
Arrhythmias after SARS-CoV-2 Vaccination in Patients with a Cardiac Implantable Electronic Device: A Multicenter Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design
2.2. Participants
2.3. Methods
2.4. Definition of Terms
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Dhama, K.; Khan, S.; Tiwari, R.; Sircar, S.; Bhat, S.; Malik, Y.S.; Singh, K.P.; Chaicumpa, W.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J. Coronavirus Disease 2019-COVID-19. Clin. Microbiol. Rev. 2020, 33, e00028-20. [Google Scholar] [CrossRef] [PubMed]
- Maiese, A.; Frati, P.; Del Duca, F.; Santoro, P.; Manetti, A.C.; La Russa, R.; Di Paolo, M.; Turillazzi, E.; Fineschi, V. Myocardial Pathology in COVID-19-Associated Cardiac Injury: A Systematic Review. Diagnostics 2021, 11, 1647. [Google Scholar] [CrossRef] [PubMed]
- Maiese, A.; Baronti, A.; Manetti, A.C.; Di Paolo, M.; Turillazzi, E.; Frati, P.; Fineschi, V. Death after the Administration of COVID-19 Vaccines Approved by EMA: Has a Causal Relationship Been Demonstrated? Vaccines 2022, 10, 308. [Google Scholar] [CrossRef] [PubMed]
- Kyriakidis, N.C.; Lopez-Cortes, A.; Gonzalez, E.V.; Grimaldos, A.B.; Prado, E.O. SARS-CoV-2 vaccines strategies: A comprehensive review of phase 3 candidates. NPJ Vaccines 2021, 6, 28. [Google Scholar] [CrossRef] [PubMed]
- Menni, C.; Klaser, K.; May, A.; Polidori, L.; Capdevila, J.; Louca, P.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Merino, J.; et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: A prospective observational study. Lancet Infect. Dis. 2021, 21, 939–949. [Google Scholar] [CrossRef]
- Varney, J.A.; Dong, V.S.; Tsao, T.; Sabir, M.S.; Rivera, A.T.; Ghula, S.; Moriles, K.E.M.; Cherukuri, M.L.; Fazal, R.; Azevedo, C.B.; et al. COVID-19 and arrhythmia: An overview. J. Cardiol. 2022, 79, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.; Lee, Y.W.; Lim, S.Y.; Lee, J.H.; Lim, J.S.; Lee, S.; Park, S.; Kim, S.-K.; Lim, Y.J.; Kim, E.O.; et al. Adverse Reactions Following the First Dose of ChAdOx1 nCoV-19 Vaccine and BNT162b2 Vaccine for Healthcare Workers in South Korea. J. Korean Med. Sci. 2021, 36, e115. [Google Scholar] [CrossRef] [PubMed]
- Ananwattanasuk, T.; Tanawuttiwat, T.; Chokesuwattanaskul, R.; Lathkar-Pradhan, S.; Barham, W.; Oral, H.; Thakur, R.K.; Jongnarangsin, K. Programming implantable cardioverter-defibrillator in primary prevention: Guideline concordance and outcomes. Heart Rhythm 2020, 17, 1101–1106. [Google Scholar] [CrossRef] [PubMed]
- Haigney, M.C.; Zareba, W.; Nasir, J.M.; McNitt, S.; McAdams, D.; Gentlesk, P.J.; Goldstein, R.E.; Moss, A.J.; MADIT II Investigators. Gender differences and risk of ventricular tachycardia or ventricular fibrillation. Heart Rhythm 2009, 6, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Al-Ali, D.; Elshafeey, A.; Mushannen, M.; Kawas, H.; Shafiq, A.; Mhaimeed, N.; Mhaimeed, O.; Mhaimeed, N.; Zeghlache, R.; Salameh, M.; et al. Cardiovascular and haematological events post COVID-19 vaccination: A systematic review. J. Cell. Mol. Med. 2022, 26, 636–653. [Google Scholar] [CrossRef] [PubMed]
- Wenande, E.; Garvey, L.H. Immediate-type hypersensitivity to polyethylene glycols: A review. Clin. Exp. Allergy 2016, 46, 907–922. [Google Scholar] [CrossRef] [PubMed]
- Brojakowska, A.; Narula, J.; Shimony, R.; Bander, J. Clinical Implications of SARS-CoV-2 Interaction With Renin Angiotensin System: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2020, 75, 3085–3095. [Google Scholar] [CrossRef] [PubMed]
- Greinacher, A.; Thiele, T.; Warkentin, T.E.; Weisser, K.; Kyrle, P.A.; Eichinger, S. Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 Vaccination. N. Engl. J. Med. 2021, 384, 2092–2101. [Google Scholar] [CrossRef] [PubMed]
- Patone, M.; Mei, X.W.; Handunnetthi, L.; Dixon, S.; Zaccardi, F.; Shankar-Hari, M.; Watkinson, P.; Khunti, K.; Harnden, A.; Coupland, C.A.C.; et al. Risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination or SARS-CoV-2 infection. Nat. Med. 2022, 28, 410–422. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic * | Patient Cohort n = 180 |
|---|---|
| Median (IQR) age in years | 70 (59–79) [min = 24, max = 98] |
| Male:Female, n(%) | 101 (56): 79 (43) |
| Mean (SD) BMI (kg/m2) | 23.6 (4.3) |
| Number of vaccines received | |
| 1 | 180 (100) |
| 2 | 83 (49) |
| 3 | 4 (2) |
| Indication | |
| Sinus node dysfunction | 54 (30) |
| AV block | 57 (32) |
| Primary prevention for VT/VF | 33 (18) |
| Secondary prevention for VT/VF | 19 (11) |
| Cardiac resynchronization | 10 (6) |
| Unknown | 7 (4) |
| Type of device | |
| Single chamber pacemaker | 17 |
| Dual chamber pacemaker | 93 |
| Single chamber AICD | 41 |
| Dual chamber AICD | 15 |
| CRT-D | 12 |
| CRT-P | 2 |
| Company of device | |
| Abbott | 51 |
| Boston | 68 |
| Medtronic | 61 |
| Vaccine received | |
| ChAdOx1 | 154 (86) |
| Sinovac/Sinopharm | 21 (12) |
| mRNA | 5 (3) |
| Comorbidities | |
| Atrial fibrillation | 44 (31) |
| Ischemic heart disease | 43 (24) |
| Chronic kidney disease ** | 30 (17) |
| Valvular heart disease *** | 20 (11) |
| Brugada syndrome | 13 (7) |
| Left ventricular ejection fraction (LVEF) **** | |
| ≥40% | 82 |
| <40% | 30 |
| Side Effect * | Overall N = 180 |
|---|---|
| Any side effect (%) | 38 (21%) |
| Fever | 13 (7%) |
| Headache | 2 (1%) |
| Local reaction | 9 (5%) |
| Dyspnea | 1 (0.5%) |
| Insomnia | 1 (0.5%) |
| >1 side effect | 12 (7%) |
| Vaccination 1 (N = 180) | ||
|---|---|---|
| Timing | Variable | N |
| Pre-vaccination | Any SVT * | 4 |
| sum of SVT ** | 7 | |
| Any VT # | 3 | |
| sum of VT ## | 6 | |
| Post-vaccination | Any SVT | 7 |
| sum of SVT | 63 | |
| Any VT | 9 | |
| sum of VT | 47 | |
| Vaccination 2 (N = 83) | ||
| Timing | Variable | N |
| Pre-vaccination | Any SVT | 10 |
| sum of SVT | 79 | |
| Any VT | 3 | |
| sum of VT | 6 | |
| Post-vaccination | Any SVT | 13 |
| sum of SVT | 81 | |
| Any VT | 1 | |
| sum of VT | 3 | |
| Vaccination 3 (N = 4) | ||
| Timing | Variable | N |
| Pre-vaccination | Any SVT | 0 |
| N of SVT | 0 | |
| Any VT | 0 | |
| N of VT | 0 | |
| Post-vaccination | Any SVT | 1 |
| N of SVT | 3 | |
| Any VT | 0 | |
| N of VT | 0 | |
| All vaccinations (N = 267) | ||
| Timing | Variable | N |
| Pre-vaccination | Any SVT | 14 |
| N of SVT | 86 | |
| Any VT | 6 | |
| N of VT | 12 | |
| Post-vaccination | Any SVT | 21 |
| N of SVT | 147 | |
| Any VT | 10 | |
| N of VT | 50 |
| Univariable | Multivariable | |||
|---|---|---|---|---|
| Characteristic | IRR (95% CI) | p | aIRR (95% CI) | p |
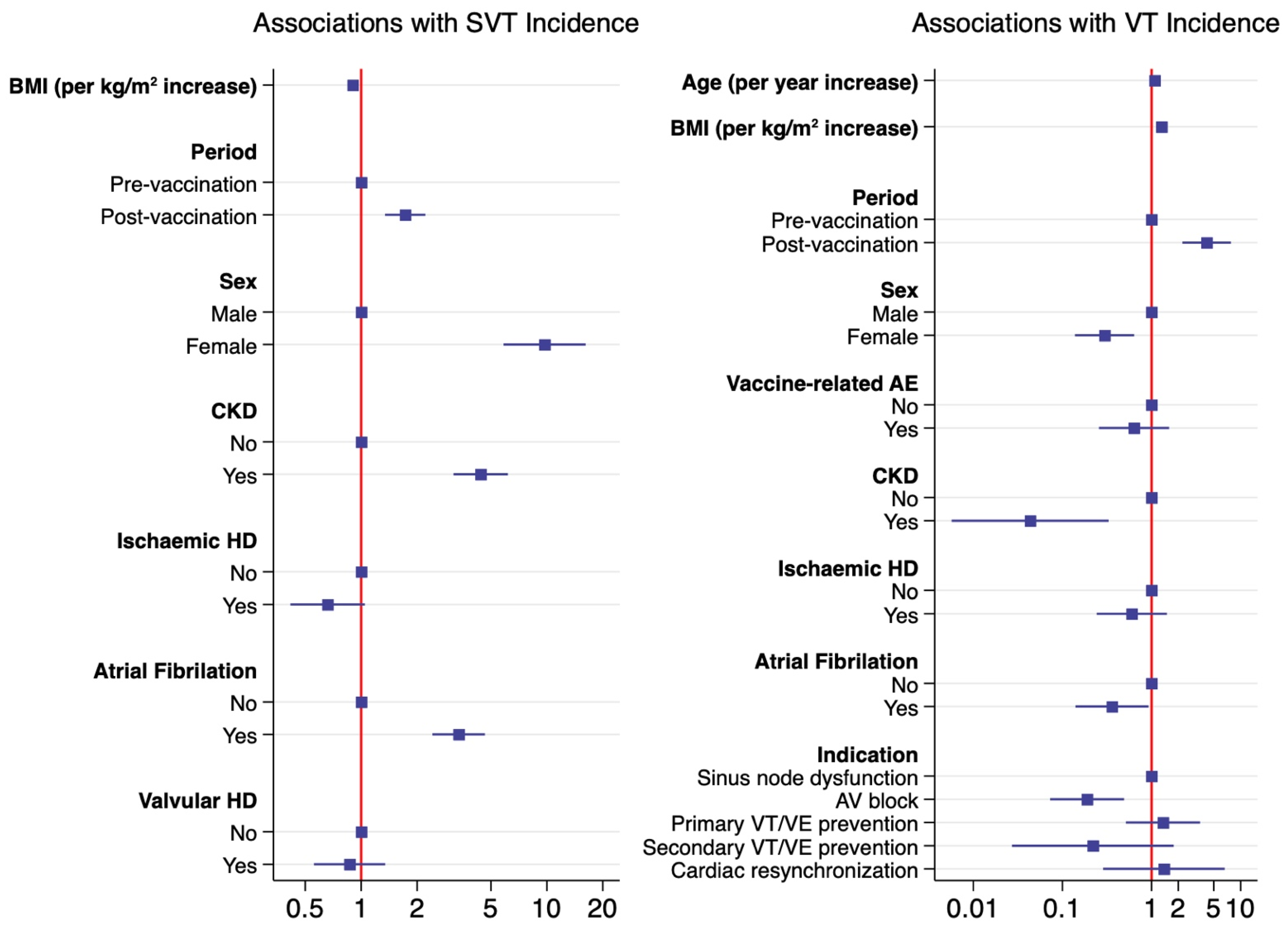
| Post- vs pre-vaccination | 1.72 (1.33–2.21) | <0.001 | 1.73 (1.34–2.22) | <0.001 |
| Female vs. male sex | 10.88 (6.74–17.55) | <0.001 | 9.72 (5.84–16.17) | <0.001 |
| Age (per year increase) | 1.00 (0.99–1.004) | 0.30 | ||
| BMI (per kg/m2 increase) | 0.87 (0.83–0.9) | <0.001 | 0.90 (0.87–0.94) | <0.001 |
| Experienced vaccine-related AE | 1.01 (0.71–1.43) | 0.97 | ||
| CKD | 4.26 (3.14–5.8) | <0.001 | 4.40 (3.14–6.16) | <0.001 |
| IHD | 0.57 (0.38–0.84) | 0.005 | 0.66 (0.42–1.05) | 0.08 |
| AF | 3.88 (2.88–5.22) | <0.001 | 3.35 (2.42–4.64) | <0.001 |
| Valvular HD | 2.89 (2.05–4.08) | <0.001 | 0.87 (0.56–1.35) | 0.87 |
| Brugada syndrome | 0.57 (0.28–1.13) | 0.11 | ||
| Characteristic | Univariable | Multivariable | ||
|---|---|---|---|---|
| IRR (95% CI) | p | aIRR (95% CI) | p | |
| Post- vs. pre-vaccination | 4.09 (2.21–7.56) | <0.001 | 4.16 (2.22–7.79) | <0.001 |
| Female vs. male sex | 0.35 (0.19–0.64) | 0.001 | 0.3 (0.14–0.64) | 0.002 |
| Age (per year increase) | 1.02 (0.999–1.04) | 0.07 | 1.09 (1.05–1.13) | <0.001 |
| BMI (per kg/m2 increase) | 1.35 (1.29–1.41) | <0.001 | 1.3 (1.23–1.36) | <0.001 |
| Experienced vaccine-related AE | 0.45 (0.20–1.01) | 0.053 | 0.64 (0.26–1.58) | 0.33 |
| Hypertension | 6.25 (3.05–12.81) | <0.001 | ||
| DM | 0.33 (0.14–0.78) | 0.01 | ||
| CKD | 0.08 (0.01–0.6) | 0.01 | 0.04 (0.01–0.33) | 0.002 |
| IHD | 4.03 (2.40–6.77) | <0.001 | 0.6 (0.24–1.49) | 0.27 |
| AF | 0.26 (0.11–0.62) | 0.002 | 0.36 (0.14–0.93) | 0.03 |
| Valvular HD | 0.76 (0.30–1.93) | 0.56 | ||
| Indication | <0.001 | 0.004 | ||
| Sinus node dysfunction | 1 (ref) | 1 (ref) | ||
| AV block | 0.33 (0.13–0.85) | 0.19 (0.07–0.49) | ||
| Primary prevention for VT/VF | 2.91 (1.64–5.16) | 1.35 (0.52–3.51) | ||
| Secondary prevention for VT/VF | 0.15 (0.02–1.16) | 0.22 (0.03–1.78) | ||
| Cardiac resynchronization | 0.57 (0.13–2.54) | 1.38 (0.29–6.62) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sangpornsuk, N.; Rungpradubvong, V.; Tokavanich, N.; Srisomwong, S.; Ananwattanasuk, T.; Teerawongsakul, P.; Kerr, S.J.; Suwanwalaikorn, M.; Jongnarangsin, K.; Chokesuwattanaskul, R. Arrhythmias after SARS-CoV-2 Vaccination in Patients with a Cardiac Implantable Electronic Device: A Multicenter Study. Biomedicines 2022, 10, 2838. https://doi.org/10.3390/biomedicines10112838
Sangpornsuk N, Rungpradubvong V, Tokavanich N, Srisomwong S, Ananwattanasuk T, Teerawongsakul P, Kerr SJ, Suwanwalaikorn M, Jongnarangsin K, Chokesuwattanaskul R. Arrhythmias after SARS-CoV-2 Vaccination in Patients with a Cardiac Implantable Electronic Device: A Multicenter Study. Biomedicines. 2022; 10(11):2838. https://doi.org/10.3390/biomedicines10112838
Chicago/Turabian StyleSangpornsuk, Naruepat, Voravut Rungpradubvong, Nithi Tokavanich, Sathapana Srisomwong, Teetouch Ananwattanasuk, Padoemwut Teerawongsakul, Stephen J. Kerr, Mathurin Suwanwalaikorn, Krit Jongnarangsin, and Ronpichai Chokesuwattanaskul. 2022. "Arrhythmias after SARS-CoV-2 Vaccination in Patients with a Cardiac Implantable Electronic Device: A Multicenter Study" Biomedicines 10, no. 11: 2838. https://doi.org/10.3390/biomedicines10112838