local side effects of bladder photodynamic therapy: Impact of the fluence rate. J. Urol. 2013, 190, 731–736. [Google Scholar] [CrossRef] [PubMed]
- Rocha, L.B.; Gomes-Da-Silva, L.C.; Dąbrowski, J.M.; Arnaut, L.G. Elimination of primary tumours and control of metastasis with rationally designed bacteriochlorin photodynamic therapy regimens. Eur. J. Cancer 2015, 51, 1822–1830. [Google Scholar] [CrossRef] [PubMed]
- Preise, D.; Oren, R.; Glinert, I.; Kalchenko, V.; Jung, S.; Scherz, A.; Salomon, Y. Systemic antitumor protection by vascular-targeted photodynamic therapy involves cellular and humoral immunity. Cancer Immunol. Immunother. 2009, 58, 71–84. [Google Scholar] [CrossRef]
- Kirschner, A.N.; Wang, J.; Rajkumar-Calkins, A.; Neuzil, K.E.; Chang, S.S. Intravesical anti-pd-1 immune checkpoint inhibition treats urothelial bladder cancer in a mouse model. J. Urol. 2020, 205, 1336–1343. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No Response (NR) | Moderate Response (MR) | Near Complete Response (Near CR) | Complete Response (CR) |
|---|---|---|---|
| Rat with strong muscle-infiltrative tumor | Rats with few tumor cells or islets of tumor cells in several areas | Rats with singular islet of tumor cells or very few tumor cells | Absence of tumor cells |
| Time after Grafting (d) | Treatments | Tumor Response Grades | |||||
|---|---|---|---|---|---|---|---|
| NR | MR | Near CR | CR | Near CR + CR | |||
| 12 | HAL BL (n = 8) | 1/8 | 2/8 | 3/8 | 2/8 | 5/8 | 63% |
| 30 | CTR ND NL (n = 12) | 12/12 | 0/12 | 0/12 | 0/12 | 0/12 | 0% |
| CTR BL (n = 6) | 6/6 | 0/6 | 0/6 | 0/6 | 0/6 | 0% | |
| HAL BL (n = 13) | 8/13 | 1/13 | 0/13 | 4/13 | 4/13 | 31% | |
| Time after Grafting (Days) | Treatments | 50 < PD-L1 < 100% Strong | 1 < PD-L1 < 49% Moderate | PD-L1 < 1% Weak |
|---|---|---|---|---|
| 7 | HAL BL (n = 4) | 0/4 | 1/4 | 3/4 |
| 12 | CTR ND NL (n = 4) | 3/4 | 1/4 | 0/4 |
| CTR BL (n = 4) | 3/4 | 1/4 | 0/4 | |
| HAL BL (n = 6) | 4/6 | 0/6 | 2/6 | |
| 30 | CTR ND NL (n = 11) | 2/11 | 1/11 | 8/11 |
| CTR BL (n = 5) | 2/5 | 2/5 | 1/5 | |
| HAL BL (n = 12) | 0/12 | 1/12 | 11/12 |
| Treatments | Tumor Response Grades | |||||
|---|---|---|---|---|---|---|
| NR | MR | Near CR | CR | Near CR + CR | ||
| CTR PDL1 ives (n = 9) | 9/9 | 0/9 | 0/9 | 0/9 | 0/9 | 0% |
| CTR PDL1 i.p (n = 10) | 10/10 | 0/10 | 0/10 | 0/10 | 0/10 | 0% |
| HAL BL PDL1 i.p (n = 9) | 7/9 | 0/9 | 1/9 | 1/9 | 2/9 | 22% |
| HAL BL PDL1 ives (n = 10) | 6/10 | 1/10 | 0/10 | 3/10 | 3/10 | 30% |
| HAL BL PD-L1 ives co-administered (n = 8) | 3/8 | 2/8 | 2/8 | 1/8 | 3/8 | 38% |
| HAL BL * (n = 13) | 8/13 | 1/13 | 0/13 | 4/13 | 4/13 | 31% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lamy, L.; Thomas, J.; Leroux, A.; Bisson, J.-F.; Myren, K.; Godal, A.; Stensrud, G.; Bezdetnaya, L. Antitumor Effect and Induced Immune Response Following Exposure of Hexaminolevulinate and Blue Light in Combination with Checkpoint Inhibitor in an Orthotopic Model of Rat Bladder Cancer. Biomedicines 2022, 10, 548. https://doi.org/10.3390/biomedicines10030548
Lamy L, Thomas J, Leroux A, Bisson J-F, Myren K, Godal A, Stensrud G, Bezdetnaya L. Antitumor Effect and Induced Immune Response Following Exposure of Hexaminolevulinate and Blue Light in Combination with Checkpoint Inhibitor in an Orthotopic Model of Rat Bladder Cancer. Biomedicines. 2022; 10(3):548. https://doi.org/10.3390/biomedicines10030548
Chicago/Turabian StyleLamy, Laureline, Jacques Thomas, Agnès Leroux, Jean-François Bisson, Kari Myren, Aslak Godal, Gry Stensrud, and Lina Bezdetnaya. 2022. "Antitumor Effect and Induced Immune Response Following Exposure of Hexaminolevulinate and Blue Light in Combination with Checkpoint Inhibitor in an Orthotopic Model of Rat Bladder Cancer" Biomedicines 10, no. 3: 548. https://doi.org/10.3390/biomedicines10030548