

Odontogenic Chronic Rhinosinusitis: Structured Histopathology Evidence in Different Patho-Physiological Mechanisms
 , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Treatment
2.2.1. Transoral Approach
2.2.2. Transnasal Endoscopic Approach
2.3. Histopathological Investigations
2.4. Statistical Analysis
3. Results
Structured Histopathology and oCRS Sub-Cohorts Stratified on Etiological Basis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bauer, W.H. Maxillary sinusitis of dental origin. Am. J. Orthod Dentofacial Orthop. 1943, 29, 133–151. [Google Scholar] [CrossRef]
- Aukštakalnis, R.; Simonavičiūtė, R.; Simuntis, R. Treatment options for odontogenic maxillary sinusitis: A review. Stomatologija. 2018, 20, 22–26. [Google Scholar] [PubMed]
- Brescia, G.; Saia, G.; Apolloni, F.; Marioni, G. A novel nasal endoscopic approach for removing displaced dental implants from the maxillary sinus. Am. J. Otolaryngol. 2017, 38, 92–95. [Google Scholar] [CrossRef] [PubMed]
- Brescia, G.; Fusetti, S.; Apolloni, F.; Marioni, G.; Saia, G. Displaced dental materials in the maxillary sinus: An original series. Analysis and definition of a surgical decision-making process. Ann. Otol. Rhinol. Laryngol. 2019, 128, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Workman, A.D.; Granquist, E.J.; Adappa, N.D. Odontogenic sinusitis: Developments in diagnosis, microbiology, and treatment. Curr. Opin. Otolaryngol. Head Neck Surg. 2018, 26, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Little, R.E.; Long, C.M.; Loehrl, T.A.; Poetker, D.M. Odontogenic sinusitis: A review of the current literature. Laryngoscope Investig. Otolaryngol. 2018, 3, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Raman, A.; Papagiannopoulos, P.; Kuhar, H.N.; Gattuso, P.; Batra, P.S.; Tajudeen, B.A. Histopathologic features of chronic sinusitis precipitated by odontogenic infection. Am. J. Rhinol. Allergy 2019, 33, 113–120. [Google Scholar] [CrossRef]
- Menditti, D.; Laino, L.; Di Domenico, M.; Troiano, G.; Guglielmotti, M.; Sava, S.; Mezzogiorno, A.; Baldi, A. Cysts and pseudocysts of the oral cavity: Revision of the literature and a new proposed classification. In Vivo 2018, 32, 999–1007. [Google Scholar] [CrossRef] [Green Version]
- Goyal, V.K.; Ahmad, A.; Turfe, Z.; Peterson, E.I.; Craig, J.R. Predicting odontogenic sinusitis in unilateral sinus disease: A prospective, multivariate analysis. Am. J. Rhinol. Allergy. 2021, 35, 164–171. [Google Scholar] [CrossRef]
- Brook, I. Sinusitis of odontogenic origin. Otolaryngol. Head Neck Surg. 2006, 135, 349–355. [Google Scholar] [CrossRef]
- Eggmann, F.; Connert, T.; Bühler, J.; Dagassan-Berndt, D.; Weiger, R.; Walter, C. Do periapical and periodontal pathologies affect Schneiderian membrane appearance? Systematic review of studies using cone-beam computed tomography. Clin. Oral Investig. 2017, 21, 1611–1630. [Google Scholar] [CrossRef] [PubMed]
- Vidal, F.; Coutinho, T.M.; Carvalho Ferreira, D.; Souza, R.C.; Gonçalves, L.S. Odontogenic sinusitis: A comprehensive review. Acta Odontol. Scand. 2017, 75, 623–633. [Google Scholar] [CrossRef] [PubMed]
- Snidvongs, K.; Lam, M.; Sacks, R.; Earls, P.; Kalish, L.; Phillips, P.S.; Pratt, E.; Harvey, R.J. Structured histopathology profiling of chronic rhinosinusitis in routine practice. Int. Forum Allergy Rhinol. 2012, 2, 376–385. [Google Scholar] [CrossRef] [PubMed]
- Kuhar, H.N.; Tajudeen, B.A.; Mahdavinia, M.; Gattuso, P.; Ghai, R.; Batra, P.S. Inflammatory infiltrate and mucosal remodeling in chronic rhinosinusitis with and without polyps: Structured histopathologic analysis. Int. Forum Allergy Rhinol. 2017, 7, 679–689. [Google Scholar] [CrossRef] [PubMed]
- Brescia, G.; Alessandrini, L.; Giacomelli, L.; Parrino, D.; Zanotti, C.; Tealdo, G.; Franz, L.; Carraro, V.; Barion, U.; Marioni, G. A classification of chronic rhinosinusitis with nasal polyps based on structured histopathology. Histopathology 2020, 76, 296–307. [Google Scholar] [CrossRef]
- Brescia, G.; Alessandrini, L.; Marioni, G. Structured histopathology for endotyping and planning rational treatment in chronic rhinosinusitis. Am. J. Otolaryngol. 2021, 42, 102795. [Google Scholar] [CrossRef]
- Lund, V.J.; Mackay, I.S. Staging in rhinosinusitus. Rhinology 1993, 31, 183–184. [Google Scholar]
- Manani, G.; Bacci, C.; Zanette, G.; Facco, E. Stato attuale della sedazione cosciente in odontoiatria/Contemporary state of sedation in dentistry. Dent. Cadmos 2012, 80, 357–369. [Google Scholar] [CrossRef]
- Nakayama, T.; Asaka, D.; Okushi, T.; Yoshikawa, M.; Moriyama, H.; Otori, N. Endoscopic medial maxillectomy with preservation of inferior turbinate and nasolacrimal duct. Am. J. Rhinol. Allergy 2012, 26, 405–408. [Google Scholar] [CrossRef]
- Omura, K.; Asaka, D.; Nayak, J.V.; Tanaka, Y. Transseptal access with crossing multiple incisions for improved pedicle control and septum preservation: “How I do it”. Am. J. Rhinol. Allergy 2017, 31, 139–141. [Google Scholar] [CrossRef]
- Omura, K.; Nomura, K.; Aoki, S.; Otori, N.; Tanaka, Y. Direct approach to the anterior and lateral part of the maxillary sinus with an endoscope. Auris Nasus Larynx 2019, 46, 871–875. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.L.; Xiong, P.; Zhang, L.; Cao, P.P.; Liao, B.; Lu, X.; Cui, Y.H.; Liu, Z. Features of airway remodeling in different types of Chinese chronic rhinosinusitis are associated with inflammation patterns. Allergy 2013, 68, 101–109. [Google Scholar] [CrossRef]
- Brescia, G.; Alessandrini, L.; Frasconi, S.; Contro, G.; Frigo, A.C.; Marioni, G. Structured histopathology and laboratory evidence in nasal polyposis with different pathogenesis. Am. J. Otolaryngol. 2022, 44, 103649. [Google Scholar] [CrossRef]
- Lee, K.; Tai, J.; Lee, S.H.; Kim, T.H. Advances in the knowledge of the underlying airway remodeling mechanisms in chronic rhinosinusitis based on the endotypes: A review. Int. J. Mol. Sci. 2021, 22, 910. [Google Scholar] [CrossRef] [PubMed]
- Contro, G.; Brescia, G.; Alessandrini, L.; Barion, U.; Padoan, R.; Frigo, A.C.; Schiavon, F.; Marioni, G. Neutrophil infiltrates and eosinophil aggregates in chronic rhinosinusitis with nasal polyps and EGPA. Clin. Rheumatol. 2021, 40, 1949–1957. [Google Scholar] [CrossRef]
- Lombardi, C.; Berti, A.; Cottini, M. The emerging roles of eosinophils: Implications for the targeted treatment of eosinophilic-associated inflammatory conditions. Curr. Res. Immunol. 2022, 3, 42–53. [Google Scholar] [CrossRef] [PubMed]
- Brescia, G.; Alessandrini, L.; Parrino, D.; Franz, L.; Barion, U.; Marioni, G. Emerging contribution of histopathology to our understanding of chronic rhinosinusitis endotypes: Tissue eosinophil count and aggregates. Am. J. Rhinol. Allergy 2020, 34, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, G.A.; Yacoub, M.R.; Ripa, M.; Mannina, D.; Cariddi, A.; Saporiti, N.; Ciceri, F.; Castagna, A.; Colombo, G.; Dagna, L. Eosinophils from physiology to disease: A comprehensive review. Biomed. Res. Int. 2018, 2018. [Google Scholar] [CrossRef] [Green Version]
- Zitzmann, N.U.; Berglundh, T.; Marinello, C.P.; Lindhe, J. Experimental peri-implant mucositis in man. J. Clin. Periodontol. 2001, 28, 517–523. [Google Scholar] [CrossRef]
- Shafizadeh, M.; Amid, R.; Mahmoum, M.; Kadkhodazadeh, M. Histopathological characterization of peri-implant diseases: A systematic review and meta-analysis. Arch. Oral Biol. 2021, 132, 105288. [Google Scholar] [CrossRef]
- Gualini, F.; Berglundh, T. Immunohistochemical characteristics of inflammatory lesions at implants. J. Clin. Periodontol. 2003, 30, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Obădan, F.; Crăiţoiu, Ş.; Manolea, H.O.; Hîncu, M.C.; Iacov-Crăiţoiu, M.M. The evaluation of the morphological evolution of the tissue integration of dental implants through conventional histology and immunohistochemistry techniques. Rom. J. Morphol. Embryol. 2018, 59, 851–859. [Google Scholar] [PubMed]
- Noskovicova, N.; Hinz, B.; Pakshir, P. Implant fibrosis and the underappreciated role of myofibroblasts in the foreign body reaction. Cells 2021, 10, 1794. [Google Scholar] [CrossRef] [PubMed]
- Mynatt, R.G.; Do, J.; Janney, C.; Sindwani, R. Squamous metaplasia and chronic rhinosinusitis: A clinicopathological study. Am. J. Rhinol. 2008, 22, 602–605. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Main Features | No. of Cases (%) |
|---|---|
| Sex | |
| Male | 24 (57.1) |
| Female | 18 (42.9) |
| Allergy/Asthma | |
| None | 35 (83.3) |
| Allergy | 2 (4.8) |
| Asthma | 2 (4.8) |
| Allergy and asthma | 3 (7.1) |
| Sinonasal polyps’ phenotype | |
| No | 21 (50.0) |
| Yes | 21 (50.0) |
| Total (42 Cases) | Radicular Cyst (11 Cases) | Dental Implants (9 Cases) | Other Tooth Diseases (22 Cases) | p-Value | |
|---|---|---|---|---|---|
| oCRS with nasal polyps | 21 (50.0) | 4 (36.4) | 6 (66.7) | 11 (50.0) | 0.4375 |
| oCRS without nasal polyps | 21 (50.0) | 7 (63.6) | 3 (33.3) | 11 (50.0) | |
| Unilateral polyposis | 19 (90.5) | 4 (100.0) | 5 (83.3) | 10 (90.9) | |
| Bilateral polyposis | 2 (9.5) | 0 (0.0) | 1 (16.7) | 1 (9.1) | |
| CT score | |||||
| Mean (SD) | 4.7 (3.4) | 4.5 (2.6) | 5.8 (1.9) | 4.1 (4.2) | 0.3423 |
| Median (Range) | 4.0 (1.0–12.0) | 5.0 (1.0–7.0) | 5.5 (4.0–9.0) | 2.0 (1.0–12.0) |
| No. of Cases (%) | Radicular Cyst (1) No. of Cases = 11 | Dental Implant (2) No. of Cases = 9 | Other Tooth Diseases (3) No. of Cases = 22 | Overall p-Value | Difference (95% CI) 2 vs. 1 | Difference (95% CI) 3 vs. 1 | Difference (95% CI) 2 vs. 3 | |
|---|---|---|---|---|---|---|---|---|
| Degree of inflammation | ||||||||
| 0 or 1 | 10 (23.8) | 3 (27.3) | 1 (11.1) | 6 (27.3) | 0.7106 | |||
| 2 or 3 | 32 (76.2) | 8 (72.7) | 8 (88.9) | 16 (72.7) | 16.2 (−25.1; 52.3) | 0.0 (−30.7; 36.3) | 16.2 (−22.8; 43. 2) | |
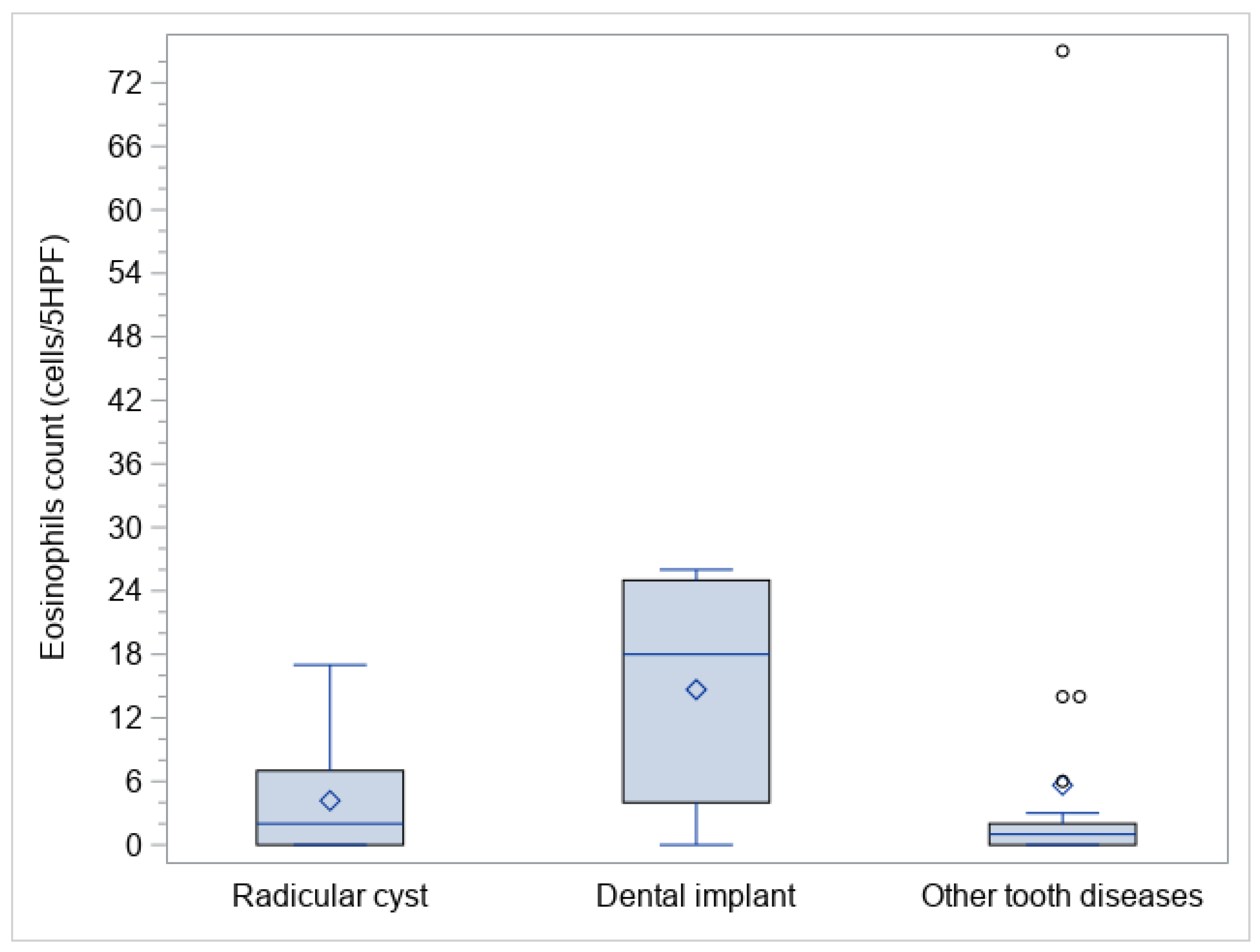
| Eosinophils count (cells/5HPF) | ||||||||
| Mean (SD) | 7.2 (13.3) | 4.2 (5.3) | 14.7 (10.7) | 5.6 (16.0) | 0.0118 | |||
| Median (Range) | 2.0 (0.0–75.0) | 2.0 (0.0–17.0) | 18.0 (0.0–26.0) | 1.0 (0.0–75.0) | 10 (0; 22) | 0 (−4; 1) | 11 (2; 22) | |
| Eosinophil aggregates | ||||||||
| No | 41 (97.6) | 11 (100.0) | 9 (100.0) | 21 (95.5) | 1.0000 | |||
| Yes | 1 (2.4) | 0 (0.0) | 0 (0.0) | 1 (4.5) | - | 4.5 (−24.5; 23.3) | −4.5 (−23.2; 30.0) | |
| Neutrophil infiltrate | ||||||||
| No | 16 (38.1) | 5 (45.5) | 2 (22.2) | 9 (40.9) | 0.5873 | |||
| Yes | 26 (61.9) | 6 (54.5) | 7 (77.8) | 13 (59.1) | 23.3 (−21.3; 62.6) | 4.6 (−31.1; 40.6) | 18.7 (−21.5; 49.1) | |
| Basal membrane thickening | ||||||||
| 0 or 1 | 37 (88.1) | 8 (72.7) | 9 (100.0) | 20 (90.9) | 0.1909 | |||
| 2 or 3 | 5 (11.9) | 3 (27.3) | 0 (0.0) | 2 (9.1) | −27.3 (−61.0; 9.9) | −18.2 (−51.8; 9.9) | −9.1 (−30.0; 25.5) | |
| Subepithelial edema | ||||||||
| 0 or 1 | 36 (85.7) | 8 (72.7) | 6 (66.7) | 22 (100.0) | 0.0099 | |||
| 2 or 3 | 6 (14.3) | 3 (27.3) | 3 (33.3) | 0 (0.0) | 6.1 (−32.2; 48.3) | −27.3 (−61.0; −4.1) | 33.3 (6.5; 70.1) | |
| Hyperplastic—papillary changes | ||||||||
| No | 33 (78.6) | 9 (81.8) | 6 (66.7) | 18 (81.8) | 0.6151 | |||
| Yes | 9 (21.4) | 2 (18.2) | 3 (33.3) | 4 (18.2) | 15.1 (−25.7; 54.8) | 0.0 (−33.7; 27.3) | 15.1 (−17.6; 52.0) | |
| Mucosal ulceration | ||||||||
| No | 32 (76.2) | 6 (54.5) | 7 (77.8) | 19 (86.4) | 0.1327 | |||
| Yes | 10 (23.8) | 5 (45.5) | 2 (22.2) | 3 (13.6) | −23.2 (−62.6; 21.3) | −31.8 (−64.5; 1.8) | 8.6 (−20.2; 47.4) | |
| Squamous metaplasia | ||||||||
| No | 30 (71.4) | 5 (45.5) | 9 (100.0) | 16 (72.7) | 0.0258 | |||
| Yes | 12 (28.6) | 6 (54.5) | 0 (0.0) | 6 (27.3) | −54.5 (−83.3; −14.9) | −27.3 (−61.0; 11.1) | −27.3 (−50.5; 9.3) | |
| Fibrosis | ||||||||
| No | 22 (52.4) | 4 (36.4) | 8 (88.9) | 10 (45.5) | 0.0408 | |||
| Yes | 20 (47.6) | 7 (63.6) | 1 (11.1) | 12 (54.5) | −52.5 (−82.7; −8.1) | −9.1 (−42.6; 28.7) | −43.4 (−70.1; 2.1) | |
| Fungal elements | ||||||||
| No | 39 (92.9) | 10 (90.9) | 9 (100.0) | 20 (90.9) | 1.0000 | |||
| Yes | 3 (7.1) | 1 (9.1) | 0 (0.0) | 2 (9.1) | −9.1 (−41.3; 25.2) | 0.0 (−32.9; 22.9) | −9.1 (−30.0; 25.5) | |
| Charcot–Leyden crystals | ||||||||
| No | 42 (100.0) | 11 (100.0) | 9 (100.0) | 22 (100.0) | - | |||
| Yes | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||||
| Globet cells hyperplasia | ||||||||
| 0 or 1 | 30 (71.4) | 7 (63.6) | 5 (55.6) | 18 (81.8) | 0.2875 | |||
| 2 or 3 | 12 (28.6) | 4 (36.4) | 4 (44.4) | 4 (18.2) | 8.1 (−38.0; 50.2) | −18.2 (−53.1; 13.6) | 26.2 (−9.6; 61.9) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brescia, G.; Alessandrini, L.; Bacci, C.; Bissolotti, G.; Fedrigo, M.; Contro, G.; Frasconi, S.; Boccuto, M.G.; Calcavecchia, A.; Frigo, A.C.; et al. Odontogenic Chronic Rhinosinusitis: Structured Histopathology Evidence in Different Patho-Physiological Mechanisms. Biomedicines 2022, 10, 2768. https://doi.org/10.3390/biomedicines10112768
Brescia G, Alessandrini L, Bacci C, Bissolotti G, Fedrigo M, Contro G, Frasconi S, Boccuto MG, Calcavecchia A, Frigo AC, et al. Odontogenic Chronic Rhinosinusitis: Structured Histopathology Evidence in Different Patho-Physiological Mechanisms. Biomedicines. 2022; 10(11):2768. https://doi.org/10.3390/biomedicines10112768
Chicago/Turabian StyleBrescia, Giuseppe, Lara Alessandrini, Christian Bacci, Guido Bissolotti, Marny Fedrigo, Giacomo Contro, Samuele Frasconi, Maria Grazia Boccuto, Arianna Calcavecchia, Anna Chiara Frigo, and et al. 2022. "Odontogenic Chronic Rhinosinusitis: Structured Histopathology Evidence in Different Patho-Physiological Mechanisms" Biomedicines 10, no. 11: 2768. https://doi.org/10.3390/biomedicines10112768