
Molecular Diagnostic Tools against SARS-CoV-2 in Poland in 2022


Abstract
:1. Introduction
- Nasopharyngeal swabs, with a relatively very high positive rate of 92.2%; the disadvantage is that sampling is uncomfortable for patients [2];
- BALF (bronchoalveolar lavage fluid), with an improvement of diagnostic accuracy in severe cases; however, it requires both a suction device and a skilled operator, and it is also a painful process for the patients. Examination of BAL fluid has been shown to have a sensitivity of 90–100% [3];
- Rectal swabs or stools, with positive rates varying from 29% to 83.3% [3]; such a wide range of the value has resulted in this method not being adopted in Poland;
- Blood, with a highly unsatisfactory sensitivity of 7.3% [4]. This result implies that COVID-19 diagnostics should not be performed on blood samples; however, since it is stated that viremia in COVID-19 may occur, nurses and diagnosticians should be particularly careful when working with the blood of infected patients);
- Urine is unsuitable for diagnostics, with a sensitivity of tests on this material close to 0% [4].
2. Method Types
2.1. RT-qPCR
2.2. Isothermal Amplification Methods
2.2.1. RT-LAMP (Reverse Transcription Loop-Mediated Isothermal Amplification)
2.2.2. CRISPR (Clustered Regularly Interspaced Short Palindromic Repeats)
2.3. Genomic Sequencing
2.4. An Alternative to NAATs
2.5. Diagnostic Windows
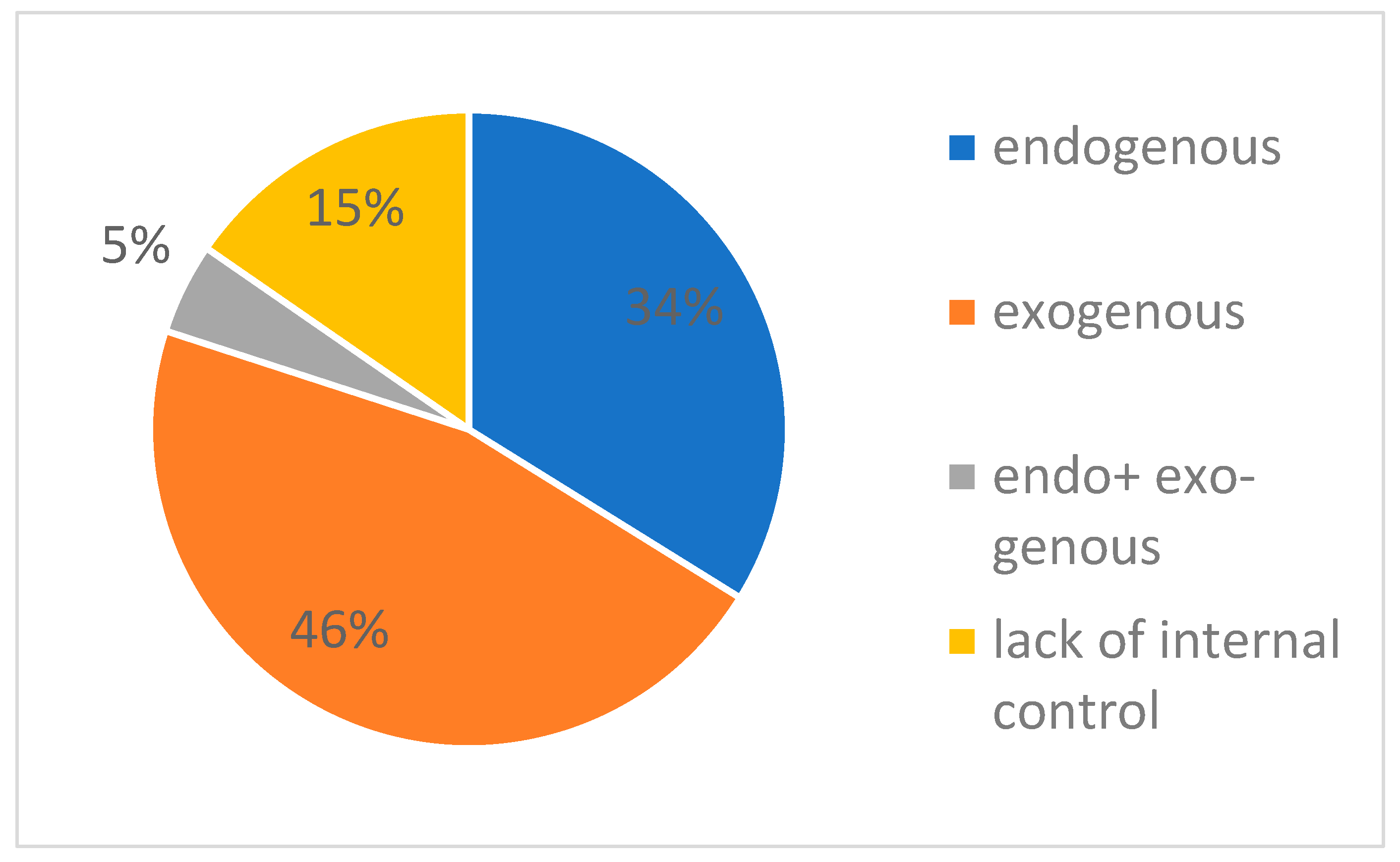
3. Diagnostic Errors and Ways to Prevent Them
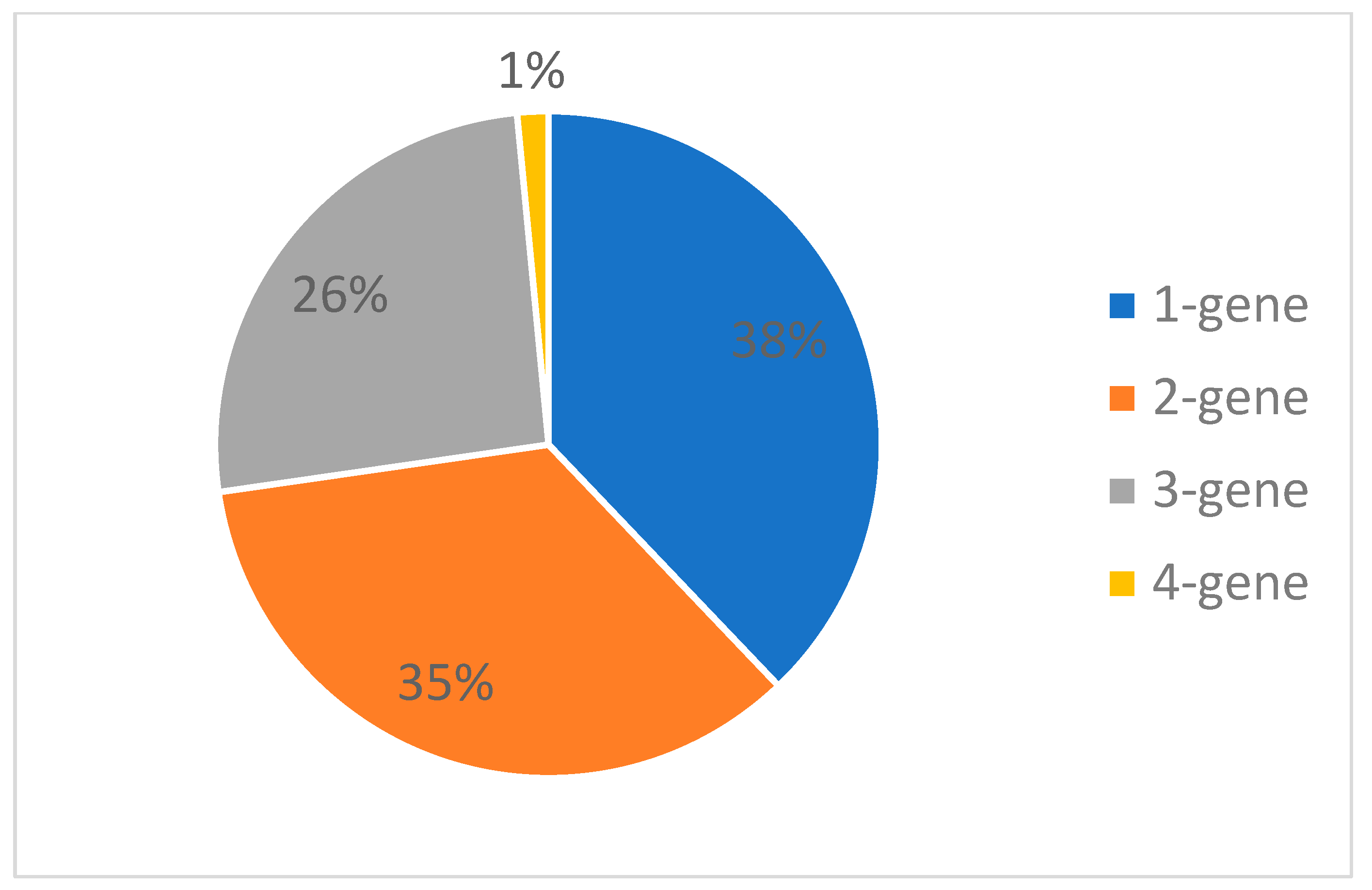
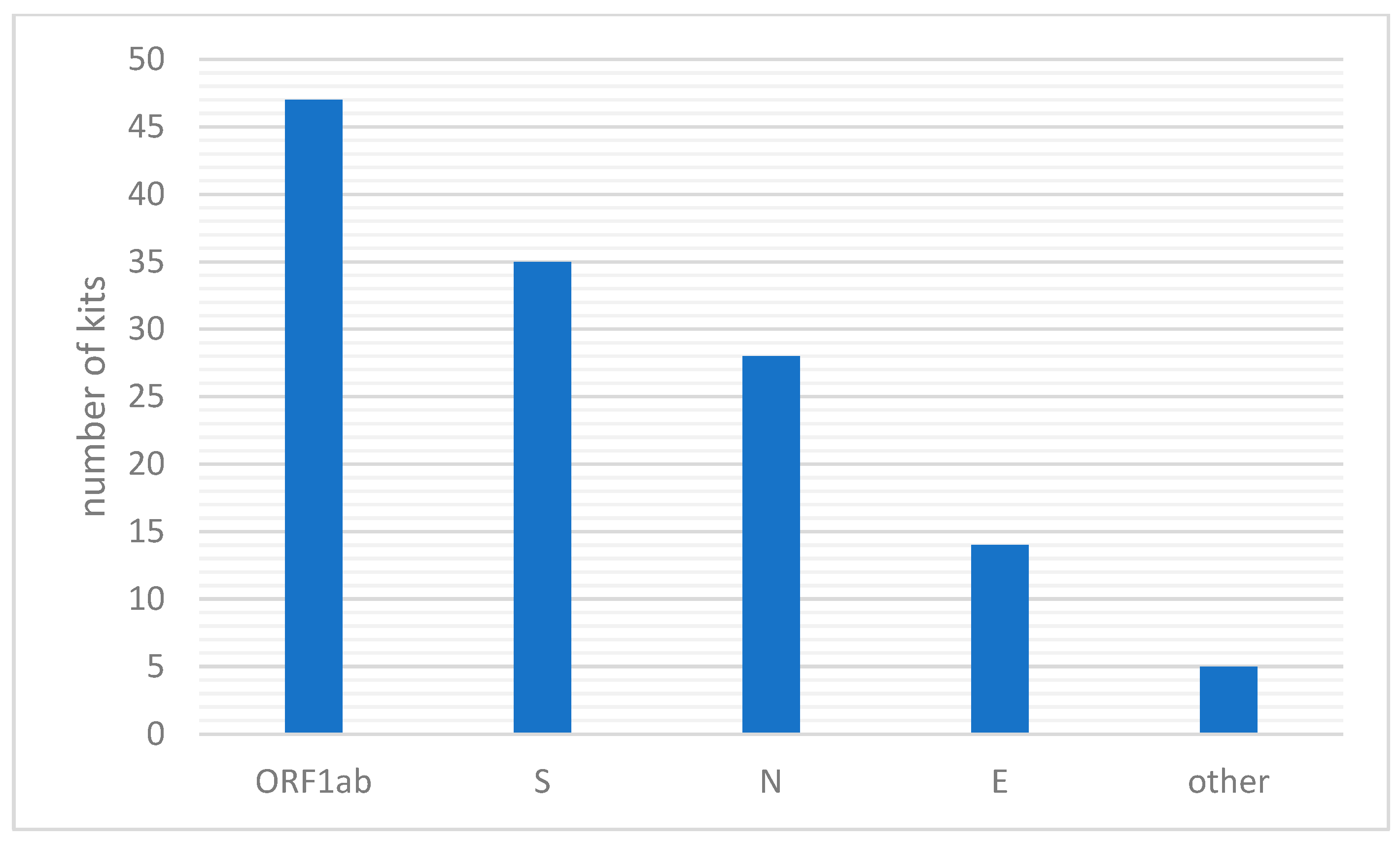
4. What Genes Are Analyzed in PCR for the Detection of SARS-CoV-2?
5. Do Diagnostic Kits Detect Current SARS-CoV-2 Variants?
6. Recurrence of Positive SARS-CoV-2 in Patients Recovered from COVID-19
7. Additional Advantages of Some Tests: Multiplexing—Detection of Other Pathogens in One Test
8. Comparison of Diagnostic Products Dedicated to the Detection of SARS-CoV-2 Available in Poland to Those Available in Other Countries
9. Summary and Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arena, F.; Pollini, S.; Rossolini, G.M.; Margaglione, M. Summary of the Available Molecular Methods for Detection of SARS-CoV-2 during the Ongoing Pandemic. Int. J. Mol. Sci. 2021, 22, 1298. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.A.; Herigon, J.C.; Benedetti, A.; Pollock, N.R.; Denkinger, C.M. Performance of Saliva, Oropharyngeal Swabs, and Nasal Swabs for SARS-CoV-2 Molecular Detection: A Systematic Review and Meta-analysis. J. Clin. Microbiol. 2021, 59, e02881-20. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Yang, M.; Yuan, J.; Wang, F.; Wang, Z.; Li, J.; Zhang, M.; Xing, L.; Wei, J.; Peng, L.; et al. Laboratory Diagnosis and Monitoring the Viral Shedding of SARS-CoV-2 Infection. Innovation 2020, 1, 100061. [Google Scholar] [CrossRef] [PubMed]
- Böger, B.; Fachi, M.M.; Vilhena, R.O.; Cobre, A.F.; Tonin, F.S.; Pontarolo, R. Systematic review with meta-analysis of the accuracy of diagnostic tests for COVID-19. Am. J. Infect. Control 2021, 49, 21–29. [Google Scholar] [CrossRef]
- Datta, M.; Singh, D.D.; Naqvi, A.R. Molecular Diagnostic Tools for the Detection of SARS-CoV-2. Int. Rev. Immunol. 2021, 40, 143–156. [Google Scholar] [CrossRef]
- Moreira, V.M.; Mascarenhas, P.; Machado, V.; Botelho, J.; Mendes, J.J.; Taveira, N.; Almeida, M.G. Diagnosis of SARS-CoV-2 Infection by RT-PCR Using Specimens Other Than Naso- and Oropharyngeal Swabs: A Systematic Review and Meta-Analysis. Diagnostics 2021, 11, 363. [Google Scholar] [CrossRef]
- Ruhan, A.; Wang, H.; Wang, W.; Tan, W. Summary of the Detection Kits for SARS-CoV-2 Approved by the National Medical Products Administration of China and Their Application for Diagnosis of COVID-19. Virol. Sin. 2020, 35, 699–712. [Google Scholar] [CrossRef]
- Raciborski, F.; Pinkas, J.; Jankowski, M.; Sierpiński, R.; Zgliczyński, W.S.; Szumowski, Ł.; Rakocy, K.; Wierzba, W.; Gujski, M. Dynamics of the coronavirus disease 2019 outbreak in Poland: An epidemiological analysis of the first 2 months of the epidemic. Polish Arch. Intern. Med. 2020, 130, 615–621. [Google Scholar] [CrossRef]
- Fulawka, L.; Kuzan, A. COVID-19 Diagnostics Outside and Inside the National Health Service: A Single Institutional Experience. Diagnostics 2021, 11, 2044. [Google Scholar] [CrossRef]
- Javalkote, V.S.; Kancharla, N.; Bhadra, B.; Shukla, M.; Soni, B.; Sapre, A.; Goodin, M.; Bandyopadhyay, A.; Dasgupta, S. CRISPR-based assays for rapid detection of SARS-CoV-2. Methods 2020, 203, 594–603. [Google Scholar] [CrossRef]
- Duś-Ilnicka, I.; Szymczak, A.; Małodobra-Mazur, M.; Tokarski, M. Role of Laboratory Medicine in SARS-CoV-2 Diagnostics. Lessons Learned from a Pandemic. Healthcare 2021, 9, 915. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wang, Y.; Wang, B.; Lou, J.; Ni, P.; Jin, Y.; Chen, S.; Duan, G.; Zhang, R. Application of CRISPR/Cas Systems in the Nucleic Acid Detection of Infectious Diseases. Diagnostics 2022, 12, 2455. [Google Scholar] [CrossRef] [PubMed]
- Krüttgen, A.; Cornelissen, C.G.; Dreher, M.; Hornef, M.W.; Imöhl, M.; Kleines, M. Comparison of the SARS-CoV-2 Rapid antigen test to the real star SARS-CoV-2 RT PCR kit. J. Virol. Methods 2021, 288, 114024. [Google Scholar] [CrossRef] [PubMed]
- Wellinghausen, N.; Voss, M.; Ivanova, R.; Deininger, S. Evaluation of the SARS-CoV-2-IgG response in outpatients by five commercial immunoassays. GMS Infect. Dis. 2020, 8, Doc22. [Google Scholar] [CrossRef]
- Drain, P.K. Rapid Diagnostic Testing for SARS-CoV-2. N. Engl. J. Med. 2022, 386, 264–272. [Google Scholar] [CrossRef]
- Dao, T.L.; Hoang, V.T.; Gautret, P. Recurrence of SARS-CoV-2 viral RNA in recovered COVID-19 patients: A narrative review. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 13–25. [Google Scholar] [CrossRef]
- Healy, B.; Khan, A.; Metezai, H.; Blyth, I.; Asad, H. The impact of false positive COVID-19 results in an area of low prevalence. Clin. Med. 2021, 21, e54. [Google Scholar] [CrossRef]
- Islam, K.U.; Iqbal, J. An Update on Molecular Diagnostics for COVID-19. Front. Cell. Infect. Microbiol. 2020, 10, 560616. [Google Scholar] [CrossRef]
- Vindeirinho, J.M.; Pinho, E.; Azevedo, N.F.; Almeida, C. SARS-CoV-2 Diagnostics Based on Nucleic Acids Amplification: From Fundamental Concepts to Applications and Beyond. Front. Cell. Infect. Microbiol. 2022, 12, 799678. [Google Scholar] [CrossRef]
- Ishige, T.; Murata, S.; Taniguchi, T.; Miyabe, A.; Kitamura, K.; Kawasaki, K.; Nishimura, M.; Igari, H.; Matsushita, K. Highly sensitive detection of SARS-CoV-2 RNA by multiplex rRT-PCR for molecular diagnosis of COVID-19 by clinical laboratories. Clin. Chim. Acta 2020, 507, 139. [Google Scholar] [CrossRef]
- Singh, D.; Yi, S.V. On the origin and evolution of SARS-CoV-2. Exp. Mol. Med. 2021, 53, 537–547. [Google Scholar] [CrossRef] [PubMed]
- Araf, Y.; Akter, F.; Tang, Y.D.; Fatemi, R.; Parvez, M.S.A.; Zheng, C.; Hossain, M.G. Omicron variant of SARS-CoV-2: Genomics, transmissibility, and responses to current COVID-19 vaccines. J. Med. Virol. 2022, 94, 1825–1832. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Collier, A.-R.Y.; Rowe, M.; Mardas, F.; Ventura, J.D.; Wan, H.; Miller, J.; Powers, O.; Chung, B.; Siamatu, M.; et al. Neutralization of the SARS-CoV-2 Omicron BA.1 and BA.2 Variants. N. Engl. J. Med. 2022, 386, 1579–1580. [Google Scholar] [CrossRef] [PubMed]
- Metzger, C.M.J.A.; Lienhard, R.; Seth-Smith, H.M.B.; Roloff, T.; Wegner, F.; Sieber, J.; Bel, M.; Greub, G.; Egli, A. PCR performance in the SARS-CoV-2 Omicron variant of concern? Swiss Med. Wkly. 2021, 151, w30120. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.Y.; Jian, M.J.; Chang, C.K.; Lin, J.C.; Yeh, K.M.; Yang, Y.S.; Chen, C.W.; Hsieh, S.S.; Tang, S.H.; Perng, C.L.; et al. Multicenter study evaluating one multiplex RT-PCR assay to detect SARS-CoV-2, influenza A/B, and respiratory syncytia virus using the LabTurbo AIO open platform: Epidemiological features, automated sample-to-result, and high-throughput testing. Aging 2021, 13, 24931. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Preanalytical Phase | Analytical Phase | Post-Analytical Phase | Prevention | |
|---|---|---|---|---|
| False-negative results | -Incorrect sampling -Too long storage -Inappropriate storage conditions | -Incorrect extraction technique -Pipetting errors -Abnormal RT-PCR reaction conditions (temperature, reagent concentrations) -Using incorrectly stored reagents -Target mutation | -Misinterpretation -Incorrect determination of baseline and threshold | -Positive controls (viral RNA sequence) -Internal controls, e.g., endogenous (housekeeping genes) and exogenous (artificial construct) |
| False-positive results | -Sample contamination at the collection point | -RNA contamination during extraction -Use of contaminated reagents -Cross-reaction with other viruses (e.g., other coronaviruses) | -Misinterpretation -Incorrect determination of baseline and threshold | -Negative controls (with no template) -Test based on 2 or 3 viral genes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fulawka, L.; Kuzan, A. Molecular Diagnostic Tools against SARS-CoV-2 in Poland in 2022. Biomedicines 2022, 10, 3259. https://doi.org/10.3390/biomedicines10123259
Fulawka L, Kuzan A. Molecular Diagnostic Tools against SARS-CoV-2 in Poland in 2022. Biomedicines. 2022; 10(12):3259. https://doi.org/10.3390/biomedicines10123259
Chicago/Turabian StyleFulawka, Lukasz, and Aleksandra Kuzan. 2022. "Molecular Diagnostic Tools against SARS-CoV-2 in Poland in 2022" Biomedicines 10, no. 12: 3259. https://doi.org/10.3390/biomedicines10123259