
Hidradenitis Suppurativa in Patients with HIV: A Scoping Review
 , , ,
, , ,
Abstract
:1. Introduction
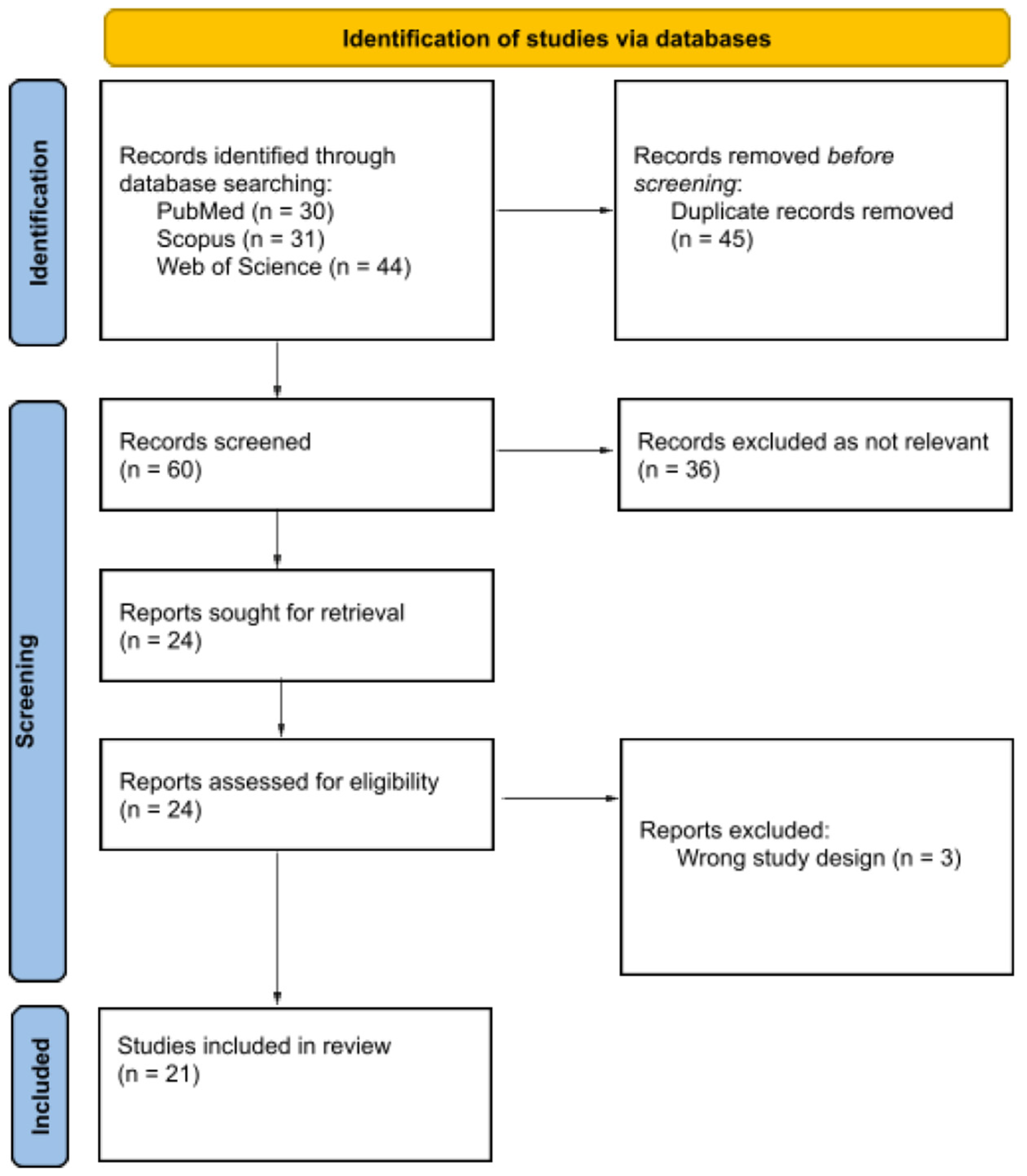
2. Materials and Methods
3. Results
4. Discussion
4.1. Epidemiology
4.2. Pathogenesis
4.3. Clinical Manifestations
4.4. Histopathology
4.5. Therapy
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li Pomi, F.; Macca, L.; Motolese, A.; Ingrasciotta, Y.; Berretta, M.; Guarneri, C. Neoplastic Implications in Patients Suffering from Hidradenitis Suppurativa under Systemic Treatments. Biomedicines 2021, 9, 1594. [Google Scholar] [CrossRef] [PubMed]
- Elkin, K.; Daveluy, S.; Avanaki, K. (Mohammad) Hidradenitis Suppurativa: Current Understanding, Diagnostic and Surgical Challenges, and Developments in Ultrasound Application. Ski. Res. Technol. 2020, 26, 11–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campanati, A.; Orciani, M.; Sorgentoni, G.; Consales, V.; Offidani, A.; di Primio, R. Pathogenetic Characteristics of Mesenchymal Stem Cells in Hidradenitis Suppurativa. JAMA Dermatol. 2018, 154, 1184. [Google Scholar] [CrossRef] [PubMed]
- Goldburg, S.R.; Strober, B.E.; Payette, M.J. Hidradenitis Suppurativa. J. Am. Acad. Dermatol. 2020, 82, 1045–1058. [Google Scholar] [CrossRef] [PubMed]
- Zouboulis, C.C.; Benhadou, F.; Byrd, A.S.; Chandran, N.S.; Giamarellos-Bourboulis, E.J.; Fabbrocini, G.; Frew, J.W.; Fujita, H.; González-López, M.A.; Guillem, P.; et al. What Causes Hidradenitis Suppurativa ?—15 Years After. Exp. Dermatol. 2020, 29, 1154–1170. [Google Scholar] [CrossRef]
- Rankin, B.D.; Haber, R.M. Case Report of Hidradenitis Suppurativa Localized to the Face in an HIV Patient. SAGE Open Med. Case Rep. 2021, 9, 2050313X2110579. [Google Scholar] [CrossRef]
- Gomez, J.; Barnes, L.A.; Yost, J.M.; Gordon, J.; Ginsberg, B.A.; Aleshin, M. Hidradenitis Suppurativa in Sexual and Gender Minorities: A Review and Considerations for Providers. J. Am. Acad. Dermatol 2022, in press. [CrossRef]
- Keele, B.F.; van Heuverswyn, F.; Li, Y.; Bailes, E.; Takehisa, J.; Santiago, M.L.; Bibollet-Ruche, F.; Chen, Y.; Wain, L.V.; Liegeois, F.; et al. Chimpanzee Reservoirs of Pandemic and Nonpandemic HIV-1. Science 2006, 313, 523–526. [Google Scholar] [CrossRef] [Green Version]
- Eggena, M.P.; Barugahare, B.; Jones, N.; Okello, M.; Mutalya, S.; Kityo, C.; Mugyenyi, P.; Cao, H. Depletion of Regulatory T Cells in HIV Infection Is Associated with Immune Activation. J. Immunol. 2005, 174, 4407–4414. [Google Scholar] [CrossRef] [Green Version]
- Epstein, H.; Morris, M. Concurrent Partnerships and HIV: An Inconvenient Truth. J. Int. AIDS Soc. 2011, 14, 13. [Google Scholar] [CrossRef]
- Hughes, J.P.; Baeten, J.M.; Lingappa, J.R.; Magaret, A.S.; Wald, A.; de Bruyn, G.; Kiarie, J.; Inambao, M.; Kilembe, W.; Farquhar, C.; et al. Determinants of Per-Coital-Act HIV-1 Infectivity Among African HIV-1–Serodiscordant Couples. J. Infect. Dis. 2012, 205, 358–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanser, F.; Bärnighausen, T.; Hund, L.; Garnett, G.P.; McGrath, N.; Newell, M.-L. Effect of Concurrent Sexual Partnerships on Rate of New HIV Infections in a High-Prevalence, Rural South African Population: A Cohort Study. Lancet 2011, 378, 247–255. [Google Scholar] [CrossRef] [Green Version]
- Polis, C.B.; Curtis, K.M. Use of Hormonal Contraceptives and HIV Acquisition in Women: A Systematic Review of the Epidemiological Evidence. Lancet Infect. Dis. 2013, 13, 797–808. [Google Scholar] [CrossRef]
- Polis, C.B.; Curtis, K.M.; Hannaford, P.C.; Phillips, S.J.; Chipato, T.; Kiarie, J.N.; Westreich, D.J.; Steyn, P.S. An Updated Systematic Review of Epidemiological Evidence on Hormonal Contraceptive Methods and HIV Acquisition in Women. AIDS 2016, 30, 2665–2683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butler, A.R.; Smith, J.A.; Polis, C.B.; Gregson, S.; Stanton, D.; Hallett, T.B. Modelling the Global Competing Risks of a Potential Interaction between Injectable Hormonal Contraception and HIV Risk. AIDS 2013, 27, 105–113. [Google Scholar] [CrossRef] [Green Version]
- Weiss, H.A.; Quigley, M.A.; Hayes, R.J. Male Circumcision and Risk of HIV Infection in Sub-Saharan Africa: A Systematic Review and Meta-Analysis. AIDS 2000, 14, 2361–2370. [Google Scholar] [CrossRef]
- Cohen, M.S.; Gay, C.L.; Busch, M.P.; Hecht, F.M. The Detection of Acute HIV Infection. J. Infect. Dis. 2010, 202, S270–S277. [Google Scholar] [CrossRef] [Green Version]
- Zetola, N.M.; Pilcher, C.D. Diagnosis and Management of Acute HIV Infection. Infect. Dis. Clin. N. Am. 2007, 21, 19–48. [Google Scholar] [CrossRef]
- Buchacz, K.; Baker, R.K.; Palella, F.J.; Chmiel, J.S.; Lichtenstein, K.A.; Novak, R.M.; Wood, K.C.; Brooks, J.T. AIDS-Defining Opportunistic Illnesses in US Patients, 1994–2007: A Cohort Study. AIDS 2010, 24, 1549–1559. [Google Scholar] [CrossRef]
- Bonnet, F.; Lewden, C.; May, T.; Heripret, L.; Jougla, E.; Bevilacqua, S.; Costagliola, D.; Salmon, D.; Chêne, G.; Morlat, P.; et al. Opportunistic Infections as Causes of Death in HIV-Infected Patients in the HAART Era in France. Scand. J. Infect. Dis. 2005, 37, 482–487. [Google Scholar] [CrossRef]
- Palella, F.J.; Delaney, K.M.; Moorman, A.C.; Loveless, M.O.; Fuhrer, J.; Satten, G.A.; Aschman, D.J.; Holmberg, S.D. Declining Morbidity and Mortality among Patients with Advanced Human Immunodeficiency Virus Infection. N. Engl. J. Med. 1998, 338, 853–860. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, J.E.; Hanson, D.; Dworkin, M.S.; Frederick, T.; Bertolli, J.; Lindegren, M.L.; Holmberg, S.; Jones, J.L. Epidemiology of Human Immunodeficiency Virus–Associated Opportunistic Infections in the United States in the Era of Highly Active Antiretroviral Therapy. Clin. Infect. Dis. 2000, 30, S5–S14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Long, J.L.; Engels, E.A.; Moore, R.D.; Gebo, K.A. Incidence and Outcomes of Malignancy in the HAART Era in an Urban Cohort of HIV-Infected Individuals. AIDS 2008, 22, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Marfatia, Y.; Singhal, P.; Khambhati, R. Hidradenitis Suppurativa in AIDS. Indian J. Sex Transm. Dis. AIDS 2010, 31, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alecsandru, D.; Padilla, B.; Izquierdo, J.A.A.; Fernández-Cruz, E.; Sánchez-Ramón, S. Severe Refractory Hidradenitis Suppurativa in an HIV-Positive Patient Successfully Treated With Infliximab. Arch. Dermatol. 2010, 146, 1343. [Google Scholar] [CrossRef] [PubMed]
- Husein-ElAhmed, H.; Fernandez-Pugnaire, M.-A.; Ruiz-Carrascosa, J.-C. Severe Hidradenitis Suppurative in an HIV-Positive Male: Use of Multiple Treatment Modalities, Including Tumor Necrosis Factor Blockade. AIDS Patient Care STDS 2011, 25, 507–508. [Google Scholar] [CrossRef] [PubMed]
- Manglani, M.; Prabhu, G.; Phiske, M.; Laddha, P. Hidradenitis Suppurativa in a HIV-Infected Child. J. Postgrad. Med. 2012, 58, 207. [Google Scholar] [CrossRef]
- Dhadke, S.V.; Korade, M.B.; Sangle, S.A.; Dhadke, V.N. Hidradenitis Suppurativa Complicating Epithelial Malignancy in Immunocompromised Patient. J. Assoc. Physicians India 2016, 64, 90–92. [Google Scholar] [PubMed]
- Bouaddi, M.; Hassam, B. Hidradenite Suppurative et Psoriasis: Anguille Sous Roche. Pan Afr. Med. J. 2017, 27, 200. [Google Scholar] [CrossRef]
- Molina-Leyva, A.; Badiola, J. Severe Refractory Hidradenitis Suppurativa Successfully Treated with Adalimumab in an HIV-Positive/Hepatitis C Virus-Positive Patient. AIDS 2018, 32, 2436–2438. [Google Scholar] [CrossRef]
- Claytor, J.D.; Viramontes, O.; Conner, S.; Wen, K.W.; Beck, K.; Chin-Hong, P.V.; Henrich, T.J.; Peluso, M.J. TNF-α Inhibition in the Setting of Undiagnosed HIV Infection: A Call for Enhanced Screening Guidelines. AIDS 2021, 35, 2163–2168. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.H.; Patel, K.R.; Singam, V.; Rastogi, S.; Silverberg, J.I. Associations of Cutaneous and Extracutaneous Infections with Hidradenitis Suppurativa in U.S. Children and Adults. Br. J. Dermatol. 2020, 182, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Kurayev, A.; Ashkar, H.; Saraiya, A.; Gottlieb, A.B. Hidradenitis Suppurativa: Review of the Pathogenesis and Treatment. J. Drugs Dermatol. 2016, 15, 1017–1022. [Google Scholar]
- Guet-Revillet, H.; Coignard-Biehler, H.; Jais, J.-P.; Quesne, G.; Frapy, E.; Poirée, S.; le Guern, A.-S.; le Flèche-Matéos, A.; Hovnanian, A.; Consigny, P.-H.; et al. Bacterial Pathogens Associated with Hidradenitis Suppurativa, France. Emerg. Infect. Dis. 2014, 20, 1990–1998. [Google Scholar] [CrossRef] [PubMed]
- Sartorius, K.; Killasli, H.; Oprica, C.; Sullivan, A.; Lapins, J. Bacteriology of Hidradenitis Suppurativa Exacerbations and Deep Tissue Cultures Obtained during Carbon Dioxide Laser Treatment. Br. J. Dermatol. 2012, 166, 879–883. [Google Scholar] [CrossRef]
- Motolese, A.; Ceccarelli, M.; Macca, L.; Li Pomi, F.; Ingrasciotta, Y.; Nunnari, G.; Guarneri, C. Novel Therapeutic Approaches to Psoriasis and Risk of Infectious Disease. Biomedicines 2022, 10, 228. [Google Scholar] [CrossRef]
- Bui, H.; Skiba, P.N.; Breskin, A.; Sayed, C. Hidradenitis Suppurativa among Patients with HIV: Investigating Patient and Disease Characteristics and Misdiagnosis. Br. J. Dermatol. 2021, 185, 1070–1072. [Google Scholar] [CrossRef]
- Deng, P.H.; Wang, C.J.; Armstrong, A.W. An Association between Hidradenitis Suppurativa and HIV. Br. J. Dermatol. 2020, 182, 490–491. [Google Scholar] [CrossRef]
- Wortsman, X.; Wortsman, J. Ultrasound Detection of Retained Hair Tracts in Hidradenitis Suppurativa. Dermatol. Surg. 2015, 41, 867–869. [Google Scholar] [CrossRef]
- Nazzaro, G.; Zerboni, R.; Passoni, E.; Barbareschi, M.; Marzano, A.V.; Muratori, S.; Veraldi, S. High-frequency Ultrasound in Hidradenitis Suppurativa as Rationale for Permanent Hair Laser Removal. Ski. Res. Technol. 2019, 25, 587–588. [Google Scholar] [CrossRef]
- Benzecry, V.; Grancini, A.; Guanziroli, E.; Nazzaro, G.; Barbareschi, M.; Marzano, A.V.; Muratori, S.; Veraldi, S. Hidradenitis Suppurativa/Acne Inversa: A Prospective Bacteriological Study and Review of the Literature. G. Ital. Di Dermatol. E Venereol. 2020, 155, 459–463. [Google Scholar] [CrossRef] [PubMed]
- Ceccarelli, M.; Venanzi Rullo, E.; Vaccaro, M.; Facciolà, A.; d’Aleo, F.; Paolucci, I.A.; Cannavò, S.P.; Cacopardo, B.; Pinzone, M.R.; Pellicanò, G.F.; et al. HIV-associated Psoriasis: Epidemiology, Pathogenesis, and Management. Dermatol. Ther. 2019, 32, e12806. [Google Scholar] [CrossRef] [PubMed]
- Facciolà, A.; Venanzi Rullo, E.; Ceccarelli, M.; D’Andrea, F.; Coco, M.; Micali, C.; Cacopardo, B.; Marino, A.; Cannavò, S.P.; di Rosa, M.; et al. Malignant Melanoma in HIV: Epidemiology, Pathogenesis, and Management. Dermatol. Ther. 2020, 33, e13180. [Google Scholar] [CrossRef] [PubMed]
- Venanzi Rullo, E.; Maimone, M.G.; Fiorica, F.; Ceccarelli, M.; Guarneri, C.; Berretta, M.; Nunnari, G. Non-Melanoma Skin Cancer in People Living With HIV: From Epidemiology to Clinical Management. Front. Oncol. 2021, 11, 689789. [Google Scholar] [CrossRef]
- Von Laffert, M.; Stadie, V.; Wohlrab, J.; Marsch, W.C. Hidradenitis Suppurativa/Acne Inversa: Bilocated Epithelial Hyperplasia with Very Different Sequelae. Br. J. Dermatol. 2011, 164, 367–371. [Google Scholar] [CrossRef]
- Jemec, G.B.E.; Thomsen, B.M.; Hansen, U. The Homogeneity of Hidradenitis Suppurativa Lesions. APMIS 1997, 105, 378–383. [Google Scholar] [CrossRef]
- ATTANOOS, R.L.; APPLETON, M.A.C.; HUGHES, L.E.; ANSELL, I.D.; DOUGLAS-JONES, A.G.; WILLIAMS, G.T. Granulomatous Hidradenitis Suppurativa and Cutaneous Crohn’s Disease. Histopathology 1993, 23, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.D.B.; Okoye, G.A.; Sokumbi, O. Histopathology of Hidradenitis Suppurativa: A Systematic Review. Dermatopathology 2022, 9, 251–257. [Google Scholar] [CrossRef]
- Boer, J.; Weltevreden, E.F. Hidradenitis Suppurativa or Acne Inversa. A Clinicopathological Study of Early Lesions. Br. J. Dermatol. 1996, 135, 721–725. [Google Scholar] [CrossRef]
- De Simone, C.; Perino, F.; Caldarola, G.; D’Agostino, M.; Peris, K. Treatment of Psoriasis with Etanercept in Immunocompromised Patients: Two Case Reports. J. Int. Med. Res. 2016, 44, 67–71. [Google Scholar] [CrossRef] [Green Version]
- Morar, N.; Willis-Owen, S.A.; Maurer, T.; Bunker, C.B. HIV-Associated Psoriasis: Pathogenesis, Clinical Features, and Management. Lancet Infect. Dis. 2010, 10, 470–478. [Google Scholar] [CrossRef]
- Cepeda, L.T.; Pieretti, M.; Chapman, S.F.; Horenstein, M.G. CD30-Positive Atypical Lymphoid Cells in Common Non-Neoplastic Cutaneous Infiltrates Rich in Neutrophils and Eosinophils. Am. J. Surg. Pathol. 2003, 27, 912–918. [Google Scholar] [CrossRef] [PubMed]
- Keane, N.M.; Price, P.; Lee, S.; Stone, S.F.; French, M.A. An Evaluation of Serum Soluble CD30 Levels and Serum CD26 (DPPIV) Enzyme Activity as Markers of Type 2 and Type 1 Cytokines in HIV Patients Receiving Highly Active Antiretroviral Therapy. Clin. Exp. Immunol. 2008, 126, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Cascajo, C. Strong Immunoexpression of the Monoclonal Antibody CD-30 in Lymphocytic Infiltrates of the Skin Not By Itself Evidence for Diagnosing Malignant Lymphoma. Am. J. Dermatopathol. 2001, 23, 79–80. [Google Scholar] [CrossRef]
- Gallitano, S.M.; McDermott, L.; Brar, K.; Lowenstein, E. Use of Tumor Necrosis Factor (TNF) Inhibitors in Patients with HIV/AIDS. J. Am. Acad. Dermatol. 2016, 74, 974–980. [Google Scholar] [CrossRef]
- Akarsu, S.; Avcı, C. Effects of Biologic Therapies for Cutaneous Inflammatory Diseases in HIV-Infected Individuals: Reliable or Not? J. Basic Clin. Health Sci. 2018, 2, 61–67. [Google Scholar] [CrossRef]
- Rosales Santillan, M.; Morss, P.C.; Porter, M.L.; Kimball, A.B. Biologic Therapies for the Treatment of Hidradenitis Suppurativa. Expert Opin. Biol. Ther. 2020, 20, 621–633. [Google Scholar] [CrossRef]
- Saunte, D.M.L.; Jemec, G.B.E. Hidradenitis Suppurativa. JAMA 2017, 318, 2019. [Google Scholar] [CrossRef]
- Chen, J.; Raymond, K. Roles of Rifampicin in Drug-Drug Interactions: Underlying Molecular Mechanisms Involving the Nuclear Pregnane X Receptor. Ann. Clin. Microbiol. Antimicrob. 2006, 5, 3. [Google Scholar] [CrossRef] [Green Version]
- Dooley, K.E.; Flexner, C.; Andrade, A.S. Drug Interactions Involving Combination Antiretroviral Therapy and Other Anti-Infective Agents: Repercussions for Resource-Limited Countries. J. Infect. Dis. 2008, 198, 948–961. [Google Scholar] [CrossRef] [Green Version]
- Bardazzi, F.; Magnano, M.; Campanati, A.; Loconsole, F.; Carpentieri, A.; Potenza, C.; Bernardini, N.; Lernia, V.; Carrera, C.; Raone, B.; et al. Biologic Therapies in HIV-Infected Patients with Psoriasis: An Italian Experience. Acta Derm. Venereol. 2017, 97, 989–990. [Google Scholar] [CrossRef] [PubMed]
- Campanati, A.; Ganzetti, G.; Giuliodori, K.; Molinelli, E.; Offidani, A. Biologic Therapy in Psoriasis: Safety Profile. Curr. Drug Saf. 2016, 11, 4–11. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors, Reference Number and Year | Type of Study | Sex/Age (Year) | Duration | Location | Severity | Treatment | Outcome |
|---|---|---|---|---|---|---|---|
| Marfatia Y et al. [24], 2010 | Case report | M/35 | 2 years | Face, thighs, gluteal region, and axilla | Not reported | Doxycicline, ibuprofen, dapsone | Partial response with recurrence |
| Alecsandru D et al. [25], 2010 | Case report | M/47 | >1 year | Axillary, gluteal, perianal, thoracic and abdominal | Severe | Infliximab, clindamycin | Remission |
| Husein-ElAhmed H et al. [26], 2011 | Case report | M/47 | 10 weeks | Inguino-scrotal perineum and gluteal areas | Not reported | Infliximab | Partial response with recurrence |
| Mangiani M et al. [27], 2012 | Case report | M/13 | 1 months | Right axilla | Not reported | Antiretroviral therapy (zidovudine, lamivudine, nevirapine) | Remission |
| Dhadke S et al. [28], 2016 | Case report | M/“Middle-age” | 10 days | Right cheek, neck, chest, shoulder, and axilla | Not reported | Local antibiotic washes, amoxicillin and clavulanic acid, prednisolone | Exitus |
| Bouaddi M et al. [29], 2017 | Case report | M/45 | 6 months | Armpits | Mild | Not reported | Not reported |
| Molina-Leyva A et al. [30], 2018 | Case report | W/39 | 16 weeks | Left and right axilla | Severe | Adalimumab | Remission |
| Claytor J et al. [31], 2021 | Case report | F/55 | “several months” | Axillary and groin | Not reported | Infliximab and methotrexate (discontinued after HIV diagnosis) | Uncontrolled after infliximab and methotrexate discontinuation |
| Rankin B et al. [6], 2021 | Case report | M/31 | 4 months | Right jawline | Moderate | Doxycycline, Isotretinoin, intralesional triamcinolone acetonide | Remission |
| Pearls for Physicians | |
|---|---|
| Evidence | Recommendations |
| Patients with HIV may develop recalcitrant forms of inflammatory comorbidities | A multidisciplinary approach is mandatory in case of suspect cutaneous manifestations |
| Patients with HS have multiple potential risk factors that can increase their infection rate | As HS and HIV are largely misdiagnosed or not regarded by patients, particular attention should be paid to anamnesis and screening |
| HIV could promote the onset and progression of HS owing to immune dysregulation | Physicians may aware of late forms of HS |
| Atypical clinical presentations (and the association between physiopathologically different dermatoses) could be subtended by retroviral infection | The involvement of atypical sites should be considered as a ’wake-up call’ |
| Clinical and therapeutic management of HS patients is characterized by a high rate of failures and recurrences, more so with HIV | Management and treatment should be as tailored as possible |
| First-line treatment options may be ineffective in HIV&HS patients or contraindicated because of concomitant medications | Different treatments, including surgery, must be considered, especially in most severe cases |
| Clinical experience seems to demonstrate that TNF-alpha inhibitors and newer biologics interfering with IL-17 and IL-23 can provide improvement in patients with HIV | Biotechnological treatments should be considered for treatment in motivated HIV&HS patients, who are monitored for CD4+ count |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Macca, L.; Moscatt, V.; Ceccarelli, M.; Ingrasciotta, Y.; Nunnari, G.; Guarneri, C. Hidradenitis Suppurativa in Patients with HIV: A Scoping Review. Biomedicines 2022, 10, 2761. https://doi.org/10.3390/biomedicines10112761
Macca L, Moscatt V, Ceccarelli M, Ingrasciotta Y, Nunnari G, Guarneri C. Hidradenitis Suppurativa in Patients with HIV: A Scoping Review. Biomedicines. 2022; 10(11):2761. https://doi.org/10.3390/biomedicines10112761
Chicago/Turabian StyleMacca, Laura, Vittoria Moscatt, Manuela Ceccarelli, Ylenia Ingrasciotta, Giuseppe Nunnari, and Claudio Guarneri. 2022. "Hidradenitis Suppurativa in Patients with HIV: A Scoping Review" Biomedicines 10, no. 11: 2761. https://doi.org/10.3390/biomedicines10112761