
Oxaliplatin-Related Hypersensitivity Reactions: A Single Institution Series and Literature Review

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shao, Y.-Y.; Hu, F.-C.; Liang, J.-T.; Chiu, W.-T.; Cheng, A.-L.; Yang, C.-H. Characteristics and risk factors of oxaliplatin-related hypersensitivity reactions. J. Formos. Med. Assoc. 2010, 109, 362–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, B.B.; Cuddahy, T.; Briscella, C.; Ross, N.; Olszanski, A.; Denlinger, C.S. Oxaliplatin: Detection and Management of Hypersensitivity Reactions. Clin. J. Oncol. Nurs. 2019, 23, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.H.; Bradley, T.; Tai, J.; Budman, D.R. Hypersensitivity to oxaliplatin: An investigation of incidence and risk factors and literature review. Oncology 2009, 76, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Huang, R.; Zhao, L.; Wang, X.; Shangguan, X.; Li, W.; Li, M.; Yin, X.; Zhang, C.; Liu, D. Safety Profile of Oxaliplatin in 3,687 Patients With Cancer in China: A Post-Marketing Surveillance Study. Front. Oncol. 2021, 11, 757196. [Google Scholar] [CrossRef]
- Hewitt, M.R.; Sun, W. Oxaliplatin-associated hypersensitivity reactions: Clinical presentation and management. Clin. Color. Cancer 2006, 6, 114–117. [Google Scholar] [CrossRef]
- Palapinyo, S.; Klaewsongkram, J.; Sriuranpong, V.; Areepium, N. Incidence of oxaliplatin hypersensitivity reaction among colorectal cancer patients: A 5-year retrospective study. Pharm. Pract. 2022, 20, 2635. [Google Scholar] [CrossRef]
- Yanai, T.; Iwasa, S.; Hashimoto, H.; Kato, K.; Hamaguchi, T.; Yamada, Y.; Shimada, Y.; Yamamoto, H. Successful Rechallenge for Oxaliplatin Hypersensitivity Reactions in Patients with Metastatic Colorectal Cancer. Anticancer Res. 2012, 32, 5521–5526. [Google Scholar]
- Saif, M.W. Hypersensitivity reactions associated with oxaliplatin. Expert Opin. Drug Saf. 2006, 5, 687–694. [Google Scholar] [CrossRef]
- Syrigou, E.; Makrilia, N.; Koti, I.; Saif, M.W.; Syrigos, K.N. Hypersensitivity reactions to antineoplastic agents: An overview. Anti-Cancer Drugs 2009, 20, 1–6. [Google Scholar] [CrossRef]
- Castells, M.; Sancho-Serra, M.D.C.; Simarro, M. Hypersensitivity to antineoplastic agents: Mechanisms and treatment with rapid desensitization. Cancer Immunol. Immunother. 2012, 61, 1575–1584. [Google Scholar] [CrossRef]
- Wang, G.; Yang, B.; Fu, Z.; Wang, X.; Zhang, Z. Efficacy and safety of oxaliplatin-based regimen versus cisplatin-based regimen in the treatment of gastric cancer: A meta-analysis of randomized controlled trials. Int. J. Clin. Oncol. 2019, 24, 614–623. [Google Scholar] [CrossRef] [PubMed]
- Aroldi, F.; Prochilo, T.; Bertocchi, P.; Zaniboni, A. Oxaliplatin-induced hypersensitivity reaction: Underlying mechanisms and management. J. Chemother. 2015, 27, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Syrigou, E.; Syrigos, K.; Saif, M.W. Hypersensitivity reactions to oxaliplatin and other antineoplastic agents. Curr. Allergy Asthma Rep. 2008, 8, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Bano, N.; Najam, R.; Qazi, F.; Mateen, A. Clinical Features of Oxaliplatin Induced Hypersensitivity Reactions and Therapeutic Approaches. Asian Pac. J. Cancer Prev. 2016, 17, 1637–1641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parel, M.; Ranchon, F.; Nosbaum, A.; You, B.; Vantard, N.; Schwiertz, V.; Gourc, C.; Gauthier, N.; Guedat, M.-G.; He, S.; et al. Hypersensitivity to oxaliplatin: Clinical features and risk factors. BMC Pharmacol. Toxic. 2014, 15, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maindrault-Goebel, F.; André, T.; Tournigand, C.; Louvet, C.; Perez-Staub, N.; Zeghib, N.; De Gramont, A. Allergic-type reactions to oxaliplatin: Retrospective analysis of 42 patients. Eur. J. Cancer 2005, 41, 2262–2267. [Google Scholar] [CrossRef]
- Polyzos, A.; Tsavaris, N.; Gogas, H.; Souglakos, J.; Vambakas, L.; Vardakas, N.; Polyzos, K.; Tsigris, C.; Mantas, D.; Papachristodoulou, A.; et al. Clinical features of hypersensitivity reactions to oxaliplatin: A 10-year experience. Oncology. 2009, 76, 36–41. [Google Scholar] [CrossRef]
- Martinez, S.A.; Segal, N.H.; Cercek, A.; Yaeger, R.; Stadler, Z.; Kemeny, N.E.; Nusrat, M.; Shahrokni, A.; Connell, L.; Saltz, L.B. Simplified Graded Infusion Strategy for Mitigation of Oxaliplatin Hypersensitivity. Clin. Color. Cancer 2022, 21, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Lee, J.-H.; Kim, S.; Kim, S.; Park, K.H.; Lee, C.; Kang, B.; Beom, S.-H.; Shin, S.J.; Jung, M.; et al. A New Practical Desensitization Protocol for Oxaliplatin-Induced Immediate Hypersensitivity Reactions: A Necessary and Useful Approach. J. Investig. Allergol. Clin. Immunol. 2016, 26, 168–176. [Google Scholar] [CrossRef] [Green Version]
- US Department of Health and Human Services. Common Terminology Criteria for Adverse Events. Version 5.0. Published 27 November 2017. 2020. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf (accessed on 3 October 2022).
- Thomas, R.R.; Quinn, M.G.; Schuler, B.; Grem, J.L. Hypersensitivity and idiosyncratic reactions to oxaliplatin. Cancer 2003, 97, 2301–2307. [Google Scholar] [CrossRef]
- Siu, S.W.K.; Chan, R.T.T.; Au, G.K.H. Hypersensitivity reactions to oxaliplatin: Experience in a single institute. Ann. Oncol. 2006, 17, 259–261. [Google Scholar] [CrossRef]
- A Bautista, M.; Stevens, W.T.; Chen, C.-S.; Curtis, B.R.; Aster, R.H.; Hsueh, C.-T. Hypersensitivity reaction and acute immune-mediated thrombocytopenia from oxaliplatin: Two case reports and a review of the literature. J. Hematol. Oncol. 2010, 26, 3–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brandi, G.; Pantaleo, M.A.; Galli, C.; Falcone, A.; Antonuzzo, A.; Mordenti, P.; Di Marco, M.C.; Biasco, G. Hypersensitivity reactions related to oxaliplatin (OHP). Br. J. Cancer 2003, 89, 477–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sohn, K.-H.; Kang, D.-Y.; Kim, J.-Y.; Lee, S.-Y.; Lee, K.-H.; Han, S.-W.; Kang, H.-R. Incidence and Risk of Oxaliplatin-Induced Hypersensitivity in Patients with Asymptomatic Prior Exposure: A Prospective Observational Study. J. Allergy Clin. Immunol. Pract. 2018, 6, 1642–1648. [Google Scholar] [CrossRef] [PubMed]
- Mori, Y.; Nishimura, T.; Kitano, T.; Yoshimura, K.-I.; Matsumoto, S.; Kanai, M.; Hazama, M.; Ishiguro, H.; Nagayama, S.; Yanagihara, K.; et al. Oxaliplatin-free interval as a risk factor for hypersensitivity reaction among colorectal cancer patients treated with FOLFOX. Oncology 2010, 79, 136–143. [Google Scholar] [CrossRef]
- Couraud, S.; Planus, C.; Rioufol, C.; Mornex, F. Hypersensibilité aux sels de platine. Rev. De Pneumol. Clin. 2008, 64, 20–26. [Google Scholar] [CrossRef]
- Lenz, G.; Hacker, U.T.; Kern, W.; Schalhorn, A.; Hiddemann, W. Adverse reactions to oxaliplatin: A retrospective study of 25 patients treated in one institution. Anticancer Drugs 2003, 14, 731–733. [Google Scholar] [CrossRef]
- Okayama, T.; Ishikawa, T.; Sugatani, K.; Yoshida, N.; Kokura, S.; Matsuda, K.; Tsukamoto, S.; Ihara, N.; Kuriu, Y.; Nakanishi, M.; et al. Hypersensitivity reactions to oxaliplatin: Identifying the risk factors and judging the efficacy of a desensitization protocol. Clin. Ther. 2015, 37, 1259–1269. [Google Scholar] [CrossRef]
- Wu, Y.; Aravind, S.; Nalysnyk, L.; Ranganathan, M.G. Dose Delay Amongst Cancer Patients Undergoing Chemotherapy. Blood 2008, 112, 4698. [Google Scholar] [CrossRef]
- Roselló, S.; Blasco, I.; Fabregat, L.G.; Cervantes, A.; Jordan, K. ESMO Guidelines Committee. Management of infusion reactions to systemic anticancer therapy: ESMO Clinical Practice Guidelines. Ann. Oncol. 2018, 29 (Suppl. S4), 260. [Google Scholar] [CrossRef]
- Gowda, A.; Goel, R.; Berdzik, J.; Leichman, C.G.; Javle, M. Hypersensitivity Reactions to oxaliplatin: Incidence and management. Oncology 2004, 18, 1671–1684. [Google Scholar]
- Rottenberg, S.; Disler, C.; Perego, P. The rediscovery of platinum-based cancer therapy. Nat. Rev. Cancer 2021, 21, 37–50. [Google Scholar] [CrossRef]
- Torres, M.J. The complexity of drug hypersensitivity reactions. Allergy 2021, 76, 985–987. [Google Scholar] [CrossRef] [PubMed]
- Rébé, C.; Demontoux, L.; Pilot, T.; Ghiringhelli, F. Platinum Derivatives Effects on Anticancer Immune Response. Biomolecules 2019, 10, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, D.Y.Q.; Yeo, C.H.F.; Ang, W.H. Immuno-chemotherapeutic platinum(IV) prodrugs of cisplatin as multimodal anticancer agents. Angew. Chem. Int. Ed. Engl. 2014, 53, 6752–6756. [Google Scholar] [CrossRef] [PubMed]
- Pichler, W.J. Delayed drug hypersensitivity reactions. Ann. Intern. Med. 2003, 139, 683–693. [Google Scholar] [CrossRef]
- Kantari, C.; Pederzoli-Ribeil, M.; Witko-Sarsat, V. The role of neutrophils and monocytes in innate immunity. Contrib. Microbiol. 2008, 15, 118–146. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Krempski, J.W.; Nadeau, K. Advances and novel developments in mechanisms of allergic inflammation. Allergy 2020, 75, 3100–3111. [Google Scholar] [CrossRef]
- Seki, K.; Tsuduki, Y.; Ioroi, T.; Yamane, M.; Yamauchi, H.; Shiraishi, Y.; Ogawa, T.; Nakata, I.; Nishiguchi, K.; Matsubayashi, T.; et al. Serum lactate dehydrogenase levels as a predictive marker of oxaliplatin-induced hypersensitivity reactions in Japanese patients with advanced colorectal cancer. Int. J. Med. Sci. 2014, 11, 641–645. [Google Scholar] [CrossRef]


{kind=link}
| Study Population | Pts with HSRs | |
|---|---|---|
| n = 153 1 | n = 17 | |
| (100%) | (11%) | |
| Female | 83 (54.3) | 10 (58.8) |
| Male | 70 (45.7) | 7 (41.2) |
| Age, years | 70 (27–87) | 69 (51–82) |
| (median, range) | ||
| Diagnosis | ||
| Colorectal cancer | 108 (70.6) | 14 (82.4) |
| Pancreatic cancer | 12 (7.8) | 1 (5.9) |
| Biliary tract cancer | 6 (3.9) | 2 (11.7) |
| Stomach cancer | 26 (17.0) | 0 (0) |
| Esophagus cancer | 1 (0.7) | 0 (0) |
| Chemotherapy regimen | ||
| FOLFOX | 21 (13.7) | 2 (11.7) |
| XELOX | 71 (46.4) | 6 (35.3) |
| FOLFOX + bevacizumab | 17 (11.0) | 1 (5.9) |
| FOLFOX + cetuximab | 2 (1.3) | 2 (11.7) |
| FOLFOX + panitumumab | 13 (8.5) | 2 (11.7) |
| FOLFOX + trastuzumab | 1 (0.7) | 0 (0) |
| FLOT | 6 (3.9) | 0 (0) |
| FOLFIRINOX | 3 (2.0) | 0 (0) |
| FOLFOXIRI + bevacizumab | 4 (2.6) | 2 (11.7) |
| XELOX + bevacizumab | 13 (8.5) | 2 (11.7) |
| XELOX + trastuzumab | 2 (1.3) | 0 (0) |
| Purpose of treatment | ||
| Adjuvant | 65 (42.5) | 3 (17.6) |
| Palliative | 88 (57.5) | 14 (82.4) |
| Prior exposure to platinum salts 2 | ||
| Yes | 30 (19.6) | 8 (47.1) |
| No | 123 (80.4) | 9 (52.9) |
| Number of infusions | ||
| Median (range) | 5 (1–12) | 6 (1–11) |
| Premedication 3 | ||
| Steroids (8 mg) | 13 (8.5) | 2 (11.7) |
| Steroids (12 mg) | 137 (89.5) | 13 (76.5) |
| Steroids (18.8 mg) | 0 (0) | 1 (5.9) |
| Antihistamines (10 mg) | 37 (24.2) | 5 (29.4) |
| Antiemetics | 153 (100) | 17 (100) |
| History of allergic diseases | ||
| Yes | 22 (14.4) | 3 (17.6) |
| No | 131 (85.6) | 14 (82.4) |
| Total Reactions | n = 17 (%) |
|---|---|
| Severity 1 | |
| Grade 1 | 1 (5.9) |
| Grade 2 | 3 (17.6) |
| Grade 3 | 12 (70.6) |
| Grade 4 | 1 (5.9) |
| Grade 5 | 0 (0) |
| Cycle number of event (median, range) | 2 (1–11) |
| Premedication | |
| Steroids | 17 (100) |
| Antihistamines | 5 (29.4) |
| Antiemetics | 17 (100) |
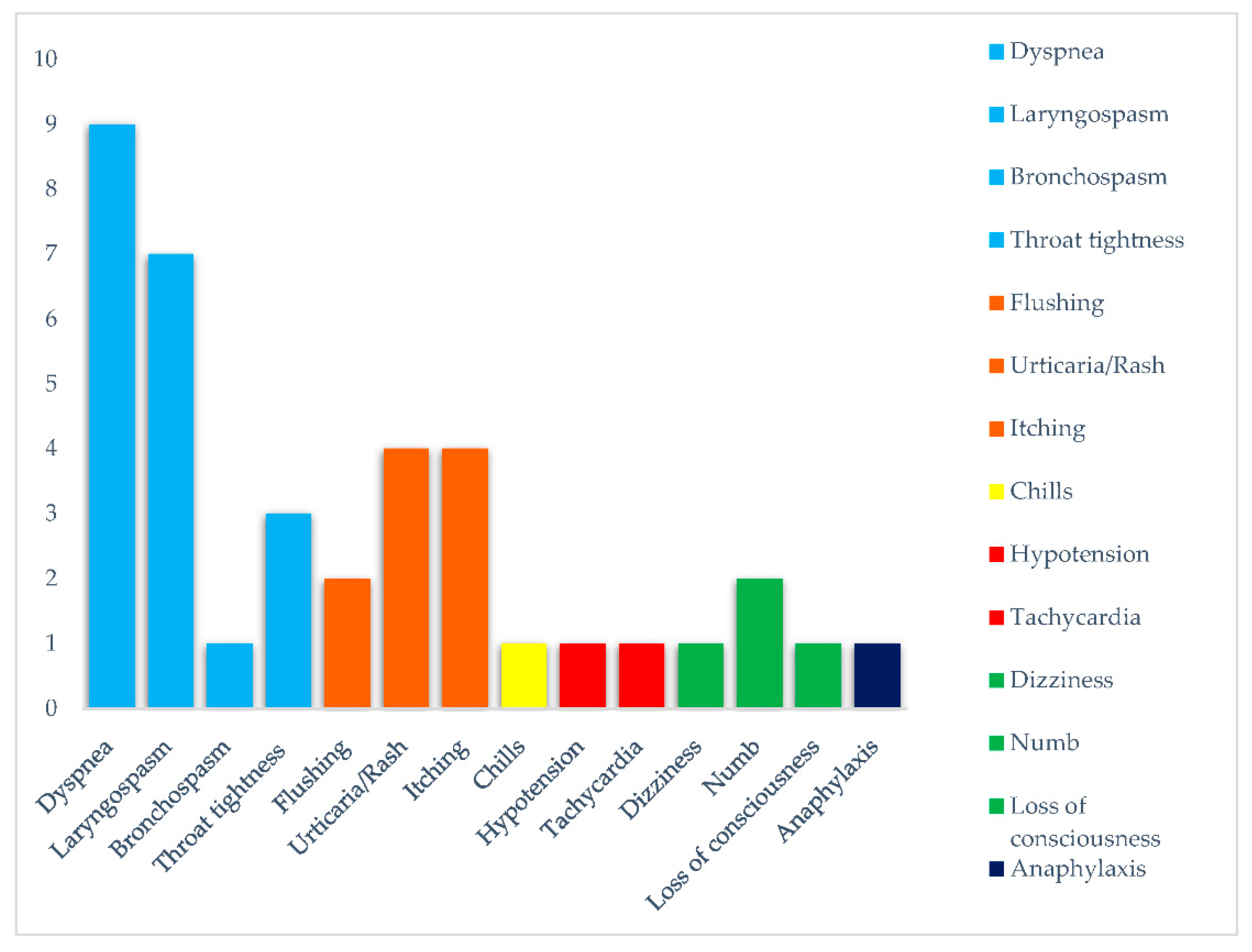
| Symptoms | |
| Respiratory | |
| Dyspnea | 9 (52.9) |
| Laryngospasm | 7 (41.2) |
| Bronchospasm | 1 (5.9) |
| Throat tightness | 3 (17.6) |
| Cutaneous | |
| Flushing | 2 (11.7) |
| Urticaria/rash | 4 (23.5) |
| Itching | 4 (23.5) |
| General | |
| Chills | 1 (5.9) |
| Cardiovascular | |
| Hypotension | 1 (5.9) |
| Tachycardia | 1 (5.9) |
| Neurological | |
| Dizziness | 1 (5.9) |
| Numb | 2 (11.7) |
| Loss of consciousness | 1 (5.9) |
| Anaphylaxis | 1 (5.9) |
| Management of reaction | |
| Infusion interruption | 17 (100) |
| Steroids administration | 14 (82.4) |
| Antihistamines administration | 5 (29.4) |
| Oxygen administration | 3 (17.6) |
| Saline solution administration | 3 (17.6) |
| Epinephrine administration | 1 (5.9) |
| Rechallenge | |
| Yes | 13 (76.5) |
| No | 4 (23.5) |
| Subsequent Reaction | |
| Yes | 6 (46.2) |
| No | 7 (53.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbin, F.; Ghidini, M.; Panichi, A.; Tomasello, G.; Bareggi, C.; Galassi, B.; Denaro, N.; Ruatta, F.; Cauchi, C.; Rossino, M.G.; et al. Oxaliplatin-Related Hypersensitivity Reactions: A Single Institution Series and Literature Review. Biomedicines 2022, 10, 3275. https://doi.org/10.3390/biomedicines10123275
Barbin F, Ghidini M, Panichi A, Tomasello G, Bareggi C, Galassi B, Denaro N, Ruatta F, Cauchi C, Rossino MG, et al. Oxaliplatin-Related Hypersensitivity Reactions: A Single Institution Series and Literature Review. Biomedicines. 2022; 10(12):3275. https://doi.org/10.3390/biomedicines10123275
Chicago/Turabian StyleBarbin, Francesca, Michele Ghidini, Alessandra Panichi, Gianluca Tomasello, Claudia Bareggi, Barbara Galassi, Nerina Denaro, Fiorella Ruatta, Carolina Cauchi, Maria Grazia Rossino, and et al. 2022. "Oxaliplatin-Related Hypersensitivity Reactions: A Single Institution Series and Literature Review" Biomedicines 10, no. 12: 3275. https://doi.org/10.3390/biomedicines10123275