
Circulating Cancer Associated Macrophage-like Cells as a Potential New Prognostic Marker in Pancreatic Ductal Adenocarcinoma
 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Cohort
2.2. Blood Collection
2.3. CAML and CTC Detection
2.4. Statistical Analysis
3. Results
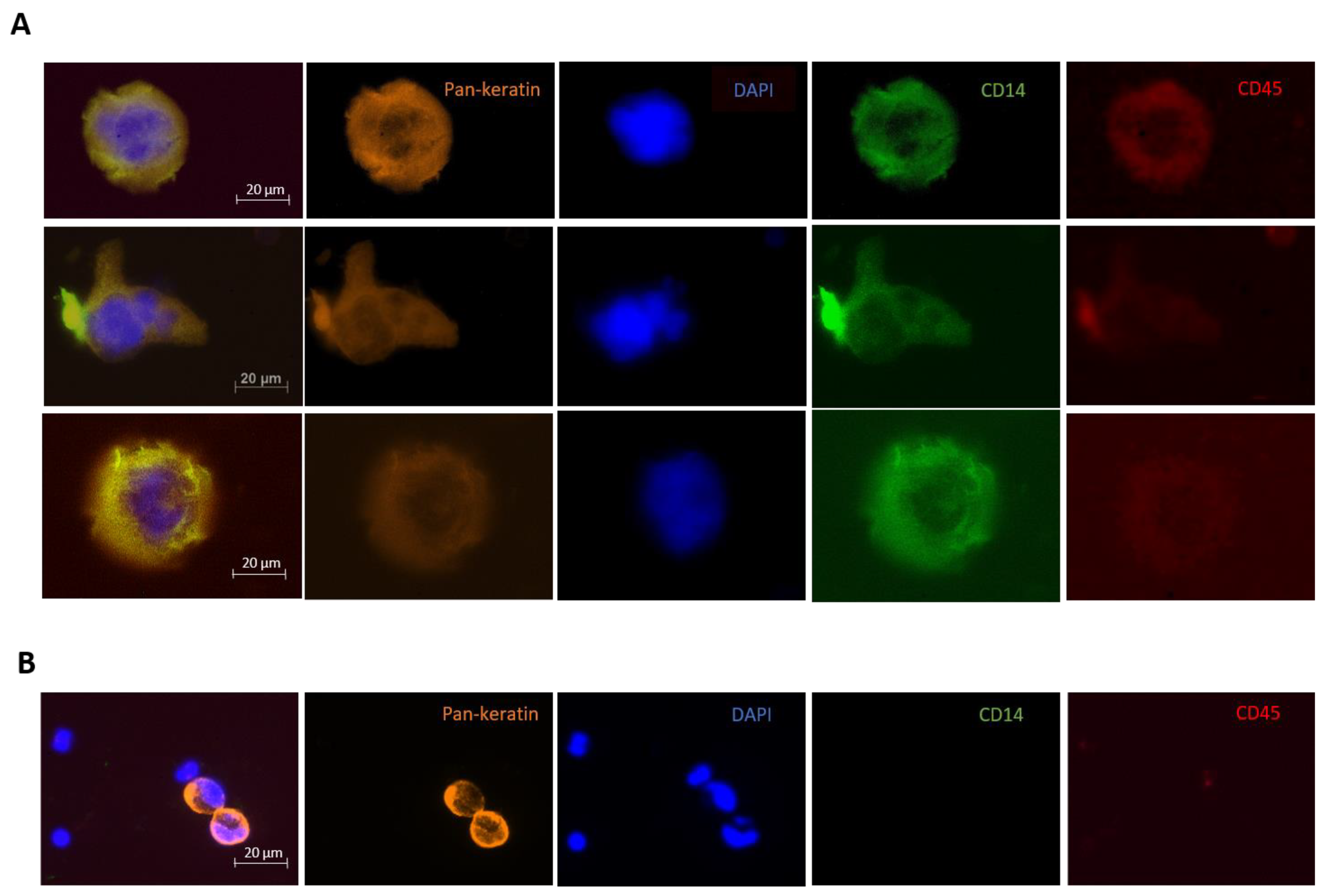
3.1. CAML Detection
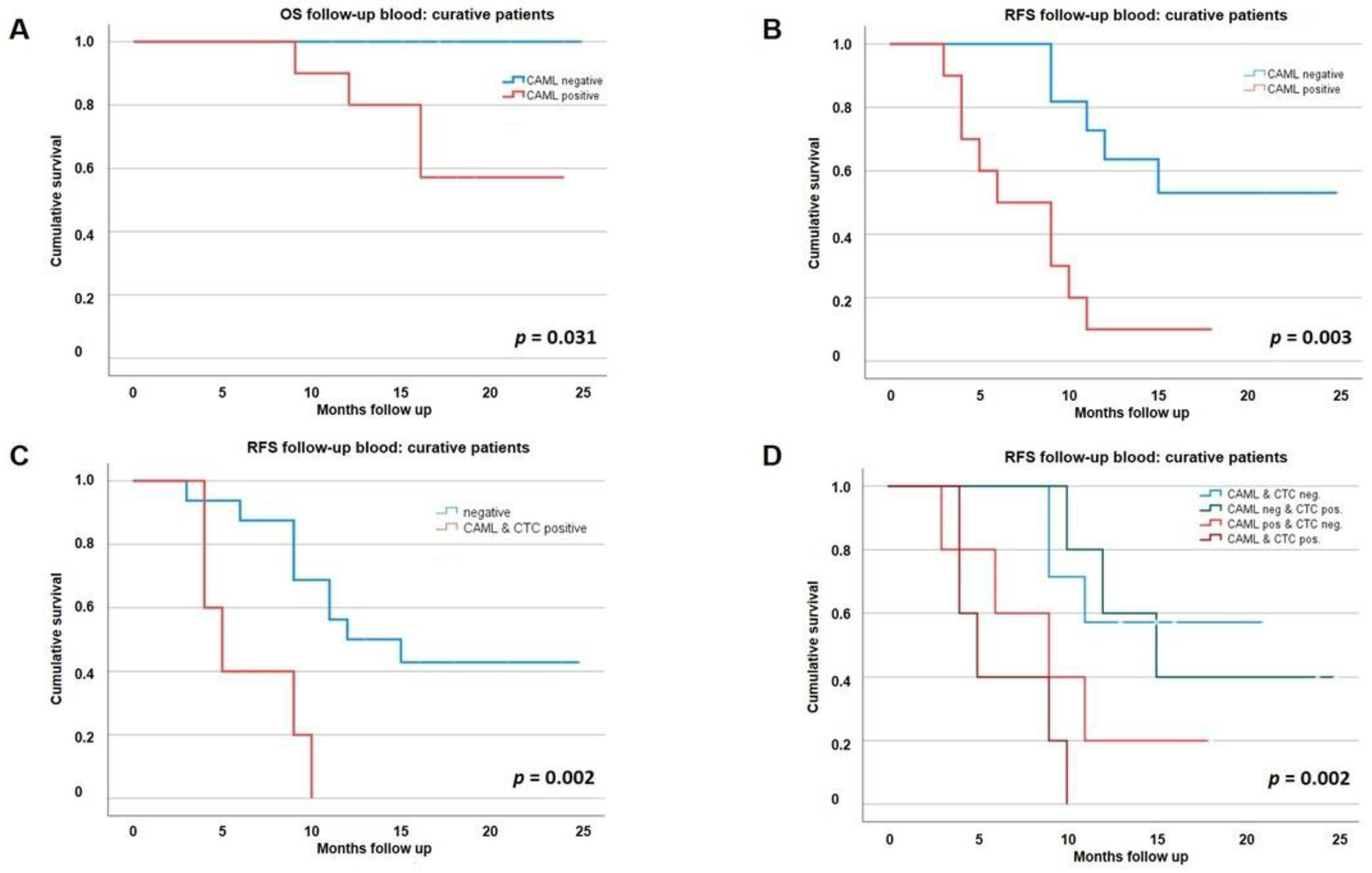
3.2. Clinical Value of CAMLs alongside CTCs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pantel, K.; Alix-Panabières, C. Liquid biopsy and minimal residual disease—Latest advances and implications for cure. Nat. Rev. Clin. Oncol. 2019, 16, 409–424. [Google Scholar] [CrossRef] [PubMed]
- Yeo, D.; Bastian, A.; Strauss, H.; Saxena, P.; Grimison, P.; Rasko, J.E.J. Exploring the Clinical Utility of Pancreatic Cancer Circulating Tumor Cells. Int. J. Mol. Sci. 2022, 23, 1671. [Google Scholar] [CrossRef] [PubMed]
- Effenberger, K.E.; Schroeder, C.; Hanssen, A.; Wolter, S.; Eulenburg, C.; Tachezy, M.; Gebauer, F.; Izbicki, J.R.; Pantel, K.; Bockhorn, M. Improved Risk Stratification by Circulating Tumor Cell Counts in Pancreatic Cancer. Clin. Cancer Res. 2018, 24, 2844–2850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martini, V.; Timme-Bronsert, S.; Fichtner-Feigl, S.; Hoeppner, J.; Kulemann, B. Circulating Tumor Cells in Pancreatic Cancer: Current Perspectives. Cancers 2019, 11, 1659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, M.M.; Ramani, V.C.; Jeffrey, S.S. Circulating tumor cell technologies. Mol. Oncol. 2016, 10, 374–394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, X.-L.; Li, Y.-Y.; Zhang, J.; Huang, J.-W.; Jia, H.-Y.; Liu, L.; Li, P. Prognostic Role of Circulating Tumor Cells in Patients with Pancreatic Cancer: A Meta-analysis. Asian Pac. J. Cancer Prev. 2014, 15, 6015–6020. [Google Scholar] [CrossRef] [Green Version]
- Han, L.; Chen, W.; Zhao, Q. Prognostic value of circulating tumor cells in patients with pancreatic cancer: A meta-analysis. Tumor Biol. 2013, 35, 2473–2480. [Google Scholar] [CrossRef]
- Gast, C.E.; Silk, A.D.; Zarour, L.; Riegler, L.; Burkhart, J.G.; Gustafson, K.T.; Parappilly, M.S.; Roh-Johnson, M.; Goodman, J.R.; Olson, B.; et al. Cell fusion potentiates tumor heterogeneity and reveals circulating hybrid cells that correlate with stage and survival. Sci. Adv. 2018, 4, eaat7828. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Zhou, N.; Yu, X.; Zhang, X.; Li, S.; Lei, Z.; Hu, R.; Li, H.; Mao, Y.; Wang, X.; et al. Tumacrophage: Macrophages transformed into tumor stem-like cells by virulent genetic material from tumor cells. Oncotarget 2017, 8, 82326–82343. [Google Scholar] [CrossRef] [Green Version]
- Adams, D.L.; Martin, S.S.; Alpaugh, R.K.; Charpentier, M.; Tsai, S.; Bergan, R.C.; Ogden, I.M.; Catalona, W.; Chumsri, S.; Tang, C.-M.; et al. Circulating giant macrophages as a potential biomarker of solid tumors. Proc. Natl. Acad. Sci. USA 2014, 111, 3514–3519. [Google Scholar] [CrossRef]
- Tang, C.-M.; Adams, D.L. Clinical Applications of Cancer-Associated Cells Present in the Blood of Cancer Patients. Biomedicines 2022, 10, 587. [Google Scholar] [CrossRef] [PubMed]
- Pereira-Veiga, T.; Schneegans, S.; Pantel, K.; Wikman, H. Circulating tumor cell-blood cell crosstalk: Biology and clinical relevance. Cell Rep. 2022, 40, 111298. [Google Scholar] [CrossRef] [PubMed]
- Lustberg, M.B.; Balasubramanian, P.; Miller, B.; Garcia-Villa, A.; Deighan, C.; Wu, Y.; Carothers, S.; Berger, M.; Ramaswamy, B.; Macrae, E.R.; et al. Heterogeneous atypical cell populations are present in blood of metastatic breast cancer patients. Breast Cancer Res. 2014, 16, R23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clawson, G.A.; Matters, G.; Xin, P.; Imamura-Kawasawa, Y.; Du, Z.; Thiboutot, D.M.; Helm, K.F.; Neves, R.; Abraham, T. Macrophage-Tumor Cell Fusions from Peripheral Blood of Melanoma Patients. PLoS ONE 2015, 10, e0134320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, D.L.; Adams, D.K.; Alpaugh, R.K.; Cristofanilli, M.; Martin, S.S.; Chumsri, S.; Tang, C.M.; Marks, J.R. Circulating Cancer-Associated Macrophage-like Cells Differentiate Malignant Breast Cancer and Benign Breast Conditions. Cancer Epidemiol. Biomark. Prev. 2016, 25, 1037–1042. [Google Scholar] [CrossRef] [Green Version]
- Mu, Z.; Wang, C.; Ye, Z.; Rossi, G.; Sun, C.; Li, L.; Zhu, Z.; Yang, H.; Cristofanilli, M. Prognostic values of cancer associated macrophage-like cells (CAML) enumeration in metastatic breast cancer. Breast Cancer Res. Treat. 2017, 165, 733–741. [Google Scholar] [CrossRef]
- Manjunath, Y.; Mitchem, J.B.; Suvilesh, K.N.; Avella, D.M.; Kimchi, E.T.; Staveley-O’Carroll, K.F.; Deroche, C.B.; Pantel, K.; Li, G.; Kaifi, J.T. Circulating Giant Tumor-Macrophage Fusion Cells Are Independent Prognosticators in Patients With NSCLC. J. Thorac. Oncol. 2020, 15, 1460–1471. [Google Scholar] [CrossRef]
- Clawson, G.A.; Matters, G.L.; Xin, P.; McGovern, C.; Wafula, E.; Depamphilis, C.; Meckley, M.; Wong, J.; Stewart, L.; D’Jamoos, C.; et al. “Stealth dissemination” of macrophage-tumor cell fusions cultured from blood of patients with pancreatic ductal adenocarcinoma. PLoS ONE 2017, 12, e0184451. [Google Scholar] [CrossRef] [Green Version]
- Nitschke, C.; Markmann, B.; Tölle, M.; Kropidlowski, J.; Belloum, Y.; Goetz, M.R.; Schlüter, H.; Kwiatkowski, M.; Sinn, M.; Izbicki, J.; et al. Characterization of RARRES1 Expression on Circulating Tumor Cells as Unfavorable Prognostic Marker in Resected Pancreatic Ductal Adenocarcinoma Patients. Cancers 2022, 14, 4405. [Google Scholar] [CrossRef]
- Koch, C.; Joosse, S.A.; Schneegans, S.; Wilken, O.J.W.; Janning, M.; Loreth, D.; Müller, V.; Prieske, K.; Banys-Paluchowski, M.; Horst, L.J.; et al. Pre-Analytical and Analytical Variables of Label-Independent Enrichment and Automated Detection of Circulating Tumor Cells in Cancer Patients. Cancers 2020, 12, 442. [Google Scholar] [CrossRef]
- Loreth, D.; Schuette, M.; Zinke, J.; Mohme, M.; Piffko, A.; Schneegans, S.; Stadler, J.; Janning, M.; Loges, S.; Joosse, S.; et al. CD74 and CD44 Expression on CTCs in Cancer Patients with Brain Metastasis. Int. J. Mol. Sci. 2021, 22, 6993. [Google Scholar] [CrossRef] [PubMed]
- Neves, R.P.L.; Ammerlaan, W.; Andree, K.C.; Bender, S.; Cayrefourcq, L.; Driemel, C.; Koch, C.; Luetke-Eversloh, M.V.; Oulhen, M.; Rossi, E.; et al. Proficiency Testing to Assess Technical Performance for CTC-Processing and Detection Methods in CANCER-ID. Clin. Chem. 2021, 67, 631–641. [Google Scholar] [CrossRef] [PubMed]
- Götze, J.; Nitschke, C.; Uzunoglu, F.G.; Pantel, K.; Sinn, M.; Wikman, H. Tumor-Stroma Interaction in PDAC as a New Approach for Liquid Biopsy and its Potential Clinical Implications. Front. Cell Dev. Biol. 2022, 10, 918795. [Google Scholar] [CrossRef] [PubMed]
- Buscail, E.; Alix-Panabières, C.; Quincy, P.; Cauvin, T.; Chauvet, A.; Degrandi, O.; Caumont, C.; Verdon, S.; Lamrissi, I.; Moranvillier, I.; et al. High Clinical Value of Liquid Biopsy to Detect Circulating Tumor Cells and Tumor Exosomes in Pancreatic Ductal Adenocarcinoma Patients Eligible for Up-Front Surgery. Cancers 2019, 11, 1656. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Curative Patients n = 36 | ||||||||
|---|---|---|---|---|---|---|---|---|
| n | % | No CAML Detection at Baseline n = 23 | CAML Detection at Baseline n = 13 | p Value | ||||
| n | % | n | % | |||||
| Age | ≤67 years | 18 | 50.0 | 11 | 47.8 | 7 | 53.8 | 1.000 |
| >67 years | 18 | 50.0 | 12 | 52.2 | 6 | 46.2 | ||
| Gender | male | 17 | 47.2 | 11 | 47.8 | 6 | 46.2 | 1.000 |
| female | 19 | 52.8 | 12 | 52.2 | 7 | 53.8 | ||
| ECOG | 0 | 20 | 55.6 | 11 | 47.8 | 9 | 69.2 | 0.446 |
| 1 | 14 | 38.9 | 10 | 43.5 | 4 | 30.8 | ||
| 2 | 2 | 5.6 | 2 | 8.7 | 0 | 0 | ||
| Neoadjuvant treatment | no | 29 | 80.6 | 19 | 82.6 | 10 | 76.9 | 0.686 |
| yes | 7 | 19.4 | 4 | 17.4 | 3 | 23.1 | ||
| Surgical procedure | PD/PPPD | 20 | 55.6 | 13 | 56.5 | 7 | 53.8 | 1.000 |
| left pancreatectomy | 13 | 36.1 | 8 | 34.8 | 5 | 38.5 | ||
| total pancreatectomy | 3 | 8.3 | 2 | 8.7 | 1 | 7.7 | ||
| Adjuvant treatment | No 1 | 7 | 19.4 | 4 | 17.4 | 3 | 23.1 | 0.686 |
| yes | 29 | 80.6 | 19 | 82.6 | 10 | 76.9 | ||
| Dindo classification | 0–2 | 19 | 52.8 | 13 | 56.5 | 6 | 46.2 | 0.156 |
| 3–4 | 12 | 33.3 | 7 | 30.4 | 5 | 38.5 | ||
| 5 | 5 | 13.9 | 3 | 13.0 | 2 | 15.4 | ||
| pT stage | T1-2 | 17 | 47.2 | 11 | 47.8 | 6 | 46.2 | 1.000 |
| T3-4 | 19 | 52.8 | 12 | 52.2 | 7 | 53.8 | ||
| pN stage | N0 | 10 | 27.8 | 8 | 34.8 | 2 | 15.4 | 0.270 |
| N + (N1/2) | 26 | 72.2 | 15 | 65.2 | 11 | 84.6 | ||
| Grading 2 | G2 | 23 | 69.7 | 14 | 66.7 | 9 | 75.0 | 0.710 |
| G3 | 10 | 30.3 | 7 | 33.3 | 3 | 25.0 | ||
| R status | R0, CRM- | 18 | 50.0 | 11 | 47.8 | 7 | 53.8 | 1.000 |
| R0, CRM + /R1 | 18 | 50.0 | 12 | 52.2 | 6 | 46.2 | ||
| UICC | I-II | 28 | 77.8 | 18 | 78.3 | 10 | 64.3 | 1.000 |
| III | 8 | 22.2 | 5 | 21.7 | 3 | 62.5 | ||
| Ca 19-9 | ≤500 U/mL | 26 | 72.2 | 17 | 73.9 | 9 | 69.2 | 1.000 |
| >500 U/mL | 10 | 27.8 | 6 | 26.1 | 4 | 30.8 | ||
| no | 16 | 44.4 | 9 | 39.1 | 7 | 53.8 | ||
| Recurrence | yes | 20 | 55.6 | 14 | 60.9 | 6 | 46.2 | 0.493 |
| no | 27 | 75.0 | 17 | 73.9 | 10 | 76.9 | ||
| CTC detection at baseline | yes | 9 | 25.0 | 6 | 26.1 | 3 | 23.1 | 1.000 |
| Univariate | N = 33 $ | |||
|---|---|---|---|---|
| Univariate Analyses | Median RFS, Months (95% CI) | p-Value | ||
| Age | ≤67 years | 17 | 10.0 (7.2–12.8) | 0.218 |
| >67 years | 16 | 15.7 (11.0–20.5) * | ||
| Gender | male | 16 | 9.0 (3.8–14.2) | 0.170 |
| female | 17 | 15.0 (9.5–20.5) | ||
| ECOG performance status | 0 | 20 | 16.0 (9.0–21.8) | 0.296 |
| 1 | 12 | 11.3 (6.3–14.1) | ||
| 2 | 1 | 10.0 (10.0–10.0) | ||
| Uicc stage | I-II | 26 | 16.1 (12.6–19.6) * | 0.005 |
| III | 7 | 6.0 (3.4–8.6) | ||
| R-status | R0; CRM- | 17 | 10.0 (6.0–14.0) | 0.227 |
| R0; CRM + /R1 | 16 | 16.0 (9.1–22.9) | ||
| Grading ~ | G2 | 21 | 11.0 (9.6–12.4) | 0.353 |
| G3 | 9 | 14.8 (10.3–19.4) * | ||
| Neoadjuvant treatment | no | 26 | 12.0 (6.0–18.0) | 0.089 |
| yes | 7 | 9.0 (0–19.3) | ||
| Adjuvant treatment | no | 4 | 6.0 (0.0–12.0) * | 0.009 |
| yes | 29 | 12.0 (6.7–17.3) | ||
| Clavien-dindo | 0–2 | 20 | 16.0 (7.9–24.1) | 0.161 |
| 3–4 | 13 | 10.0 (7.7–12.3) | ||
| Ca 19-9 baseline | <500 U/mL | 24 | 12.0 (5.9–18.1) | 0.881 |
| ≥500 U/mL | 9 | 11.0 (8.2–13.8) | ||
| CAMLs detected at FUP # | no | 12 | 18.6 (14.4–22.8) * | 0.003 |
| yes | 10 | 6.0 (1.9–10.1) | ||
| Combined analysis CAML detection and CTC detection at FUP # | no | 17 | 12 (4.7–19.3) | 0.002 |
| yes, both detectable | 5 | 5 (2.9–8.1) |
| Multivariate I: RFS Curative Cohort | HR (95% CI) | p-Value | |
| Adjuvant treatment | no | 0.4 (0.04–3.5) | 0.381 |
| yes | reference | ||
| UICC | no | reference | |
| yes | 1.9 (1.1–3.4) | 0.032 | |
| CAMLs detected at FUP | no | reference | |
| yes | 8.7 (2.0–37.0) | 0.023 | |
| Multivariate II: RFS curative cohort | HR (95% CI) | p-value | |
| Adjuvant treatment | no | 0.4 (0.05–3.9) | 0.451 |
| yes | reference | ||
| UICC | no | reference | |
| yes | 2.5 (1.3–4.7) | 0.004 | |
| Combined analysis CAML detection and CTC detection at FUP | no | reference | 0.003 |
| yes | 8.7 (2.0–37.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nitschke, C.; Markmann, B.; Konczalla, L.; Kropidlowski, J.; Pereira-Veiga, T.; Scognamiglio, P.; Schönrock, M.; Sinn, M.; Tölle, M.; Izbicki, J.; et al. Circulating Cancer Associated Macrophage-like Cells as a Potential New Prognostic Marker in Pancreatic Ductal Adenocarcinoma. Biomedicines 2022, 10, 2955. https://doi.org/10.3390/biomedicines10112955
Nitschke C, Markmann B, Konczalla L, Kropidlowski J, Pereira-Veiga T, Scognamiglio P, Schönrock M, Sinn M, Tölle M, Izbicki J, et al. Circulating Cancer Associated Macrophage-like Cells as a Potential New Prognostic Marker in Pancreatic Ductal Adenocarcinoma. Biomedicines. 2022; 10(11):2955. https://doi.org/10.3390/biomedicines10112955
Chicago/Turabian StyleNitschke, Christine, Benedikt Markmann, Leonie Konczalla, Jolanthe Kropidlowski, Thais Pereira-Veiga, Pasquale Scognamiglio, Martin Schönrock, Marianne Sinn, Marie Tölle, Jakob Izbicki, and et al. 2022. "Circulating Cancer Associated Macrophage-like Cells as a Potential New Prognostic Marker in Pancreatic Ductal Adenocarcinoma" Biomedicines 10, no. 11: 2955. https://doi.org/10.3390/biomedicines10112955