
Irradiation Alters the Expression of MUC1, CD44 and Hyaluronan in Oral Mucosal Epithelium
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Characteristics
2.2. Sample Harvesting
2.2.1. MUC1 Staining
2.2.2. HA Staining
2.2.3. CD44 Staining
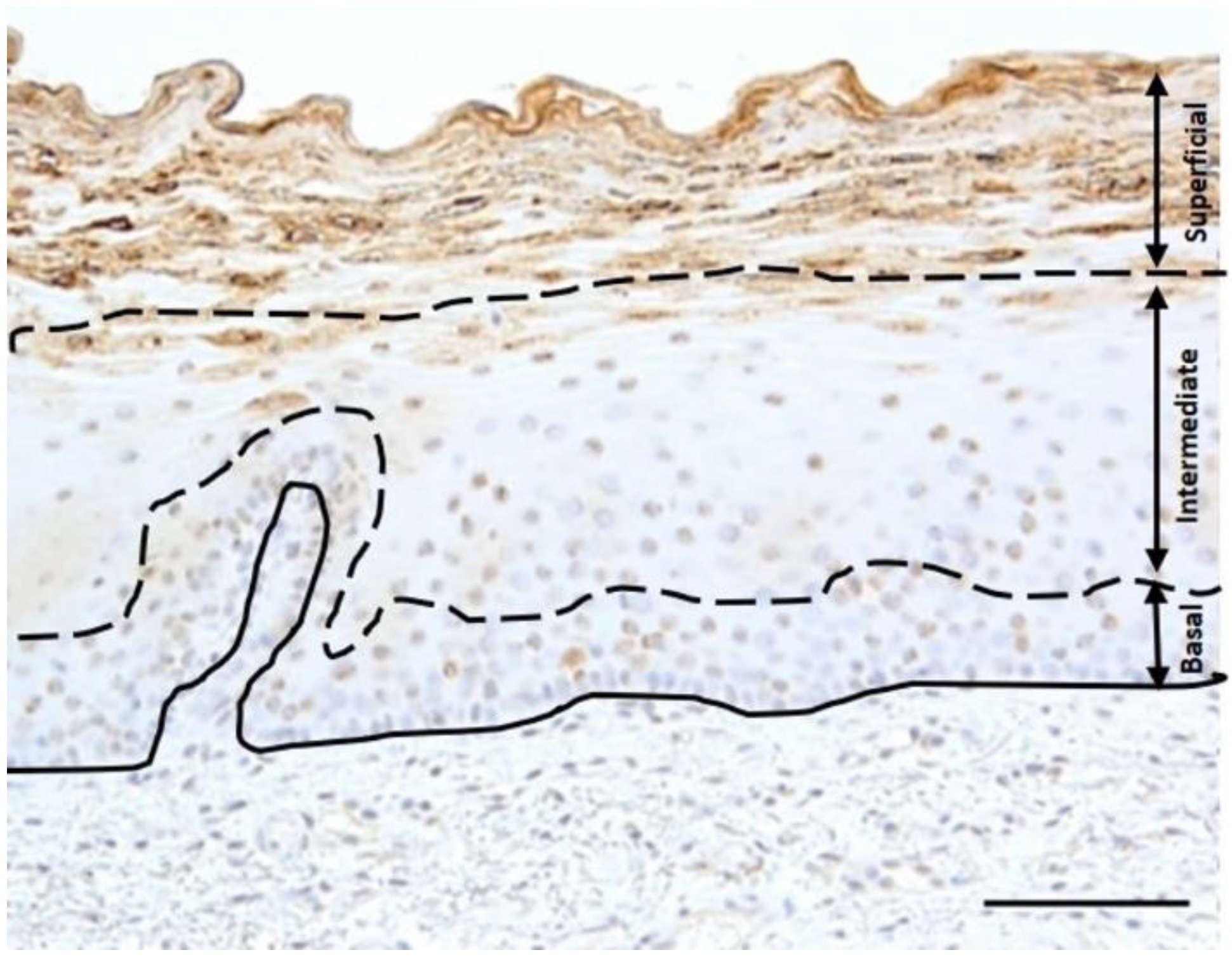
2.3. Staining Analysis and Statistics
2.4. Transmission Electron Microscopy (TEM)
3. Results
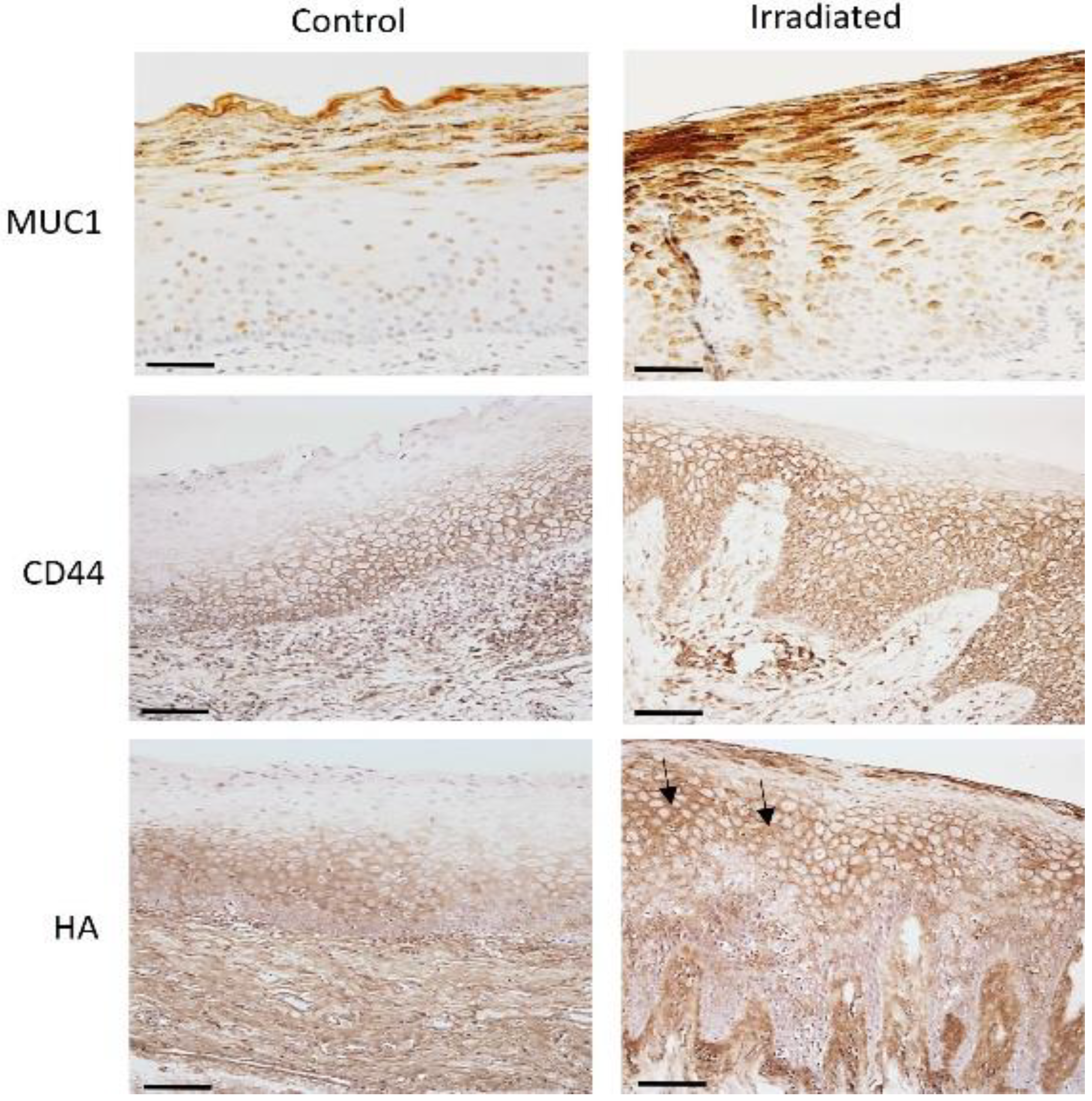
3.1. The Intensity of MUC1, CD44 and HA in Control and Irradiated Mucosa
3.2. Immunostaining of HA and CD44 in Irradiated Mucosa
3.3. MUC1 and CD44 Atypical Immunostaining in Irradiated Mucosa
3.4. Cell Junction Alteration in the Suprabasal Cell Layer
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- El-Naggar, A.K.; Chan, C.J.; Grandis, J.R.; Takata, T.; Slootweg, P.J. WHO classification of Head and Neck Tumours; IARC: Lyon, France, 2017. [Google Scholar]
- Bianco, B.C.F.; Sperandio, F.F.; Hanemann, J.A.C.; Pereira, A.A.C. New WHO odontogenic tumor classification: Impact on prevalence in a population. J. Appl. Oral. Sci. 2019, 28, e20190067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuonen, F.; Secondini, C.; Rüegg, C. Molecular pathways: Emerging pathways mediating growth, invasion, and metastasis of tumors progressing in an irradiated microenvironment. Clin. Cancer Res. 2012, 18, 5196–5202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsumoto, M.; Komiyama, K.; Okaue, M.; Shimoyama, Y.; Iwakami, K.; Namaki, S.; Tanaka, H.; Moro, I.; Sato, H. Predicting tumor metastasis in patients with oral cancer by means of the proliferation marker Ki67. J. Oral. Sci. 1999, 41, 53–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Girod, S.C.; Pfeiffer, P.; Ries, J.; Pape, H.D. Proliferative activity and loss of function of tumor suppressor genes as ‘biomarkers’ in diagnosis and prognosis of benign and preneoplastic oral lesions and oral squamous cell carcinoma. Br. J. Oral. Maxillofac. Surg. 1998, 36, 252–260. [Google Scholar] [CrossRef]
- Smith, B.D.; Smith, G.L.; Carter, D.; Sasaki, C.T.; Haffty, B.G. Prognostic significance of vascular endothelial growth factor protein levels in oral and oropharyngeal squamous cell carcinoma. J. Clin. Oncol. 2000, 18, 2046–2052. [Google Scholar] [CrossRef]
- Bagutti, C.; Speight, P.M.; Watt, F.M. Comparison of integrin, cadherin, and catenin expression in squamous cell carcinomas of the oral cavity. J. Pathol. 1998, 186, 8–16. [Google Scholar] [CrossRef]
- Hussein, A.A.; Forouzanfar, T.; Bloemena, E.; de Visscher, J.; Brakenhoff, R.H.; Leemans, C.R.; Helder, M.N. A review of the most promising biomarkers for early diagnosis and prognosis prediction of tongue squamous cell carcinoma. Br. J. Cancer 2018, 119, 724–736. [Google Scholar] [CrossRef] [Green Version]
- McAuley, J.L.; Linden, S.K.; Png, C.W.; King, R.M.; Pennington, H.L.; Gendler, S.J.; Florin, T.H.; Hill, G.R.; Korolik, V.; McGuckin, M.A. MUC1 cell surface mucin is a critical element of the mucosal barrier to infection. J. Clin. Investig. 2007, 117, 2313–2324. [Google Scholar] [CrossRef]
- Piyush, T.; Chacko, A.R.; Sindrewicz, P.; Hilkens, J.; Rhodes, J.M.; Yu, L.G. Interaction of galectin-3 with MUC1 on cell surface promotes EGFR dimerization and activation in human epithelial cancer cells. Cell. Death. Differ. 2017, 24, 1937–1947. [Google Scholar] [CrossRef]
- Ukkonen, H.; Kashyap, B.; Sirvio, E.; Dekker, H.; Vahanikkila, H.; Pirhonen, P.; Mikkonen, J.J.W.; ten Bruggenkate, C.M.; Schulten, E.A.J.M.; Koistinen, A.; et al. Effect of Radiotherapy on Expression of Transmembrane Mucin MUC1 in Oral Mucosal Cells. Int. J. Oral-Med. Sci. 2020, 19, 1–10. [Google Scholar] [CrossRef]
- Wang, S.J.; Earle, C.; Wong, G.; Bourguignon, L.Y.W. Role of hyaluronan synthase 2 to promote CD44-dependent oral cavity squamous cell carcinoma progression. Head Neck. 2013, 35, 511–520. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, M.; Takahashi, H.; Rajabi, H.; Alam, M.; Suzuki, Y.; Yin, L.; Tagde, A.; Maeda, T.; Hiraki, M.; Sukhatme, V.P.; et al. Functional interactions of the cystine/glutamate antiporter, CD44v and MUC1-C oncoprotein in triple-negative breast cancer cells. Oncotarget 2016, 7, 11756–11769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosunen, A.; Ropponen, K.; Kellokoski, J.; Pukkila, M.; Virtaniemi, J.; Valtonen, H.; Kumpulainen, E.; Johansson, R.; Tammi, R.; Tammi, M.; et al. Reduced expression of hyaluronan is a strong indicator of poor survival in oral squamous cell carcinoma. Oral. Oncol. 2004, 40, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Zhao, S.; Karnad, A.; Freeman, J.W. The biology and role of CD44 in cancer progression: Therapeutic implications. J Hematol Oncol. 2018, 11, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heldin, P.; Karousou, E.; Bernert, B.; Porsch, H.; Nishitsuka, K.; Skandalis, S.S. Importance of hyaluronan-CD44 interactions in inflammation and tumorigenesis. Connect. Tissue Res. 2008, 49, 215–218. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Rahmanian, M.; Widstrom, C.; Lepperdinger, G.; Frost, G.I.; Heldin, P. Irradiation-induced expression of hyaluronan (HA), synthase 2 and hyaluronidase 2 genes in rat lung tissue accompanies active turnover of HA and induction of types I and III collagen gene expression. Am. J. Respir. Cell. Mol. Biol. 2000, 23, 411–418. [Google Scholar] [CrossRef] [Green Version]
- Tammi, R.; Tammi, M.; Häkkinen, L.; Larjava, H. Histochemical localization of hyaluronate in human oral epithelium using a specific hyaluronate-binding probe. Arch. Oral. Biol. 1990, 35, 219–224. [Google Scholar] [CrossRef]
- Hirvikoski, P.; Tammi, R.; Kumpulainen, E.; Virtaniemi, J.; Parkkinen, J.J.; Tammi, M.; Johansson, R.; Agren, U.; Karhunen, J.; Kosma, V.M. Irregular expression of hyaluronan and its CD44 receptor is associated with metastatic phenotype in laryngeal squamous cell carcinoma. Virchows. Arch. 1999, 434, 37–44. [Google Scholar] [CrossRef]
- Wang, C.; Tammi, M.; Guo, H.; Tammi, R. Hyaluronan distribution in the normal epithelium of esophagus, stomach, and colon and their cancers. Am. J. Pathol. 1996, 148, 1861–1869. [Google Scholar]
- Ukkonen, H.; Pirhonen, P.; Herrala, M.; Mikkonen, J.J.; Singh, S.P.; Sormunen, R.; Kullaa, A.M. Oral mucosal epithelial cells express the membrane anchored mucin MUC1. Arch. Oral. Biol. 2017, 73, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Hämäläinen, K.; Kosma, V.M.; Eloranta, M.L.; Tammi, R.; Tammi, M.; Leppänen, M.; Leppänen, M.; Heinonen, S.; Anttila, M. Downregulated CD44 and hyaluronan expression in vulvar intraepithelial neoplasia and squamous cell carcinomas. Acta Obstet. Gynecol. Scand. 2010, 89, 108–119. [Google Scholar] [CrossRef] [PubMed]
- Arciniegas, E.; Carrillo, L.M.; Rojas, H.; Ramírez, R.; Reyes, O.; Suárez, A.; Ortega, F. Mucin1 expression in focal epidermal dysplasia of actinic keratosis. Ann. Transl. Med. 2015, 3, 245. [Google Scholar] [PubMed]
- Litvinov, S.V.; Hilkens, J. The epithelial sialomucin, episialin, is sialylated during recycling. J. Biol. Chem. 1993, 268, 21364–21371. [Google Scholar] [CrossRef]
- Kashyap, B.; Kullaa, A.M. Regulation of mucin 1 expression and its relationship with oral diseases. Arch. Oral. Biol. 2020, 117, 104791. [Google Scholar] [CrossRef]
- Ratushny, V.; Gober, M.D.; Hick, R.; Ridky, T.W.; Seykora, J.T. From keratinocyte to cancer: The pathogenesis and modeling of cutaneous squamous cell carcinoma. J. Clin. Investig. 2012, 122, 464–472. [Google Scholar] [CrossRef] [Green Version]
- Sonis, S.T. The pathobiology of mucositis. Nat. Rev. 2004, 4, 277. [Google Scholar] [CrossRef]
- Chase, L.P.; Toto, P.D.; Magalotti, M.F. Radiation-induced Changes in the Epithelium of the Buccal Mucosa. J. Dent. Res. 1961, 40, 929–935. [Google Scholar] [CrossRef]
- Raina, D.; Agarwal, P.; Lee, J.; Bharti, A.; McKnight, C.J.; Sharma, P.; Kharbanda, S.; Kufe, D. Characterization of the MUC1-C Cytoplasmic Domain as a Cancer Target. PLoS ONE 2015, 10, e0135156. [Google Scholar]
- Bourguignon, L.Y.W. Matrix Hyaluronan-CD44 Interaction Activates MicroRNA and LncRNA Signaling Associated with Chemoresistance, Invasion, and Tumor Progression. Front. Oncol. 2019, 9, 492. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patients (N = 59) | Male/Female | Age Range (Mean Age) | Tumor Site (N) | Total RT Dose (Gy) (Mean Dose) | Local RT Dose * (Gy) (Mean Dose) | Interval RT Biopsy (Months) |
|---|---|---|---|---|---|---|
| Group 1 Controls (N = 35) | 16/19 | 33–79 y (56 y) | - | - | - | - |
| Group 2 (N = 24) | 20/4 | 54–84 y (69 y) | OC (N = 14) SG (N = 5) NP or L (N = 5) | 54–70 (62 Gy) 54–70 Gy 60–70 Gy 70 Gy | 15–66 (41 Gy) 34–66 Gy 32–60 Gy 15–34 Gy | 11–199 11–199 10–23 72–171 |
| MUC1 | CD44 | HA | ||||
|---|---|---|---|---|---|---|
| Control (n = 35) | IR (n = 24) | Control (n = 35) | IR (n = 24) | Control (n = 35) | IR (n = 24) | |
| Superficial cells | ||||||
| -Considerable staining | 83% | 75% | 3% | 33% | 3% | 29% |
| -Some staining | 17% | 13% | 26% | 38% | 26% | 38% |
| -No staining | 0% | 13% | 71% | 29% | 71% | 33% |
| p < 0.01 | p < 0.01 | |||||
| Intermediate layer | ||||||
| -Considerable staining | 31% | 71% | 17% | 86% | 17% | 58% |
| -Some staining | 57% | 13% | 50% | 14% | 46% | 42% |
| -No staining | 11% | 17% | 33% | 0% | 37% | 0% |
| p < 0.001 | p < 0.001 | p < 0.0001 | ||||
| Basal layer | ||||||
| -Considerable staining | 0% | 38% | 66% | 71% | 34% | 38% |
| -Some staining | 0% | 46% | 33% | 29% | 54% | 54% |
| -No staining | 100% | 17% | 0% | 0% | 11% | 8% |
| p < 0001 | ||||||
| Stroma | ||||||
| -Considerable staining | 0% | 4% | 60% | 40% | 60% | 29% |
| -Some staining | 0% | 0% | 40% | 43% | 40% | 54% |
| -No staining | 100% | 96% | 0% | 17% | 0% | 17% |
| p < 0.01 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kashyap, B.; Naumanen, K.; Mikkonen, J.; Dekker, H.; Schulten, E.; Bloemena, E.; Pasonen-Seppänen, S.; Kullaa, A. Irradiation Alters the Expression of MUC1, CD44 and Hyaluronan in Oral Mucosal Epithelium. Biomedicines 2022, 10, 2816. https://doi.org/10.3390/biomedicines10112816
Kashyap B, Naumanen K, Mikkonen J, Dekker H, Schulten E, Bloemena E, Pasonen-Seppänen S, Kullaa A. Irradiation Alters the Expression of MUC1, CD44 and Hyaluronan in Oral Mucosal Epithelium. Biomedicines. 2022; 10(11):2816. https://doi.org/10.3390/biomedicines10112816
Chicago/Turabian StyleKashyap, Bina, Konsta Naumanen, Jopi Mikkonen, Hannah Dekker, Engelbert Schulten, Elisabeth Bloemena, Sanna Pasonen-Seppänen, and Arja Kullaa. 2022. "Irradiation Alters the Expression of MUC1, CD44 and Hyaluronan in Oral Mucosal Epithelium" Biomedicines 10, no. 11: 2816. https://doi.org/10.3390/biomedicines10112816