
Modulatory Effects of NBF1, an Algal Fiber-Rich Bioformula, on Adiponectin and C-Reactive Protein Levels, and Its Therapeutic Prospects for Metabolic Syndrome and Type-2 Diabetes Patients
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Dietary Survey and Intervention with NBF1
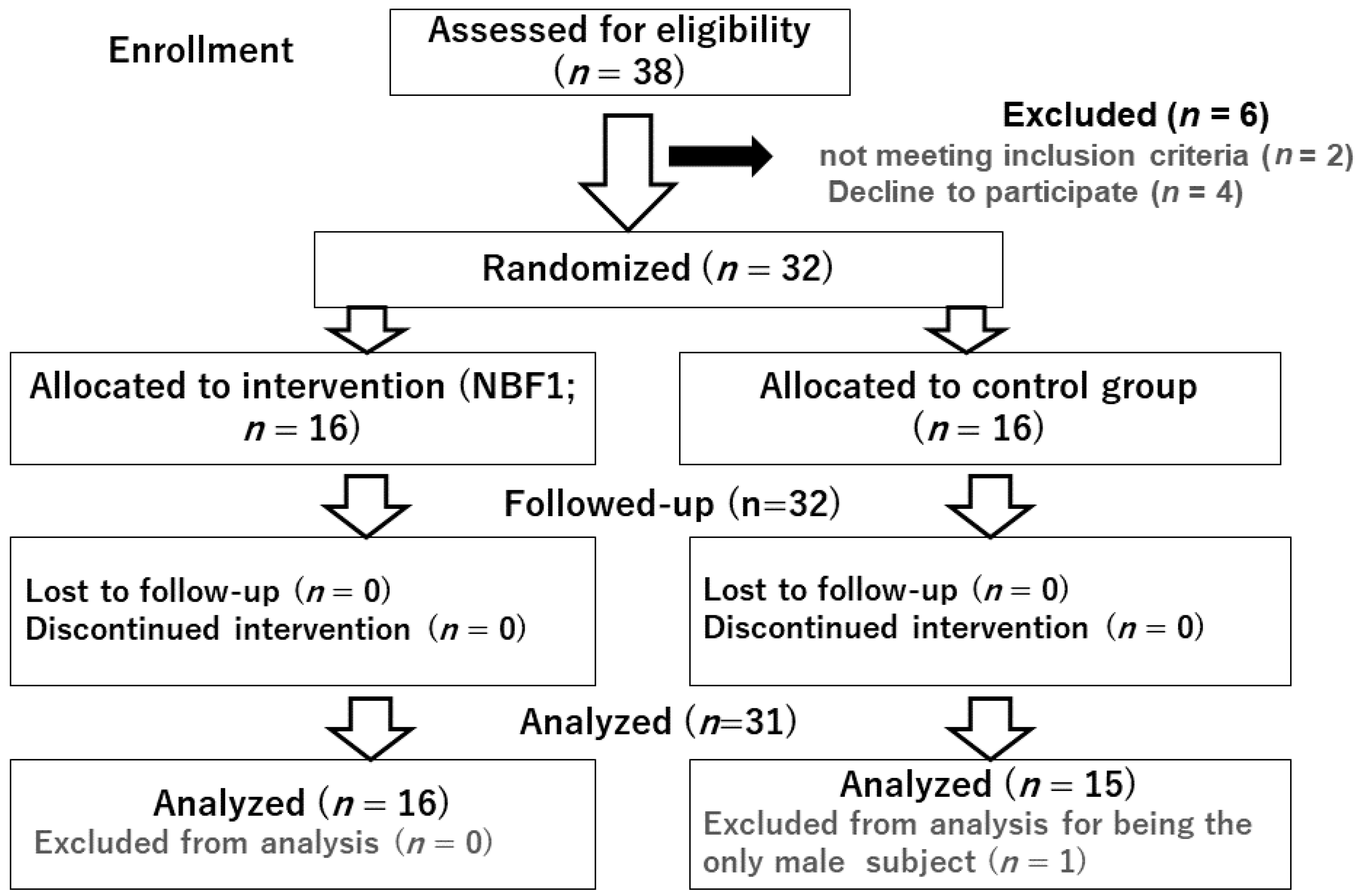
2.1.1. Participants and Sample Size of the Dietary Intervention
2.1.2. Diet History Survey
2.1.3. Composition of the Supplements
2.2. Outcome Variables
2.3. Enzyme-Linked Immunosorbent Assay (ELISA) for Measurement of Bio Markers
2.4. Clinical Case Reports
2.5. Data Collection and Analysis
3. Results
3.1. Sociodemographic Characteristics, Dietary Intake of Macro and Micronutrients
3.2. Relationship between Daily Algal Fiber and n3PUFA Intake and Cardiometabolic Markers
3.3. Effects of NBF1 Supplementation on Metabolic Markers in T2DM Patients and Subject with Metabolic Risk (Case Reports)
- (1)
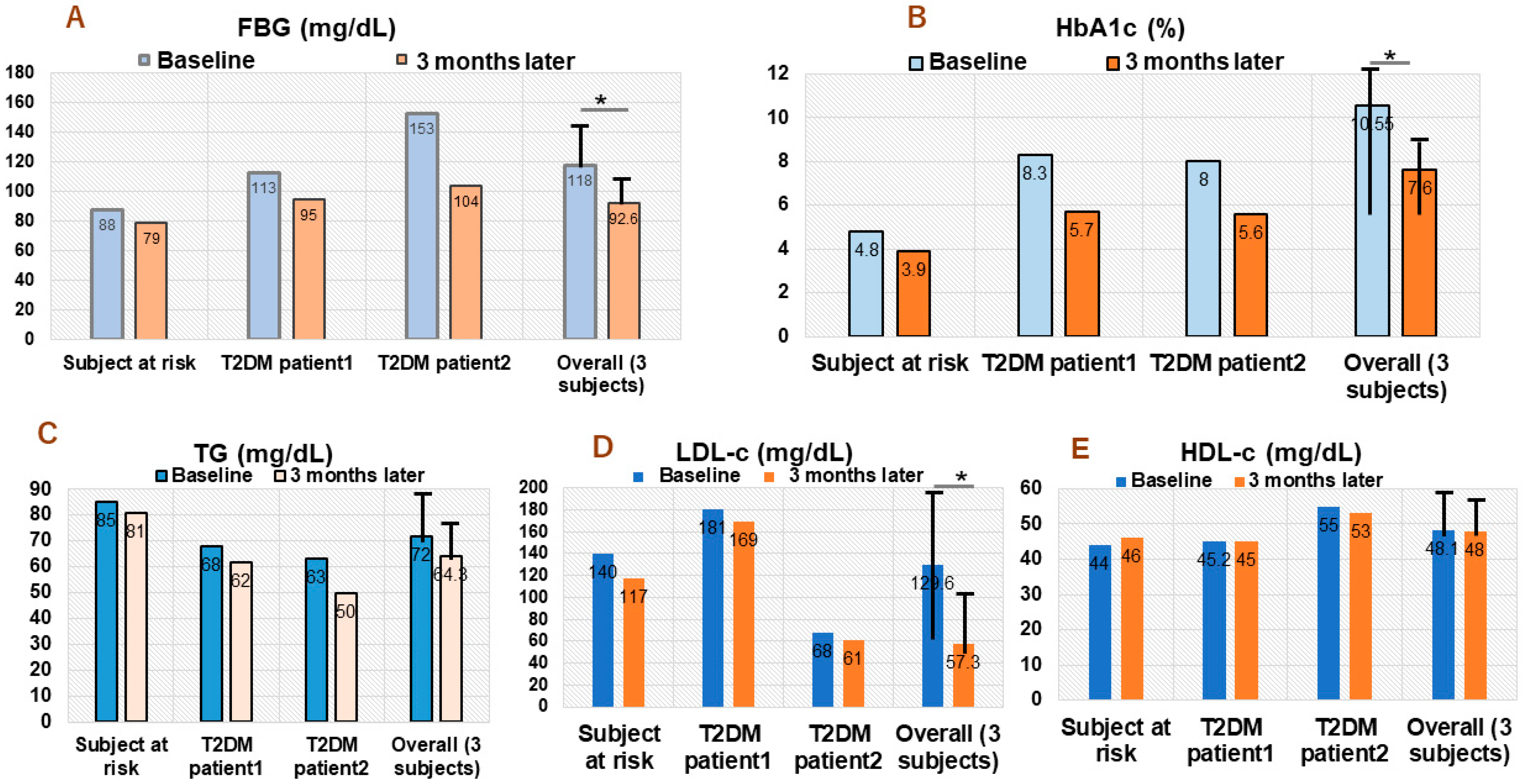
- Subject with hypercholesterolemia: 53 years old African healthcare worker with a history of high blood pressure, which has been successfully stabilized using antihypertensive drug (methyldopa). He had normal FBG and HbA1c, but high LDL-c level (140 mg/dL) at day 1 of NBF1 intake in 2020. An improvement of FBG (change: −15 mg/dL), HbA1c (change: −0.9%), TG −8 mg/dL), LDL-c (change: −23 mg/dL) were observed after a 3-month dietary intervention (Figure 2).
- (2)
- T2DM patient 1: 56 years old African living in Japan; he has been under oral thiazolidinedione for 2 years, before adding NFB1 in 2019. At baseline (day 1 of NBF1), fasting blood glucose (FBG) was 113 mg/dL, 8.3% for HbA1c, and elevated LDL-c (181 mg/dL) levels. Noticeable decrease of FBG (change: −18 mg/dL), HbA1c (−2.6%), TG (−6 mg/dL) and LDL-c (−12 mg/dL) were observed after 3 months of NBF1 supplementation (Figure 2).
- (3)
- T2DM patient 2: 57 years old African living in DR Congo; he has been under a combination of oral thiazolidinedione and insulin injection for 8 months, and NFB1 was added in 2019. Baseline FBG (153 mg/dL) and HbA1c (8%) were high. However, a marked improvement of metabolic health markers was observed, particularly for FBG (−49 mg/dL), HbA1c (−2.4%), TG (−13 mg/dL), and LDL-c (−7 mg/dL) after 3 months of NBF1 intake (Figure 2).
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Karupaiah, T.; Chuah, K.A.; Chinna, K.; Pressman, P.; Clemens, R.A.; Sundram, H.K. A cross-sectional study on the dietary pattern impact on cardiovascular disease biomarkers in Malaysia. Sci. Rep. 2019, 9, 13666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pico, C.; Serra, F.; Rodriguez, A.M.; Keijer, J.; Palou, A. Biomarkers of nutrition and health: New tools for new approaches. Nutrients 2019, 11, 1092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eyre, H.; Kahn, R.; Robertson, R.M. Preventing cancer, cardiovascular disease, and diabetes: A common agenda for the American Cancer Society, the American Diabetes Association, and the American Heart Association. Diabetes Care 2004, 27, 1812–1824. [Google Scholar] [CrossRef] [Green Version]
- Kachan, D.; Lewis, J.E.; Davila, E.P.; Arheart, K.L.; LeBlanc, W.G.; Fleming, L.F.; Cabán-Martinez, A.J.; Lee, D.J. Nutrient intake and adherence to dietary recommendations among US workers. J. Occup. Environ. Med. 2012, 54, 101–105. [Google Scholar] [CrossRef] [Green Version]
- Stampfer, M.J.; Hu, F.B.; Manson, J.E.; Rimm, E.B.; Willett, W.C. Primary prevention of coronary heart disease in women through diet and lifestyle. N. Engl. J. Med. 2000, 343, 16–22. [Google Scholar] [CrossRef]
- Hruby, A.; Jacques, P.F. Dietary protein and changes in markers of cardiometabolic health across 20 years of follow-up in middle-aged Americans. Publ. Health Nutr. 2018, 21, 2998–3010. [Google Scholar] [CrossRef] [Green Version]
- Ridker, P.M.; Buring, J.E.; Cook, N.R.; Rifai, N. C-reactive protein, the metabolic syndrome, and risk of incident cardiovascular events. Circulation 2003, 107, r20–r26. [Google Scholar] [CrossRef]
- Pradhan, A.D.; Manson, J.E.; Rifai, N.; Buring, J.E.; Ridker, P.M. C-reactive protein, interleukin 6, and the risk of developing type-2 diabetes mellitus. JAMA 2001, 286, 327–334. [Google Scholar] [CrossRef]
- Freeman, D.J.; Norrie, J.; Caslake, M.J.; Gaw, A.; Ford, I.; Lowe, G.D.O.; O′Reilly, D.S.J.; Packard, C.J.; Sattar, N.; West of Scotland Coronary Prevention Study Group. C-Reactive Protein Is an Independent predictor of risk for the development of diabetes in the West of Scotland Coronary Prevention Study. Diabetes 2002, 51, 1596–1600. [Google Scholar] [CrossRef] [Green Version]
- Maeda, N.; Shimomura, I.; Kishida, K.; Nishizawa, H.; Matsuda, M.; Nagaretani, H.; Furuyama, N.; Kondo, H.; Takahashi, M.; Arita, Y.; et al. Diet-induced insulin resistance in mice lacking adiponectin/ACRP30. Nat. Med. 2002, 8, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Kandasamy, A.D.; Sung, M.M.; Boisvenue, J.J.; Barr, A.J.; Dyck, J.R.B. Adiponectin gene-therapy ameliorates high fat, high sucrose diet-induced metabolic perturbations in mice. Nutr. Diab. 2012, 2, e95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ngatu, R.N.; Ikeda, M.; Watanabe, H.; Tanaka, M.; Inoue, M.; Kanbara, S.; Nojima, S. Uncovering adiponectin replenishing property of sujiaonori algal biomaterial in humans. Mar. Drugs 2017, 15, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, J.; Stryjecki, C.; Reddon, H.; Peralta-Romero, J.; Karam-Araujo, R.; Suarez, F. Adiponectin is associated with cardiometabolic traits in Mexican children. Sci. Rep. 2019, 9, 3084. [Google Scholar] [CrossRef] [Green Version]
- Ridker, P.M.; Wilson, P.W.F.; Grandy, S.M. Should C-reative protein be added to metabolic syndrome and to assessment of global cardiovascular risk? Circulation 2004, 109, 2818–20125. [Google Scholar] [CrossRef]
- Doi, Y.; Wakugawa, Y.; Kiyohara, Y.; Yonemoto, K.; Kubo, M.; Iwase, M.; Iida, M. Elevated C-reactive protein is a predictor of diabetes in a general Japanese population: The Hisayama study. Diab. Care 2005, 28, 2497–2500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oda, E.; Kawai, R. Reproducibility of high-sensitivity C-reactive protein as an inflammatory component of metabolic syndrome in Japanese. Circ. J. 2010, 74, 1488–1493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arai, Y.; Kamide, K.; Hirose, N. Adipokines and aging. Front. Endocrinol. 2019, 10, 142. [Google Scholar] [CrossRef]
- Ngatu, R.N. Health Effects of Dietary Supplementation of SUJIAONORI (Ulva Prolifera Muller) Biomaterials on Salivary Adiponectin, Cardiovascular Risk Parameters and Skin Health in Apparently Health Humans. Available online: https://trialsearch.who.int/Default.aspx (accessed on 21 August 2022).
- Hotta, K.; Funahashi, T.; Arita, Y.; Takahashi, M.; Matsuda, M.; Okamoto, Y.; Iwahashi, H.; Kuriyama, H.; Ouchi, N.; Maeda, K.; et al. Plasma concentration of a novel adipose-specific protein, adiponectin, in type 2 diabetic patients. Arterioscler. Thromb. Vasc. Biol. 2000, 20, 1595–1599. [Google Scholar] [CrossRef] [Green Version]
- Kubota, N.; Terauchi, Y.; Yamauchi, T.; Kubota, T.; Moroi, M.; Matsui, J.; Eto, K.; Yamashita, T.; Kamon, J.; Satoh, H.; et al. Disruption of adiponectin causes insulin resistance and neointimal formation. J. Biol. Chem. 2002, 277, 25863–25866. [Google Scholar] [CrossRef] [Green Version]
- Kumada, M.; Kihara, S.; Sumitsuji, S.; Kawamoto, T.; Matsumoto, S.; Ouchi, N.; Arita, Y.; Okamoto, Y.; Shimomura, L.; Hiraoka, H.; et al. Association of hypoadiponectinemia with coronary artery disease in men. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 85–89. [Google Scholar] [CrossRef]
- Okuda, M.; Sasaki, S. Assessment of foods with sodium and potassium intake in Japanese youths using the brief-type self-administered diet history questionnaire. Nutrients 2021, 13, 2345. [Google Scholar] [CrossRef] [PubMed]
- Kuo, I.C.; Wu, P.H.; Lin, H.Y.H.; Niu, S.W.; Huang, J.C.; Hung, C.C.; Chiu, Y.W.; Chen, H.C. The association of adiponectin with metabolic syndrome and clinical outcome in patients with non-diabetic chronic kidney disease. PLoS ONE 2019, 14, e0220158. [Google Scholar] [CrossRef] [Green Version]
- Fisman, E.Z.; Tenenbaum, A. Adiponectin: A manifold therapeutic target for metabolic syndrome, diabetes, and coronary disease? Cardiovasc. Diabetol. 2014, 13, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Achari, A.E.; Jain, S.K. Adiponectin, a therapeutic target for obesity, diabetes, and endothelial dysfunction. Int. J. Mol. Sci. 2017, 18, 1321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Vu, V.; Sweeney, G. Examining the Potential of Developing and Implementing Use of Adiponectin-Targeted Therapeutics for Metabolic and Cardiovascular Diseases. Front. Endocrinol. 2019, 10, 842. [Google Scholar] [CrossRef] [Green Version]
- Ngatu, R.N. Adiponectin modulators: New approach for scaling up noncommunicable diseases (NCDs) prevention and management? J. Int. Univ. Health Welf. 2019, 24, 73–75. [Google Scholar]
- Ngo, D.H.; Kim, S.K. Sulfated polysaccharides as bioactive agents from marine algae. Int. J. Biol. Macromol. 2013, 62, 70–75. [Google Scholar] [CrossRef]
- Wang, L.; Wang, X.; Wu, H.; Liu, R. Overview on biological activities and molecular characteristics of sulfated polysaccharides from marine green algae in recent years. Mar. Drugs 2014, 12, 4984–5020. [Google Scholar] [CrossRef] [Green Version]
- Ngatu, R.N.; Tanaka, M.; Ikeda, M.; Inoue, M.; Kanbara, S.; Nojima, S. Sujiaonori- derived algal biomaterials inhibit allergic reaction in allergen-sensitized RBL-2H3 cell line and improve skin health in humans. J. Funct. Biomater. 2017, 8, 37. [Google Scholar] [CrossRef] [Green Version]
- Farimani, A.R.; Hariri, M.; Azimi-Nezhad, M.; Borji, A.; Zarei, S.; Hooshmand, E. The effects of n-3 PUFAs on circulating adiponectin and leptin in patients with type 2 diabetes mellitus: A systematic review and meta-analysis of randomized controlled trials. Acta Diabetol. 2018, 55, 641–652. [Google Scholar] [CrossRef]
- Wu, P.; Wen, W.; Li, J.; Xu, J.; Zhao, M.; Chen, H.; Sun, J. Systematic review and meta-analysis of randomized Controlled Trials on the Effect of SGLT2 Inhibitor on Blood Leptin and Adiponectin Level in Patients with Type 2 Diabetes. Horm. Metab. Res. 2019, 51, 487–494. [Google Scholar] [CrossRef] [PubMed]
- University of Tokyo. Dietary Assessment Method Developed in Department of Social and Preventive Epidemiology at University of Tokyo. Available online: http://www.nutrepi.m.u-tokyo.ac.jp/english/dhq/dhq.html (accessed on 21 August 2022).
- Kobayashi, S.; Honda, S.; Murakami, K.; Sasaki, S.; Okubo, H.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Both comprehensive and brief self-administered diet history questionnaires satisfactorily rank nutrient intakes in Japanese adults. J. Epidemiol. 2012, 22, 151–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health, Labour and Welfare of Japan. The National Health and Nutrition Survey in Japan; Ministry of Health and Welfare: Tokyo, Japan, 2008. (In Japanese) [Google Scholar]
- Agency SaT. Standard Tables of Food Composition in Japan, 5th ed.; Printing Bureau of the Ministry of Finance: Tokyo, Japan, 2005. (In Japanese) [Google Scholar]
- Toyomaki, A.; Koga, M.; Okada, E.; Nakai, Y.; Miyazaki, A.; Tamakoshi, A.; Kiso, Y.; Kusumi, I. The relationship between a low grain intake dietary pattern and impulsive behaviors in middle-aged Japanese people. PLoS ONE 2017, 12, e0181057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maciejczyk, M.; Bielas, M.; Zalewska, A.; Gerreth, K. Salivary biomarkers of oxidative stress and inflammation in stroke patients: From basic research to clinical practice. Oxid. Med. Cell Longev. 2021, 2021, 5545330. [Google Scholar] [CrossRef]
- Desai, G.S.; Mathews, S.T. Saliva as a non-invasive diagnostic tool for inflammation and insulin resistance. World J. Diabetes 2014, 5, 730–738. [Google Scholar] [CrossRef]
- Kim, S.K.; Li, Y.X. Medicinal benefits of sulfated polysaccharides from sea vegetables. Adv. Food Nutr. Res. 2011, 64, 391–402. [Google Scholar] [CrossRef] [PubMed]
- Stanton, A.V.; James, K.; Brennan, M.M.; Buskandar, F.; Shortall, K.; El-Sayed, T.; Kennedy, J.; Hayes, H.; Fahey, A.G.; Pender, N.; et al. Omega-3 index and blood pressure responses to eating foods naturally enriched with omega-3 polyunsaturated fatty acids: A randomized controlled trial. Sci. Rep. 2020, 10, 15444. [Google Scholar] [CrossRef]
- Kim, S.K.; Pangestuti, R. Biological activities and potential health benefits of fucoxanthin derived from marine brown algae. Adv. Food Nutr. Res. 2011, 64, 111–128. [Google Scholar] [CrossRef]
- Lee, J.C.; Hou, M.F.; Huang, H.W.; Chang, F.R.; Yeh, C.C.; Tang, J.Y.; Chang, H.W. Marine algal natural products with anti-oxidative, anti-inflammatory, and anti-cancer properties. Cancer Cell Int. 2013, 13, 55. [Google Scholar] [CrossRef] [Green Version]
- Peng, J.; Zhao, F.; Yang, X.; Pan, X.; Wu, M.; Peng, Y.G. Association between dyslipidemia and risk of type 2 diabetes mellitus in middle-aged and older Chinese adults: A secondary analysis of a nationwide cohort. BMJ Open 2021, 11, e042821. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Control (n = 16) | NBF1 Group (n = 15) | p-Value | ||
|---|---|---|---|---|---|
| Mean (SD) | 95% CI | Mean (SD) | 95% CI | ||
| Clinical parameters | |||||
| Age (years) | 23.06 (1.55) | 19.74–26.39 | 23.06 (2.21) | 18.33–27.78 | 0.499 |
| BMI (kg/m2) | 21.43 (0.60) | 20.14–22.73 | 21.11 (0.59) | 19.84–22.3 | 0.353 |
| Diastolic BP (mmHg) | 73.26 (1.35) | 70.35–76.17 | 73.5 (1.34) | 70.63–76.36 | 0.451 |
| Systolic BP (mmHg) | 110.53 (2.09) | 105.04 –114.02 | 109.68 (2.04) | 103.92–112.25 | 0.046 * |
| Nutrients intake | |||||
| Vitamin B6 (mg/day) | 1.07 (0.18) | 0.69–1.46 | 0.781 (0.08) | 0.59–0.97 | 0.08 |
| Vitamin B12 (mg/day) | 9.43 (2.6) | 3.84–15.01 | 4.74 (0.46) | 3.73–5.75 | 0.055 |
| Vitamin C (mg/day) | 86.74 (18.49) | 57.08–136.40 | 85.31 (9.23) | 87.17–135.44 | 0.166 |
| Vitamin D (mg/day) | 13.21 (3.94) | 4.75–21.67 | 5.98 (0.59) | 4.69–17.27 | 0.058 |
| Total folates (mg/day) | 224.44 (50.35) | 176.43–392.44 | 215.66 (23.8) | 163.77–267.56 | 0.125 |
| α-tocopherol (mg/day) | 6.02 (0.74) | 4.42–7.61 | 6.22 (0.49) | 3.94–6.11 | 0.145 |
| n-3 PUFA (g/day) | 2.34 (0.29) | 1.21–2.98 | 3.24 (1.14) | 2.99–4.61 | 0.000 * |
| n-6 PUFA (g/day) | 7.81 (3.25) | 6.02–9.61 | 8.75 (3.12) | 5.35–10.98 | 0.218 |
| Fiber (g/day) | 9.63 (2.66) | 8.45–10.01 | 12.08 (1.53) | 11.93–13.44 | 0.000 * |
| Plant protein (g/day) | 18.98 (3.15) | 12.21–25.74 | 23.41 (1.77) | 19.56–27.25 | 0.124 |
| Animal protein (g/day) | 29.918 (3.8) | 21.75–38.08 | 23.45 (2.58) | 17.87–29.03 | 0.088 |
| Cholesterol (mg/day) | 236.68 (19.14) | 175.3–258.04 | 204.31 (38.5) | 201.69–446.9 | 0.031 * |
| A | ||||||
| Nutrients | CRP (pg/mL) | Adiponectin (ng/mL) | ||||
| β(SE) | 95% CI | p | β(SE) | 95% CI | p | |
| Vitamin B6 | −12.8 (6.71) | −22.91–201.81 | 0.023 * | 0.14 (0.13) | −0.013–1.04 | 0.293 |
| Vitamin B12 | 31.45 (10.27) | 26.78–60.12 | 0.135 | −7.88 (6.57) | −13.98–8.26 | 0.276 |
| Vitamin C | −8.79 (2.27) | −81.74–64.15 | 0.755 | 1.43 (0.28) | 0.26–2.11 | 0.182 |
| Vitamin D | −149.5 (78.3) | −267.31–32.69 | 0.033 * | 3.69 (2.95) | 3.42–17.81 | 0.034 * |
| Folates | 2.51 (10.58) | −22.69–31.71 | 0.688 | 0.65 (0.46) | −0.45–1.17 | 0.205 |
| α−tocopherol | 34.32 (20.17) | −159.1–228.72 | 0.283 | 26.4 (23.95) | −11.78–80.5 | 0.148 |
| Cholesterol | 0.05 (0.14) | −0.03–0.02 | 0.971 | −1.55 (1.42) | −8.65–5.54 | 0.655 |
| NBF1-n-3 PUFA | −65.82 (2.81) | −187.9–174.2 | 0.048 * | 5.96 (5.06) | 1.51–18.42 | 0.038 * |
| NBF1-n-6 PUFA | 7.41 (4.29) | −2.54–17.42 | 0.112 | 0.68 (0.33) | −1.46–3.95 | 0.079 |
| NBF1-fiber | −25.73 (43.97) | −122.52–71.06 | 0.057 | 10.51 (1.79) | 5.79–18.23 | 0.005 * |
| Plant protein | −0.11 (0.01) | −0.003–0.05 | 0.313 | 0.13 (0.06) | −0.54–0.57 | 0.962 |
| Animal protein | 2.09 (0.12) | −0.25–3.09 | 0.808 | −0.09 (2.22) | −0.57–1.37 | 0.678 |
| B | ||||||
| Nutrients | DBP (mmHg) | SBP (mmHg) | Nutrients | |||
| β(SE) | 95% CI | p | β(SE) | 95% CI | p | |
| Vitamin B6 | −2.48 (1.67) | −5.91–0.94 | 0.081 | 3.28(0.45) | −3.29–7.21 | 0.891 |
| Vitamin B12 | 0.24 (0.20) | −0.18–0.67 | 0.258 | 0.25 (0.23) | −0.024–0.73 | 0.305 |
| Vitamin C | −0.02 (0.08) | −0.06–0.01 | 0.278 | −0.22 (0.03) | −0.09–0.51 | 0.838 |
| Vitamin D | −0.02 (0.09) | −0.17–0.21 | 0.757 | 0.19 (0.15) | −0.13–0.54 | 0.243 |
| Folates | −0.07 (0.06) | −0.02–0.05 | 0.232 | −0.04 (0.02) | −0.07–0.37 | 0.471 |
| α−tocopherol | −0.51 (0.39) | −1.31–0.29 | 0.205 | −0.19 (0.07) | −1.58–1.55 | 0.890 |
| Cholesterol | −0.01 (0.00) | −0.02–0.01 | 0.089 | 0.03 (0.01) | −0.02–0.03 | 0.811 |
| NBF1-n-3 PUFA | −2.54 (0.39) | −5.81–5.03 | 0.042 * | −5.05 (1.98) | −12.83–8.86 | 0.301 |
| NBF1-n-6 PUFA | −0.43 (0.23) | −0.90–0.04 | 0.072 | −0.45 (0.04) | −1.34–0.43 | 0.304 |
| NBF1-fiber | 0.12 (0.05) | −0.01–0.05 | 0.853 | 0.29 (0.23) | −0.41–0.87 | 0.440 |
| Plant protein | 0.78 (0.37) | 0.24–1.65 | 0.592 | −0.15 (0.22) | −0.62–0.30 | 0.485 |
| Animal protein | 0.45 (0.12) | 0.19–0.71 | 0.11 | 0.14 (0.17) | −0.21–0.55 | 0.423 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ngatu, N.R.; Ikeda, M.; Tonduangu, D.K.; Nangana, S.L.; Hirao, T. Modulatory Effects of NBF1, an Algal Fiber-Rich Bioformula, on Adiponectin and C-Reactive Protein Levels, and Its Therapeutic Prospects for Metabolic Syndrome and Type-2 Diabetes Patients. Biomedicines 2022, 10, 2572. https://doi.org/10.3390/biomedicines10102572
Ngatu NR, Ikeda M, Tonduangu DK, Nangana SL, Hirao T. Modulatory Effects of NBF1, an Algal Fiber-Rich Bioformula, on Adiponectin and C-Reactive Protein Levels, and Its Therapeutic Prospects for Metabolic Syndrome and Type-2 Diabetes Patients. Biomedicines. 2022; 10(10):2572. https://doi.org/10.3390/biomedicines10102572
Chicago/Turabian StyleNgatu, Nlandu Roger, Mitsunori Ikeda, Daniel Kuezina Tonduangu, Severin Luzitu Nangana, and Tomohiro Hirao. 2022. "Modulatory Effects of NBF1, an Algal Fiber-Rich Bioformula, on Adiponectin and C-Reactive Protein Levels, and Its Therapeutic Prospects for Metabolic Syndrome and Type-2 Diabetes Patients" Biomedicines 10, no. 10: 2572. https://doi.org/10.3390/biomedicines10102572