
Evaluation of the Role of Faecal Calprotectin in the Management of Psoriatic Patients under Treatment with Biologic Drugs

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Faecal Calprotectin
2.2. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of Patients
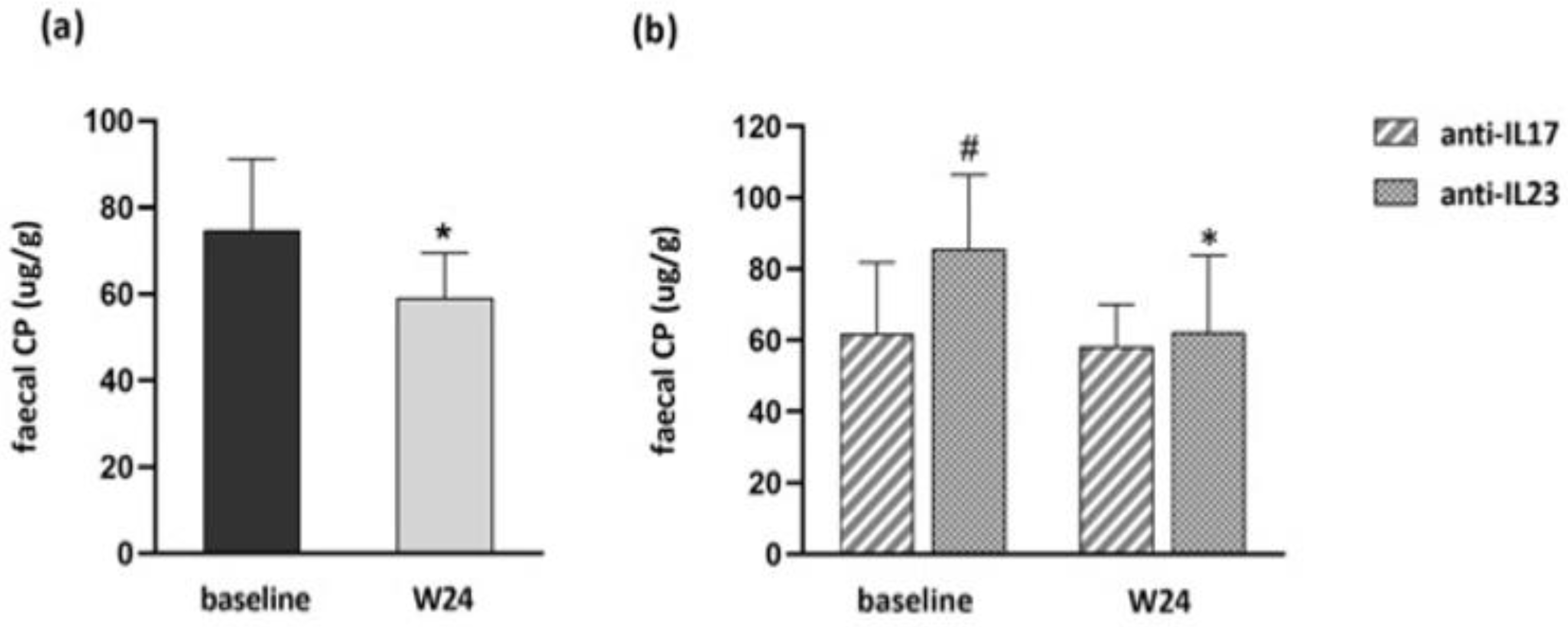
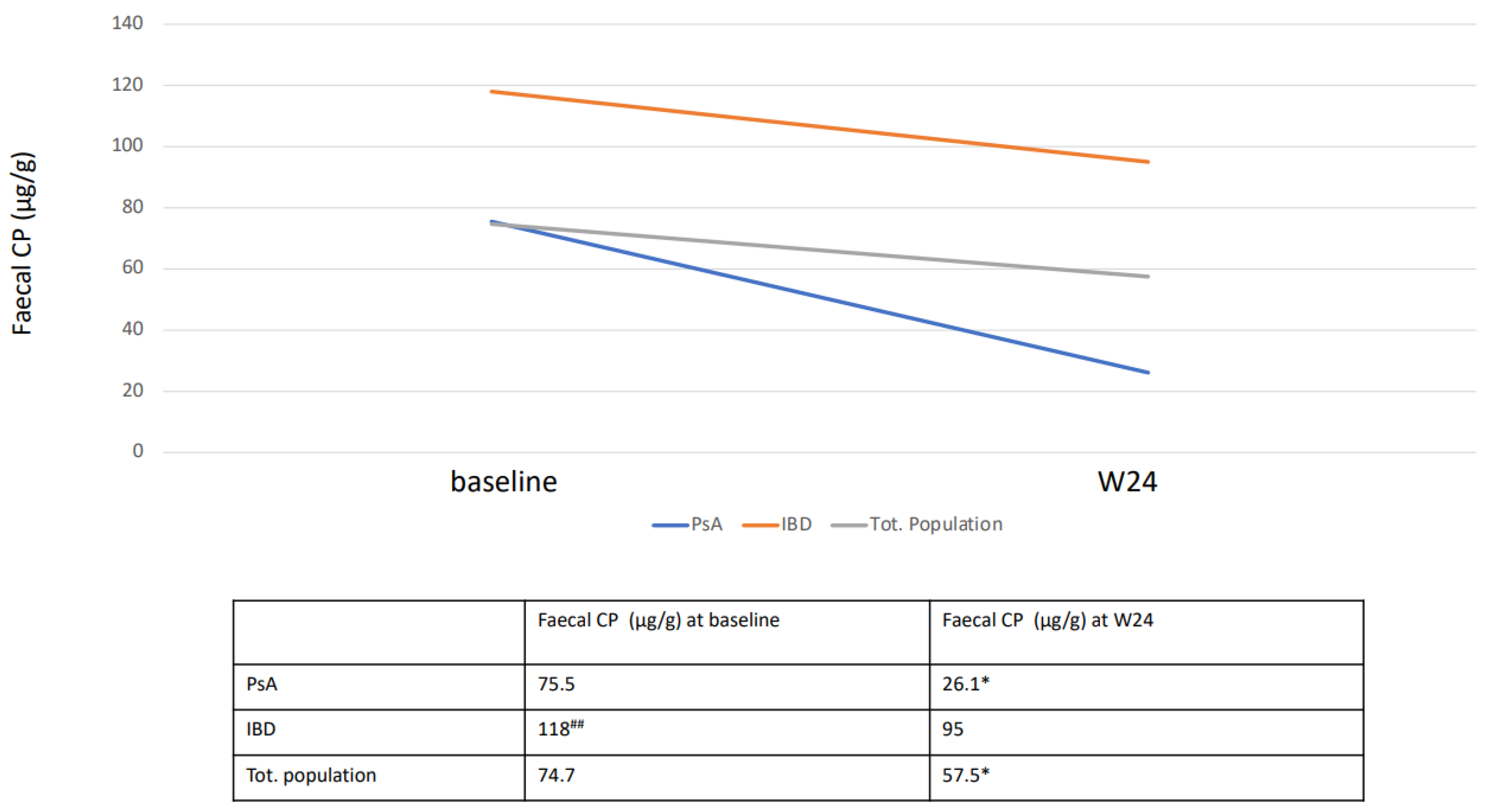
3.2. Faecal CP Level Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schön, M.P.; Boehncke, W.H. Psoriasis. N. Engl. J. Med. 2005, 352, 1899–1912. [Google Scholar] [CrossRef] [PubMed]
- Parisi, R.; Symmons, D.P.; Griffiths, C.E.; Ashcroft, D.M. Identification and Management of Psoriasis and Associated ComorbidiTy (IMPACT) project team. Global epidemiology of psoriasis: A systematic review of incidence and prevalence. J. Investig. Dermatol. 2013, 133, 377–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griffiths, C.E.; Barker, J.N. Pathogenesis and clinical features of psoriasis. Lancet 2007, 370, 263–271. [Google Scholar] [CrossRef]
- Ni, C.; Chiu, M.W. Psoriasis and comorbidities: Links and risks. Clin. Cosmet. Investig. Dermatol. 2014, 7, 119–132. [Google Scholar]
- Visconti, M.J.; Bashyam, A.M.; Feldman, S.R. Treatment decisions in psoriasis. J. Comp. Eff. Res. 2019, 8, 947–949. [Google Scholar] [CrossRef] [Green Version]
- Ahmad Fadzil, M.H.; Ihtatho, D.; Mohd Affandi, A.; Hussein, S.H. Objective assessment of psoriasis erythema for PASI scoring. J. Med. Eng. Technol. 2009, 33, 516–524. [Google Scholar] [CrossRef]
- Mahil, S.K.; Capon, F.; Barker, J.N. Update on psoriasis immunopathogenesis and targeted immunotherapy. Semin. Immunopathol. 2016, 38, 11–27. [Google Scholar] [CrossRef] [Green Version]
- Cohen, A.D.; Dreiher, J.; Birkenfeld, S. Psoriasis associated with ulcerative colitis and Crohn’s disease. J. Eur. Acad. Dermatol. Venereol. 2009, 23, 561–565. [Google Scholar] [CrossRef]
- Li, W.Q.; Han, J.L.; Chan, A.T.; Qureshi, A.A. Psoriasis, psoriatic arthritis and increased risk of incident Crohn’s disease in U.S. women. Ann. Rheum. Dis. 2013, 72, 1200–1205. [Google Scholar] [CrossRef] [Green Version]
- Alinaghi, F.; Tekin, H.G.; Burisch, J.; Wu, J.J.; Thyssen, J.P.; Egeberg, A. Global prevalence and bidirectional association between psoriasis and inflammatory bowel disease-a systematic review and meta-analysis. J. Crohns. Colitis 2020, 14, 351–360. [Google Scholar] [CrossRef]
- Swindell, W.R.; Johnston, A.; Xing, X.; Voorhees, J.J.; Elder, J.T.; Gudjonsson, J.E. Modulation of epidermal transcription circuits in psoriasis: New links between inflammation and hyperproliferation. PLoS ONE 2013, 8, e79253. [Google Scholar] [CrossRef] [PubMed]
- Korman, N.J. Management of psoriasis as a systemic disease: What is the evidence? Br. J. Dermatol. 2020, 182, 840–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghoreschi, K.; Balato, A.; Enerbäck, C.; Sabat, R. Therapeutics targeting the IL-23 and IL-17 pathway in psoriasis. Lancet 2021, 397, 754–766. [Google Scholar] [CrossRef]
- Chiricozzi, A.; Romanelli, P.; Volpe, E.; Borsellino, G.; Romanelli, M. Scanning the immunopathogenesis of psoriasis. Int. J. Mol. Sci. 2018, 19, 179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harden, J.L.; Johnson-Huang, L.M.; Chamian, M.F.; Lee, E.; Pearce, T.; Leonardi, C.L.; Haider, A.; Lowes, M.A.; Krueger, J.G. Humanized anti-IFN-gamma (HuZAF) in the treatment of psoriasis. J. Allergy Clin. Immunol. 2015, 135, 553–556. [Google Scholar] [CrossRef] [PubMed]
- Balato, A.; Scala, E.; Balato, N.; Caiazzo, G.; Di Caprio, R.; Monfrecola, G.; Raimondo, A.; Lembo, S.; Ayala, F. Biologics that inhibit the Th17 pathway and related cytokines to treat inflammatory disorders. Expert Opin. Biol. Ther. 2017, 17, 1363–1374. [Google Scholar] [CrossRef]
- Zhang, X.; Mosser, D. Macrophage activation by endogenous danger signals. J. Pathol. 2008, 214, 161–178. [Google Scholar] [CrossRef]
- Scher, J.U.; Ubeda, C.; Artacho, A.; Attur, M.; Isaac, S.; Reddy, S.M.; Marmon, S.; Neimann, A.; Brusca, S.; Patel, T.; et al. Decreased bacterial diversity characterizes the altered gut microbiota in patients with psoriatic arthritis, resembling dysbiosis in inflammatory bowel disease. Arthritis Rheumatol. 2015, 67, 128–139. [Google Scholar] [CrossRef] [Green Version]
- Asmar, R.E.; Panigrahi, P.; Bamford, P.; Berti, I.; Not, T.; Coppa, G.V.; Catassi, C.; Fasano, A. Host-dependent zonulin secretion causes the impairment of the small intestine barrier function after bacterial exposure. Gastroenterology 2002, 123, 1607–1615. [Google Scholar] [CrossRef]
- Oppenheim, J.J.; Yang, D. Alarmins: Chemotactic activators of immune responses. Curr. Opin. Immunol. 2005, 17, 359–365. [Google Scholar] [CrossRef]
- Caiazzo, G.; Fabbrocini, G.; Di Caprio, R.; Raimondo, A.; Scala, E.; Balato, N.; Balato, A. Psoriasis, cardiovascular events, and biologics: Lights and shadows. Front. Immunol. 2018, 9, 1668. [Google Scholar] [CrossRef] [PubMed]
- Edgeworth, J.; Gorman, M.; Bennett, R.; Freemont, P.; Hogg, N. Identification of p8,14 as a highly abundant heterodimeric calcium binding protein complex of myeloid cells. J. Biol. Chem. 1991, 266, 7706–7713. [Google Scholar] [CrossRef]
- Shabani, F.; Farasat, A.; Mahdavi, M.; Gheibi, N. Calprotectin (S100A8/S100A9): A key protein between inflammation and cancer. Inflamm. Res. 2018, 67, 801–812. [Google Scholar] [CrossRef] [PubMed]
- Jukic, A.; Bakiri, L.; Wagner, E.F.; Tilg, H.; Adolph, T.E. Calprotectin: From biomarker to biological function. Gut 2021, 70, 1978–1988. [Google Scholar] [CrossRef]
- Wang, S.; Song, R.; Wang, Z.; Jing, Z.; Wang, S.; Ma, J. S100A8/A9 in Inflammation. Front. Immunol. 2018, 9, 1298. [Google Scholar] [CrossRef] [Green Version]
- Ayling, R.M.; Kok, K. Fecal Calprotectin. Adv. Clin. Chem. 2018, 87, 161–190. [Google Scholar]
- Pruenster, M.; Vogl, T.; Roth, J.; Sperandio, M. S100A8/A9: From basic science to clinical application. Pharmacol. Ther. 2016, 167, 120–131. [Google Scholar] [CrossRef]
- Holzinger, D.; Tenbrock, K.; Roth, J. Alarmins of the S100-family in Juvenile autoimmune and auto-inflammatory diseases. Front. Immunol. 2019, 10, 182. [Google Scholar] [CrossRef]
- Vaos, G.; Kostakis, I.D.; Zavras, N. Chatzemichael A. The role of calprotectin in pediatric disease. Biomed. Res. Int. 2013, 2013, 542363. [Google Scholar] [CrossRef] [Green Version]
- Kang, K.Y.; Park, S.H.; Hong, Y.S. Relationship between faecal calprotectin and inflammation in peripheral joints and entheses in axial spondyloarthritis. Scand. J. Rheumatol. 2020, 49, 397–404. [Google Scholar] [CrossRef]
- Emad, Y.; Ragab, Y.; Hammam, N.; El-Shaarawy, N.; Fawzi, M.; Amer, A.; El-Makhzangy, H.; Ismail, A.; Ibrahim, O.; Hassan, Y.; et al. The clinical utility of faecal calprotectin in patients with differentiated and undifferentiated spondyloarthritis: Relevance and clinical implications. Reumatol. Clin. 2022, 18, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Khaki-Khatibi, F.; Qujeq, D.; Kashifard, M.; Moein, S.; Maniati, M.; Vaghari-Tabari, M. Calprotectin in inflammatory bowel disease. Clin. Chim. Acta 2020, 510, 556–565. [Google Scholar] [CrossRef]
- Haidmayer, A.; Bosch, P.; Lackner, A.; D′Orazio, M.; Fessler, J.; Stradner, M.H. Effects of probiotic strains on disease activity and enteric permeability in psoriatic arthritis-a pilot open-label study. Nutrients 2020, 12, 2337. [Google Scholar] [CrossRef] [PubMed]
- Jarlborg, M.; Courvoisier, D.S.; Lamacchia, C.; Martinez Prat, L.; Mahler, M.; Bentow, C.; Finckh, A.; Gabay, C.; Nissen, M.J.; physicians of the Swiss Clinical Quality Management (SCQM) registry. Serum calprotectin: A promising biomarker in rheumatoid arthritis and axial spondyloarthritis. Arthritis Res. Ther. 2020, 22, 105. [Google Scholar] [CrossRef]
- Qian, M.; Song, N.J. Serum calprotectin correlates with risk and disease severity in psoriasis patients and the decrease of calprotectin predicts better response to tumor necrosis factor inhibitors. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 3642. [Google Scholar] [PubMed]
- Adarsh, M.B.; Dogra, S.; Vaiphei, K.; Vaishnavi, C.; Sinha, S.K.; Sharma, A. Evaluation of subclinical gut inflammation using faecal calprotectin levels and colonic mucosal biopsy in patients with psoriasis and psoriatic arthritis. Br. J. Dermatol. 2019, 181, 401–402. [Google Scholar] [CrossRef]
- Andréasson, K.; Ohlsson, B.; Mandl, T. Elevated levels of faecal calprotectin in primary Sjögren’s syndrome is common and associated with concomitant organic gastrointestinal disease. Arthritis Res. Ther. 2016, 18, 9. [Google Scholar] [CrossRef] [Green Version]
- Jensen, M.D.; Kjeldsen, J.; Nathan, T. Fecal calprotectin is equally sensitive in Crohn’s disease affecting the small bowel and colon. Scand. J. Gastroenterol. 2011, 46, 694–700. [Google Scholar] [CrossRef]
- Langhorst, J.; Elsenbruch, S.; Koelzer, J.; Rueffer, A.; Michalsen, A.; Dobos, G.J. Noninvasive markers in the assessment of intestinal inflammation in inflammatory bowel diseases: Performance of fecal lactoferrin, calprotectin, and PMN-elastase, CRP, and clinical indices. Am. J. Gastroenterol. 2008, 103, 162–169. [Google Scholar] [CrossRef]
- Moein, S.; Qujeq, D.; Vaghari Tabari, M.; Kashifard, M.L.; Hajian-Tilaki, K. Diagnostic accuracy of fecal calprotectin in assessing the severity of inflammatory bowel disease: From laboratory to clinic. Caspian J. Intern. Med. 2017, 8, 178–182. [Google Scholar]
- Diamanti, A.; Panetta, F.; Basso, M.S.; Forgione, A.; Colistro, F.; Bracci, F.; Papadatou, B.; Francalanci, P.; Torroni, F.; Knafelz, D.; et al. Diagnostic work-up of inflammatory bowel disease in children: The role of calprotectin assay. Inflamm. Bowel Dis. 2010, 16, 1926–1930. [Google Scholar] [CrossRef] [PubMed]
- Roseth, A.G.; Aadland, E.; Jahnsen, J.; Raknerud, N. Assessment of disease activity in ulcerative colitis by faecal calprotectin, a novel granulocyte marker protein. Digestion 1997, 58, 176–180. [Google Scholar] [CrossRef] [PubMed]
- Limburg, P.J.; Ahlquist, D.A.; Sandborn, W.J.; Mahoney, D.W.; Devens, M.E.; Harrington, J.J.; Zinsmeister, A.R. Fecal calprotectin levels predict colorectal inflammation among patients with chronic diarrhea referred for colonoscopy. Am. J. Gastroenterol. 2000, 95, 2831–2837. [Google Scholar] [CrossRef] [PubMed]
- Bunn, S.K.; Bisset, W.M.; Main, M.J.; Golden, B.E. Fecal calprotectin as a measure of disease activity in childhood inflammatory bowel disease. J. Pediatr. Gastroenterol. Nutr. 2001, 32, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Kolho, K.L.; Sipponen, T.; Valtonen, E.; Savilahti, E. Fecal calprotectin, MMP-9, and human beta-defensin-2 levels in pediatric inflammatory bowel disease. Int. J. Colorectal Dis. 2014, 29, 43–50. [Google Scholar] [CrossRef]
- Ollech, J.E.; Normatov, I.; Peleg, N.; Wang, J.; Patel, S.A.; Rai, V.; Yi, Y.; Singer, J.; Dalal, S.R.; Sakuraba, A.; et al. Effectiveness of ustekinumab dose escalation in patients with Crohn’s disease. Clin. Gastroenterol. Hepatol. 2021, 19, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Dreesen, E.; Baert, F.; Laharie, D.; Bossuyt, P.; Bouhnik, Y.; Buisson, A.; Lambrecht, G.; Louis, E.; Oldenburg, B.; Pariente, B.; et al. Monitoring a combination of calprotectin and infliximab identifies patients with mucosal healing of Crohn’s disease. Clin. Gastroenterol. Hepatol. 2020, 18, 637–646.e11. [Google Scholar] [CrossRef]
- Miossec, P.; Kolls, J.K. Targeting IL-17 and TH17 cells in chronic inflammation. Nat. Rev. Drug Discov. 2012, 11, 763–776. [Google Scholar] [CrossRef]
- Iwakura, Y.; Ishigame, H.; Saijo, S.; Nakae, S. Functional specialization of interleukin-17 family members. Immunity 2011, 34, 149–162. [Google Scholar] [CrossRef] [Green Version]
- Hohenberger, M.; Cardwell, L.A.; Oussedik, E.; Feldman, S.R. Interleukin-17 inhibition: Role in psoriasis and inflammatory bowel disease. J. Dermatolog. Treat. 2018, 29, 13–18. [Google Scholar] [CrossRef]
- van den Berg, W.B.; McInnes, I.B. Th17 cells and IL-17 a—Focus on immunopathogenesis and immunotherapeutics. Semin. Arthritis Rheum. 2013, 43, 158–170. [Google Scholar] [CrossRef] [PubMed]
- Harper, E.G.; Guo, C.; Rizzo, H.; Lillis, J.V.; Kurtz, S.E.; Skorcheva, I.; Purdy, D.; Fitch, E.; Iordanov, M.; Blauvelt, A. Th17 cytokines stimulate CCL20 expression in keratinocytes in vitro and in vivo: Implications for psoriasis pathogenesis. J. Investig. Dermatol. 2009, 129, 2175–2183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohnmacht, C.; Marques, R.; Presley, L.; Sawa, S.; Lochner, M.; Eberl, G. Intestinal microbiota, evolution of the immune system and the bad reputation of pro-inflammatory immunity. Cell Microbiol. 2011, 13, 653–659. [Google Scholar] [CrossRef]
- Hueber, W.; Sands, B.E.; Lewitzky, S.; Vandemeulebroecke, M.; Reinisch, W.; Higgins, P.D.; Wehkamp, J.; Feagan, B.G.; Yao, M.D.; Karczewski, M.; et al. Secukinumab, a human anti-IL-17A monoclonal antibody, for moderate to severe Crohn’s disease: Unexpected results of a randomised, double-blind placebo-controlled trial. Gut 2012, 61, 1693–1700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Targan, S.R.; Feagan, B.; Vermeire, S.; Panaccione, R.; Melmed, G.Y.; Landers, C.; Li, D.; Russell, C.; Newmark, R.; Zhang, N.; et al. A randomized, double-blind, placebo-controlled phase 2 study of brodalumab in patients with moderate-to-severe Crohn’s disease. Am. J. Gastroenterol. 2016, 111, 1599–1607. [Google Scholar] [CrossRef]
- Yamada, A.; Wang, J.; Komaki, Y.; Komaki, F.; Micic, D.; Sakuraba, A. Systematic review with meta-analysis: Risk of new onset IBD with the use of anti-interleukin-17 agents. Aliment. Pharmacol. Ther. 2019, 50, 373–385. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, S.; Colombel, J.F.; Feagan, B.G.; Reich, K.; Deodhar, A.A.; McInnes, I.B.; Porter, B.; Das Gupta, A.; Pricop, L.; Fox, T. Incidence rates of inflammatory bowel disease in patients with psoriasis, psoriatic arthritis and ankylosing spondylitis treated with secukinumab: A retrospective analysis of pooled data from 21 clinical trials. Ann. Rheum. Dis. 2019, 78, 473–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavelka, K.; Kivitz, A.; Dokoupilova, E.; Blanco, R.; Maradiaga, M.; Tahir, H.; Pricop, L.; Andersson, M.; Readie, A.; Porter, B. Efficacy, safety, and tolerability of secukinumab in patients with active ankylosing spondylitis: A randomized, double-blind phase 3 study, MEASURE 3. Arthritis Res. Ther. 2017, 19, 285. [Google Scholar] [CrossRef] [Green Version]
- Baraliakos, X.; Kivitz, A.J.; Deodhar, A.A.; Braun, J.; Wei, J.C.; Delicha, E.M.; Talloczy, Z.; Porter, B. MEASURE 1 Study Group. Long-term effects of interleukin-17A inhibition with secukinumab in active ankylosing spondylitis: 3-year efficacy and safety results from an extension of the Phase 3 MEASURE 1 trial. Clin. Exp. Rheumatol. 2018, 36, 50–55. [Google Scholar]
- Braun, J.; Baraliakos, X.; Deodhar, A.; Baeten, D.; Sieper, J.; Emery, P.; Readie, A.; Martin, R.; Mpofu, S.; Richards, H.B. MEASURE 1 study group. Effect of secukinumab on clinical and radiographic outcomes in ankylosing spondylitis: 2-year results from the randomised phase III MEASURE 1 study. Ann. Rheum. Dis. 2017, 76, 1070–1077. [Google Scholar] [CrossRef]
- Braun, J.; Baraliakos, X.; Deodhar, A.; Poddubnyy, D.; Emery, P.; Delicha, E.M.; Talloczy, Z.; Porter, B. Secukinumab shows sustained efficacy and low structural progression in ankylosing spondylitis: 4-year results from the MEASURE 1 study. Rheumatology 2019, 58, 859–868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marzo-Ortega, H.; Sieper, J.; Kivitz, A.; Blanco, R.; Cohen, M.; Martin, R.; Readie, A.; Richards, H.B.; Porter, B.; Measure 2 Study Group. Secukinumab and sustained improvement in signs and symptoms of patients with active ankylosing spondylitis through two years: Results from a phase III study. Arthritis Care Res. 2017, 69, 1020–1029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marzo-Ortega, H.; Sieper, J.; Kivitz, A.; Blanco, R.; Cohen, M.; Delicha, E.M.; Rohrer, S.; Richards, H. Secukinumab provides sustained improvements in the signs and symptoms of active ankylosing spondylitis with high retention rate: 3-year results from the phase III trial, MEASURE 2. RMD Open 2017, 3, e000592. [Google Scholar] [CrossRef] [PubMed]
- Fauny, M.; Moulin, D.; D′Amico, F.; Netter, P.; Petitpain, N.; Arnone, D.; Jouzeau, J.Y.; Loeuille, D.; Peyrin-Biroulet, L. Paradoxical gastrointestinal effects of interleukin-17 blockers. Ann. Rheum. Dis. 2020, 79, 1132–1138. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Patients (n = 129) N, %, Mean ± SD |
|---|---|
| Demographics | |
| Male | 73 |
| Female | 56 |
| Age (years) | 54 ± 13.6 |
| Weight (kg) | 79.5 ± 15.5 |
| Height (cm) | 173.8 ± 11.5 |
| BMI (kg/m²) | 28.3 ± 5.8 |
| Co-morbidities | |
| PsA | 4.65 % |
| Hypertension | 5.42 % |
| Diabetes | 3.87 % |
| Dyslipidaemia | 5.42 % |
| Inflammatory Bowel Disease | 5.28 % |
| Other | 10.8 % |
| Psoriasis | |
| Family History of PsO | 6.20% |
| PASI | 17 ± 4.8 |
| Previous therapy | |
| Bio-naïve | 32% |
| Bio-experienced | 68% |
| ≥2 Biological agent | 40% |
| Pz | Current Therapy | Faecal CP (μg/g) at Baseline | Faecal CP (μg/g) at W24 | Diagnosis |
|---|---|---|---|---|
| 1 | Secukinumab | 49 | 154 | Crohn’s disease |
| 2 | Secukinumab | 50 | 110 | Ulcerative proctitis |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Brizzi, E.V.; Rocco, A.; Babino, G.; Buononato, D.; Argenziano, G.; Balato, A. Evaluation of the Role of Faecal Calprotectin in the Management of Psoriatic Patients under Treatment with Biologic Drugs. Biomedicines 2022, 10, 2968. https://doi.org/10.3390/biomedicines10112968
Di Brizzi EV, Rocco A, Babino G, Buononato D, Argenziano G, Balato A. Evaluation of the Role of Faecal Calprotectin in the Management of Psoriatic Patients under Treatment with Biologic Drugs. Biomedicines. 2022; 10(11):2968. https://doi.org/10.3390/biomedicines10112968
Chicago/Turabian StyleDi Brizzi, Eugenia Veronica, Annachiara Rocco, Graziella Babino, Dario Buononato, Giuseppe Argenziano, and Anna Balato. 2022. "Evaluation of the Role of Faecal Calprotectin in the Management of Psoriatic Patients under Treatment with Biologic Drugs" Biomedicines 10, no. 11: 2968. https://doi.org/10.3390/biomedicines10112968