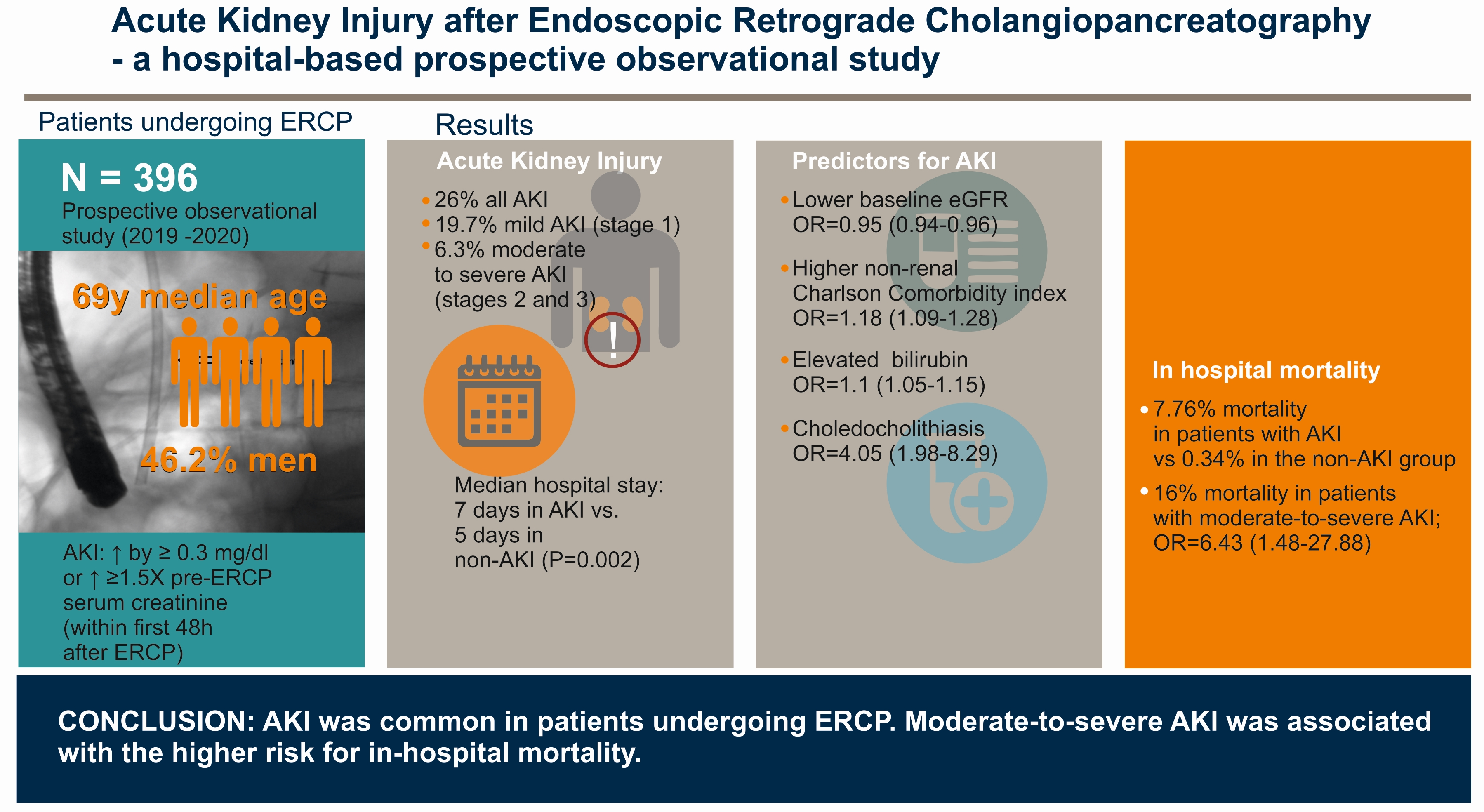
Acute Kidney Injury after Endoscopic Retrograde Cholangiopancreatography—A Hospital-Based Prospective Observational Study

 , ,
, ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Variables
2.3. Estimation of Renal Function and Definition of AKI
2.4. Endoscopic Retrograde Cholangiopancreatography
2.5. Outcomes
2.6. Statistical Analysis
3. Results
3.1. Incidence and Risk Factors of AKI
3.2. Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rustagi, T.; Jamidar, P.A. Endoscopic Retrograde Cholangiopancreatography–Related Adverse Events: General overview. Gastrointest. Endosc. Clin. N. Am. 2015, 25, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Forbes, N.; Leontiadis, G.I.; Vaska, M.; Elmunzer, B.J.; Yuan, Y.; Bishay, K.; Meng, Z.W.; Iannuzzi, J.; O’Sullivan, D.E.; Mah, B.; et al. Adverse events associated with endoscopic retrograde cholangiopancreatography: Protocol for a systematic review and meta-analysis. BMJ Open 2021, 11, e053302. [Google Scholar] [CrossRef] [PubMed]
- Moffatt, D.C.; Yu, B.N.; Yie, W.; Bernstein, C.N. Trends in utilization of diagnostic and therapeutic ERCP and cholecystectomy over the past 25 years: A population-based study. Gastrointest. Endosc. 2013, 79, 615–622. [Google Scholar] [CrossRef]
- Ivanovic, L.F.; Silva, B.C.; Lichtenstein, A.; de Paiva, E.F.; Bueno-Garcia, M.L. Kidney injury and other complications related to colonoscopy in inpatients at a tertiary teaching hospital. Clinics 2018, 73, e456. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Bin Im, C.; Lee, S.S.; Jeon, H.; Choi, J.W.; Kim, H.J.; Cha, R.R.; Cho, H.C.; Lee, J.M.; Ha, C.Y.; et al. Impact of acute kidney injury on mortality in patients with acute variceal bleeding. BMC Gastroenterol. 2021, 21, 290. [Google Scholar] [CrossRef] [PubMed]
- Cakmak, U.; Merhametsiz, O.; Oguz, E.G.; Ercan, Z.; Haspulat, A.; Ozkan, S.K.; Canbakan, B.; Aylı, M.D. Effects of acute kidney injury on clinical outcomes in patients with upper gastrointestinal bleeding. Ren. Fail. 2015, 38, 176–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kabaria, S.; Tawadros, A.; Rotundo, L.; Patel, G.; Patel, P.; Sushil, A. Impact of Acute Kidney Injury in Hospitalizations with Non-Variceal Upper Gastrointestinal Bleeding. J. Gastroenterol. Res. 2021, 5, 170–180. [Google Scholar] [CrossRef]
- Gordon, V.; Chowdhury, A.; Keim, S. Etiology and Comorbidity Diagnoses Effect on Outcomes for Patients Undergoing Endoscopic Retrograde Cholangiopancreatography. Cureus 2020, 12, e10209. [Google Scholar] [CrossRef]
- Sawas, T.; Bazerbachi, F.; Haffar, S.; Cho, W.K.; Levy, M.J.; Martin, J.A.; Petersen, B.T.; Topazian, M.D.; Chandrasekhara, V.; Abu Dayyeh, B.K. End-stage renal disease is associated with increased post endoscopic retrograde cholangiopancreatography adverse events in hospitalized patients. World J. Gastroenterol. 2018, 24, 4691–4697. [Google Scholar] [CrossRef]
- Park, J.-S.; Jeong, S.; Cho, J.H.; Kwon, C.-I.; Jang, S.I.; Lee, T.H.; Han, J.-H.; Hwang, J.C.; Lee, D.H. Clinical outcome of endoscopic retrograde cholangiopancreatography for choledocholithiasis in end-stage renal disease patients on hemodialysis. Turk. J. Gastroenterol. 2020, 31, 538–546. [Google Scholar] [CrossRef]
- Tsujung, Y.; Shriya, G.; Ntasha, R.; Muhammad, S.; Salma, H.; Lutfor, N.; Subash, G.; Ruchir, G.; Hardikkumar, S.; Achint, P.; et al. Temporal Trend and Predictors of Acute Kidney Injury in Patients Undergoing Endoscopic Retrograde Cholangiopancreatography. Am. J. Gastroenterol. 2021, 116, S466. [Google Scholar] [CrossRef]
- Shinoura, S.; Tokushige, A.; Chinen, K.; Mori, H.; Kato, S.; Ueda, S. Association between contrast-induced nephrotoxicity and contrast enhanced computed tomography followed by endoscopic retrograde cholangiopancreatography. Eur. J. Radiol. 2020, 129, 109074. [Google Scholar] [CrossRef] [PubMed]
- Seibert, D.G.; Al-Kawas, F.H.; Graves, J.; Gaskins, R.D. Prospective Evaluation of Renal Function Following ERCP. Endoscopy 1991, 23, 355–356. [Google Scholar] [CrossRef]
- Lutfor, N.; Shriya, G.; Salma, H.; Ntasha, R.; Muhammad, S.; Ruchir, G.; Subash, G.; Tsujung, Y.; Hardikkumar, S.; Achint, P.; et al. Impact of Acute Kidney Injury on In-Hospital Outcomes of Endoscopic Retrograde Cholangiopancreatography. Am. J. Gastroenterol. 2021, 116, S1388. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Chakraborty, R.K.; Burns, B. Systemic Inflammatory Response Syndrome. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Kiriyama, S.; Kozaka, K.; Takada, T.; Strasberg, S.M.; Pitt, H.A.; Gabata, T.; Hata, J.; Liau, K.-H.; Miura, F.; Horiguchi, A.; et al. Tokyo Guidelines 2018: Diagnostic criteria and severity grading of acute cholangitis (with videos). J. Hepato-Biliary-Pancreat. Sci. 2018, 25, 17–30. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Kidney Disease; Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int. Suppl. 2012, 2, S1–S138. [Google Scholar]
- Susantitaphong, P.; Cruz, D.N.; Cerda, J.; Abulfaraj, M.; Alqahtani, F.; Koulouridis, I.; Jaber, B.L.; Acute Kidney Injury Advisory Group of the American Society of Nephrology. World Incidence of AKI: A Meta-Analysis. Clin. J. Am. Soc. Nephrol. 2013, 8, 1482–1493. [Google Scholar] [CrossRef] [Green Version]
- Kellum, J.A.; Romagnani, P.; Ashuntantang, G.; Ronco, C.; Zarbock, A.; Anders, H.-J. Acute kidney injury. Nat. Rev. Dis. Prim. 2021, 7, 52. [Google Scholar] [CrossRef] [PubMed]
- Hurst, F.P.; Bohen, E.M.; Osgard, E.M.; Oliver, D.K.; Das, N.P.; Gao, S.W.; Abbott, K. Association of Oral Sodium Phosphate Purgative Use with Acute Kidney Injury. J. Am. Soc. Nephrol. 2007, 18, 3192–3198. [Google Scholar] [CrossRef] [PubMed]
- Tryliskyy, Y.; Bryce, G.J. Post-ERCP pancreatitis: Pathophysiology, early identification and risk stratification. Adv. Clin. Exp. Med. 2018, 27, 149–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adas, G.; Kemik, A.; Adas, M.; Koc, B.; Gurbuz, E.; Akcakaya, A.; Karahan, S. Metabolic and inflammatory responses after ERCP. Int. J. Biomed. Sci. 2013, 9, 237–242. [Google Scholar]
- Mulay, S.R.; Linkermann, A.; Anders, H.-J. Necroinflammation in Kidney Disease. J. Am. Soc. Nephrol. 2015, 27, 27–39. [Google Scholar] [CrossRef] [Green Version]
- Bell, S.; James, M.T.; Farmer, C.K.T.; Tan, Z.; De Souza, N.; Witham, M.D. Development and external validation of an acute kidney injury risk score for use in the general population. Clin. Kidney J. 2020, 13, 402–412. [Google Scholar] [CrossRef]
- James, M.T.; Grams, M.E.; Woodward, M.; Elley, C.R.; Green, J.A.; Wheeler, D.C.; de Jong, P.; Gansevoort, R.T.; Levey, A.S.; Warnock, D.G.; et al. A Meta-analysis of the Association of Estimated GFR, Albuminuria, Diabetes Mellitus, and Hypertension With Acute Kidney Injury. Am. J. Kidney Dis. 2015, 66, 602–612. [Google Scholar] [CrossRef] [Green Version]
- Charlson, M.E.; Carrozzino, D.; Guidi, J.; Patierno, C. Charlson Comorbidity Index: A Critical Review of Clinimetric Properties. Psychother. Psychosom. 2022, 91, 8–35. [Google Scholar] [CrossRef]
- Talib, S.; Sharif, F.; Manzoor, S.; Yaqub, S.; Kashif, W. Charlson Comorbidity Index for Prediction of Outcome of Acute Kidney Injury in Critically Ill Patients. Iran J. Kidney Dis. 2017, 11, 115–123. [Google Scholar]
- Wu, Y.H.; Wu, C.Y.; Cheng, C.Y.; Tsai, S.F. Severe hyperbilirubinemia is associated with higher risk of contrast-related acute kidney injury following contrast-enhanced computed tomography. PLoS ONE 2020, 15, e0231264. [Google Scholar] [CrossRef] [Green Version]
- Somagutta, M.R.; Jain, M.S.; Pormento, M.K.L.; Pendyala, S.K.; Bathula, N.R.; Jarapala, N.; Mahadevaiah, A.; Sasidharan, N.; Gad, M.A.; Mahmutaj, G.; et al. Bile Cast Nephropathy: A Comprehensive Review. Cureus 2022, 14, e23606. [Google Scholar] [CrossRef]
- Fairfield, C.J.; Wigmore, S.J.; Harrison, E.M. Gallstone Disease and the Risk of Cardiovascular Disease. Sci. Rep. 2019, 9, 5830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuznetsova, T.; Cauwenberghs, N.; Knez, J.; Thijs, L.; Liu, Y.-P.; Gu, Y.-M.; Staessen, J.A. Doppler Indexes of Left Ventricular Systolic and Diastolic Flow and Central Pulse Pressure in Relation to Renal Resistive Index. Am. J. Hypertens. 2014, 28, 535–545. [Google Scholar] [CrossRef]
- Kandathil, A.; Abbara, S.; Hanna, M.; Minhajuddin, A.; Wehrmann, L.; Merchant, A.M.; Mills, R.; Fox, A.A. Atherosclerosis on CT Angiogram Predicts Acute Kidney Injury After Transcatheter Aortic Valve Replacement. Am. J. Roentgenol. 2018, 211, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Khadzhynov, D.; Schmidt, D.; Hardt, J.; Rauch, G.; Gocke, P.; Eckardt, K.-U.; Schmidt-Ott, K.M. The Incidence of Acute Kidney Injury and Associated Hospital Mortality. Dtsch. Arztebl. Int. 2019, 116, 397–404. [Google Scholar] [CrossRef]
- Chertow, G.M.; Burdick, E.; Honour, M.; Bonventre, J.V.; Bates, D.W. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J. Am. Soc. Nephrol. 2005, 16, 3365–3370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ostermann, M.; Chang, R. The Riyadh ICU Program Users Group Correlation between the AKI classification and outcome. Crit. Care 2008, 12, R144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Girling, B.J.; Channon, S.W.; Haines, R.W.; Prowle, J.R. Acute kidney injury and adverse outcomes of critical illness: Correlation or causation? Clin. Kidney J. 2019, 13, 133–141. [Google Scholar] [CrossRef] [Green Version]
- Grams, M.E.; Rabb, H. The distant organ effects of acute kidney injury. Kidney Int. 2012, 81, 942–948. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.A.; Cozzi, M.; Bush, E.L.; Rabb, H. Distant Organ Dysfunction in Acute Kidney Injury: A Review. Am. J. Kidney Dis. 2018, 72, 846–856. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Parameter | Total ERCP Group (n = 396) | AKI Group (n = 103) | Non-AKI Group (n = 293) | p | |
|---|---|---|---|---|---|
| Age, (years) a | 69 {17} | 70.83 ± 12.26 | 68 {18} | 0.004 | |
| Male gender, n (%) c | 183 (46.21) | 53 (51.45) | 130 (44.36) | 0.251 | |
| Clinical and laboratory data on admission | |||||
| SIRS, n (%) c | 88 (22.22) | 32 (31.06) | 56 (19.11) | 0.018 | |
| CCI a | 5 {4} | 6 {4} | 5 {4} | <0.001 | |
| Nonrenal CCI a | 5 {4} | 6 {4} | 5 {4} | 0.001 | |
| White blood cell counts (×103/µL) a | 8.15 {4.2} | 9.1 {5} | 7.9 {3.9} | 0.001 | |
| Neutrophil counts (×103/µL) a | 6.2 {4.4} | 7.4 {5.2} | 5.9 {4} | 0.0004 | |
| Haematocrit (%) b | 36.71 ± 5.74 | 35.51 ± 6.11 | 37.14 ± 5.55 | 0.013 | |
| Platelet count (×103/µL) a | 232 {114} | 221.02 ± 110.63 | 250.23 ± 92.16 | 0.002 | |
| INR | 1.12 {0.26} | 1.17 {0.29} | 1.12 {0.17} | 0.208 | |
| Glycaemia (mg/dL) a | 104 {44} | 113 {66} | 102 {37} | 0.019 | |
| Serum creatinine (mg/dL) a | 0.87 {0.39} | 1.22 {0.89} | 0.8 {0.26} | <0.001 | |
| eGFR (mL/min/1.73 m2) a | 79.72 {37.11} | 52.75 ± 26.04 | 85.84 ± 27.93 | <0.001 | |
| Serum lipase (U/L) a | 144.5 {209} | 135 {242} | 145 {188} | 0.291 | |
| Bilirubin (mg/dL) a | 4.2 {8.1} | 7.1 {11.4} | 3.7 {7} | <0.001 | |
| AST (U/L) a | 86 {130} | 88 {94} | 86 {147} | 0.538 | |
| ALT (U/L) a | 116.5 {175} | 101 {100} | 132 {216} | 0.044 | |
| ALP (U/L) a | 285 {343} | 397 {482} | 243 {279} | <0.001 | |
| Gamma-GT (U/L) a | 467 {599} | 482 {751} | 460 {558} | 0.386 | |
| Albumin (g/dL) b | 3.03 ± 0.73 | 2.73 ± 0.71 | 3.13 ± 0.70 | <0.001 | |
| C-reactive protein (mg/dL) a | 23.05 {79.4} | 48.9 {120} | 17.23 {67.8} | <0.001 | |
| Sepsis, n (%) c | 36 (9.1) | 21 (20.4) | 15 (5.12) | <0.001 | |
| Acute cholangitis, n (%) c | 223 (56.31) | 82 (79.61) | 141 (48.12) | <0.001 | |
| Indications of ERCP | |||||
| Choledocholithiasis, n (%) c | 240 (60.6) | 72 (69.9) | 168 (57.33) | 0.026 * | |
| Malignant biliary obstruction, n (%) c | 84 (21.21) | 21 (20.38) | 63 (21.50) | 0.889 | |
| Biliary/pancreatic duct stricture, n (%) c | 72 (18.18) | 10 (9.7) | 62 (21.16) | 0.001 * | |
| Types of ERCP-procedures | |||||
| Biliary/pancreatic drainage, n (%) c | 240 (60.6) | 72 (69.9) | 168 (57.33) | 0.026 * | |
| Sphincterotomy, n (%) c | 84 (21.21) | 21 (20.38) | 63 (21.50) | 0.889 | |
| Biopsy, n (%) c | 72 (18.18) | 10 (9.7) | 62 (21.16) | 0.001 * | |
| ERCP duration (minutes) | 34.9 ± 9.7 | 33.5 ± 7.3 | 35.3 ± 10.4 | 0.189 | |
| Predictor | Unadjusted OR (95% CI) | p | Adjusted OR (95% CI) | p |
|---|---|---|---|---|
| Age (per one year) | 1.03 (1.01–1.05) | 0.004 | 1.07 (1.02–1.12) | 0.001 |
| Choledocholithiasis | 1.73 (1.07–2.79) | 0.026 | 3.31 (1.29–8.54) | <0.001 |
| Biliary/pancreatic duct stricture | 0.40 (0.19–0.81) | 0.012 | - | |
| eGFR (per one mL/min/1.73 m2) | 0.95 (0.94–0.96) | <0.001 | 0.91 (0.89–0.97) | <0.001 |
| Acute cholangitis | 2.08 (1.39–3.11) | <0.001 | - | - |
| Sepsis | 4.74 (2.34–9.62) | <0.001 | - | - |
| C-reactive protein (per one mg/L) | 1.01 (1.00–1.01) | <0.001 | - | - |
| Albumin (per one g/dL) | 0.45 (0.33–0.63) | <0.001 | - | - |
| Nonrenal CCI (per one point) | 1.18 (1.09–1.28) | <0.001 | 1.21 (1.02–1.44) | 0.034 |
| Systemic inflammatory response syndrome | 1.89 (1.14–3.16) | 0.013 | - | |
| White blood cell count (per unit) | 1.07 (1.02–1.12) | 0.003 | Not used | |
| Neutrophil counts (per unit) | 1.08 (1.03–1.13) | 0.001 | Not used | |
| Haematocrit (per unit) | 0.95 (0.91–0.99) | 0.014 | - | |
| Platelet count (per unit) | 0.99 (0.99–1.00) | 0.010 | 1 (1.00–1.01) | 0.004 |
| Glycaemia (per one mg/dL) | 1.01 (1.00–1.01) | 0.012 | 1.01 (1.00–1.03) | 0.021 |
| Bilirubin (per one mg/dL) | 1.06 (1.04–1.09) | <0.001 | 1.12 (1.06–1.18) | <0.001 |
| ALT (per one U/L) | 0.99 (0.99–1.00) | 0.006 | 0.97 (0.94–1.00) | 0.003 |
| ALP (per one U/L) | 1.00 (1.01–1.02) | 0.001 | 1.01 (1.00–1.04) | 0.002 |
| Parameter | Total ERCP Group (n = 396) | AKI Group (n = 103) | Non-AKI Group (n = 293) | p | |
|---|---|---|---|---|---|
| Death, n (%) b | 9 (2.27) | 8 (7.76) | 1 (0.34) | <0.001 | |
| Cause of death, n (%) | Infection, n (%) b | 3 (0.75) | 2 (1.94) | 1 (0.34) | 0.167 |
| Malignancy progression, n (%) b | 3 (0.75) | 3 (2.91) | 0 (0) | 0.017 | |
| Heart failure, n (%) b | 2 (0.5) | 2 (1.94) | 0 (0) | 0.067 | |
| Cardiac arrest of unknown aetiology, n (%) b | 1 (0.25) | 1 (0.97) | 0 (0) | 0.260 | |
| Length of hospital stay, (days) a | 5 {5} | 7 {6} | 5 {5} | 0.002 | |
| Types of complications | |||||
| Pancreatitis, n (%) b | 14 (3.53) | 5 (4.85) | 9 (3.07) | 0.369 | |
| Bleeding, n (%) b | 2 (0.5) | 1 (0.97) | 1 (0.34) | 0.453 | |
| Perforation, n (%) b | 2 (0.5) | 1 (0.97) | 1 (0.34) | 0.453 | |
| Predictor | Unadjusted OR (95% CI) | p | Adjusted OR (95% CI) | p |
|---|---|---|---|---|
| AKI stage 2 and 3 | 13.94 (3.48–55.77) | <0.001 | 6.43 (1.48–27.88) | 0.013 |
| eGFR (per one mL/min/1.73 m2) | 0.97 (0.95–0.99) | 0.022 | 0.98 (0.95–1.02) | 0.077 |
| Albumin (per one g/dL) | 0.19 (0.07–0.49) | 0.001 | 0.18 (0.08–0.39) | <0.001 |
| Nonrenal CCI (per one point) | 1.42 (1.15–1.76) | 0.001 | 1.25 (1.03–1.52) | 0.025 |
| Systemic inflammatory response syndrome | 4.56 (1.20–17.37) | 0.026 | - | |
| White blood cell counts (per unit) | 1.16 (1.07–1.26) | <0.001 | Not used | |
| Neutrophil counts (per unit) | 1.16 (1.06–1.27) | <0.001 | Not used | |
| Bilirubin (per one mg/dL) | 1.07 (1.01–1.14) | 0.015 | - | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gadalean, F.; Parv, F.; Milas, O.; Petrica, L.; Ratiu, I.; Miutescu, B.; Goldis, A.; Gluhovschi, C.; Bob, F.; Simulescu, A.; et al. Acute Kidney Injury after Endoscopic Retrograde Cholangiopancreatography—A Hospital-Based Prospective Observational Study. Biomedicines 2022, 10, 3166. https://doi.org/10.3390/biomedicines10123166
Gadalean F, Parv F, Milas O, Petrica L, Ratiu I, Miutescu B, Goldis A, Gluhovschi C, Bob F, Simulescu A, et al. Acute Kidney Injury after Endoscopic Retrograde Cholangiopancreatography—A Hospital-Based Prospective Observational Study. Biomedicines. 2022; 10(12):3166. https://doi.org/10.3390/biomedicines10123166
Chicago/Turabian StyleGadalean, Florica, Florina Parv, Oana Milas, Ligia Petrica, Iulia Ratiu, Bogdan Miutescu, Adrian Goldis, Cristina Gluhovschi, Flaviu Bob, Anca Simulescu, and et al. 2022. "Acute Kidney Injury after Endoscopic Retrograde Cholangiopancreatography—A Hospital-Based Prospective Observational Study" Biomedicines 10, no. 12: 3166. https://doi.org/10.3390/biomedicines10123166