
Characterization of Vascular Patterns Associated with Endothelial Glycocalyx Damage in Early- and Late-Onset Preeclampsia
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Inclusion and Exclusion Criteria
2.3. Diagnostic Evaluation of Preeclampsia and Fetal Growth Restriction
2.4. Hemodynamics and Cardiovascular Parameters
2.5. Ultrasonic Dopplerography of Vessels
2.6. Detection of Proteoglycan Levels in Blood Serum
2.7. Statistical Analysis
3. Results
3.1. Clinical Results
3.2. Assessment of Blood Flow in the Maternal-Placental-Fetal Axis
3.3. Hemodynamic Parameters in Patients with PE and in Normotensive Women of Normal Pregnancy Groups
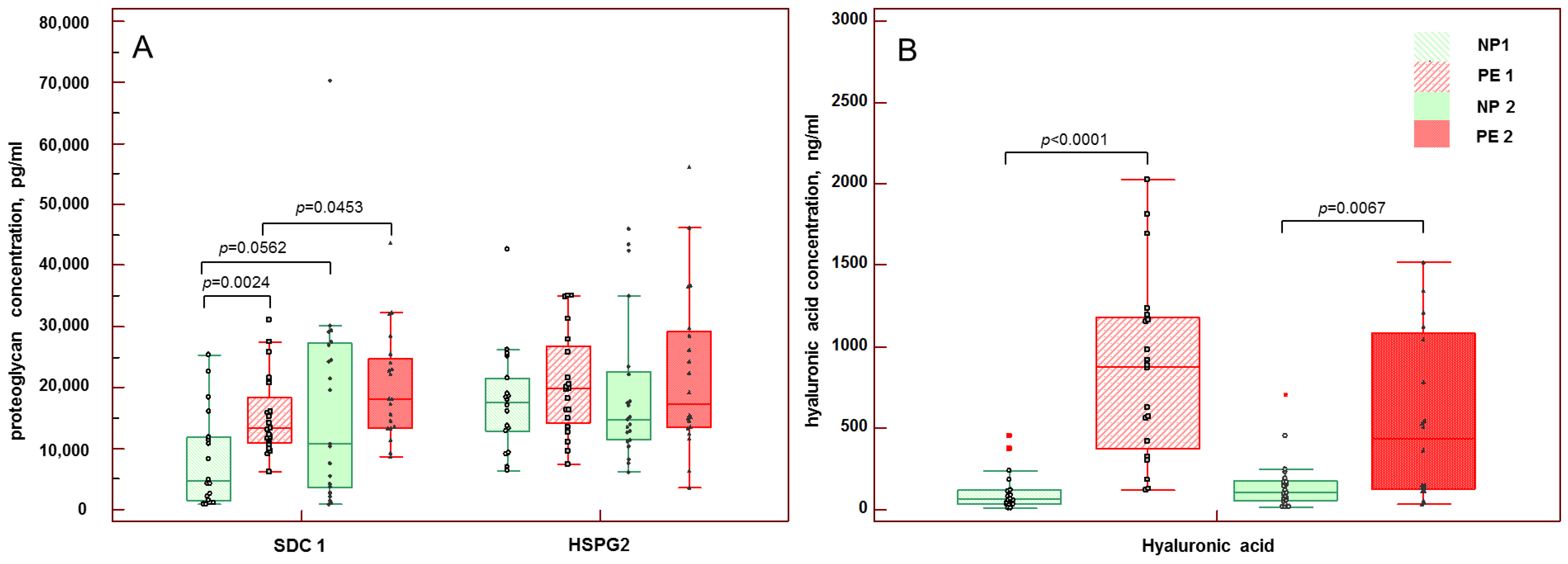
3.4. Concentrations of Soluble Components of eGC in Maternal Blood
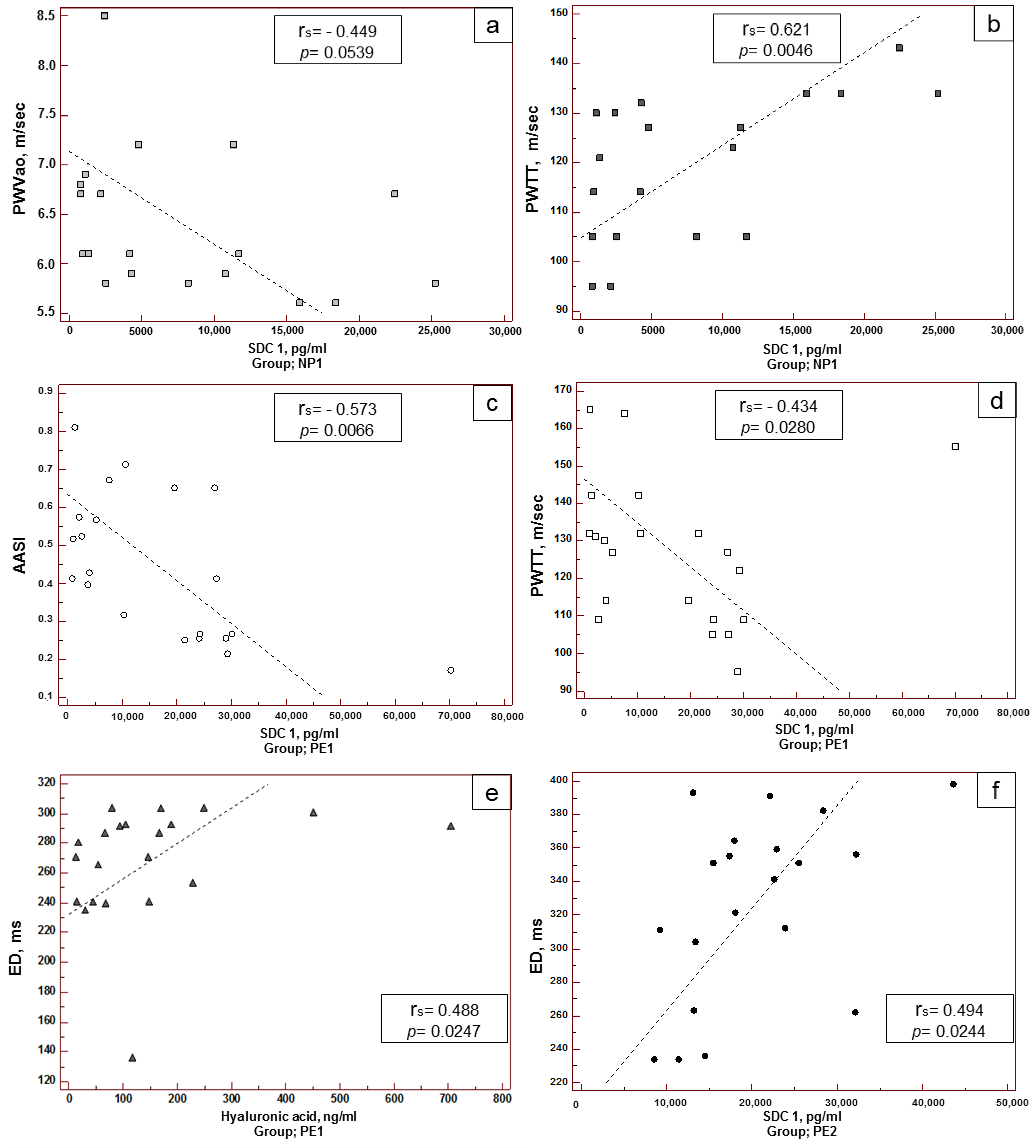
3.5. Correlation of Maternal Hemodynamic Parameters with the Concentration of Soluble Components of eGC in Blood
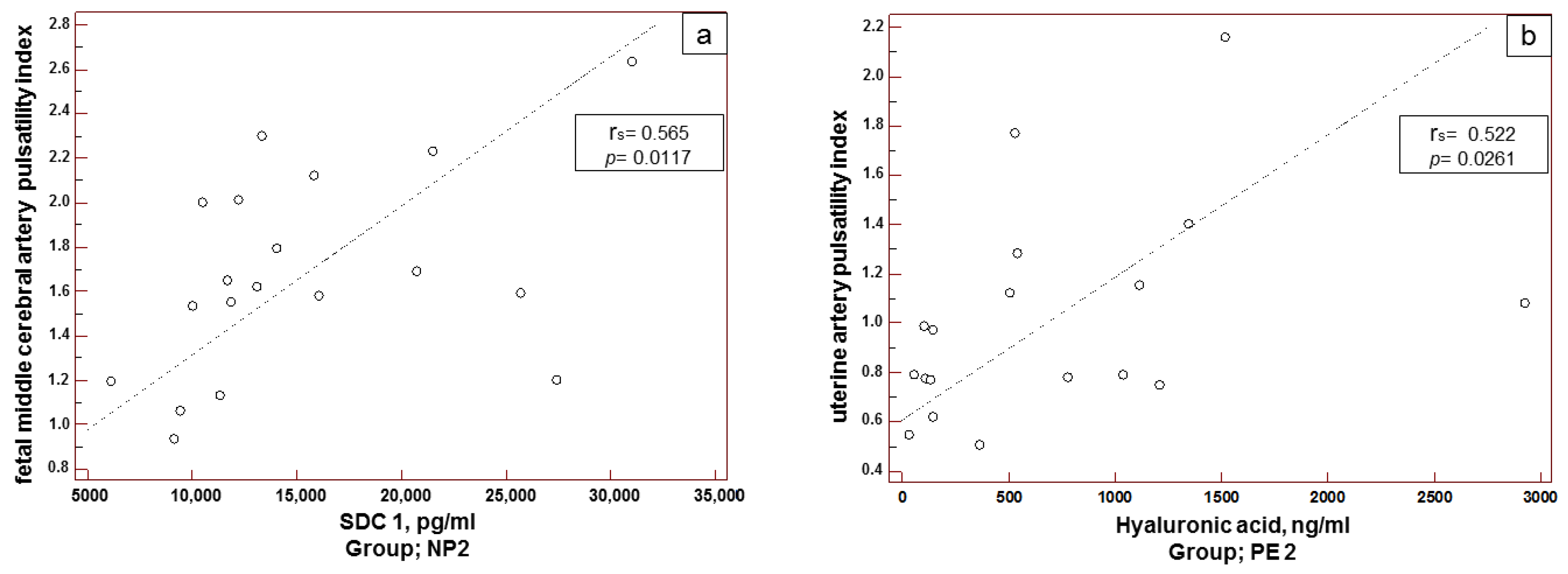
3.6. Correlation between Maternal–Placental–Fetal Hemodynamic Parameters and Blood Concentration of Soluble Components of eGC
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AASI | arterial stiffness index |
| AC | abdominal circumference |
| AIx | augmentation index |
| BMI | body mass index |
| BP | blood pressure |
| CPR | cerebroplacental ratio |
| DAD | diastolic blood pressure |
| DBPM | daily blood pressure monitoring |
| (dP/dt)max | maximal blood pressure increase velocity |
| ED | ejection duration |
| eGC | endothelial glycocalyx |
| FGR | fetal growth restriction |
| GA | gestational age |
| HA | hyaluronic acid |
| HSPG2 | heparan sulfate proteoglycan 2 |
| LMW-HA | low-molecular weight hyaluronic acid |
| max DADao | maximal aortal diastolic blood pressure |
| max SADao | maximal aortal systolic blood pressure |
| MCA | middle cerebral artery |
| med DADao | mean aortal diastolic blood pressure |
| med SADao | mean aortal systolic blood pressure |
| min DADao | minimal aortal diastolic blood pressure |
| min SADao | minimal aortal systolic blood pressure |
| NP1 | healthy pregnancy of 20–34 weeks |
| NP2 | healthy pregnancy > 34 weeks or onwards |
| PE | preeclampsia |
| PE1 | early-onset PE |
| PE2 | late-onset PE |
| PI | pulsatility index |
| PPA | pulse pressure amplification |
| PP | pulse pressure |
| RWTT | reflected wave transit time |
| PWVao | aortic pulse wave velocity |
| SAD | systolic blood pressure |
| SDC 1 | syndecan-1 |
| SEVR | subendocardial viability ratio |
| UA | umbilical artery |
| UtA | uterine arteries |
References
- Sinkey, R.G.; Battarbee, A.N.; Bello, N.A.; Ives, C.W.; Oparil, S.; Tita, A.T.N. Prevention, Diagnosis, and Management of Hypertensive Disorders of Pregnancy: A Comparison of International Guidelines. Curr. Hypertens. Rep. 2020, 22, 66. [Google Scholar] [CrossRef]
- Khalil, A.; Garcia-Mandujano, R.; Maiz, N.; Elkhouli, M.; Nicolaides, K.H. Longitudinal changes in maternal hemodynamics in a population at risk for pre-eclampsia. Ultrasound Obstet. Gynecol. 2014, 44, 197–204. [Google Scholar] [CrossRef]
- Jerrard-Dunne, P.; Mahmud, A.; Feely, J. Ambulatory arterial stiffness index, pulse wave velocity and augmentation index-interchangeable or mutually exclusive measures? J. Hypertens. 2008, 26, 529–534. [Google Scholar] [CrossRef] [Green Version]
- Omboni, S.; Posokhov, I.N.; Kotovskaya, Y.N.; Protogerou, A.D.; Blacher, J. Twenty-Four-Hour Ambulatory Pulse Wave Analysis in Hypertension Management: Current Evidence and Perspectives. Curr. Hypertens. Rep. 2016, 18, 72. [Google Scholar] [CrossRef]
- Omboni, S.; Posokhov, I.N.; Rogoza, A.N. Evaluation of 24-Hour Arterial Stiffness Indices and Central Hemodynamics in Healthy Normotensive Subjects versus Treated or Untreated Hypertensive Patients: A Feasibility Study. Int. J. Hypertens. 2015, 2015, 601812. [Google Scholar] [CrossRef]
- Ziganshina, M.M.; Yarotskaya, E.L.; Bovin, N.V.; Sukhikh, G.T. Endothelial Dysfunction as a Consequence of Endothelial Glycocalyx Damage: A Role in the Pathogenesis of Preeclampsia. In Endothelial Dysfunction—Old Concepts and New Challengesin; Lenasi, H., Ed.; IntechOpen: London, UK, 2018; pp. 113–145. [Google Scholar]
- Weinbaum, S.; Cancel, L.M.; Fu, B.M.; Tarbell, J.M. The Glycocalyx and Its Role in Vascular Physiology and Vascular Related Diseases. Cardiovasc. Eng. Technol. 2021, 12, 37–71. [Google Scholar] [CrossRef]
- Dogné, S.; Flamion, B. Endothelial Glycocalyx Impairment in Disease: Focus on Hyaluronan Shedding. Am. J. Pathol. 2020, 190, 768–780. [Google Scholar] [CrossRef]
- Qu, J.; Cheng, Y.; Wu, W.; Yuan, L.; Liu, X. Glycocalyx Impairment in Vascular Disease: Focus on Inflammation. Front. Cell Dev. Biol. 2021, 9, 730621. [Google Scholar] [CrossRef]
- Tarbell, J.M.; Cancel, L.M. The glycocalyx and its significance in human medicine. J. Intern. Med. 2016, 280, 97–113. [Google Scholar] [CrossRef] [Green Version]
- Pillinger, N.L.; Kam, P. Endothelial glycocalyx: Basic science and clinical implications. Anaesth. Intensiv. Care 2017, 45, 295–307. [Google Scholar] [CrossRef]
- Neves, F.M.; Meneses, G.C.; Sousa, N.E.; Menezes, R.R.; Parahyba, M.C.; Martins, A.M.; Libório, A.B. Syndecan-1 in Acute Decompensated Heart Failure-Association with Renal Function and Mortality. Circ. J. 2015, 79, 1511–1519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bogner-Flatz, V.; Braunstein, M.; Ocker, L.E.; Kusmenkov, T.; Tschoep, J.; Ney, L.; Böcker, W.; Annecke, T. On-the-Scene Hyaluronan and Syndecan-1 Serum Concentrations and Outcome after Cardiac Arrest and Resuscitation. Mediat. Inflamm. 2019, 2019, 8071619. [Google Scholar] [CrossRef] [PubMed]
- Mitsuda, S.; Uzawa, K.; Sawa, M.; Ando, T.; Yoshikawa, T.; Miyao, H.; Yorozu, T.; Ushiyama, A. Vascular Endothelial Glycocalyx Plays a Role in the Obesity Paradox According to Intravital Observation. Front. Cardiovasc. Med. 2021, 8, 727888. [Google Scholar] [CrossRef] [PubMed]
- Weissgerber, T.L.; Garcia-Valencia, O.; Milic, N.M.; Codsi, E.; Cubro, H.; Nath, M.C.; White, W.M.; Nath, K.A.; Garovic, V.D. Early Onset Preeclampsia Is Associated with Glycocalyx Degradation and Reduced Microvascular Perfusion. J. Am. Heart Assoc. 2019, 8, e010647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kornacki, J.; Wirstlein, P.; Wender-Ozegowska, E. Markers of Endothelial Injury and Dysfunction in Early- and Late-Onset Preeclampsia. Life 2020, 10, 239. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, M.; Mayer, M.; Cancel, L.M.; Bartosch, A.M.; Mathews, R.; Tarbell, J.M. The glycocalyx core protein Glypican 1 protects vessel wall endothelial cells from stiffness-mediated dysfunction and disease. Cardiovasc. Res. 2021, 117, 1592–1605. [Google Scholar] [CrossRef]
- Brown, M.A.; Magee, L.A.; Kenny, L.C.; Karumanchi, S.A.; McCarthy, F.P.; Saito, S.; Hall, D.R.; Warren, C.E.; Adoyi, G.; Ishaku, S. The hypertensive disorders of pregnancy: ISSHP classification, diagnosis & management recommendations for international practice. Hypertension 2018, 72, 24–43. [Google Scholar] [CrossRef] [Green Version]
- Gordijn, S.J.; Beune, I.M.; Thilaganathan, B.; Papageorghiou, A.; Baschat, A.A.; Baker, P.N.; Silver, R.M.; Wynia, K.; Ganzevoort, W. Consensus definition of fetal growth restriction: A Delphi procedure. Ultrasound Obstet. Gynecol. 2016, 48, 333–339. [Google Scholar] [CrossRef]
- Dorogova, I.V.; Panina, E.S. Comparison of the BPLab® sphygmomanometer for ambulatory blood pressure monitoring with mercury sphygmomanometry in pregnant women: Validation study according to the British Hypertension Society protocol. Vasc. Health Risk Manag. 2015, 11, 245–249. [Google Scholar] [CrossRef]
- Ushiyama, A.; Kataoka, H.; Iijima, T. Glycocalyx and its involvement in clinical pathophysiologies. J. Intensiv. Care 2016, 4, 59. [Google Scholar] [CrossRef]
- Ikonomidis, I.; Voumvourakis, A.; Makavos, G.; Triantafyllidi, H.; Pavlidis, G.; Katogiannis, K.; Benas, D.; Vlastos, D.; Trivilou, P.; Varoudi, M.; et al. Association of impaired endothelial glycocalyx with arterial stiffness, coronary microcirculatory dysfunction, and abnormal myocardial deformation in untreated hypertensives. J. Clin. Hypertens. 2018, 20, 672–679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ling, H.Z.; Guy, H.Z.G.P.; Bisquera, A.; Poon, L.C.; Nicolaides, K.H.; Kametas, N.A. Maternal hemodynamics in screen-positive and screen-negative women of the ASPRE trial. Ultrasound Obstet. Gynecol. 2019, 54, 51–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrazzi, E.; Stampalija, T.; Monasta, L.; di Martino, D.; Vonck, S.; Gyselaers, W. Maternal hemodynamics: A method to classify hypertensive disorders of pregnancy. Am. J. Obstet. Gynecol. 2018, 218, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Valensise, H.; Vasapollo, B.; Gagliardi, G.; Novelli, G.P. Early and late preeclampsia: Two different maternal hemodynamic states in the latent phase of the disease. Hypertension 2008, 52, 873–880. [Google Scholar] [CrossRef] [Green Version]
- Melchiorre, K.; Sutherland, G.; Sharma, R.; Nanni, M.; Thilaganathan, B. Mid-gestational maternal cardiovascular profile in preterm and term pre-eclampsia: A prospective study. Int. J. Obstet. Gynaecol. 2013, 120, 496–504. [Google Scholar] [CrossRef]
- Valensise, H.; Vasapollo, B.; Novelli, G.P.; Giorgi, G.; Verallo, P.; Galante, A.; Arduini, D. Maternal and fetal hemodynamic effects induced by nitric oxide donors and plasma volume expansion in pregnancies with gestational hypertension complicated by intrauterine growth restriction with absent end-diastolic flow in the umbilical artery. Ultrasound Obstet. Gynecol. 2008, 31, 55–64. [Google Scholar] [CrossRef]
- Vasapollo, B.; Novelli, G.P.; Valensise, H. Total vascular resistance and left ventricular morphology as screening tools for complications in pregnancy. Hypertension 2008, 51, 1020–1026. [Google Scholar] [CrossRef] [Green Version]
- Ghossein-Doha, C.; Khalil, A.; Lees, C.C. Maternal hemodynamics: A 2017 update. Ultrasound Obstet. Gynecol. 2017, 49, 10–14. [Google Scholar] [CrossRef] [Green Version]
- Tay, J.; Foo, L.; Masini, G.; Bennett, P.R.; McEniery, C.M.; Wilkinson, I.B.; Lees, C.C. Early and late preeclampsia are characterized by high cardiac output, but in the presence of fetal growth restriction, cardiac output is low: Insights from a prospective study. Am. J. Obstet. Gynecol. 2018, 2018, 1–12. [Google Scholar] [CrossRef]
- Masini, G.; Foo, L.F.; Tay, J.; Wilkinson, I.B.; Valensise, H.; Gyselaers, W.; Lees, C.C. Preeclampsia has 2 phenotypes that require different treatment strategies. Am. J. Obstet. Gynecol. 2021, 226, S1006–S1018. [Google Scholar] [CrossRef]
- Hofmann-Kiefer, K.F.; Chappell, D.; Knabl, J.; Frank, H.G.; Martinoff, N.; Conzen, P.; Becker, B.F.; Rehm, M. Placental syncytiotrophoblast maintains a specific type of glycocalyx at the fetomaternal border: The glycocalyx at the fetomaternal interface in healthy women and patients with HELLP syndrome. Reprod. Sci. 2013, 20, 1237–1245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gandley, R.E.; Althouse, A.; Jeyabalan, A.; Bregand-White, J.M.; McGonigal, S.; Myerski, A.C.; Gallaher, M.; Powers, R.W.; Hubel, C.A. Low Soluble Syndecan-1 Precedes Preeclampsia. PLoS ONE 2016, 11, e0157608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofmann-Kiefer, K.F.; Knabl, J.; Martinoff, N.; Schiessl, B.; Conzen, P.; Rehm, M.; Becker, B.F.; Chappell, D. Increased serum concentrations of circulating glycocalyx components in HELLP syndrome compared to healthy pregnancy: An observational study. Reprod. Sci. 2013, 20, 318–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lahsinoui, H.H.; Amraoui, F.; Spijkers, L.J.A.; Veenboer, G.J.M.; Peters, S.L.M.; van Vlies, N.; Vogt, L.; Ris-Stalpers, C.; van den Born, B.J.N.; Afink, J.B. Soluble syndecan-1 and glycosaminoglycans in preeclamptic and normotensive pregnancies. Sci. Rep. 2021, 11, 4387. [Google Scholar] [CrossRef] [PubMed]
- Ziganshina, M.M.; Yarotskaya, E.L.; Bovin, N.V.; Pavlovich, S.V.; Sukhikh, G.T. Can Endothelial Glycocalyx Be a Major Morphological Substrate in Pre-Eclampsia? Int. J. Mol. Sci. 2020, 21, 3048. [Google Scholar] [CrossRef]
- Ziganshina, M.M.; Amiraslanov, E.Y.; Yarotskaya, E.L.; Dolgushina, N.V.; Sergunina, O.A.; Nikolaeva, M.A.; Kan, N.E.; Tyutyunnik, V.L.; Mantrova, D.A.; Loginova, N.S.; et al. Autoantibodies to endothelial cells in patients with hypertensive disorders during pregnancy. Pregnancy Hypertens. 2018, 12, 65–70. [Google Scholar] [CrossRef]
- Ziganshina, M.M.; Shilova, N.V.; Khasbiullina, N.R.; Bovin, N.V.; Sukhikh, G.T. Autoantibodies against endothelial antigens in preeclampsia. Akusherstvo Ginekol. 2016, 3, 24–31. [Google Scholar] [CrossRef]
- Gibbins, K.J.; Tebo, A.E.; Nielsen, S.K.; Branch, D.W. Antiphospholipid antibodies in women with severe preeclampsia and placental insufficiency: A case-control study. Lupus 2018, 27, 1903–1910. [Google Scholar] [CrossRef]
- Figueroa–Diesel, H.; Hernandez–Andrade, E.; Acosta–Rojas, R. Doppler changes in the main fetal brain arteries at different stages of hemodynamic adaptation in severe intrauterine growth restriction. Ultrasound Obstet. Gynecol. 2007, 30, 297–302. [Google Scholar] [CrossRef]
- Teng, Y.H.; Aquino, R.S.; Park, P.W. Molecular functions of syndecan-1 in disease. Matrix Biol. 2012, 31, 3–16. [Google Scholar] [CrossRef]
- Manon-Jensen, T.; Multhaupt, H.A.; Couchman, J.R. Mapping of matrix metalloproteinase cleavage sites on syndecan-1 and syndecan-4 ectodomains. FEBS J. 2013, 280, 2320–2331. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Tiemeier, G.L.; van den Berg, B.M.; Rabelink, T.J. Endothelial Glycocalyx Hyaluronan: Regulation and Role in Prevention of Diabetic Complications. Am. J. Pathol. 2020, 190, 781–790. [Google Scholar] [CrossRef] [PubMed]
- Ziganshina, M.M.; Pavlovich, S.V.; Bovin, N.V.; Sukhikh, G.T. Hyaluronic Acid in Vascular and Immune Homeostasis during Normal Pregnancy and Preeclampsia. Acta Nat. 2016, 8, 59–71. [Google Scholar] [CrossRef]
- Everett, T.R.; Mahendru, A.A.; McEniery, C.M.; Wilkinson, I.B.; Lees, C.C. Raised uterine artery impedance is associated with increased maternal arterial stiffness in the late second trimester. Placenta 2012, 33, 572–577. [Google Scholar] [CrossRef]
- Nichols, W.W.; O’Rourke, M.F.; Vlachopoulos, C. McDonald’s Blood Flow in Arteries: Theoretical, Experimental and Clinical Principles, 6th ed.; CRC Press: Boca Raton, FL, USA, 2010. [Google Scholar]
- Fullerton, G.; Crilly, M.A.; Bhattacharya, S.; Danielian, P.J. Measurement of aortic augmentation index in pregnant women with raised blood pressure and subsequent outcomes: A preliminary prospective cohort study. Hypertens. Pregnancy 2014, 33, 476–487. [Google Scholar] [CrossRef]
- Vlachopoulos, C.; Aznaouridis, K.; O’Rourke, M.F. Prediction of cardiovascular events and all-cause mortality with central haemodynamics: A systematic review and meta-analysis. Eur. Heart J. 2010, 31, 1865–1871. [Google Scholar] [CrossRef] [Green Version]
- Garg, P.; Jaryal, A.K.; Kachhawa, G.; Kriplani, A.; Deepak, K.K. Sequential profile of endothelial functions and arterial stiffness in preeclampsia during the course of pregnancy. Pregnancy Hypertens. 2019, 18, 88–95. [Google Scholar] [CrossRef]
- Khalil, A.; Akolekar, R.; Syngelaki, A.; Elkhouli, M.; Nicolaides, N. Maternal haemodynamics at 11-13 weeks of gestation and adverse pregnancy outcomes. Pregnancy Hypertens. 2012, 2, 223–224. [Google Scholar] [CrossRef]
- Perry, H.; Gutierrez, J.; Binder, J.; Thilaganathan, B.; Khalil, A. Maternal arterial stiffness in hypertensive pregnancies with and without small-for-gestational-age neonate. Ultrasound Obstet. Gynecol. 2020, 56, 44–50. [Google Scholar] [CrossRef]
- Bauer, A.; Hametner, B.; Weber, T.; Wassertheurer, S. Method Comparison and Validation of the Determination of Ejection Duration from Oscillometric Measurements. IFAC-PapersOnLine 2018, 51, 343–348. [Google Scholar] [CrossRef]
- Scandale, G.; Dimitrov, G.; Recchia, M.; Carzaniga, G.; Minola, M.; Perilli, E.; Carotta, M.; Catalano, M. Arterial stiffness and subendocardial viability ratio in patients with peripheral arterial disease. J. Clin. Hypertens. 2018, 20, 478–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voyvodic, P.L.; Min, D.; Liu, R.; Williams, E.; Chitalia, V.; Dunn, A.K.; Baker, A.B. Loss of syndecan-1 induces a pro-inflammatory phenotype in endothelial cells with a dysregulated response to atheroprotective flow. J. Biol. Chem. 2014, 289, 9547–9559. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Geng, X.; Jin, S.; Xu, J.; Guo, M.; Shen, D.; Ding, X.; Liu, H.; Xu, X. The Association of Syndecan-1, Hypercoagulable State and Thrombosis and in Patients with Nephrotic Syndrome. Clin. Appl. Thromb. Hemost. 2021, 27, 10760296211010256. [Google Scholar] [CrossRef] [PubMed]
- Le, V.; Mei, L.; Voyvodic, P.L.; Zhao, C.; Busch, D.J.; Stachowiak, J.C.; Baker, A.B. Molecular tension in syndecan-1 is regulated by extracellular mechanical cues and fluidic shear stress. Biomaterials 2021, 275, 120947. [Google Scholar] [CrossRef] [PubMed]
- Erkayıran, U.; To, A.; Karaküçük, S.; Seyithanoğlu, M.; Arslanca, T. Evaluation of serum perlecan levels in pregnancy with mild and severe preeclampsia. J. Health Sci. Med. 2021, 4, 538–542. [Google Scholar] [CrossRef]
- Unfer, V.; Tilotta, M.; Kaya, C.; Noventa, M.; Török, P.; Alkatout, I.; Gitas, G.; Bilotta, G.; Laganà, A.S. Absorption, distribution, metabolism and excretion of hyaluronic acid during pregnancy: A matter of molecular weight. Expert Opin. Drug Metab. Toxicol. 2021, 17, 823–840. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Group | p-Values | |||||
|---|---|---|---|---|---|---|
| Variable | NP1 | PE1 | NP2 | PE2 | NP1 vs. PE1 | NP2 vs. PE2 |
| n | 19 | 20 | 21 | 20 | ||
| Maternal age, y a | 33.28 ± 1.21 | 33.60 ± 1.32 | 34.29 ± 1.08 | 34.75 ± 1.13 | 0.8589 | 0.7680 |
| GA at blood sampling, wk a | 29.95 ± 0.64 | 30.28 ± 0.53 | 36.61 ± 0.52 | 37.03 ± 0.33 | 0.6927 | 0.5002 |
| Nulliparous b | 11 (61%) | 4 (20%) | 7 (33%) | 11 (55%) | 0.0129 | 0.1775 |
| BMI, kg/m2 c | 24.8 (23.0–26.34) | 25.20 (23.92–30.88) | 26.89 (23.18–28.74) | 28.12 (26.45–31.63) | 0.3648 | 0.0217 |
| Pre-existing hypertension, n (%) b | 0 | 9 (45%) | 0 | 7 (35%) * | 0.0021 | 0.0054 |
| PE with FGR, n (%) b | 0 | 6 (30%) | 0 | 4 (20%) ** | <0.0001 | <0.0001 |
| Haemoglobin, g% c | 120.0 (115.0–124.5) | 108.5 (104.5–119.5) | 119.0 (112.5–123.5) | 121.0 (114.5–125.5) | 0.0075 | 0.3322 |
| Thrombocytes (109/L) c | 227.50 (207.5–300.0) | 176.5 (142.5–220.5) | 232.0 (182.5–262.0) | 210.5 (178.5–259.0) | 0.0177 | 0.7149 |
| Birth weight, g c | 3040.0 (2867.5–3348.8) | 1313.5 (875.0–1682.0) | 3265.0 (3060.0–3528.0) | 2479.5 (2120.0–3363.0) | <0.0001 | 0.0124 |
| Newborns’ Apgar scores (1 min) c | 8 (8–8) | 7 (6–7) | 8 (8–8) | 8 (7.5–8.0) | 0.0002 | 0.3391 |
| Newborns’ Apgar scores (5 min) c | 9 (8.25–9) | 8 (7–8) | 9 (8.75–9) | 9 (8–9) | 0.0003 | 0.3082 |
| Group | p-Values | |||||
|---|---|---|---|---|---|---|
| Variable | NP1 | PE1 | NP2 | PE2 | NP1 vs. PE1 | NP2 vs. PE2 |
| n | 19 | 20 | 21 | 20 | ||
| UtA-PI | 0.66 0.76 0.87 | 1.20 1.41 1.66 | 0.66 0.75 0.86 | 0.77 0.88 1.15 | <0.0001 | 0.0448 |
| UmA-PT | 0.77 0.86 0.92 | 0.97 1.03 1.54 | 0.72 0.88 1.00 | 0.74 0.84 0.94 | 0.0004 | 0.8360 |
| CPR | 1.84 2.14 2.39 | 0.85 1.64 1.90 | 1.73 1.97 2.07 | 1.60 1.82 2.16 | 0.0037 | 0.6217 |
| MCA-PI | 1.78 1.88 2.20 | 1.28 1.62 2.01 | 1.30 1.60 1.95 | 1.35 1.51 1.68 | 0.0836 | 0.8242 |
| Hemodynamic Parameters * | NP1, n = 19 | PE1, n = 20 | p-Value |
|---|---|---|---|
| AASI | 0.315 0.396 0.520 | 0.384 0.317 0.504 | 0.8440 |
| AIx, % | −70.5 −62.0 −50.8 | −57.0 −47.0 −33.5 | 0.0243 |
| (dP/dt)max, mm Hg/sec | 295.6 342.0 371.5 | 456.0 560.5 675.5 | <0.0001 |
| ED, ms | 257.3 292.0 311.5 | 247.6 293.0 304.0 | 0.9775 |
| PPA, % | 108.3 123.0 155.5 | 113.3 123.0 137.0 | 0.9439 |
| PWVao, m/sec | 5.8 6.1 6.8 | 6.0 6.8 7.2 | 0.1854 |
| RWTT, m/sec | 105.0 123.0 131.5 | 121.5 128.5 134.0 | 0.1176 |
| SEVR, % | 78.8 96.0 115.8 | 84.5 101.5 163.0 | 0.3609 |
| Max DADao, mm Hg | 80.3 82.0 84.8 | 103.0 106.0 109.0 | <0.0001 |
| Max SADao mm Hg | 127.3 129.0 131.0 | 153.5 162.0 172.0 | <0.0001 |
| Min DADao, mm Hg | 61.3 64.0 69.5 | 74.0 76.0 79.0 | <0.0001 |
| Min SADao, mm Hg | 98.8 103.0 108.8 | 111.5 116.5 120.5 | <0.0001 |
| Med DADao, mm Hg | 72.3 78.0 78.8 | 93.0 94.5 100.0 | <0.0001 |
| Med SADao, mm Hg | 112.0 117.0 119.8 | 138.0 143.0 147.5 | <0.0001 |
| Circadian rhythm | 1.0 1.0 1.0 | 1.0 2.0 2.0 | <0.0001 |
| Hemodynamic Parameters * | NP2, n = 21 | PE2, n = 20 | p-Value |
|---|---|---|---|
| AASI | 0.263 0.412 0.592 | 0.452 0.562 0.651 | 0.0621 |
| AIx, % | −71.0 −56.0 −32.3 | −52.5 −38.0 −23.0 | 0.0518 |
| (dP/dt)max, mm Hg/sec | 266.8 370.0 456.0 | 340.0 434.0 544.5 | 0.0446 |
| ED, ms | 241.0 281.0 293.0 | 283.5 346.0 361.5 | 0.0015 |
| PPA, % | 110.8 119.0 137.0 | 121.0 127.5 142.0 | 0.1174 |
| PWVao, m/sec | 5.9 6.9 7.2 | 6.6 7.2 8.8 | 0.1065 |
| RWTT, m/sec | 109.0 127.0 134.5 | 111.0 118.5 130.0 | 0.2299 |
| SEVR, % | 72.0 102.0 133.0 | 115.5 129.5 152.5 | 0.0224 |
| Max DADao, mm Hg | 79.0 81.0 86.3 | 100.5 105.5 110.0 | <0.0001 |
| Max SADao mm Hg | 127.0 129.0 134.0 | 151.0 161.5 170.0 | <0.0001 |
| Min DADao, mm Hg | 64.8 69.0 69.0 | 77.5 79.5 83.0 | <0.0001 |
| Min SADao, mm Hg | 103.0 105.0 108.3 | 112.0 119.0 123.0 | <0.0001 |
| Med DADao, mm Hg | 72.8 75.0 81.0 | 90.0 93.5 102.0 | <0.0001 |
| Med SADao, mm Hg | 115.5 119.0 121.0 | 133.0 140.5 147.0 | <0.0001 |
| Circadian rhythm | 1.0 1.0 1.0 | 1.0 2.0 2.0 | <0.0001 |
| Proteoglycans | Hemodynamic Parameters | |||||
|---|---|---|---|---|---|---|
| max DAD | max SAD | min DAD | min SAD | med DAD | med SAD | |
| Group NP1 | ||||||
| SDC-1 | 0.720; p = 0.0005 | N.S. | 0.641; p = 0.0031 | 0.621; p = 0.0046 | 0.706; p = 0.0007 | 0.601; p = 0.0065 |
| HSPG2 | N.S. | N.S. | −0.467; p = 0.0438 | N.S. | N.S. | N.S. |
| HA | N.S. | N.S. | N.S. | N.S. | N.S. | N.S. |
| Early-onset PE | ||||||
| SDC-1 | N.S. | N.S. | N.S. | N.S. | N.S. | N.S. |
| HSPG2 | −0.607; p = 0.0035 | N.S. | N.S. | N.S. | −0.552; p = 0.0094 | N.S. |
| HA | N.S. | N.S. | N.S. | N.S. | N.S. | N.S. |
| Group NP2 | ||||||
| SDC-1 | N.S. | N.S. | N.S. | N.S. | N.S. | N.S. |
| HSPG2 | −0.454; p = 0.0441 | N.S. | N.S. | N.S. | N.S. | N.S. |
| HA | 0.446; p = 0.0488 | N.S. | N.S. | N.S. | 0.459; p = 0.0416 | N.S. |
| Late-onset PE | ||||||
| SDC-1 | −0.522; p = 0.0181 | −0.553; p = 0.0155 | −0.632; p = 0.0028 | −0.603; p = 0.0049 | N.S. | −0.562; p = 0.0099 |
| HSPG2 | N.S. | N.S. | N.S. | N.S. | N.S. | N.S. |
| HA | N.S. | N.S. | N.S. | N.S. | N.S. | N.S. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ziganshina, M.M.; Muminova, K.T.; Khasbiullina, N.R.; Khodzhaeva, Z.S.; Yarotskaya, E.L.; Sukhikh, G.T. Characterization of Vascular Patterns Associated with Endothelial Glycocalyx Damage in Early- and Late-Onset Preeclampsia. Biomedicines 2022, 10, 2790. https://doi.org/10.3390/biomedicines10112790
Ziganshina MM, Muminova KT, Khasbiullina NR, Khodzhaeva ZS, Yarotskaya EL, Sukhikh GT. Characterization of Vascular Patterns Associated with Endothelial Glycocalyx Damage in Early- and Late-Onset Preeclampsia. Biomedicines. 2022; 10(11):2790. https://doi.org/10.3390/biomedicines10112790
Chicago/Turabian StyleZiganshina, Marina M., Kamilla T. Muminova, Nailia R. Khasbiullina, Zulfiya S. Khodzhaeva, Ekaterina L. Yarotskaya, and Gennady T. Sukhikh. 2022. "Characterization of Vascular Patterns Associated with Endothelial Glycocalyx Damage in Early- and Late-Onset Preeclampsia" Biomedicines 10, no. 11: 2790. https://doi.org/10.3390/biomedicines10112790