
Responsive Neurostimulation for Seizure Control: Current Status and Future Directions

Abstract
:1. Introduction
2. Surgical Intervention in Epilepsy
3. Introduction to Neuromodulatory Therapies
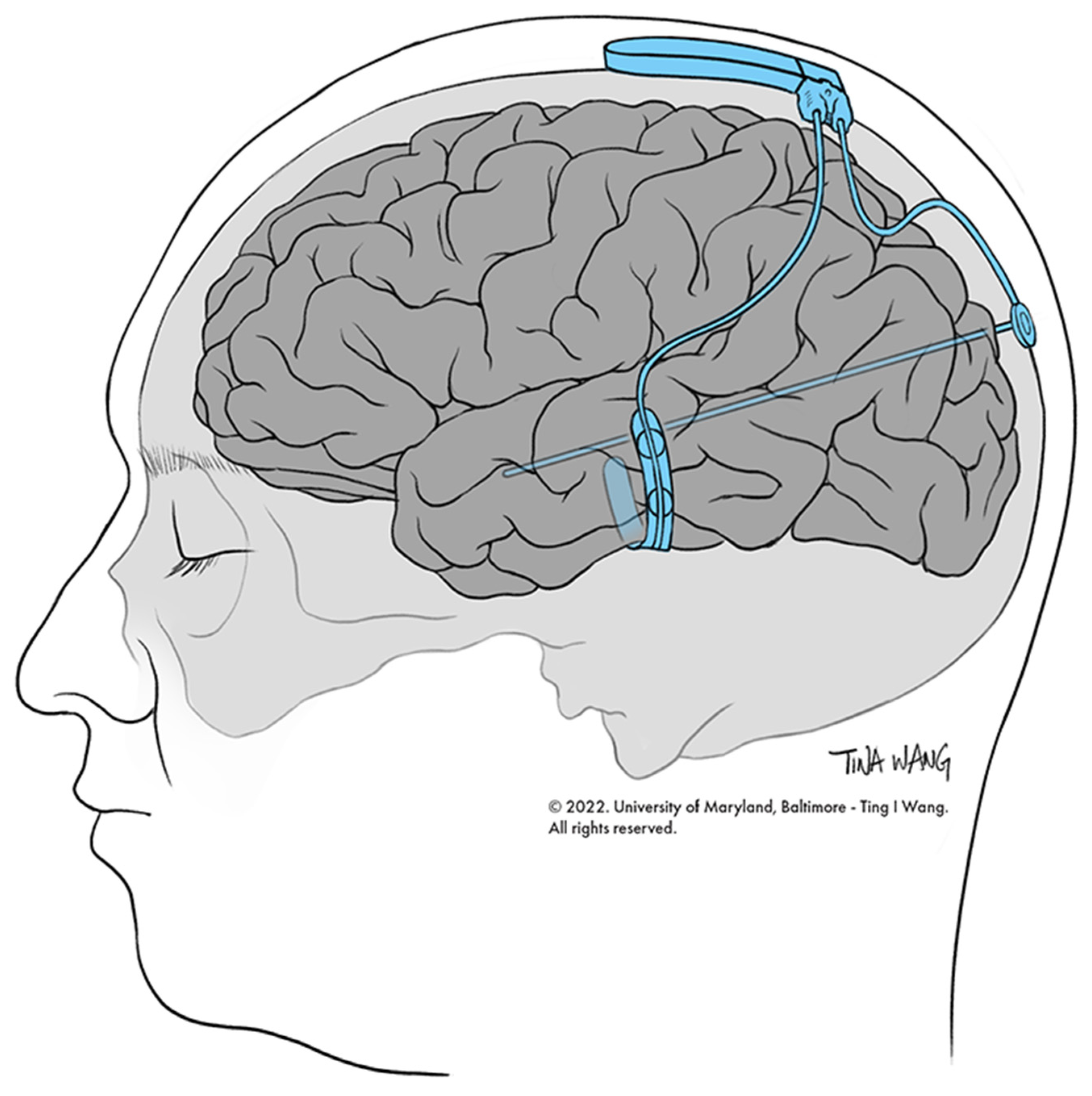
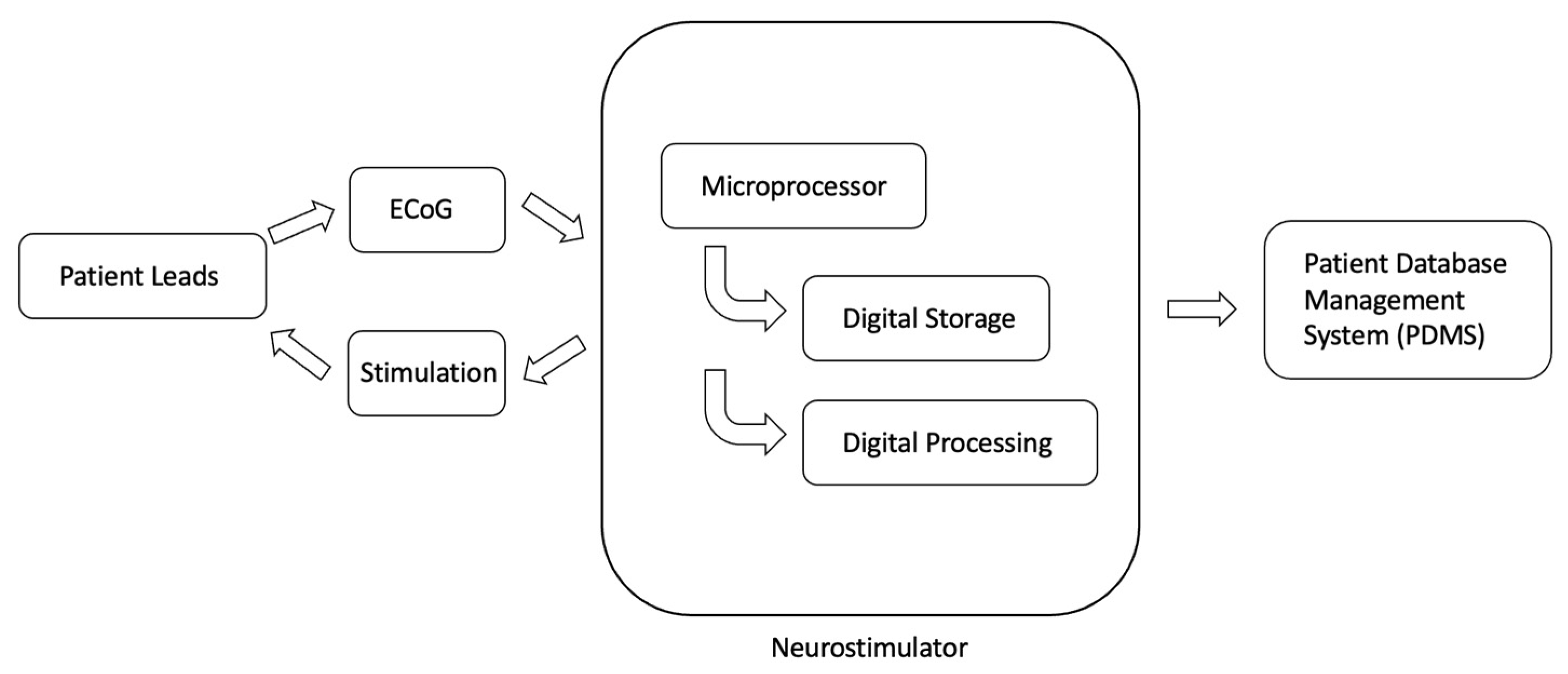
4. Introduction to RNS
5. RNS for Focal Epilepsy
6. RNS Modulation of Epileptic Networks
6.1. Epilepsy as a Network Disorder
6.2. Modulation of Epileptic Network
7. Improving Seizure Prediction and Control
7.1. Improving Seizure Prediction
7.2. Improving Seizure Control
7.3. Ambulatory ECoG Data
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Nomenclature Table
| Term | Abbreviation |
| Afterdischarges | AD |
| Anterior thalamic nucleus | ATN |
| Anti-seizure medications | ASMs |
| Area under the curve | AUC |
| Brief pulse stimuli | BPS |
| Centromedian nucleus | CMN |
| Computed tomography | CT |
| Convolutional neural network | CNN |
| Deep brain stimulation | DBS |
| Drug-resistant epilepsy | DRE |
| Electrocorticography | ECoG |
| Electroencephalography | EEG |
| Epilepsy monitoring unit | EMU |
| Epileptogenic focus | EF |
| Food and Drug Administration | FDA |
| Interictal epileptiform activity | IEA |
| Intracranial electroencephalography | iEEG |
| Long-term treatment | LTT |
| Magnetic resonance-guided laser-interstitial thermal therapy | MR-guided LITT |
| Magnetic resonance imaging | MRI |
| Magnetoencephalogram | MEG |
| Mesial temporal lobe epilepsy | MTLE |
| Odds ratio | OR |
| Patient data management system | PDMS |
| Positron emission tomography | PET |
| Principal component analysis | PCA |
| Responsive neurostimulation | RNS |
| Seizure onset zone | SOZ |
| Stereotactic electroencephalography | SEEG |
| Support vector machine | SVM |
| Temporal lobe epilepsy | TLE |
References
- Thijs, R.D.; Surges, R.; O’Brien, T.J.; Sander, J.W. Epilepsy in adults. Lancet 2019, 393, 689–701. [Google Scholar] [CrossRef]
- Helbig, I.; Scheffer, I.E.; Berkovic, S.F. Genetic Epilepsies. Mol. Neurol. 2007, 24, 371–383. [Google Scholar] [CrossRef]
- Scheffer, I.E.; Berkovic, S.; Capovilla, G.; Connolly, M.B.; French, J.; Guilhoto, L.; Hirsch, E.; Jain, S.; Mathern, G.W.; Mosh, S.L.; et al. ILAE classification of the epilepsies: Position paper of the ILAE Commission for Classification and Terminology. Epilepsia 2017, 58, 512–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarmast, S.T.; Abdullahi, A.M.; Jahan, N. Current Classification of Seizures and Epilepsies: Scope, Limitations and Recommendations for Future Action. Cureus 2020, 12, e10549. [Google Scholar] [CrossRef]
- Blümcke, I. Neuropathology of focal epilepsies: A critical review. Epilepsy Behav. 2009, 15, 34–39. [Google Scholar] [CrossRef]
- Ostendorf, A.P.; Ahrens, S.M.; Lado, F.A.; Arnold, S.T.; Bai, S.; Owen, M.K.B.; Chapman, K.E.; Clarke, D.F.; Eisner, M.; Fountain, N.B.; et al. United States Epilepsy Center Characteristics. Neurology 2022, 98, e449–e458. [Google Scholar] [CrossRef]
- Kwan, P.; Brodie, M.J. Early identification of refractory epilepsy. N. Engl. J. Med. 2000, 342, 314–319. [Google Scholar] [CrossRef]
- Sperli, F.; Spinelli, L.; Seeck, M.; Kurian, M.; Michel, C.M.; Lantz, G. EEG source imaging in pediatric epilepsy surgery: A new perspective in presurgical workup. Epilepsia 2006, 47, 981–990. [Google Scholar] [CrossRef]
- Britton, J.; Frey, L. A Brief History of EEG. In Electroencephalography (EEG): An Introductory Text and Atlas of Normal and Abnormal Findings in Adults, Children, and Infants; St. Louis, E., Frey, L., Eds.; American Epilepsy Society: Chicago, IL, USA, 2016. [Google Scholar]
- Reif, P.S.; Strzelczyk, A.; Rosenow, F. The history of invasive EEG evaluation in epilepsy patients. Seizure 2016, 41, 191–195. [Google Scholar] [CrossRef] [Green Version]
- Teplan, M. Fundamentals of Eeg Measurement. Meas. Sci. Rev. 2002, 2, 1–11. [Google Scholar]
- Buzsáki, G.; Anastassiou, C.A.; Koch, C. The origin of extracellular fields and currents—EEG, ECoG, LFP and spikes. Nat. Rev. Neurosci. 2012, 13, 407–420. [Google Scholar] [CrossRef]
- Almeida, A.N.; Martinez, V.; Feindel, W. The First Case of Invasive EEG Monitoring for the Surgical Treatment of Epilepsy: Historical Significance and Context. Epilepsia 2005, 46, 1082–1085. [Google Scholar] [CrossRef]
- Nunez, P.L.; Srinivasan, R. Electric Fields of the Brain the Neurophysics of EEG, 2nd ed.; Oxford University Press: Oxford, UK, 2006. [Google Scholar]
- Sanchez-Reyes, L.M.; Rodriguez-Resendiz, J.; Avecilla-Ramirez, G.N.; Garcia-Gomar, M.L.; Robles-Ocampo, J.B. Impact of EEG Parameters Detecting Dementia Diseases: A Systematic Review. IEEE Access 2021, 9, 78060–78074. [Google Scholar] [CrossRef]
- Ibrahimi, D.; Mendiola-Santibañez, J.D.; Martínez, E.C.; Rodríguez-Reséndiz, J.; Pacheco, I.T. Cortical Activity at Baseline and during Light Stimulation in Patients with Strabismus and Amblyopia. IEEE Access 2021, 9, 22430–22446. [Google Scholar] [CrossRef]
- Ortiz-Echeverri, C.J.; Salazar-Colores, S.; Rodríguez-Reséndiz, J.; Gómez-Loenzo, R.A. A New Approach for Motor Imagery Classification Based on Sorted Blind Source Separation, Continuous Wavelet Transform, and Convolutional Neural Network. Sensors 2019, 19, 4541. [Google Scholar] [CrossRef] [Green Version]
- Penfield, W.; Jasper, H.H. Epilepsy and the Functional Anatomy of the Human Brain, 1st ed.; Herbert, H., Penfield, W., Eds.; Little Brown: Boston, MA, USA, 1954; ISBN 9780316698337. [Google Scholar]
- North, R.Y.; Raskin, J.S.; Curry, D.J. MRI-Guided Laser Interstitial Thermal Therapy for Epilepsy. Neurosurg. Clin. N. Am. 2017, 28, 545–557. [Google Scholar] [CrossRef]
- Engel, J.; McDermott, M.P.; Wiebe, S.; Langfitt, J.T.; Stern, J.M.; Dewar, S.; Sperling, M.R.; Gardiner, I.; Erba, G.; Fried, I.; et al. Early surgical therapy for drug-resistant temporal lobe epilepsy: A randomized trial. JAMA 2012, 307, 922–930. [Google Scholar] [CrossRef]
- Engel, J.; Wiebe, S.; French, J.; Sperling, M.; Williamson, P.; Spencer, D.; Gumnit, R.; Zahn, C.; Westbrook, E.; Enos, B. Practice parameter: Temporal lobe and localized neocortical resections for epilepsy: Report of the Quality Standards Subcommittee of the American Academy of Neurology, in association with the American Epilepsy Society and the American Association of Neurological Surgeons. Neurology 2003, 60, 538–547. [Google Scholar] [CrossRef]
- Vakharia, V.N.; Duncan, J.S.; Witt, J.A.; Elger, C.E.; Staba, R.; Engel, J. Getting the best outcomes from epilepsy surgery. Ann. Neurol. 2018, 83, 676–690. [Google Scholar] [CrossRef]
- Benbadis, S.R. Neurostimulation for the treatment of epilepsy. Epilepsy Behav. 2018, 88S, 1. [Google Scholar] [CrossRef]
- Geller, E.B. Responsive neurostimulation: Review of clinical trials and insights into focal epilepsy. Epilepsy Behav. 2018, 88S, 11–20. [Google Scholar] [CrossRef]
- Neuropathic Pain: Pathophysiological Response of Nerves to Injury-ClinicalKey. Available online: https://www.clinicalkey.com/#!/content/book/3-s2.0-B9780702040597000619%20 (accessed on 20 May 2022).
- Lesser, R.P.; Kim, S.H.; Beyderman, L.; Miglioretti, D.L.; Webber, W.R.S.; Bare, M.; Cysyk, B.; Krauss, G.; Gordon, B. Brief bursts of pulse stimulation terminate afterdischarges caused by cortical stimulation. Neurology 1999, 53, 2073–2081. [Google Scholar] [CrossRef]
- Motamedi, G.K.; Lesser, R.P.; Miglioretti, D.L.; Mizuno-Matsumoto, Y.; Gordon, B.; Webber, W.R.S.; Jackson, D.C.; Sepkuty, J.P.; Crone, N.E. Optimizing parameters for terminating cortical afterdischarges with pulse stimulation. Epilepsia 2002, 43, 836–846. [Google Scholar] [CrossRef]
- Groves, D.A.; Brown, V.J. Vagal nerve stimulation: A review of its applications and potential mechanisms that mediate its clinical effects. Neurosci. Biobehav. Rev. 2005, 29, 493–500. [Google Scholar] [CrossRef]
- Beekwilder, J.P.; Beems, T. Overview of the clinical applications of vagus nerve stimulation. J. Clin. Neurophysiol. 2010, 27, 130–138. [Google Scholar] [CrossRef]
- Rincon, N.; Barr, D.; Velez-Ruiz, N. Neuromodulation in Drug Resistant Epilepsy. Aging Dis. 2021, 12, 1070–1080. [Google Scholar] [CrossRef]
- Toffa, D.H.; Touma, L.; El Meskine, T.; Bouthillier, A.; Nguyen, D.K. Learnings from 30 years of reported efficacy and safety of vagus nerve stimulation (VNS) for epilepsy treatment: A critical review. Seizure 2020, 83, 104–123. [Google Scholar] [CrossRef]
- Yang, J.; Phi, J.H. The Present and Future of Vagus Nerve Stimulation. J. Korean Neurosurg. Soc. 2019, 62, 344–352. [Google Scholar] [CrossRef] [Green Version]
- Lozano, A.M.; Lipsman, N.; Bergman, H.; Brown, P.; Chabardes, S.; Chang, J.W.; Matthews, K.; McIntyre, C.C.; Schlaepfer, T.E.; Schulder, M.; et al. Deep brain stimulation: Current challenges and future directions. Nat. Rev. Neurol. 2019, 15, 148–160. [Google Scholar] [CrossRef]
- Sun, Y.; Friedman, D.; Dugan, P.; Holmes, M.; Wu, X.; Liu, A. Machine Learning to Classify Relative Seizure Frequency From Chronic Electrocorticography. In Journal of Clinical Neurophysiology; Wolters Kluwer: Alphen aan den Rijn, The Netherlands, 2021. [Google Scholar] [CrossRef]
- Dalic, L.J.; Warren, A.E.L.; Young, J.C.; Thevathasan, W.; Roten, A.; Bulluss, K.J.; Archer, J.S. Cortex leads the thalamic centromedian nucleus in generalized epileptic discharges in Lennox-Gastaut syndrome. Epilepsia 2020, 61, 2214–2223. [Google Scholar] [CrossRef]
- Valentín, A.; Navarrete, E.G.; Chelvarajah, R.; Torres, C.; Navas, M.; Vico, L.; Torres, N.; Pastor, J.; Selway, R.; Sola, R.G.; et al. Deep brain stimulation of the centromedian thalamic nucleus for the treatment of generalized and frontal epilepsies. Epilepsia 2013, 54, 1823–1833. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.; Mani, R.; Danish, S. Comparison and Selection of Current Implantable Anti-Epileptic Devices. Neurotherapeutics 2019, 16, 369. [Google Scholar] [CrossRef] [PubMed]
- Sun, F.T.; Morrell, M.J. The RNS System: Responsive cortical stimulation for the treatment of refractory partial epilepsy. Expert Rev. Med. Devices 2014, 11, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Ma, B.B.; Rao, V.R. Responsive neurostimulation: Candidates and considerations. Epilepsy Behav. 2018, 88, 388–395. [Google Scholar] [CrossRef]
- Inaji, M.; Yamamoto, T.; Kawai, K.; Maehara, T.; Doyle, W.K. Responsive Neurostimulation as a Novel Palliative Option in Epilepsy Surgery. Neurol. Med. Chir. 2021, 61, 1–11. [Google Scholar] [CrossRef]
- Kokkinos, V.; Sisterson, N.D.; Wozny, T.A.; Richardson, R.M. Association of Closed-Loop Brain Stimulation Neurophysiological Features with Seizure Control among Patients with Focal Epilepsy. JAMA Neurol. 2019, 76, 800–808. [Google Scholar] [CrossRef] [Green Version]
- NeuroPace. In RNS ® System Programming Manual For the RNS ® Tablet Model 5000 and the Patient Data Management System (PDMS) Model 4340; NeuroPace Inc.: Mountain View, CA, USA, 2021.
- Ellens, N.R.; Elisevich, K.; Burdette, D.E.; Patra, S.E. A Comparison of Vagal Nerve Stimulation and Responsive Neurostimulation for the Treatment of Medically Refractory Complex Partial Epilepsy. Stereotact. Funct. Neurosurg. 2018, 96, 259–263. [Google Scholar] [CrossRef]
- Nair, D.R.; Laxer, K.D.; Weber, P.B.; Murro, A.M.; Park, Y.D.; Barkley, G.L.; Smith, B.J.; Gwinn, R.P.; Doherty, M.J.; Noe, K.H.; et al. Nine-year prospective efficacy and safety of brain-responsive neurostimulation for focal epilepsy. Neurology 2020, 95, e1244–e1256. [Google Scholar] [CrossRef]
- Bergey, G.K.; Morrell, M.J.; Mizrahi, E.M.; Goldman, A.; King-Stephens, D.; Nair, D.; Srinivasan, S.; Jobst, B.; Gross, R.E.; Shields, D.C.; et al. Long-term treatment with responsive brain stimulation in adults with refractory partial seizures. Neurology 2015, 84, 810–817. [Google Scholar] [CrossRef]
- Jobst, B.C.; Kapur, R.; Barkley, G.L.; Bazil, C.W.; Berg, M.J.; Bergey, G.K.; Boggs, J.G.; Cash, S.S.; Cole, A.J.; Duchowny, M.S.; et al. Brain-responsive neurostimulation in patients with medically intractable seizures arising from eloquent and other neocortical areas. Epilepsia 2017, 58, 1005–1014. [Google Scholar] [CrossRef]
- Geller, E.B.; Skarpaas, T.L.; Gross, R.E.; Goodman, R.R.; Barkley, G.L.; Bazil, C.W.; Berg, M.J.; Bergey, G.K.; Cash, S.S.; Cole, A.J.; et al. Brain-responsive neurostimulation in patients with medically intractable mesial temporal lobe epilepsy. Epilepsia 2017, 58, 994–1004. [Google Scholar] [CrossRef]
- Andrews, J.P.; Gummadavelli, A.; Farooque, P.; Bonito, J.; Arencibia, C.; Blumenfeld, H.; Spencer, D.D. Association of Seizure Spread with Surgical Failure in Epilepsy. JAMA Neurol. 2019, 76, 462–469. [Google Scholar] [CrossRef]
- Stam, C.J. Epilepsy: What can we Learn from Modern Network Theories? Epileptologie 2016, 33, 38–43. [Google Scholar]
- Zaveri, H.P.; Schelter, B.; Schevon, C.A.; Jiruska, P.; Jefferys, J.G.R.; Worrell, G.; Schulze-Bonhage, A.; Joshi, R.B.; Jirsa, V.; Goodfellow, M.; et al. Controversies on the network theory of epilepsy: Debates held during the ICTALS 2019 conference. Seizure 2020, 78, 78. [Google Scholar] [CrossRef]
- Bailey, P.; Gibbs, F.A. The surgical treatment of psychomotor epilepsy. J. Am. Med. Assoc. 1951, 145, 365–370. [Google Scholar] [CrossRef]
- Ramaraju, S.; Wang, Y.; Sinha, N.; McEvoy, A.W.; Miserocchi, A.; de Tisi, J.; Duncan, J.S.; Rugg-Gunn, F.; Taylor, P.N. Removal of Interictal MEG-Derived Network Hubs Is Associated With Postoperative Seizure Freedom. Front. Neurol. 2020, 11, 563847. [Google Scholar] [CrossRef]
- Sisterson, N.D.; Kokkinos, V.; Urban, A.; Li, N.; Richardson, R.M. Responsive neurostimulation of the thalamus improves seizure control in idiopathic generalised epilepsy: Initial case series. J. Neurol. Neurosurg. Psychiatry 2022, 93, 491–498. [Google Scholar] [CrossRef]
- Fan, J.M.; Lee, A.T.; Kudo, K.; Ranasinghe, K.G.; Morise, H.; Findlay, A.M.; Kirsch, H.E.; Chang, E.F.; Nagarajan, S.S.; Rao, V.R. Network connectivity predicts effectiveness of responsive neurostimulation in focal epilepsy. Brain Commun. 2022, 4, fcac104. [Google Scholar] [CrossRef]
- Charlebois, C.M.; Anderson, D.N.; Johnson, K.A.; Philip, B.J.; Davis, T.S.; Newman, B.J.; Peters, A.Y.; Arain, A.M.; Dorval, A.D.; Rolston, J.D.; et al. Patient-specific structural connectivity informs outcomes of responsive neurostimulation for temporal lobe epilepsy. Epilepsia 2022, 63, 2037–2055. [Google Scholar] [CrossRef]
- Devaluez, M.; Tir, M.; Krystkowiak, P.; Aubignat, M.; Lefranc, M. Selection of deep brain stimulation contacts using volume of tissue activated software following subthalamic nucleus stimulation. J. Neurosurg. 2020, 1, 1–8. [Google Scholar] [CrossRef]
- Middlebrooks, E.H.; Grewal, S.S.; Stead, M.; Lundstrom, B.N.; Worrell, G.A.; Van Gompel, J.J. Differences in functional connectivity profiles as a predictor of response to anterior thalamic nucleus deep brain stimulation for epilepsy: A hypothesis for the mechanism of action and a potential biomarker for outcomes. Neurosurg. Focus 2018, 45, E7. [Google Scholar] [CrossRef]
- Lee, J.; Park, J.; Yang, S.; Kim, H.; Choi, Y.S.; Kim, H.J.; Lee, H.W.; Lee, B.U. Early seizure detection by applying frequency-based algorithm derived from the principal component analysis. Front. Neuroinform. 2017, 11, 52. [Google Scholar] [CrossRef] [Green Version]
- Constantino, A.C.; Sisterson, N.D.; Zaher, N.; Urban, A.; Richardson, R.M.; Kokkinos, V. Expert-Level Intracranial Electroencephalogram Ictal Pattern Detection by a Deep Learning Neural Network. Front. Neurol. 2021, 12, 673. [Google Scholar] [CrossRef]
- Jarosiewicz, B.; Morrell, M. The RNS System: Brain-responsive neurostimulation for the treatment of epilepsy. Expert Rev. Med. Devices 2020, 18, 129–138. [Google Scholar] [CrossRef]
- Selesko, M.J.; Selesko, M.J. Time Evolution of ECoG Network Connectivity in Patients with Refractory Epilepsy. 2018. Available online: https://scholarworks.gvsu.edu/theses/897 (accessed on 27 July 2022).
- Tran, D.K.; Tran, D.C.; Mnatsakayan, L.; Lin, J.; Hsu, F.; Vadera, S. Treatment of Multi-Focal Epilepsy With Resective Surgery Plus Responsive Neurostimulation (RNS): One Institution’s Experience. Front. Neurol. 2020, 11, 1167. [Google Scholar] [CrossRef]
- Vetkas, A.; Germann, J.; Elias, G.; Loh, A.; Boutet, A.; Yamamoto, K.; Sarica, C.; Samuel, N.; Milano, V.; Fomenko, A.; et al. Identifying the neural network for neuromodulation in epilepsy through connectomics and graphs. Brain Commun. 2022, 4, fcac092. [Google Scholar] [CrossRef]
- Rao, V.R. Chronic electroencephalography in epilepsy with a responsive neurostimulation device: Current status and future prospects. Expert Rev. Med. Devices 2021, 18, 1093–1105. [Google Scholar] [CrossRef]
- Baud, M.O.; Schindler, K.; Rao, V.R. Under-sampling in epilepsy: Limitations of conventional EEG. Clin. Neurophysiol. Pract. 2020, 6, 41–49. [Google Scholar] [CrossRef]
- Chiang, S.; Fan, J.M.; Rao, V.R. Bilateral temporal lobe epilepsy: How many seizures are required in chronic ambulatory electrocorticography to estimate the laterality ratio? Epilepsia 2022, 63, 199–208. [Google Scholar] [CrossRef]
- Salinsky, M.C.; Oken, B.S.; Storzbach, D.; Dodrill, C.B. Assessment of CNS effects of antiepileptic drugs by using quantitative EEG measures. Epilepsia 2003, 44, 1042–1050. [Google Scholar] [CrossRef]
- Zaveri, H.P.; Pincus, S.M.; Goncharova, I.I.; Novotny, E.J.; Duckrow, R.B.; Spencer, D.D.; Blumenfeld, H.; Spencer, S.S. Background intracranial EEG spectral changes with anti-epileptic drug taper. Clin. Neurophysiol. 2010, 121, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Zaveri, H.P.; Pincus, S.M.; Goncharova, I.I.; Novotny, E.J.; Duckrow, R.B.; Spencer, D.D.; Spencer, S.S. A decrease in EEG energy accompanies anti-epileptic drug taper during intracranial monitoring. Epilepsy Res. 2009, 86, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Sisterson, N.D.; Kokkinos, V. Neuromodulation of Epilepsy Networks. Neurosurg. Clin. N. Am. 2020, 31, 459–470. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Neuromodulatory Intervention | 50% Responder Rate |
|---|---|
| RNS | 1 year: 44% 2 years: 55% 5 years: 50–61% [37] |
| VNS | 1 year: 45–65% [31,32] |
| DBS | 1 year: 43.4% 2 years: 53.7% 5 years: 67.8% 7 years: 74% [37] |
| Study | Authors and Year | Study Type and Number of Patients | Main Points |
|---|---|---|---|
| Association of Closed-Loop Brain Stimulation Neurophysiological Features With Seizure Control Among Patients With Focal Epilepsy | Kokkinos et al., 2019 [41] | Retrospective study, 11 patients |
|
| Network connectivity predicts effectiveness of responsive neurostimulation in focal epilepsy | Fan et al., 2022 [54] | Retrospective study, 31 patients |
|
| Patient-specific structural connectivity informs outcomes of responsive neurostimulation for temporal lobe epilepsy | Charlebois et al., 2022 [55] | Retrospective study, 22 patients |
|
| Study | Authors and Year | Study Type and Number of Patients | Machine Learning Algorithms Used | Main Points |
|---|---|---|---|---|
| Machine Learning to Classify Relative Seizure Frequency From Chronic Electrocorticography | Yueqiu et al., 2021 | Retrospective study, 5 patients |
|
|
| Expert-Level Intracranial Electroencephalogram Ictal Pattern Detection by a Deep Learning Neural Network | Constantino et al., 2021 | Retrospective study, 22 patients |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boddeti, U.; McAfee, D.; Khan, A.; Bachani, M.; Ksendzovsky, A. Responsive Neurostimulation for Seizure Control: Current Status and Future Directions. Biomedicines 2022, 10, 2677. https://doi.org/10.3390/biomedicines10112677
Boddeti U, McAfee D, Khan A, Bachani M, Ksendzovsky A. Responsive Neurostimulation for Seizure Control: Current Status and Future Directions. Biomedicines. 2022; 10(11):2677. https://doi.org/10.3390/biomedicines10112677
Chicago/Turabian StyleBoddeti, Ujwal, Darrian McAfee, Anas Khan, Muzna Bachani, and Alexander Ksendzovsky. 2022. "Responsive Neurostimulation for Seizure Control: Current Status and Future Directions" Biomedicines 10, no. 11: 2677. https://doi.org/10.3390/biomedicines10112677