
Relationship between Arterial Calcifications on Mammograms and Cardiovascular Events: A Twenty-Three Year Follow-Up Retrospective Cohort Study
 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Patient Selection
2.2. Data Collection
2.3. Statistical Analysis
2.4. Ethical Aspects
3. Results
3.1. Baseline Clinical Characteristics of the Patients and at the End of the Follow-Up Period
3.2. Development of Cardiovascular Events during the Follow-Up Period
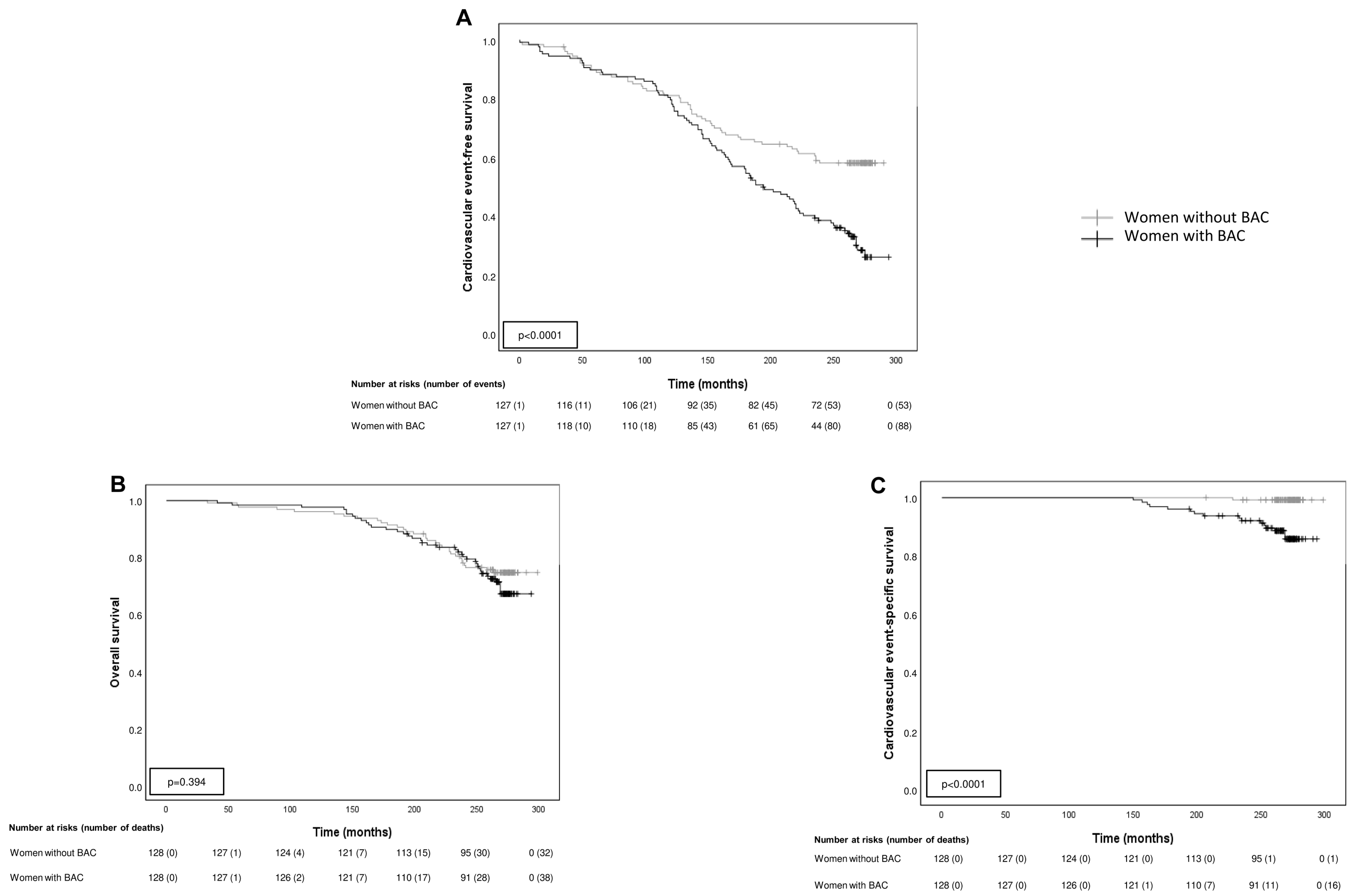
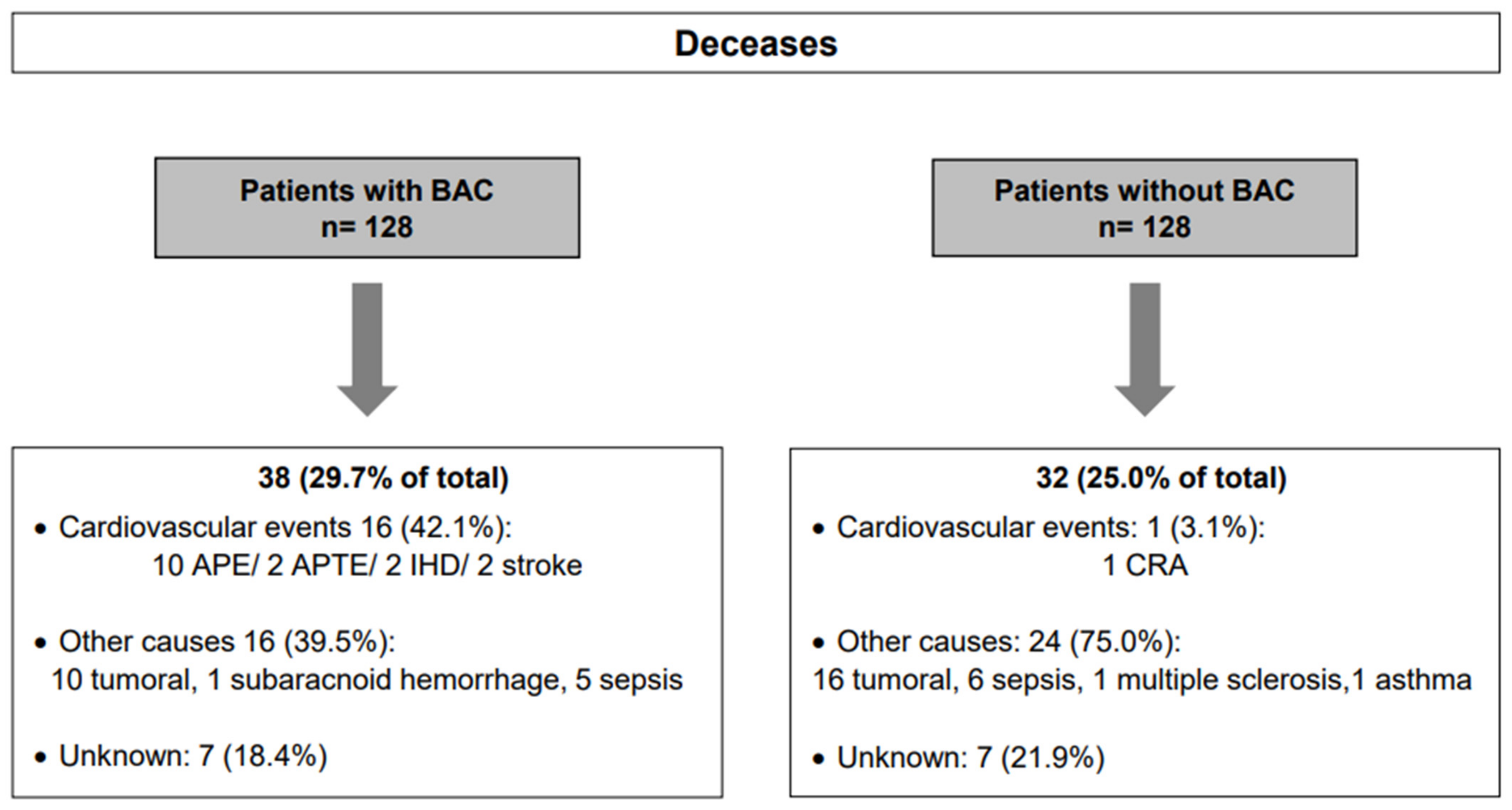
3.3. BAC Influence on Survival
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Kemmeren, J.M.; van Noord, P.A.; Beijerinck, D.; Fracheboud, J.; Banga, J.D.; van der Graaf, Y. Arterial calcification found on breast cancer screening mammograms and cardiovascular mortality in women: The DOM Project. Doorlopend Onderzoek Morbiditeit en Mortaliteit. Am. J. Epidemiol. 1998, 147, 333–341. [Google Scholar] [CrossRef] [Green Version]
- Wallin, R.; Wajih, N.; Greenwood, G.T.; Sane, D.C. Arterial calcification: A review of mechanisms, animal models, and the prospects for therapy. Med. Res. Rev. 2001, 21, 274–301. [Google Scholar] [CrossRef]
- Wang, Q.; Jin, L.; Wang, H.; Tai, S.; Liu, H.; Zhang, D. AWRK6, A Synthetic Cationic Peptide Derived from Antimicrobial Peptide Dybowskin-2CDYa, Inhibits Lipopolysaccharide-Induced Inflammatory Response. Int. J. Mol. Sci. 2018, 19, 600. [Google Scholar] [CrossRef] [Green Version]
- Abou-Hassan, N.; Tantisattamo, E.; D’Orsi, E.T.; O’Neill, W.C. The clinical significance of medial arterial calcification in end-stage renal disease in women. Kidney Int. 2015, 87, 195–199. [Google Scholar] [CrossRef]
- Ahn, K.J.; Kim, Y.J.; Cho, H.J.; Yim, H.W.; Kang, B.J.; Kim, S.H.; Kim, H.S.; Kim, K.T.; Lee, J.H.; Whang, I.Y. Correlation between breast arterial calcification detected on mammography and cerebral artery disease. Arch. Gynecol. Obstet. 2011, 284, 957–964. [Google Scholar] [CrossRef]
- Jiang, X.; Clark, M.; Singh, R.K.; Juhn, A.; Schnatz, P.F. Association of breast arterial calcification with stroke and angiographically proven coronary artery disease: A meta-analysis. Menopause 2015, 22, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Chadashvili, T.; Litmanovich, D.; Hall, F.; Slanetz, P.J. Do breast arterial calcifications on mammography predict elevated risk of coronary artery disease? Eur. J. Radiol. 2016, 85, 1121–1124. [Google Scholar] [CrossRef] [Green Version]
- Soylu, A.; Soylu, K.; Aydın, R.; Uzunkaya, F.; Aslan, K.; Polat, A.V. Calcification of breast artery as detected by mammography: Association with coronary and aortic calcification. Turk. J. Med. Sci. 2019, 49, 190–197. [Google Scholar] [CrossRef]
- McLenachan, S.; Camilleri, F.; Smith, M.; Newby, D.E.; Williams, M.C. Breast arterial calcification on mammography and risk of coronary artery disease: A SCOT-HEART sub-study. Clin. Radiol. 2019, 74, 421–428. [Google Scholar] [CrossRef] [Green Version]
- Fathala, A.L.; Alabdulkarim, F.M.; Shoukri, M.; Alanazi, M. Association between breast arterial calcifications found on mammography and coronary artery calcifications in asymptomatic Saudi women. Ann. Saudi. Med. 2018, 38, 433–438. [Google Scholar] [CrossRef] [PubMed]
- van Noord, P.A.; Beijerinck, D.; Kemmeren, J.M.; van der Graaf, Y. Mammograms may convey more than breast cancer risk: Breast arterial calcification and arterio-sclerotic related diseases in women of the DOM cohort. Eur. J. Cancer Prev. 1996, 5, 483–487. [Google Scholar] [PubMed]
- Kemmeren, J.M.; Beijerinck, D.; van Noord, P.A.; Banga, J.D.; Deurenberg, J.J.; Pameijer, F.A.; van der Graaf, Y. Breast arterial calcifications: Association with diabetes mellitus and cardiovascular mortality. Work in progress. Radiology 1996, 201, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Moshyedi, A.C.; Puthawala, A.H.; Kurland, R.J.; O’Leary, D.H. Breast arterial calcification: Association with coronary artery disease. Work in progress. Radiology 1995, 194, 181–183. [Google Scholar] [CrossRef]
- de Waard, F.; Collette, H.J.; Rombach, J.J.; Baanders-van Halewijn, E.A.; Honing, C. The DOM project for the early detection of breast cancer, Utrecht, The Netherlands. J. Chronic. Dis. 1984, 37, 1–44. [Google Scholar] [CrossRef]
- Gennarelli, M.; Jedynak, A.; Forman, L.; Wold, E.; Newman, R.B.; Dhand, A.; Kapoor, A.; Jafri, F.; Pal, S.; Pandav, J.; et al. The potential impact of mammographic breast arterial calcification on physician practices in a primary care setting. Future Cardiol. 2021, 17, 7. [Google Scholar] [CrossRef]
- Iribarren, C.; Chandra, M.; Lee, C.; Sanchez, G.; Sam, D.L.; Azamian, F.F.; Cho, H.M.; Ding, H.; Wong, N.D.; Molloi, S. Breast Arterial Calcification: A Novel Cardiovascular Risk Enhancer Among Postmenopausal Women. Circ. Cardiovasc. Imaging 2022, 15, e013526. [Google Scholar] [CrossRef]
- Pidal, D.; Sánchez Vidal, M.T.; Rodríguez, J.C.; Corte, M.D.; Pravia, P.; Guinea, O.; Pidal, I.; Bongera, M.; Escribano, D.; González, L.O.; et al. Relationship between arterial vascular calcifications seen on screening mammograms and biochemical markers of endothelial injury. Eur. J. Radiol. 2009, 69, 87–92. [Google Scholar] [CrossRef]
- Saá, J.; Fernández-Guinea, O.; García-Pravia, P.; Fernandez-Garcia, B.; Eiró, N.; del Casar, J.M.; Venta, R.; Baamonde, B.; Vizoso, F.J. Relationship between breast arterial calcifications seen on screening mammograms and age-related macular degeneration. Acta Ophthalmol. 2014, 92, e582–e584. [Google Scholar] [CrossRef] [Green Version]
- Brown, A.L.; Wahab, R.A.; Zhang, B.; Smetherman, D.H.; Mahoney, M.C. Reporting and Perceptions of Breast Arterial Calcification on Mammography: A Survey of ACR Radiologists. Acad Radiol 2022, 29 (Suppl. 1), S192–S198. [Google Scholar] [CrossRef]
- Chen, L.Y.; Sotoodehnia, N.; Buzkova, P.; Lopez, F.L.; Yee, L.M.; Heckbert, S.R.; Prineas, R.; Soliman, E.Z.; Adabag, S.; Konety, S.; et al. Atrial fibrillation and the risk of sudden cardiac death: The atherosclerosis risk in communities study and cardiovascular health study. JAMA Intern. Med. 2013, 173, 29–35. [Google Scholar] [CrossRef]
- Coronado, B.E.; Griffith, J.L.; Beshansky, J.R.; Selker, H.P. Hospital mortality in women and men with acute cardiac ischemia: A prospective multicenter study. J. Am. Coll. Cardiol. 1997, 29, 1490–1496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Margolies, L.; Salvatore, M.; Hecht, H.S.; Kotkin, S.; Yip, R.; Baber, U.; Bishay, V.; Narula, J.; Yankelevitz, D.; Henschke, C. Digital Mammography and Screening for Coronary Artery Disease. JACC Cardiovasc. Imaging 2016, 9, 350–360. [Google Scholar] [CrossRef] [PubMed]
- Ružičić, D.; Dobrić, M.; Vuković, M.; Hrnčić, D.; Đorđević, S.; Ružičić, M.; Aleksandrić, S.; Đorđević-Dikić, A.; Beleslin, B. The correlation of SYNTAX score by coronary angiography with breast arterial calcification by digital mammography. Clin. Radiol. 2018, 73, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Yoon, Y.E.; Kim, K.M.; Han, J.S.; Kang, S.H.; Chun, E.J.; Ahn, S.; Kim, S.M.; Choi, S.I.; Yun, B.; Suh, J.W. Prediction of Subclinical Coronary Artery Disease With Breast Arterial Calcification and Low Bone Mass in Asymptomatic Women: Registry for the Women Health Cohort for the BBC Study. JACC Cardiovasc. Imaging 2019, 12, 1202–1211. [Google Scholar] [CrossRef] [PubMed]
- Disthabanchong, S.; Boongird, S. Role of different imaging modalities of vascular calcification in predicting outcomes in chronic kidney disease. World J. Nephrol. 2017, 6, 100–110. [Google Scholar] [CrossRef] [PubMed]
- Gernaat, S.A.M.; van Velzen, S.G.M.; Koh, V.; Emaus, M.J.; Išgum, I.; Lessmann, N.; Moes, S.; Jacobson, A.; Tan, P.W.; Grobbee, D.E.; et al. Automatic quantification of calcifications in the coronary arteries and thoracic aorta on radiotherapy planning CT scans of Western and Asian breast cancer patients. Radiother. Oncol. 2018, 127, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Trimboli, R.M.; Codari, M.; Guazzi, M.; Sardanelli, F. Screening mammography beyond breast cancer: Breast arterial calcifications as a sex-specific biomarker of cardiovascular risk. Eur. J. Radiol. 2019, 119, 108636. [Google Scholar] [CrossRef] [PubMed]
- AlGhamdi, M.; Abdel-Mottaleb, M.; Collado-Mesa, F. DU-Net: Convolutional Network for the Detection of Arterial Calcifications in Mammograms. IEEE Trans. Med. Imaging 2020, 39, 3240–3249. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| At the Beginning | At the End of the Follow-Up Period | |||||
|---|---|---|---|---|---|---|
| Women with BAC (n = 128) | Women without BAC (n = 128) | p Value * | Women with BAC (n = 128) | Women without BAC (n = 128) | p Value * | |
| Hypertension | 38 (29.7%) | 31 (24.2%) | 0.398 | 101 (78.9%) | 86 (67.2%) | 0.049 |
| Diabetes mellitus | 9 (7%) | 4 (3.1%) | 0.255 | 36 (28.6%) | 35 (27.3%) | 0.938 |
| Dyslipidemia | 23 (18%) | 34 (26.6%) | 0.133 | 81 (63.3%) | 81 (63.3%) | 1.000 |
| Obesity | 35 (27.3%) | 22 (17.2%) | 0.071 | 47 (36.8%) | 46 (35.9%) | 1.000 |
| Tobacco | 3 (2.3%) | 7 (5.5%) | 0.333 | n.a | n.a | - |
| Women with BAC (n = 128) | Women without BAC (n = 128) | |||
|---|---|---|---|---|
| Cardiovascular Events | Nº (%) of Events (*) | RR (95% CI) | Nº (%) of Events (*) | RR (95% CI) |
| Ischemic heart disease | 26 (20.3) | 3.25 (1.53–6.90) | 8 (6.3) | 0.85 (0.77–0.94) |
| Hypertensive heart disease | 35 (27.3) | 2.85 (1.59–5.09) | 16 (12.5) | 0.79 (0.69–0.89) |
| Valvular heart disease | 37 (28.9) | 2.19 (1.28–3.75) | 13 (10.2) | 0.83 (0.73–0.94) |
| Congestive heart failure | 33 (25.8) | 2.06 (1.19–3.56) | 16 (12.5) | 0.85 (0.75–0.96) |
| Atrial fibrillation | 33 (25.8) | 1.83 (1.09–3.08) | 18 (14.1) | 0.86 (0.76–0.98) |
| Peripheral vascular disease | 28 (21.9) | 2.8 (1.42–5.52) | 10 (7.8) | 0.85 (0.76–0.94) |
| Ischemic stroke | 9 (7) | 1.5 (0.55–4.09) | 6 (4.7) | 0.98 (0.92–1.04) |
| Hemorrhagic stroke | 2 (1.6) | 1.0 (0.14–6.99) | 2 (1.6) | 1.0 (0.97–1.03) |
| Lacunar infarction | 29 (22.7) | 2.23 (1.21–4.09) | 13 (10.2) | 0.86 (0.77–0.96) |
| Total events | 232 | 1.66 (1.31–2.1) | 102 | 0.53 (0.39–0.72) |
| Cardiovascular Event-Free Survival | Cardiovascular Event-Specific Survival | ||||
|---|---|---|---|---|---|
| Risk Factors | Nº of Women | Event Frecuency | HR (95% CI) | Event Frecuency | HR (95% CI) |
| BAC/no BAC | 128/128 | 88/53 | 1.9 (1.3–2.7) *** | 16/1 | 14.1 (1.9–107.6) ** |
| Hypertension/no Hypertension | 69/187 | 38/103 | - | 11/6 | 6.6 (2.4–18.4) *** |
| DL/no DL | 57/199 | 30/111 | - | 2/15 | - |
| DM/no DM | 13/243 | 12/129 | 2.6 (1.4–4.8) ** | 3/14 | 4.9 (1.4–17.9) * |
| Obesity/no Obesity | 57/199 | 33/108 | - | 4/13 | - |
| Tobacco/no tobacco | 10/246 | 7/134 | - | 0/17 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galiano, N.G.; Eiro, N.; Martín, A.; Fernández-Guinea, O.; Martínez, C.d.B.; Vizoso, F.J. Relationship between Arterial Calcifications on Mammograms and Cardiovascular Events: A Twenty-Three Year Follow-Up Retrospective Cohort Study. Biomedicines 2022, 10, 3227. https://doi.org/10.3390/biomedicines10123227
Galiano NG, Eiro N, Martín A, Fernández-Guinea O, Martínez CdB, Vizoso FJ. Relationship between Arterial Calcifications on Mammograms and Cardiovascular Events: A Twenty-Three Year Follow-Up Retrospective Cohort Study. Biomedicines. 2022; 10(12):3227. https://doi.org/10.3390/biomedicines10123227
Chicago/Turabian StyleGaliano, Natalia González, Noemi Eiro, Arancha Martín, Oscar Fernández-Guinea, Covadonga del Blanco Martínez, and Francisco J. Vizoso. 2022. "Relationship between Arterial Calcifications on Mammograms and Cardiovascular Events: A Twenty-Three Year Follow-Up Retrospective Cohort Study" Biomedicines 10, no. 12: 3227. https://doi.org/10.3390/biomedicines10123227