
Delphi-Based Consensus on Interstitial Lung Disease Screening in Patients with Connective Tissue Diseases (Croatian National-Based Study)
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dahani, A.; Arain, S.-R.; Riaz, A.; Khan, F.; Jabeen, R. Prevalence and Pattern of Pulmonary Manifestation in Patients with Connective Tissue Disorder. Cureus 2020, 12, e7618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Lauretis, A.; Veeraraghavan, S.; Renzoni, E. Review series: Aspects of interstitial lung disease: Connective tissue disease-associated interstitial lung disease: How does it differ from IPF? How should the clinical approach differ? Chron. Respir. Dis. 2011, 8, 53–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergamasco, A.; Hartmann, N.; Wallace, L.; Verpillat, P. Epidemiology of systemic sclerosis and systemic sclerosis-associated interstitial lung disease. Clin. Epidemiol. 2019, 11, 257–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graney, B.A.; Fischer, A. Advocating for early interstitial lung disease detection in mixed connective tissue disease. Rheumatology 2018, 57, 204–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hyldgaard, C.; Hilberg, O.; Pedersen, A.-B.; Ulrichsen, S.-P.; Løkke, A.; Bendstrup, E.; Ellingsen, T. A population-based cohort study of rheumatoid arthritis-associated interstitial lung disease: Comorbidity and mortality. Ann. Rheum. Dis. 2017, 76, 1700–1706. [Google Scholar] [CrossRef] [PubMed]
- Raimundo, K.; Solomon, J.-J.; Olson, A.; Kong, A.-M.; Cole, A.-L.; Fischer, A.; Swigris, J.-J. Rheumatoid Arthritis-Interstitial Lung Disease in the United States: Prevalence, Incidence, and Healthcare Costs and Mortality. J. Rheumatol. 2019, 46, 360–369. [Google Scholar] [CrossRef] [PubMed]
- Kadura, S.; Raghu, G. Rheumatoid arthritis-interstitial lung disease: Manifestations and current concepts in pathogenesis and management. Eur. Respir. Rev. 2021, 30, 210011. [Google Scholar] [CrossRef]
- Sun, K.-Y.; Fan, Y.; Wang, Y.-X.; Zhong, Y.-J.; Wang, G.-F. Prevalence of interstitial lung disease in polymyositis and dermatomyositis: A meta-analysis from 2000 to 2020. Semin. Arthritis. Rheum. 2021, 51, 175–191. [Google Scholar] [CrossRef]
- Luppi, F.; Sebastiani, M.; Silva, M.; Sverzellati, N.; Cavazza, A.; Salvarani, C.; Manfredi, A. Interstitial lung disease in Sjögren’s syndrome: A clinical review. Clin. Exp. Rheumatol. 2020, 38 (Suppl. S126), 291–300. [Google Scholar]
- Shao, T.; Shi, X.; Yang, S.; Zhang, W.; Li, X.; Shu, J.; Alqalyoobi, S.; Zeki, A.A.; Leung, P.S.; Shuai, Z. Interstitial Lung Disease in Connective Tissue Disease: A Common Lesion With Heterogeneous Mechanisms and Treatment Considerations. Front. Immunol. 2021, 12, 684699. [Google Scholar] [CrossRef]
- Juge, P.-A.; Lee, J.S.; Ebstein, E.; Furukawa, H.; Dobrinskikh, E.; Gazal, S.; Kannengiesser, C.; Ottaviani, S.; Oka, S.; Tohma, S.; et al. Promoter Variant and Rheumatoid Arthritis with Interstitial Lung Disease. N. Engl. J. Med. 2018, 379, 2209–2219. [Google Scholar] [CrossRef] [PubMed]
- Juge, P.; Borie, R.; Kannengiesser, C.; Gazal, S.; Revy, P.; Wemeau-Stervinou, L.; Debray, M.; Ottaviani, S.; Marchand-Adam, S.; Nathan, N.; et al. Shared Genetic Predisposition in Rheumatoid Arthritis–Interstitial Lung Disease and Familial Pulmonary Fibrosis. In Proceedings of the Abstracts Accepted for Publication; BMJ Publishing Group Ltd. and European League Against Rheumatism: Madrid, Spain, 2017. [Google Scholar]
- Migita, K.; Nakamura, T.; Koga, T.; Eguchi, K. HLA-DRB1 Alleles and Rheumatoid Arthritis-Related Pulmonary Fibrosis. J. Rheumatol. 2010, 37, 205–207. [Google Scholar] [CrossRef] [Green Version]
- Furukawa, H.; Oka, S.; Shimada, K.; Sugii, S.; Ohashi, J.; Matsui, T.; Ikenaka, T.; Nakayama, H.; Hashimoto, A.; Takaoka, H.; et al. Association of Human Leukocyte Antigen with Interstitial Lung Disease in Rheumatoid Arthritis: A Protective Role for Shared Epitope. PLoS ONE 2012, 7, e33133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mori, S.; Koga, Y.; Sugimoto, M. Different Risk Factors between Interstitial Lung Disease and Airway Disease in Rheumatoid Arthritis. Res. Med. 2012, 106, 1591–1599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorlova, O.; Martin, J.-E.; Rueda, B.; Koeleman, B.P.C.; Ying, J.; Teruel, M.; Diaz-Gallo, L.-M.; Broen, J.C.; Vonk, M.C.; Simeon, C.P.; et al. Identification of Novel Genetic Markers Associated with Clinical Phenotypes of Systemic Sclerosis through a Genome-Wide Association Strategy. PLoS Genet 2011, 7, e1002178. [Google Scholar] [CrossRef]
- Gladman, D.D.; Kung, T.N.; Siannis, F.; Pellett, F.; Farewell, V.T.; Lee, P. HLA Markers for Susceptibility and Expression in Scleroderma. J. Rheumatol. 2005, 32, 1481–1487. [Google Scholar] [PubMed]
- Simeón, C.P.; Fonollosa, V.; Tolosa, C.; Palou, E.; Selva, A.; Solans, R.; Armadans, L.; Moreno, E.; Marsal, S.; Vilardell, M. Association of HLA Class II Genes with Systemic Sclerosis in Spanish Patients. J. Rheumatol. 2009, 36, 2733–2736. [Google Scholar] [CrossRef] [PubMed]
- Tikly, M.; Rands, A.; McHugh, N.; Wordsworth, P.; Welsh, K. Human Leukocyte Antigen Class II Associations with Systemic Sclerosis in South Africans. Tissue Antigens 2004, 63, 487–490. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Guo, X.; Yi, L.; Guo, G.; Tu, W.; Wu, W.; Yang, L.; Xiao, R.; Li, Y.; Chu, H.; et al. Association of HLA-DPB1 with Scleroderma and Its Clinical Features in Chinese Population. PLoS ONE 2014, 9, e87363. [Google Scholar] [CrossRef]
- Odani, T.; Yasuda, S.; Ota, Y.; Fujieda, Y.; Kon, Y.; Horita, T.; Kawaguchi, Y.; Atsumi, T.; Yamanaka, H.; Koike, T. Up-Regulated Expression of HLA-DRB5 Transcripts and High Frequency of the HLA-DRB5*01:05 Allele in Scleroderma Patients with Interstitial Lung Disease. Rheumatology 2012, 51, 1765–1774. [Google Scholar] [CrossRef] [Green Version]
- Bossini-Castillo, L.; Simeon, C.P.; Beretta, L.; Broen, J.C.; Vonk, M.C.; Ríos-Fernández, R.; Espinosa, G.; Carreira, P.; Camps, M.T.; Castillo, M.J.; et al. A Multicenter Study Confirms CD226 Gene Association with Systemic Sclerosis-Related Pulmonary Fibrosis. Arthritis Res. Ther. 2012, 14, R85. [Google Scholar] [CrossRef] [PubMed]
- Manetti, M.; Ibba-Manneschi, L.; Fatini, C.; Guiducci, S.; Cuomo, G.; Bonino, C.; Bazzichi, L.; Liakouli, V.; Giacomelli, R.; Abbate, R.; et al. Association of a Functional Polymorphism in the Matrix Metalloproteinase-12 Promoter Region with Systemic Sclerosis in an Italian Population. J. Rheumatol. 2010, 37, 1852–1857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sumita, Y.; Sugiura, T.; Kawaguchi, Y.; Baba, S.; Soejima, M.; Murakawa, Y.; Hara, M.; Kamatani, N. Genetic Polymorphisms in the Surfactant Proteins in Systemic Sclerosis in Japanese: T/T Genotype at 1580 C/T (Thr131Ile) in the SP-B Gene Reduces the Risk of Interstitial Lung Disease. Rheumatology 2007, 47, 289–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoshino, K.; Satoh, T.; Kawaguchi, Y.; Kuwana, M. Association of Hepatocyte Growth Factor Promoter Polymorphism with Severity of Interstitial Lung Disease in Japanese Patients with Systemic Sclerosis. Arthritis Rheum. 2011, 63, 2465–2472. [Google Scholar] [CrossRef] [PubMed]
- Dieudé, P.; Bouaziz, M.; Guedj, M.; Riemekasten, G.; Airò, P.; Müller, M.; Cusi, D.; Matucci-Cerinic, M.; Melchers, I.; Koenig, W.; et al. Evidence of the Contribution of the X Chromosome to Systemic Sclerosis Susceptibility: Association with the Functional IRAK1 196Phe/532Ser Haplotype. Arthritis Rheum. 2011, 63, 3979–3987. [Google Scholar] [CrossRef]
- Bredemeier, M.; Artur Bogo Chies, J.; Wieck, A.; Gatz Capobianco, K.; Hennemann Pitrez, E.; Eduardo Paim Rohde, L.; Fernando Furlan Pinotti, A.; Carlos Tavares Brenol, J.; Machado Xavier, R. TCRBV20S1 and TCRBV3S1 Gene Segment in Systemic Sclerosis. J. Rheumatol. 2008, 35, 1058–1063. [Google Scholar]
- Sharif, R.; Mayes, M.D.; Tan, F.K.; Gorlova, O.Y.; Hummers, L.K.; Shah, A.A.; Furst, D.E.; Khanna, D.; Martin, J.; Bossini-Castillo, L.; et al. IRF5 Polymorphism Predicts Prognosis in Patients with Systemic Sclerosis. Ann. Rheum. Dis. 2012, 71, 1197–1202. [Google Scholar] [CrossRef] [Green Version]
- Chinoy, H.; Salway, F.; Fertig, N.; Shephard, N.; Tait, B.D.; Thomson, W.; Isenberg, D.A.; Oddis, C.V.; Silman, A.J.; Ollier, W.E.; et al. In Adult Onset Myositis, the Presence of Interstitial Lung Disease and Myositis Specific/Associated Antibodies Are Governed by HLA Class II Haplotype, Rather Than by Myositis Subtype. Arthritis Res. Ther. 2006, 8, R13. [Google Scholar] [CrossRef] [Green Version]
- Gono, T.; Kawaguchi, Y.; Kuwana, M.; Sugiura, T.; Furuya, T.; Takagi, K.; Ichida, H.; Katsumata, Y.; Hanaoka, M.; Ota, Y.; et al. Brief Report: Association of HLA-DRB1*0101/*0405 with Susceptibility to Anti-Melanoma Differentiation-Associated Gene 5 Antibody-Positive Dermatomyositis in the Japanese Population. Arthritis Rheum. 2012, 64, 3736–3740. [Google Scholar] [CrossRef]
- Adegunsoye, A.; Vij, R.; Noth, I. Integrating Genomics Into Management of Fibrotic Interstitial Lung Disease. Chest 2019, 155, 1026–1040. [Google Scholar] [CrossRef]
- Amarnani, R.; Yeoh, S.-A.; Denneny, E.K.; Wincup, C. Lupus and the Lungs: The Assessment and Management of Pulmonary Manifestations of Systemic Lupus Erythematosus. Front. Med. 2021, 7, 610257. [Google Scholar] [CrossRef] [PubMed]
- Vacchi, C.; Sebastiani, M.; Cassone, G.; Cerri, S.; Della Casa, G.; Salvarani, C.; Manfredi, A. Therapeutic Options for the Treatment of Interstitial Lung Disease Related to Connective Tissue Diseases. A Narrative Review. J. Clin. Med. 2020, 9, 407. [Google Scholar] [CrossRef] [PubMed]
- Yoo, H.; Hino, T.; Hwang, J.; Franks, T.-J.; Han, J.; Im, Y.; Lee, H.-Y.; Chung, M.-P.; Hatabu, H.; Chung, M.P.; et al. Connective tissue disease-related interstitial lung disease (CTD-ILD) and interstitial lung abnormality (ILA): Evolving concept of CT findings, pathology and management. Eur. J. Radiol. Open 2022, 9, 100419. [Google Scholar] [CrossRef] [PubMed]
- Tansey, D.; Wells, A.-U.; Colby, T.-V.; Ip, S.; Nikolakoupolou, A.; du Bois, R.-M.; Hansell, D.-M.; Nicholson, A.-G. Variations in histological patterns of interstitial pneumonia between connective tissue disorders and their relationship to prognosis. Histopathology 2004, 44, 585–596. [Google Scholar] [CrossRef] [PubMed]
- Solomon, J.J.; Fischer, A. Connective Tissue Disease-Associated Interstitial Lung Disease: A Focused Review. J. Intensive. Care. Med. 2015, 30, 392–400. [Google Scholar] [CrossRef] [PubMed]
- Narváez, J.; Aburto, M.; Seoane-Mato, D.; Bonilla, G.; Acosta, O.; Candelas, G.; Cano-Jiménez, E.; Castellví, I.; González-Ruiz, J.M.; Corominas, H.; et al. Screening criteria for interstitial lung disease associated to rheumatoid arthritis: Expert proposal based on Delphi methodology. Reumatol. Clin. 2022, S2173-5743(22)00095-8. [Google Scholar] [CrossRef]
- Schneider, F.; Gruden, J.; Tazelaar, H.-D.; Leslie, K.-O. Pleuropulmonary pathology in patients with rheumatic disease. Arch. Pathol. Lab. Med. 2012, 136, 1242–1252. [Google Scholar] [CrossRef] [Green Version]
- Jeganathan, N.; Sathananthan, M. Connective Tissue Disease-Related Interstitial Lung Disease: Prevalence, Patterns, Predictors, Prognosis, and Treatment. Lung 2020, 198, 735–759. [Google Scholar] [CrossRef]
- Mira-Avendano, I.; Abril, A.; Burger, C.-D.; Dellaripa, P.-F.; Fischer, A.; Gotway, M.-B.; Lee, A.-S.; Lee, J.-S.; Matteson, E.-L.; Yi, E.S.; et al. Interstitial Lung Disease and Other Pulmonary Manifestations in Connective Tissue Diseases. Mayo Clin. Proc. 2019, 94, 309–325. [Google Scholar] [CrossRef] [Green Version]
- Garrote-Corral, S.; Silva-Fernández, L.; Seoane-Mato, D.; Guerra-Rodríguez, M.; Aburto, M.; Castañeda, S.; Valenzuela, C.; Narváez, J. Screening of interstitial lung disease in patients with rheumatoid arthritis: A systematic review. Reumatol. Clin. 2021, 18, 587–596. [Google Scholar] [CrossRef]
- Gargani, L.; Romei, C.; Bruni, C.; Lepri, G.; El-Aoufy, K.; Orlandi, M.; D’Errico, L.; Bandini, G.; D’Angelo, G.; Guiducci, S.; et al. Lung ultrasound B-lines in systemic sclerosis: Cut-off values and methodological indications for interstitial lung disease screening. Rheumatology 2022, 61, SI56–SI64. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Question | Consensus (n = 14) |
|---|---|
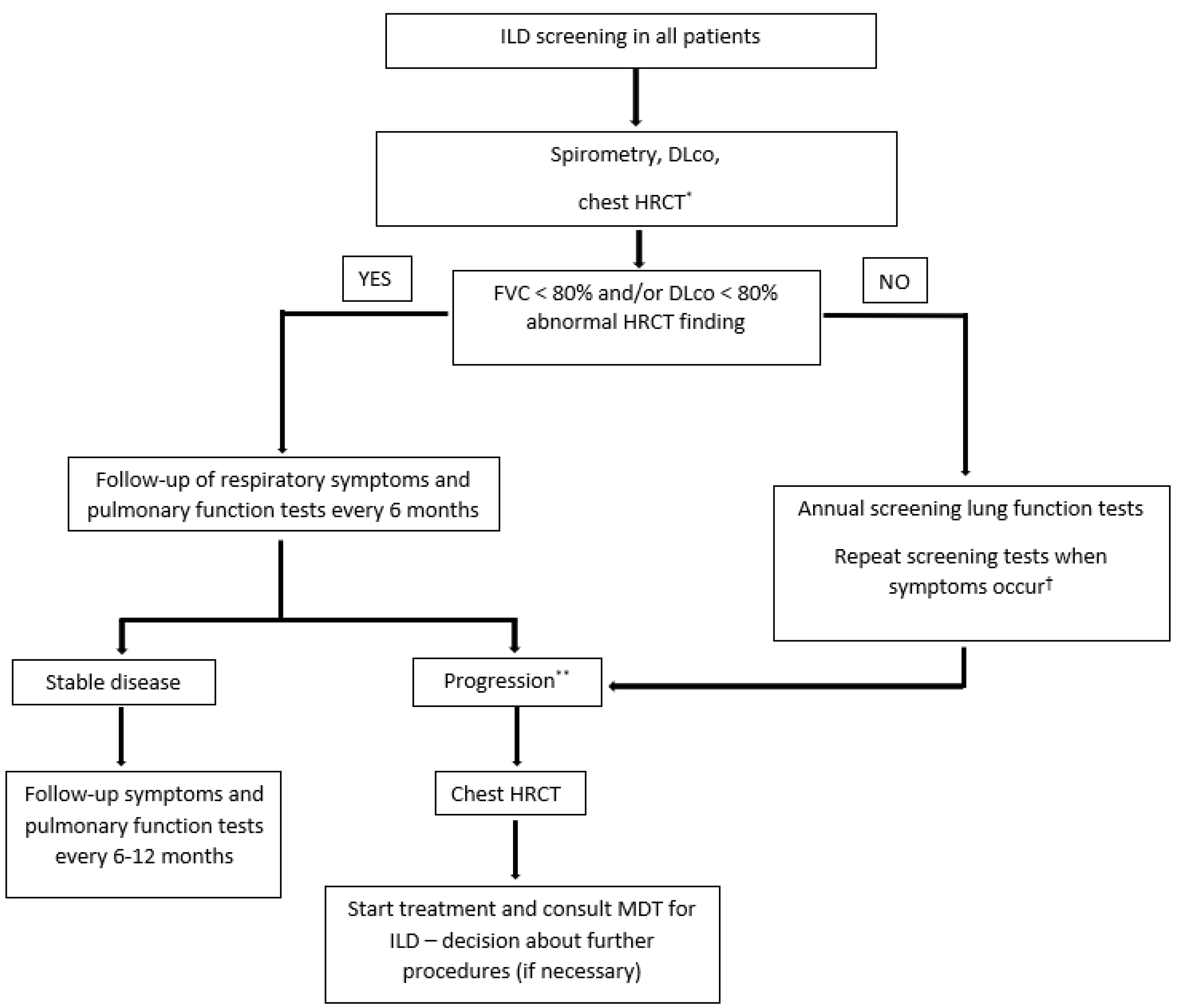
| 1. Should patients with newly diagnosed MCTD/SSc be referred to initial consultations for ILD screening (HRCT)? | Patients should be referred for ILD screening (n = 14) |
| 2. If you answered the previous question with yes, based on clinical judgment which of the following is important/essential in deciding on HRCT? | Pulmonary function tests (n = 13) Symptoms, i.e., exertional dyspnea (n = 11) |
| 3. If the patient does not have ILD (or other pulmonary pathology) on HRCT, how should possible ILD development be monitored in the patient? | Disease progression should be monitored by HRCT based on clinical judgment (n = 12) |
| 4. If you answered HRCT should be repeated based on clinical judgment, which of the following parameters should be taken into consideration when deciding? | Pulmonary function tests (n = 10) Symptoms, i.e., new onset of exertional dyspnea (n = 10) |
| 5. In a patient with MCTD/SSc and confirmed ILD, should HRCT be repeated during follow-up? | Disease progression should be monitored by HRCT based on clinical judgment (n = 12) |
| 6. If you answered HRCT should be repeated based on clinical judgment, which of the following parameters should be taken into consideration when deciding? | Pulmonary function tests (n = 11) Symptoms, i.e., new onset of exertional dyspnea (n = 9) |
| Question | Consensus (n = 14) |
|---|---|
| 1. Should patients with newly diagnosed pSS/SLE be referred to initial consultations for ILD screening (HRCT)? | Patients should be referred for ILD screening (n = 13) |
| 2. If you answered the previous question with yes, based on clinical judgment which of the following is important/essential in deciding on HRCT? | Pulmonary function tests (n = 13) Symptoms, i.e., exertional dyspnea or dry cough (n = 12) |
| 3. If the patient does not have ILD (or other pulmonary pathology) on HRCT, how should possible ILD development be monitored in the patient? | Disease progression should be monitored by HRCT based on clinical judgment (n = 13) |
| 4. If you answered HRCT should be repeated based on clinical judgment, which of the following parameters should be taken into consideration when deciding? | Symptoms, i.e., new onset of dry cough (n = 12) Pulmonary function tests (n = 10) |
| 5. In a patient with pSS/SLE and confirmed ILD, should HRCT be repeated during follow-up? | Disease progression should be monitored by HRCT based on clinical judgment (n = 14) |
| 6. If you answered HRCT should be repeated based on clinical judgment, which of the following parameters should be taken into consideration when deciding? | Pulmonary function tests (n = 13) Symptoms, i.e., new onset of exertional dyspnea or dry cough (n = 11) |
| Question | Consensus (n = 14) |
|---|---|
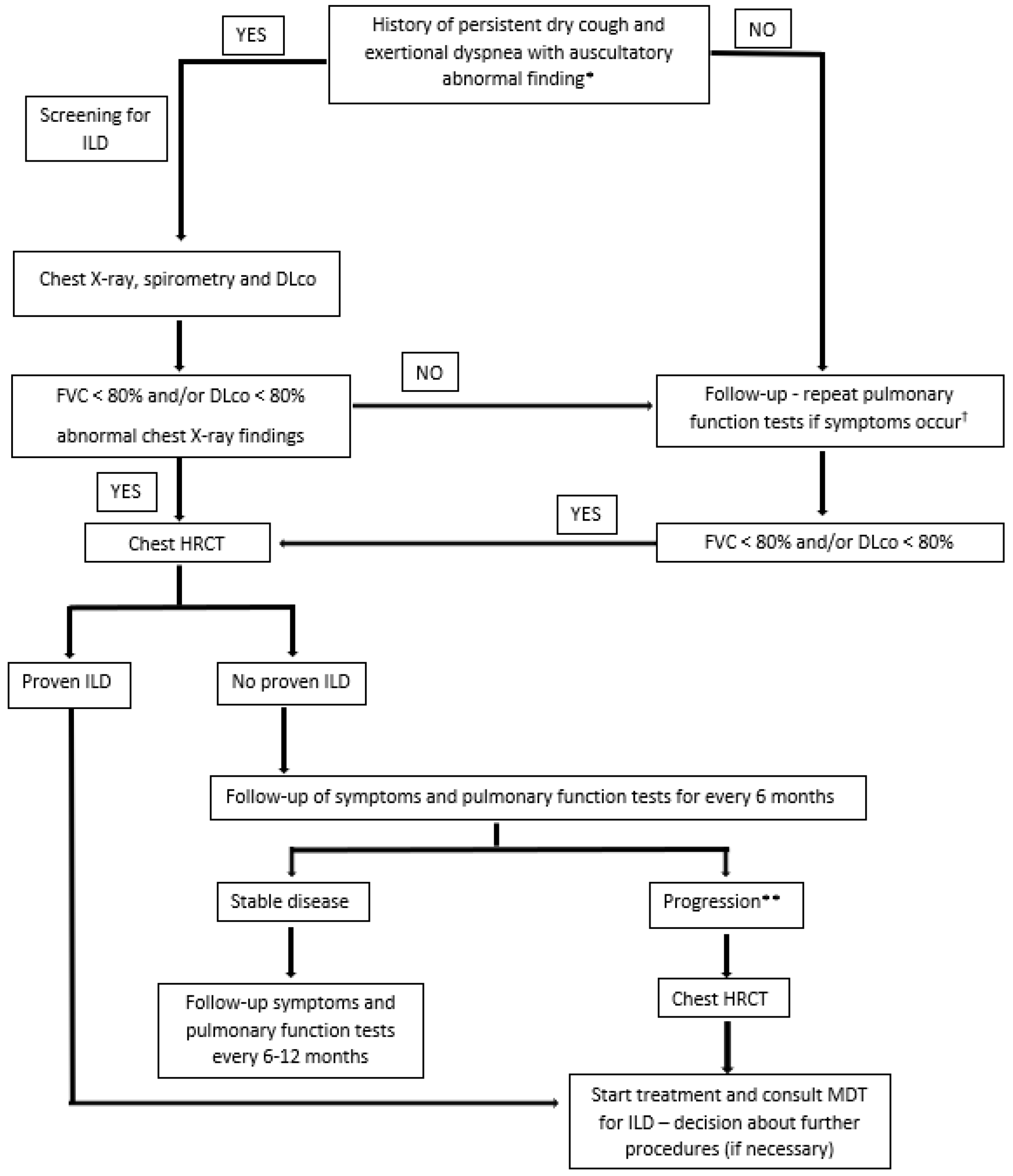
| 1. Should patients with newly diagnosed RA be referred for mandatory ILD screening? | Patients should be referred for screening (n = 14) |
| 2. What is the most important clinical symptom in newly diagnosed RA patients indicating to ILD? | Exertional dyspnea (n = 13) Persistent dry cough (n = 12) |
| 3. What is the most important screening test for ILD in newly diagnosed RA patients? | Pulmonary function tests (n = 14) |
| 4. What are the most relevant pulmonary function test results for ILD screening? | DLco < 80% of predictive value (n = 14) FVC < 80% of predictive value (n = 13) |
| 5. What test should be considered crucial for follow-up in RA patients with confirmed ILD? | Pulmonary function tests (n = 14) Clinical examination (n = 10) HRCT (n = 8) |
| 6. What should be considered crucial for follow-up in RA patients without confirmed ILD? | Clinical monitoring (n = 13) |
| 7. How often should chest X-ray be repeated in stable RA-ILD patients? | In case of symptom worsening (n = 9) |
| 8. How often should pulmonary function tests be repeated in stable RA-ILD patients? | Every 6–12 months (n = 12) |
| 9. How often should HRCT be repeated in stable RA-ILD patients? | In case of symptom worsening (n = 13) |
| 10. How often should chest X-ray be repeated in stable RA patients without confirmed ILD? | In case of symptom worsening (n = 13) |
| 11. How often should pulmonary function tests be repeated in stable RA patients without confirmed ILD? | In case of symptom worsening (n = 9) Every 12 months (n = 5) |
| 12. How often should HRCT be repeated in stable RA patients without confirmed ILD? | In case of symptom worsening (n = 12) |
| Question | Consensus (n = 14) |
|---|---|
| 1. Should patients with newly diagnosed IIM be referred for mandatory ILD screening? | Patients should be referred for screening (n = 13) |
| 2. What is the most important clinical symptom in newly diagnosed IIM patients indicating to ILD? | Persistent dry cough (n = 12) Exertional dyspnea (n = 11) |
| 3. What is the most important screening test for ILD in newly diagnosed IIM patients? | Pulmonary function tests (n = 14) Serological test (n = 13) Clinical examination (n = 11) |
| 4. What are the most relevant pulmonary function test results for ILD screening? | DLco < 80% of predictive value (n = 14) FVC < 80% of predictive value (n = 13) |
| 5. What test should be considered crucial for follow-up in IIM patients with confirmed ILD? | Pulmonary function tests (n = 14) Clinical examination (n = 10) HRCT (n = 8) |
| 6. What should be considered crucial for follow-up in IIM patients without confirmed ILD? | Pulmonary function tests (n = 13) Clinical monitoring (n = 11) |
| 7. How often should chest X-ray be repeated in stable IIM-ILD patients? | In case of symptom worsening (n = 9) |
| 8. How often should pulmonary function tests be repeated in stable IIM-ILD patients? | Every 6–12 months (n = 14) |
| 9. How often should HRCT be repeated in stable IIM-ILD patients? | In case of symptom worsening (n = 13) |
| 10. How often should chest X-ray be repeated in stable IIM patients without confirmed ILD? | In case of symptom worsening (n = 13) Every 12 months (n = 3) |
| 11. How often should pulmonary function tests be repeated in stable IIM patients without confirmed ILD? | Every 12 months (n = 10) In case of symptom worsening (n = 3) |
| 12. How often should HRCT be repeated in stable IIM patients without confirmed ILD? | In case of symptom worsening (n = 13) |
| Disease | Susceptibility Genes | Autoantibodies and Serological Immune Markers |
|---|---|---|
| RA-ILD [10,11,12,13,14,15,16] | DRB1 * 16:02, DRB1 * 15:02 TERT, RTEL1, PARN or SFTPC MUC5B | RF anti-CCP |
| SSc-ILD [10,17,18,19,20,21,22,23,24,25,26,27,28,29] | HLA-B * 62, HLA-C * 06, DRB1 * 11 DPB1 * 03:01, DR51 CD226, MMP12, SFTPB, CTGF, HGF, IRAK1, TCRBV, IRF5 CD247 | anti-Scl-70 anti-U3RNP anti-U11/U12RNP anti-RuvBL1/2 anti-EIF2B anti-PM-Scl anti-U1RNP anti-cardiolipin anti-Th/To anti-Ro52 anti-NOR90 nucleolar ANA ANCA |
| PM/DM-ILD [10,30,31] | DRB1 * 03, DRB1 * 01:01, DRB1 * 04:05 DQB1 * 06:02 | MSAs anti-Jo-1 anti-PL-12 anti-PL-7 anti-KS anti-OJ anti-EJ anti-Zo anti-Ku anti-MDA5 MAAs anti-Ro52/60 anti-U1RNP |
| MCTD-ILD [10,32] | TERC, TERT | Anti-U1RNP CIC C3 CH50 |
| pSS-ILD [10] | anti-SSA/Ro anti-SSB/La | |
| SLE-ILD [33] | anti-La anti-Scl-70 anti-U1RNP |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radić, M.; Novak, S.; Barešić, M.; Hećimović, A.; Perković, D.; Tekavec-Trkanjec, J.; Mayer, M.; Prus, V.; Morović-Vergles, J.; Marasović Krstulović, D.; et al. Delphi-Based Consensus on Interstitial Lung Disease Screening in Patients with Connective Tissue Diseases (Croatian National-Based Study). Biomedicines 2022, 10, 3291. https://doi.org/10.3390/biomedicines10123291
Radić M, Novak S, Barešić M, Hećimović A, Perković D, Tekavec-Trkanjec J, Mayer M, Prus V, Morović-Vergles J, Marasović Krstulović D, et al. Delphi-Based Consensus on Interstitial Lung Disease Screening in Patients with Connective Tissue Diseases (Croatian National-Based Study). Biomedicines. 2022; 10(12):3291. https://doi.org/10.3390/biomedicines10123291
Chicago/Turabian StyleRadić, Mislav, Srđan Novak, Marko Barešić, Ana Hećimović, Dijana Perković, Jasna Tekavec-Trkanjec, Miroslav Mayer, Višnja Prus, Jadranka Morović-Vergles, Daniela Marasović Krstulović, and et al. 2022. "Delphi-Based Consensus on Interstitial Lung Disease Screening in Patients with Connective Tissue Diseases (Croatian National-Based Study)" Biomedicines 10, no. 12: 3291. https://doi.org/10.3390/biomedicines10123291